![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
381 Cards in this Set
- Front
- Back
|
Lymphatic System |
Returns fluids that leaked from blood vessels back to blood • Consists of three parts 1. Network of lymphatic vessels (lymphatics) 2. Lymph – fluid in vessels 3. Lymph nodes – cleanse lymph |
|
|
Lymphoid Organs and Tissues |
Provide structural basis of immune system • House phagocytic cells and lymphocytes • Structures include spleen, thymus, tonsils, lymph nodes, other lymphoid tissues |
|
|
Lymphatic System: Functions |
Lymphatic vessels (lymphatics) – Return interstitial fluid and leaked plasma proteins back to blood – ~ 3L / day – Once interstitial fluid enters lymphatics, called lymph |
|
|
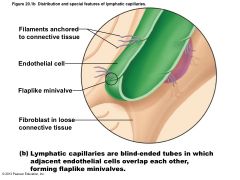
Distribution and special features of lymphatic capillaries |

|
|
|
Lymphatic Vessels: Distribution and Structure |
One-way system; lymph flows toward heart • Lymph vessels (lymphatics) include: – Lymphatic capillaries – Collecting lymphatic vessels – Lymphatic trunks and ducts |
|
|
Lymphatic Capillaries |
Similar to blood capillaries, except – Very permeable (take up proteins, cell debris, pathogens, and cancer cells) • Endothelial cells overlap loosely to form one-way minivalves • Anchored by collagen filaments, preventing collapse of capillaries; increased ECF volume opens minivalves – Pathogens travel throughout body via lymphatics |
|
|
Lymphatic Capillaries
|
Absent from bones, teeth, bone marrow, and CNS • Lacteals: specialized lymph capillaries present in intestinal mucosa – Absorb digested fat and deliver fatty lymph (chyle) to the blood |
|
|
Distribution and special features of lymphatic capillaries |
|
|
|
Lymphatic Collecting Vessels |
Similar to veins, except – Have thinner walls, with more internal valves – Anastomose more frequently • Collecting vessels in skin travel with superficial veins • Deep vessels travel with arteries • Nutrients supplied from branching vasa vasorum |
|
|
Lymphatic Trunks |
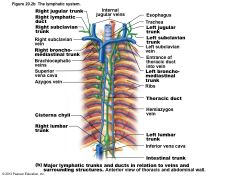
Formed by union of largest collecting ducts – Paired lumbar – Paired bronchomediastinal – Paired subclavian – Paired jugular trunks – Single intestinal trunk |
|
|
Lymphatic Ducts |
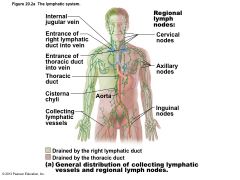
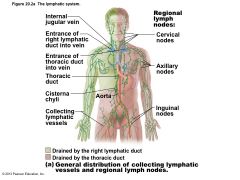
Lymph delivered into one of two large ducts – Right lymphatic duct drains right upper arm and right side of head and thorax – Thoracic duct arises as cisterna chyli; drains rest of body • Each empties lymph into venous circulation at junction of internal jugular and subclavian veins on its own side of body |
|
|
Figure 20.2a The lymphatic system |
|
|
|
Figure 20.2b The lymphatic system. |
|
|
|
Lymph Transport |
Lymph propelled by – Milking action of skeletal muscle – Pressure changes in thorax during breathing – Valves to prevent backflow – Pulsations of nearby arteries – Contractions of smooth muscle in walls of lymphatics |
|
|
Lymphoid Cells |
Lymphocytes main warriors of immune system – Arise in red bone marrow • Mature into one of two main varieties – T cells (T lymphocytes) – B cells (B lymphocytes) |
|
|
Lymphocytes |
T cells and B cells protect against antigens – Anything body perceives as foreign • Bacteria and bacterial toxins, viruses, mismatched RBCs, cancer cells |
|
|
Other Lymphoid Cells
Macrophages |
phagocytize foreign substances; help activate T cells |
|
|
Dendritic cells |
capture antigens and deliver them to lymph nodes; activate T cells |
|
|
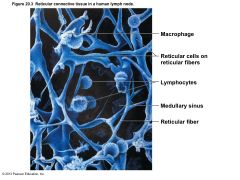
Reticular cells |
produce reticular fiber stroma that supports other cells in lymphoid organs |
|
|
Figure 20.3 Reticular connective tissue in a human lymph node. |
|
|
|
Lymphoid Tissue |
Houses, and provides proliferation site for, lymphocytes • Surveillance vantage point for lymphocytes and macrophages • Largely reticular connective tissue – type of loose connective tissue • Two main types – Diffuse lymphoid tissue; Lymphoid follicles |
|
|
Lymphoid Tissue |
Diffuse lymphoid tissue of lymphoid cells and reticular fibers in ~ every body organ – Larger collections in lamina propria of mucous membranes |
|
|
Lymphoid Tissue |
Lymphoid follicles (nodules) are solid, spherical bodies of tightly packed lymphoid cells and reticular fibers – Germinal centers of proliferating B cells – May form part of larger lymphoid organs – Isolated aggregations of Peyer's patches and in appendix |
|
|
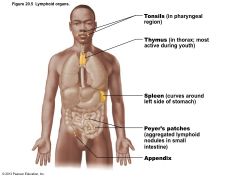
Figure 20.5 Lymphoid organs |
|
|
|
Lymph Nodes |
Principal lymphoid organs of body • Embedded in connective tissue, in clusters along lymphatic vessels • Near body surface in inguinal, axillary, and cervical regions of body |
|
|
Figure 20.2a The lymphatic system. |
|
|
|
Lymph Nodes • Functions |
1. Filter lymph—macrophages destroy microorganisms and debris 2. Immune system activation—lymphocytes activated and mount attack against antigens |
|
|
Structure of a Lymph Node |
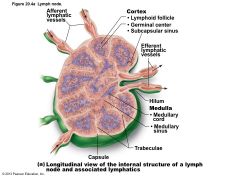
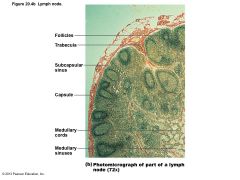
Vary in shape and size but most bean shaped • External fibrous capsule • Trabeculae extend inward and divide node into compartments • Two histologically distinct regions – Cortex – Medulla |
|
|
Structure of a Lymph Node |
• Cortex contains follicles with germinal centers, heavy with dividing B cells • Dendritic cells nearly encapsulate follicles • Deep cortex houses T cells in transit • T cells circulate continuously among blood, lymph nodes, and lymph |
|
|
Figure 20.4a Lymph node. |
|
|
|
Structure of a Lymph Node |
• Medullary cords extend inward from cortex and contain B cells, T cells, and plasma cells • Lymph sinuses contain macrophages |
|
|
Figure 20.4b Lymph node. |
|
|
|
Circulation in the Lymph Nodes |
• Lymph – Enters convex side via afferent lymphatic vessels; travels through large subcapsular sinus and smaller sinuses to medullary sinuses; exits concave side at hilum via efferent vessels • Fewer efferent vessels so flow somewhat stagnate; allows lymphocytes and macrophages time to function |
|
|
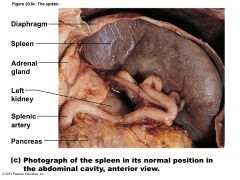
Spleen |
• Largest lymphoid organ • Served by splenic artery and vein, which enter and exit at the hilum • Functions – Site of lymphocyte proliferation and immune surveillance and response – Cleanses blood of aged cells and platelets, macrophages remove debris |
|
|
Figure 20.6c The spleen. |
|
|
|
Spleen: Additional Functions |
• Stores breakdown products of RBCs (e.g., iron) for later reuse • Stores blood platelets and monocytes • May be site of fetal erythrocyte production (normally ceases before birth) • Encased by fibrous capsule; has trabeculae • Contains lymphocytes, macrophages, and huge numbers of erythrocytes |
|
|
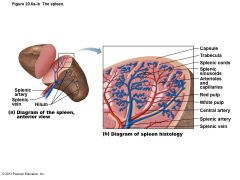
Structure of the Spleen |
• Two distinct areas – White pulp around central arteries • Mostly lymphocytes on reticular fibers; involved in immune functions – Red pulp in venous sinuses and splenic cords • Rich in RBCs and macrophages for disposal of worn-out RBCs and bloodborne pathogens • Composed of splenic cords and sinusoids |
|
|
Figure 20.6a–b The spleen. |
|
|
|
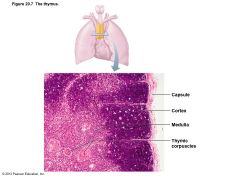
Thymus |
• Important functions early in life • Found in inferior neck; extends into mediastinum; partially overlies heart • Increases in size and most active during childhood • Stops growing during adolescence, then gradually atrophies – Still produces immunocompetent cells, though slowly |
|
|
Figure 20.7 The thymus. |
|
|
|
Thymus |
• Differs from other lymphoid organs in important ways – Has no follicles because it lacks B cells – Does not directly fight antigens • Functions strictly in T lymphocyte maturation – Keeps isolated via blood thymus barrier • Stroma of epithelial cells (not reticular fibers) – Provide environment in which T lymphocytes become immunocompetent |
|
|
Mucosa-associated Lymphoid Tissue (MALT) |
• Lymphoid tissues in mucous membranes throughout body • Protects from pathogens trying to enter body • Largest collections of MALT in tonsils, Peyer's patches, appendix • Also in mucosa of respiratory and genitourinary organs; rest of digestive tract |
|
|
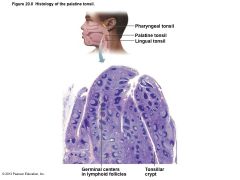
Tonsils |
• Simplest lymphoid organs • Form ring of lymphatic tissue around pharynx – Palatine tonsils—at posterior end of oral cavity – Lingual tonsil—grouped at base of tongue – Pharyngeal tonsil—in posterior wall of nasopharynx – Tubal tonsils—surrounding openings of auditory tubes into pharynx • Gather and remove pathogens in food or air |
|
|
Tonsils |
• Contain follicles with germinal centers • Are not fully encapsulated • Overlying epithelium invaginates forming tonsillar crypts – Trap and destroy bacteria and particulate matter – Allow immune cells to build memory for pathogens |
|
|
Figure 20.8 Histology of the palatine tonsil |
|
|
|
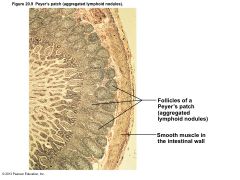
Aggregates of Lymphoid Follicles |
• Peyer's patches – Clusters of lymphoid follicles – In wall of distal portion of small intestine – Similar structures are also found in the appendix • Peyer's patches and appendix – Destroy bacteria, preventing them from breaching intestinal wall – Generate "memory" lymphocytes |
|
|
Figure 20.9 Peyer’s patch (aggregated lymphoid nodules). |
|
|
|
Developmental Aspects |
• Beginnings of lymphatic vessels and main clusters of lymph nodes by 5th week of embryonic development – Arise as lymph sacs from developing veins – Jugular lymph sacs arise right lymphatic duct and thoracic duct • Lymphatic organs (except thymus) arise from mesoderm |
|
|
Developmental Aspects |
• Lymphoid organs (except thymus) develop from mesodermal mesenchymal cells • Thymus (endodermal origin) forms as an outgrowth of pharynx • Except for spleen and tonsils, lymphoid organs poorly developed at birth • After birth high numbers of lymphocytes; their development parallels maturation of immune system |
|
|
Lymphangitis is caused by ______. |
an infection
|
|
|
Lymphedema may be treated by all EXCEPT which of the following? |
bed rest to allow enhanced blood flow and therefore healing of the affected area
|
|
|
Which of the following is NOT a part of the lymphatic system? |
blood vessels
|
|
|
What is the role of the mini-valves in lymph capillaries? |
increase permeability
|
|
|
Lymph is most similar to __________. |
interstitial fluid
|
|
|
Lymphatic collecting vessels are most closely associated with __________. |
capillary beds
|
|
|
Which of the following statements is true regarding veins versus lymphatic collecting vessels? |
Veins have fewer internal valves than do lymphatic vessels.
|
|
|
Once collected, lymph is returned to __________. |
venous circulation
|
|
|
Lymphatic vessels __________. |
return tissue fluid to the bloodstream
|
|
|
Adjacent cells in lymphatic capillaries overlap each other loosely. These cells form a unique structural modification that increases their permeability that is known as the __________.
|
minivalves
|
|
|
Which of the following promotes closure of the minivalves associated with lymph capillaries?
|
increasing pressure inside the lymph capillary
|
|
|
To what organ do the lymphatic vessels return protein-rich escaped fluids to rejoin circulation?
|
heart
|
|
|
What do collecting lymphatic vessels NOT share in common with veins of the cardiovascular system?
|
thickness of the walls
|
|
|
What is the main function of the lymphatic system?
|
The lymphatic system returns leaked fluid and plasma proteins that escape from the bloodstream to the blood.
|
|
|
Which of the following lacks lymph capillaries?
|
bones and teeth
|
|
|
Lymph from the right leg ultimately is delivered to which duct in the thoracic region?
|
thoracic duct
|
|
|
Lymph from what regions of the body is drained into the right lymphatic duct?
|
right upper limb, right side of the head and thorax
|
|
|
What is the name of the enlarged sac to which the lumbar trunks and the intestinal trunk returns lymph?
|
cisterna chyli
|
|
|
Which of the following returns lymph to the right lymphatic duct?
|
right side of the head
|
|
|
Which of the following delivers lymph into the junction of the internal jugular vein and the subclavian vein?
|
thoracic duct
|
|
|
Which of the following lymphoid cells secrete antibodies? |
plasma cells
|
|
|
Which lymphoid organ serves as the site where T lymphocytes become immunocompetent T cells? |
thymus gland
|
|
|
Which of the following is NOT a lymphatic cell? |
eosinophil
|
|
|
Antibodies are produced by __________. |
plasma cells
|
|
|
Which of the following lymphoid tissues/organs does NOT contain reticular connective tissue? |
thymus
|
|
|
Which of the following is NOT a lymphoid tissue/organ? |
bone marrow
|
|
|
What type of tissue is commonly found in all lymphoid organs and tissues (except the thymus)?
|
reticular connective tissue
|
|
|
What is the role of the B lymphocytes (B cells) in lymphoid tissue?
|
produce plasma cells that secrete antibodies
|
|
|
What is the role of dendritic cells in lymphoid tissue?
|
capture antigens and bring them back to lymph nodes
|
|
|
Within buboes, bacteria are directly attacked by ______. |
macrophages
|
|
|
Which lymphoid organ serves in immune surveillance and in filtering lymph? |
lymph nodes
|
|
|
Which of the following is a role of lymph nodes? |
They filter lymph.
|
|
|
Lymph arrives to the lymph nodes via efferent lymphatic vessels. |
False
|
|
|
Where are the three large clusters of superficial lymph nodes?
|
cervical, inguinal, and axillary regions
|
|
|
The filtration of lymph and immune system activation are the two basic functions of the __________.
|
lymph nodes
|
|
|
Lymph nodes are surrounded by a capsule from which connective tissue strands extend inward to divide the node into compartments. What is the name of these strands?
|
trabeculae
|
|
|
What region of the lymph node contains densely packed follicles with dividing B cells?
|
cortex
|
|
|
After surgical removal of the spleen (i.e., a splenectomy), some other organs take over most of its functions. Which of the following spleen functions in the adult can not be performed by bone marrow? |
removal of aged and damaged red blood cells from the blood
|
|
|
Which lymphoid organ provides a site for lymphocyte proliferation and immune surveillance and response and provides blood-cleansing functions? |
spleen
|
|
|
Of the following lymphoid organs, which is (are) structurally simplest and lack(s) a complete capsule? |
tonsils
|
|
|
Which of the following is NOT a part of MALT (mucosa-associated lymphoid tissue)? |
lymph nodes
|
|
|
Where are Peyer's patches located? |
distal portion of the small intestine
|
|
|
The __________ is (are) the most likely to become infected. |
palatine tonsils
|
|
|
Peyer's patches are located __________. |
in the wall of the small intestine
|
|
|
The first lymphoid organ(s) to appear during fetal development is (are) the __________. |
thymus
|
|
|
Which part of the spleen is the site of immune function?
|
white pulp
|
|
|
Where are worn-out erythrocytes found in the spleen?
|
red pulp
|
|
|
Where is the spleen located?
|
left side of the abdominal cavity just beneath the diaphragm and curled around the anterior aspect of the stomach
|
|
|
Where is the lingual tonsil located?
|
base of the tongue
|
|
|
Tonsillar crypts are invaginations deep into the interior of the tonsil. What is missing from the tonsil that allows for the presence of tonsillar crypts?
|
capsule
|
|
|
The thymus functions strictly in maturation of T cells. |
True
|
|
|
Immunity |
• Resistance to disease • Immune system – Two intrinsic systems • Innate (nonspecific) defense system • Adaptive (specific) defense system • Functional system rather than organ system • Innate and adaptive defenses intertwined • Release and recognize many of same defensive molecules • Innate defenses do have specific pathways for certain substances • Innate responses release proteins that alert cells of adaptive system to foreign molecules |
|
|
Immunity |
• Innate defense system has two lines of defense – First - external body membranes (skin and mucosae) – Second - antimicrobial proteins, phagocytes, and other cells • Inhibit spread of invaders • Inflammation most important mechanism • Adaptive defense system – Third line of defense attacks particular foreign substances • Takes longer to react than innate system |
|
|
Overview of innate and adaptive defenses. |

|
|
|
Innate Defenses |
• Surface barriers ward off invading pathogens – Skin, mucous membranes, and their secretions • Physical barrier to most microorganisms • Keratin resistant to weak acids and bases, bacterial enzymes, and toxins • Mucosae provide similar mechanical barriers |
|
|
Surface Barriers |
• Protective chemicals inhibit or destroy microorganisms – Acidity of skin and secretions – acid mantle – inhibits growth – Enzymes - lysozyme of saliva, respiratory mucus, and lacrimal fluid – kill many microorganisms – Defensins – antimicrobial peptides – inhibit growth – Other chemicals - lipids in sebum, dermcidin in sweat – toxic |
|
|
Surface Barriers |
• Respiratory system modifications – Mucus-coated hairs in nose – Cilia of upper respiratory tract sweep dustand bacteria-laden mucus toward mouth • Surface barriers breached by nicks or cuts - second line of defense must protect deeper tissues |
|
|
Internal Defenses: Cells and Chemicals |
• Necessary if microorganisms invade deeper tissues – Phagocytes – Natural killer (NK) cells – Antimicrobial proteins (interferons and complement proteins) – Fever – Inflammatory response (macrophages, mast cells, WBCs, and inflammatory chemicals) |
|
|
Phagocytes |
• Neutrophils most abundant but die fighting – Become phagocytic on exposure to infectious material • Macrophages develop from monocytes – chief phagocytic cells – robust cells • Free macrophages wander through tissue spaces, e.g., alveolar macrophages • Fixed macrophages permanent residents of some organs; e.g., stellate macrophages (liver) and microglia (brain) |
|
|
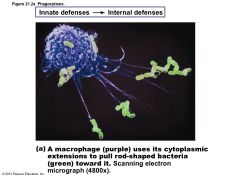
Mechanism of Phagocytosis |
• Phagocyte must adhere to particle – Some microorganisms evade adherence with capsule • Opsonization marks pathogens—coating by complement proteins or antibodies • Cytoplasmic extensions bind to and engulf particle in vesicle called phagosome • Phagosome fuses with lysosome à phagolysosome |
|
|
Figure 21.2a Phagocytosis. |
|
|
|
Figure 21.2b Phagocytosis. |

|
|
|
Mechanism of Phagocytosis |
• Pathogens killed by acidifying and digesting with lysosomal enzymes • Helper T cells cause release of enzymes of respiratory burst, which kill pathogens resistant to lysosomal enzymes by – Releasing cell-killing free radicals – Producing oxidizing chemicals (e.g., H2O2) – Increasing pH and osmolarity of phagolysosome • Defensins (in neutrophils) pierce membrane |
|
|
Natural Killer (NK) Cells |
• Nonphagocytic large granular lymphocytes • Attack cells that lack "self" cell-surface receptors – Induce apoptosis in cancer cells and virusinfected cells • Secrete potent chemicals that enhance inflammatory response |
|
|
Inflammatory Response |
• Triggered whenever body tissues injured • Prevents spread of damaging agents • Disposes of cell debris and pathogens • Alerts adaptive immune system • Sets the stage for repair |
|
|
Inflammatory Response |
• Cardinal signs of acute inflammation: 1. Redness 2. Heat 3. Swelling 4. Pain (Sometimes 5. Impairment of function) |
|
|
Inflammatory Response |
• Begins with chemicals released into ECF by injured tissues, immune cells, blood proteins • Macrophages and epithelial cells of boundary tissues bear Toll-like receptors (TLRs) • 11 types of TLRs recognize specific classes of infecting microbes • Activated TLRs trigger release of cytokines that promote inflammation |
|
|
Inflammatory Response |
• Inflammatory mediators – Kinins, prostaglandins (PGs), and complement • Dilate local arterioles (hyperemia) – Causes redness and heat of inflamed region • Make capillaries leaky • Many attract leukocytes to area • Some have inflammatory roles |
|
|
Inflammatory Response: Edema |
• á Capillary permeability à exudate to tissues – Fluid containing clotting factors and antibodies – Causes local swelling (edema) – Swelling pushes on nerve endings à pain • Pain also from bacterial toxins, prostaglandins, and kinins – Moves foreign material into lymphatic vessels – Delivers clotting proteins and complement |
|
|
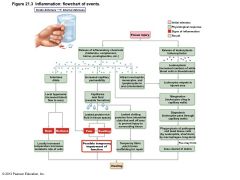
Inflammatory Response |
• Clotting factors form fibrin mesh – Scaffold for repair – Isolates injured area so invaders cannot spread |
|
|
Figure 21.3 Inflammation: flowchart of events. |
|
|
|
Phagocyte Mobilization |
• Neutrophils lead; macrophages follow – As attack continues, monocytes arrive • 12 hours after leaving bloodstream à macrophages • These "late-arrivers" replace dying neutrophils and remain for clean up prior to repair • If inflammation due to pathogens, complement activated; adaptive immunity elements arrive |
|
|
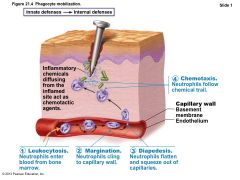
Phagocyte Mobilization |
• Steps for phagocyte mobilization 1. Leukocytosis: release of neutrophils from bone marrow in response to leukocytosisinducing factors from injured cells 2. Margination: neutrophils cling to walls of capillaries in inflamed area in response to CAMs 3. Diapedesis of neutrophils 4. Chemotaxis: inflammatory chemicals (chemotactic agent) promote positive chemotaxis of neutrophils |
|
|
Figure 21.4 Phagocyte mobilization. |
|
|
|
Antimicrobial Proteins |
• Include interferons and complement proteins • Some attack microorganisms directly • Some hinder microorganisms' ability to reproduce |
|
|
Interferons |
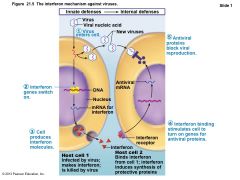
• Family of immune modulating proteins – Have slightly different physiological effects • Viral-infected cells secrete IFNs (e.g., IFN alpha and beta) to "warn" neighboring cells – IFNs enter neighboring cells à produce proteins that block viral reproduction and degrade viral RNA – IFN alpha and beta also activate NK cells |
|
|
Interferons |
• IFN gamma (immune interferon) – Secreted by lymphocytes – Widespread immune mobilizing effects – Activates macrophages • Since IFNs activate NK cells and macrophages, indirectly fight cancer • Artificial IFNs used to treat hepatitis C, genital warts, multiple sclerosis, hairy cell leukemia |
|
|
Figure 21.5 The interferon mechanism against viruses. |
|
|
|
Complement System (Complement) |
• ~20 blood proteins that circulate in inactive form • Include C1–C9, factors B, D, and P, and regulatory proteins • Major mechanism for destroying foreign substances • Our cells contain complement activation inhibitors |
|
|
Complement |
• Unleashes inflammatory chemicals that amplify all aspects of inflammatory response • Kills bacteria and certain other cell types by cell lysis • Enhances both innate and adaptive defenses |
|
|
Complement Activation |
• Three pathways to activation – Classical pathway • Antibodies bind to invading organisms and to complement components • Called complement fixation • First step in activation; more details later |
|
|
Complement |
• Lectin pathway – Lectins - produced by innate system to recognize foreign invaders – When bound to foreign invaders can also bind and activate complement • Alternative pathway – Activated spontaneously, lack of inhibitors on microorganism's surface allows process to proceed |
|
|
Complement Activation |
• Each pathway involves activation of proteins in an orderly sequence • Each step catalyzes the next • Each pathway converges on C3, which cleaves into C3a and C3b • Common terminal pathway initiated that – Enhances inflammation, promotes phagocytosis, causes cell lysis |
|
|
Complement Activation |
• Three pathways to activation – Classical pathway • Antibodies bind to invading organisms and to complement components • Called complement fixation • First step in activation; more details later |
|
|
Complement |
• Lectin pathway – Lectins - produced by innate system to recognize foreign invaders – When bound to foreign invaders can also bind and activate complement • Alternative pathway – Activated spontaneously, lack of inhibitors on microorganism's surface allows process to proceed |
|
|
Complement Activation |
• Each pathway involves activation of proteins in an orderly sequence • Each step catalyzes the next • Each pathway converges on C3, which cleaves into C3a and C3b • Common terminal pathway initiated that – Enhances inflammation, promotes phagocytosis, causes cell lysis |
|
|
Complement Activation |
• Cell lysis begins when – C3b binds to target cell à insertion of complement proteins called membrane attack complex (MAC) into cell's membrane – MAC forms and stabilizes hole in membrane à influx of water à lysis of cell • C3b also causes opsonization • C3a and other cleavage products amplify inflammation – Stimulate mast cells and basophils to release histamine – Attract neutrophils and other inflammatory cells |
|
|
Figure 21.6 Complement activation. |

|
|
|
Fever |
• Abnormally high body temperature • Systemic response to invading microorganisms • Leukocytes and macrophages exposed to foreign substances secrete pyrogens • Pyrogens act on body's thermostat in hypothalamus, raising body temperature |
|
|
Fever |
• Benefits of moderate fever – Causes liver and spleen to sequester iron and zinc (needed by microorganisms) – Increases metabolic rate à faster repair |
|
|
Adaptive Defenses |
• Adaptive immune (specific defense) system – Protects against infectious agents and abnormal body cells – Amplifies inflammatory response – Activates complement – Must be primed by initial exposure to specific foreign substance • Priming takes time |
|
|
Adaptive Defenses |
• Specific – recognizes and targets specific antigens • Systemic – not restricted to initial site • Have memory – stronger attacks to "known" antigens • Two separate, overlapping arms – Humoral (antibody-mediated) immunity – Cellular (cell-mediated) immunity |
|
|
Humoral Immunity |
• Antibodies, produced by lymphocytes, circulating freely in body fluids • Bind temporarily to target cell – Temporarily inactivate – Mark for destruction by phagocytes or complement • Humoral immunity has extracellular targets |
|
|
Cellular Immunity |
• Lymphocytes act against target cell – Directly – by killing infected cells – Indirectly – by releasing chemicals that enhance inflammatory response; or activating other lymphocytes or macrophages • Cellular immunity has cellular targets |
|
|
Antigens |
• Substances that can mobilize adaptive defenses and provoke an immune response • Targets of all adaptive immune responses • Most are large, complex molecules not normally found in body (nonself) |
|
|
Complete Antigens |
• Important functional properties – Immunogenicity: ability to stimulate proliferation of specific lymphocytes – Reactivity: ability to react with activated lymphocytes and antibodies released by immunogenic reactions • Examples: foreign protein, polysaccharides, lipids, and nucleic acids |
|
|
Haptens (Incomplete Antigens) |
• Small molecules (haptens) not immunogenic by themselves – E.g., peptides, nucleotides, some hormones • May be immunogenic if attached to body proteins and combination is marked foreign • Cause immune system to mount harmful attack • Examples: poison ivy, animal dander, detergents, and cosmetics |
|
|
Antigenic Determinants |
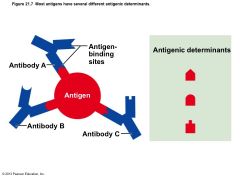
• Only certain parts (antigenic determinants) of entire antigen are immunogenic • Antibodies and lymphocyte receptors bind to them as enzyme binds substrate |
|
|
Antigenic Determinants |
• Most naturally occurring antigens have numerous antigenic determinants that – Mobilize several different lymphocyte populations – Form different kinds of antibodies against them • Large, chemically simple molecules (e.g., plastics) have little or no immunogenicity |
|
|
Figure 21.7 Most antigens have several different antigenic determinants. |
|
|
|
Self-antigens: MHC Proteins |
• Protein molecules (self-antigens) on surface of cells not antigenic to self but antigenic to others in transfusions or grafts • Example: MHC glycoproteins – Coded by genes of major histocompatibility complex (MHC) and unique to individual – Have groove holding self- or foreign antigen • T lymphocytes can only recognize antigens that are presented on MHC proteins |
|
|
Cells of the Adaptive Immune System |
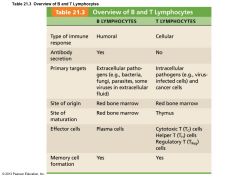
• Three types of cells – Two types of lymphocytes • B lymphocytes (B cells)—humoral immunity • T lymphocytes (T cells)—cellular immunity – Antigen-presenting cells (APCs) • Do not respond to specific antigens • Play essential auxiliary roles in immunity |
|
|
Lymphocyte Development, Maturation, and Activation |
• Five general steps – Origin – all originate in red bone marrow – Maturation – Seeding secondary lymphoid organs and circulation – Antigen encounter and activation – Proliferation and differentiation |
|
|
Figure 21.8 Lymphocyte development, maturation, and activation. |

|
|
|
Maturation |
• "Educated" to become mature; B cells in bone marrow, T cells in thymus – Immunocompetence – lymphocyte can recognize one specific antigen by binding to it • B or T cells display only one unique type of antigen receptor on surface when achieve maturity – bind only one antigen – Self-tolerance • Lymphocytes unresponsive to own antigens |
|
|
T cells |
• T cells mature in thymus under negative and positive selection pressures ("tests") – Positive selection • Selects T cells capable of recognizing self-MHC proteins (MHC restriction); failures destroyed by apoptosis – Negative selection • Prompts apoptosis of T cells that bind to selfantigens displayed by self-MHC • Ensures self-tolerance |
|
|
Figure 21.9 T cell education in the thymus. |

|
|
|
B cells |
• B cells mature in red bone marrow • Positively selected if successfully make antigen receptors • Those that are self-reactive – Eliminated by apoptosis (clonal deletion) |
|
|
Seeding Secondary Lymphoid Organs and Circulation |
• Immunocompetent B and T cells not yet exposed to antigen called naive • Exported from primary lymphoid organs (bone marrow and thymus) to "seed" secondary lymphoid organs (lymph nodes, spleen, etc.) – Increases chance of encounter with antigen |
|
|
Antigen Encounter and Activation |
• Clonal selection – Naive lymphocyte's first encounter with antigen à selected for further development – If correct signals present, lymphocyte will complete its differentiation |
|
|
Proliferation and Differentiation |
• Activated lymphocyte proliferates à exact clones • Most clones à effector cells that fight infections • Few remain as memory cells – Able to respond to same antigen more quickly second time • B and T memory cells and effector T cells circulate continuously |
|
|
Antigen Receptor Diversity |
• Genes, not antigens, determine which foreign substances immune system will recognize – Immune cell receptors result of acquired knowledge of microbes likely in environment • Lymphocytes make up to billion different types of antigen receptors – Coded for by ~25,000 genes – Gene segments are shuffled by somatic recombination |
|
|
Table 21.3 Overview of B and T Lymphocyt |
|
|
|
Antigen-presenting Cells (APCs) |
• Engulf antigens • Present fragments of antigens to T cells for recognition • Major types – Dendritic cells in connective tissues and epidermis – Macrophages in connective tissues and lymphoid organs – B cells |
|
|
Dendritic Cells and Macrophages |
• Dendritic cells phagocytize pathogens, enter lymphatics to present antigens to T cells in lymph node – Most effective antigen presenter known – Key link between innate and adaptive immunity • Macrophages widespread in lymphoid organs and connective tissues – Present antigens to T cells to activate themselves into voracious phagocytes that secrete bactericidal chemicals |
|
|
B lymphocytes |
• Do not activate naive T cells • Present antigens to helper T cell to assist own activation |
|
|
Adaptive Immunity: Summary |
• Uses lymphocytes, APCs, and specific molecules to identify and destroy nonself substances • Depends upon ability of its cells to – Recognize antigens by binding to them – Communicate with one another so that whole system mounts specific response |
|
|
Activation and Differentiation of B Cells |
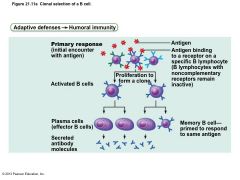
• B cell activated when antigens bind to its surface receptors and cross-link them à • Receptor-mediated endocytosis of crosslinked antigen-receptor complexes (clonal selection) à • Proliferation and differentiation into effector cells |
|
|
Fate of the Clones |
• Most clone cells become plasma cells – Secrete specific antibodies at rate of 2000 molecules per second for four to five days, then die – Antibodies circulate in blood or lymph • Bind to free antigens and mark for destruction by innate or adaptive mechanisms |
|
|
Fate of the Clones |
• Clone cells that do not become plasma cells become memory cells – Provide immunological memory – Mount an immediate response to future exposures to same antigen |
|
|
Figure 21.11a Clonal selection of a B cell. |
|
|
|
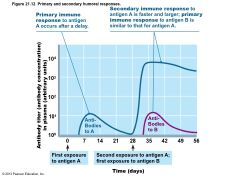
Immunological Memory |
• Primary immune response – Cell proliferation and differentiation upon first antigen exposure – Lag period: three to six days – Peak levels of plasma antibody are reached in 10 days – Antibody levels then decline |
|
|
Immunological Memory |
• Secondary immune response – Re-exposure to same antigen gives faster, more prolonged, more effective response • Sensitized memory cells respond within hours • Antibody levels peak in two to three days at much higher levels • Antibodies bind with greater affinity • Antibody level can remain high for weeks to months |
|
|
Figure 21.11 Clonal selection of a B cell |

|
|
|
Figure 21.12 Primary and secondary humoral responses |
|
|
|
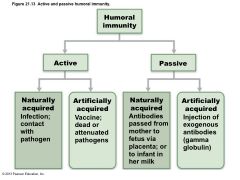
Active Humoral Immunity |
• When B cells encounter antigens and produce specific antibodies against them • Two types of active humoral immunity: – Naturally acquired—response to bacterial or viral infection – Artificially acquired—response to vaccine of dead or attenuated pathogens |
|
|
Active Humoral Immunity |
• Vaccines – Most of dead or attenuated pathogens – Spare us symptoms of primary response – Provide antigenic determinants that are immunogenic and reactive |
|
|
Passive Humoral Immunity |
• Readymade antibodies introduced into body • B cells are not challenged by antigens • Immunological memory does not occur • Protection ends when antibodies degrade |
|
|
Passive Humoral Immunity |
• Two types 1. Naturally acquired—antibodies delivered to fetus via placenta or to infant through milk 2. Artificially acquired—injection of serum, such as gamma globulin • Protection immediate but ends when antibodies naturally degrade in body |
|
|
Figure 21.13 Active and passive humoral immunity. |
|
|
|
Antibodies |
• Immunoglobulins—gamma globulin portion of blood • Proteins secreted by plasma cells • Capable of binding specifically with antigen detected by B cells • Grouped into one of five Ig classes |
|
|
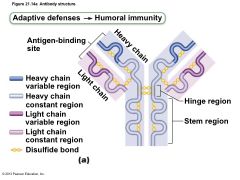
Basic Antibody Structure |
• T- or Y-shaped antibody monomer of four looping polypeptide chains linked by disulfide bonds • Two identical heavy (H) chains with hinge region at "middles" • Two identical light (L) chains • Variable (V) regions at one end of each arm combine to form two identical antigen-binding sites |
|
|
Basic Antibody Structure |
• Constant (C) regions of stem – Determine antibody class (IgM, IgA, IgD, IgG, or IgE) – Serve common functions in all antibodies by dictating • Cells and chemicals that antibody can bind • How antibody class functions to eliminate antigens |
|
|
Figure 21.14a Antibody structure |
|
|
|
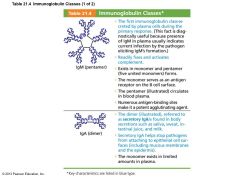
Classes of Antibodies |
• IgM – Pentamer (larger than others); first antibody released – Potent agglutinating agent – Readily fixes and activates complement • IgA (secretory IgA) – Monomer or dimer; in mucus and other secretions – Helps prevent entry of pathogens |
|
|
Table 21.4 Immunoglobulin Classes (1 of 2) |
|
|
|
Classes of Antibodies |
• IgD – Monomer attached to surface of B cells – Functions as B cell receptor • IgG – Monomer; 75–85% of antibodies in plasma – From secondary and late primary responses – Crosses placental barrier |
|
|
Classes of Antibodies |
• IgE – Monomer active in some allergies and parasitic infections – Causes mast cells and basophils to release histamine • B cells can switch antibody classes but retain antigen specificity – IgM at first; then IgG – Almost all secondary responses are IgG |
|
|
Table 21.4 Immunoglobulin Classes (2 of 2) |

|
|
|
Antibody Targets and Functions |
• Antibodies inactivate and tag antigens; do not destroy them – Form antigen-antibody (immune) complexes • Defensive mechanisms used by antibodies – Neutralization and agglutination (the two most important) – Precipitation and complement fixation |
|
|
Neutralization |
• Simplest defensive mechanism • Antibodies block specific sites on viruses or bacterial exotoxins • Prevent these antigens from binding to receptors on tissue cells • Antigen-antibody complexes undergo phagocytosis |
|
|
Agglutination |
• Antibodies bind same determinant on more than one cell-bound antigen • Cross-linked antigen-antibody complexes agglutinate – Example: clumping of mismatched blood cells |
|
|
Precipitation |
• Soluble molecules are cross-linked • Complexes precipitate and are subject to phagocytosis |
|
|
Complement Fixation and Activation |
• Main antibody defense against cellular antigens (bacteria, mismatched RBCs) • Several antibodies bind close together on a cellular antigen à complement-binding sites on stem regions align – Triggers complement fixation into cell's surface – à Cell lysis |
|
|
Complement Fixation and Activation |
• Activated complement functions – Amplifies inflammatory response – Promotes phagocytosis via opsonization – à Positive feedback cycle that enlists more and more defensive elements |
|
|
Figure 21.15 Mechanisms of antibody action. |

|
|
|
Monoclonal Antibodies as Clinical and Research Tools |
• Commercially prepared pure antibody – Specific for single antigenic determinant • Produced by hybridomas – Cell hybrids: fusion of tumor cell and B cell • Proliferate indefinitely and have ability to produce single type of antibody • Used in research, clinical testing, and cancer treatment |
|
|
Summary of Antibody Actions |
• Antigen-antibody complexes do not destroy antigens; prepare them for destruction by innate defenses • Antibodies do not invade solid tissue unless lesion present • Can act intracellularly if attached to virus before it enters cell – Activate mechanisms that destroy virus |
|
|
Cellular Immune Response |
• T cells provide defense against intracellular antigens • Some T cells directly kill cells; others release chemicals that regulate immune response |
|
|
Cellular Immune Response |
• Two populations of T cells based on which glycoprotein surface receptors displayed – CD4 cells usually become helper T cells (TH); activate B cells, other T cells, macrophages, and direct adaptive immune response • Some become regulatory T cells – which moderate immune response – Can also become memory T cells |
|
|
Cellular Immune Response |
– CD8 cells become cytotoxic T cells (TC) • Destroy cells harboring foreign antigens • Also become memory T cells – Helper, cytotoxic, and regulatory T cells are activated T cells – Naive T cells simply termed CD4 or CD8 cells |
|
|
Figure 21.16 Major types of T cells. |

|
|
|
MHC Proteins and Antigen Presentation |
• T cells respond only to processed fragments of antigens displayed on surfaces of cells • Antigen presentation vital for activation of naive T cells and normal functioning of effector T cells |
|
|
MHC Proteins |
• Two types of MHC proteins important to T cell activation – Class I MHC proteins – displayed by all cells except RBCs – Class II MHC proteins – displayed by APCs (dendritic cells, macrophages, and B cells) • Both types are synthesized at ER and bind to peptide fragments |
|
|
Class I MHC Proteins |
• Bind with fragment of protein synthesized in the cell (endogenous antigen) • Endogenous antigen is self-antigen in normal cell; a nonself antigen in infected or abnormal cell • Crucial for CD8 cell activation • Inform cytotoxic T cells of microorganisms hiding in cells (cytotoxic T cells ignore displayed selfantigens) • Act as antigen holders; form "self" part that T cells recognize |
|
|
Class II MHC Proteins |
• Bind with fragments of exogenous antigens that have been engulfed and broken down in a phagolysosome • Recognized by helper T cells • Signal CD4 cells that help is required |
|
|
MHC Restriction |
• CD4 and CD8 cells have different requirements for MHC protein that presents antigens to them – CD4 cells that become TH – bind only class II MHC proteins typically on APC surfaces – CD8 cells that become cytotoxic T cells – bind only class I MHC proteins on APC surfaces • Once activated, cytotoxic T cells seek same antigen on class I MHC proteins on any cell |
|
|
MHC Restriction |
• CD8 cells activated by class I MHC proteins • How do APCs get endogenous antigens from another cell and display them on class I MHCs? – Dendritic cells engulf dying virus-infected or tumor cells, or import antigens via temporary gap junctions with infected cells—then display both class I and class II MHCs |
|
|
T cell Activation |
• T cell activation two-step process – Antigen binding – Co-stimulation • Both occur on surface of same APC • Both required for clonal selection |
|
|
T cell Activation: Antigen Binding |
• T cell antigen receptors (TCRs) bind to antigen- MHC complex on APC surface • TCR that recognizes the nonself-self complex linked to multiple intracellular signaling pathways • Other T cell surface proteins involved in T cell activation (e.g., CD4 and CD8 help maintain coupling during antigen recognition) |
|
|
T cell Activation: Co-stimulation |
• Requires T cell binding to other surface receptors on an APC – co-stimulatory signals – Dendritic cells and macrophages produce surface B7 proteins when innate defenses mobilized – B7 binding crucial co-stimulatory signal • Cytokines (interleukin 1 and 2 from APCs or T cells) trigger proliferation and differentiation of activated T cell |
|
|
T cell Activation: Co-stimulation |
• Without co-stimulation, anergy occurs – T cells • Become tolerant to that antigen • Are unable to divide • Do not secrete cytokines |
|
|
T cell Activation: Proliferation and Differentiation |
• T cells that are activated – Enlarge and proliferate in response to cytokines – Differentiate and perform functions according to their T cell class |
|
|
Figure 21.17 Clonal selection of T cells involves simultaneous recognition of self and nonself |

|
|
|
T cell Activation: Proliferation and Differentiation |
• Primary T cell response peaks within a week • T cell apoptosis occurs between days 7 and 30 – Benefit of apoptosis: activated T cells are a hazard – produce large amount inflammatory cytokines à hyperplasia, cancer • Effector activity wanes as amount of antigen declines • Memory T cells remain and mediate secondary responses |
|
|
Cytokines |
• Chemical messengers of immune system • Mediate cell development, differentiation, and responses in immune system • Include interferons and interleukins • Interleukin 1 (IL-1) released by macrophages co-stimulates bound T cells to – Release interleukin 2 (IL-2) – Synthesize more IL-2 receptors |
|
|
Cytokines |
• IL-2 key growth factor, acting on cells that release it and other T cells – Encourages activated T cells to divide rapidly • Other cytokines amplify and regulate innate and adaptive responses – E.g., tumor necrosis factor – cell toxin – E.g., gamma interferon – enhances killing power of macrophages |
|
|
Roles of Helper T (TH) cells |
• Play central role in adaptive immune response – Activate both humoral and cellular arms – Once primed by APC presentation of antigen, they • Help activate T and B cells • Induce T and B cell proliferation • Their cytokines recruit other immune cells • Without TH, there is no immune response |
|
|
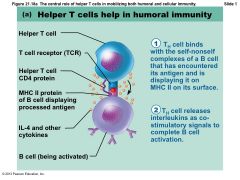
Helper T cells: Activation of B cells |
• Interact directly with B cells displaying antigen fragments bound to MHC II receptors • Stimulate B cells to divide more rapidly and begin antibody formation • B cells may be activated without TH cells by binding to T cell–independent antigens – Response weak and short-lived • Most antigens require TH co-stimulation to activate B cells: T cell–dependent antigens |
|
|
Figure 21.18a The central role of helper T cells in mobilizing both humoral and cellular immunity. |
|
|
|
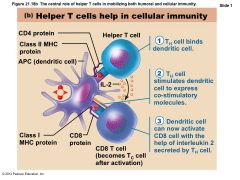
Helper T cells: Activation of CD8 cells |
• CD8 cells require TH cell activation into destructive cytotoxic T cells • Cause dendritic cells to express costimulatory molecules required for CD8 cell activation |
|
|
Figure 21.18b The central role of helper T cells in mobilizing both humoral and cellular immunity |
|
|
|
Helper T cells: Amplification of Innate Defenses |
• Amplify responses of innate immune system • Activate macrophages à more potent killers • Mobilize lymphocytes and macrophages and attract other types of WBCs |
|
|
Helper T cells: Subsets of TH cells |
• TH1 – mediate most aspects of cellular immunity • TH2 – defend against parasitic worms; mobilize eosinophils; promote allergies • TH17 – link adaptive and innate immunity by releasing IL-17; may play role in autoimmune disease |
|
|
Cytotoxic T (TC) cells |
• Directly attack and kill other cells • Activated TC cells circulate in blood and lymph and lymphoid organs in search of body cells displaying antigen they recognize |
|
|
Roles of Cytotoxic T (TC) cells |
• Targets – Virus-infected cells – Cells with intracellular bacteria or parasites – Cancer cells – Foreign cells (transfusions or transplants) |
|
|
Cytotoxic T cells |
• Bind to a self-nonself complex • Can destroy all infected or abnormal cells |
|
|
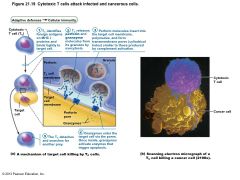
Cytotoxic T cells |
• Lethal hit – two methods: – TC cell releases perforins and granzymes by exocytosis • Perforins create pores through which granzymes enter target cell • Granzymes stimulate apoptosis – TC cell binds specific membrane receptor on target cell, and stimulates apoptosis |
|
|
Figure 21.19 Cytotoxic T cells attack infected and cancerous cells. |
|
|
|
Natural Killer cells |
• Recognize other signs of abnormality – Lack of class I MHC – Antibody coating target cell – Different surface markers of stressed cells • Use same key mechanisms as TC cells for killing their target cells • Immune surveillance—NK and TC cells prowl for markers they recognize |
|
|
Regulatory T (TReg) cells |
• Dampen immune response by direct contact or by inhibitory cytokines such as IL-10 and TGF-β • Important in preventing autoimmune reactions – Suppress self-reactive lymphocytes in periphery (outside lymphoid organs) – Research into using them to induce tolerance to transplanted tissue |
|
|
Figure 21.20 Simplified summary of the primary immune response |

|
|
|
Organ Transplants |
• Four varieties – Autografts: from one body site to another in same person – Isografts: between identical twins – Allografts: between individuals who are not identical twins – Xenografts: from another animal species |
|
|
Organ Transplants |
• Success depends on similarity of tissues – Autografts and isografts ideal donor tissues • Almost always successful if good blood supply and no infection – Research into successful xenografts from genetically engineered animals – Most common is allograft • ABO, other blood antigens, MHC antigens matched as closely as possible |
|
|
Prevention of Rejection |
• After surgery – Patient treated with immunosuppressive therapy • Corticosteroid drugs to suppress inflammation • Antiproliferative drugs • Immunosuppressant drugs • Many of these have severe side effects |
|
|
Immunosuppressive Therapy Problems |
• Patient's immune system suppressed – Cannot protect from foreign agents – Bacterial and viral infections à death – Must balance drugs for graft survival but no toxicity – Use antibiotics to control infections – Best circumstances – rejection after 10 years in 50% of patients |
|
|
Immunosuppressive Therapy Problems |
• Research to induce tolerance – Chimeric immune system • Suppress recipient's bone marrow • Douse recipient's bone marrow with bone marrow from donor of new organ • "Combined" immune system may treat transplanted organ as self – Harness regulatory T cell to suppress immune reactions |
|
|
Immunodeficiencies |
• Congenital or acquired conditions that impair function or production of immune cells or molecules such as complement or antibodies |
|
|
Congenital Immunodeficiencies |
• Severe Combined Immunodeficiency (SCID) Syndrome - genetic defect – Marked deficit in B and T cells – Defective adenosine deaminase (ADA) enzyme • Metabolites lethal to T cells accumulate – Fatal if untreated; treated with bone marrow transplants |
|
|
Hodgkin's Disease |
• Acquired immunodeficiency • Cancer of B cells • Leads to immunodeficiency by depressing lymph node cells |
|
|
Acquired Immune Deficiency Syndrome (AIDS) |
• Cripples immune system by interfering with activity of helper T cells • Characterized by severe weight loss, night sweats, and swollen lymph nodes • Opportunistic infections occur, including pneumocystis pneumonia and Kaposi's sarcoma |
|
|
Acquired Immune Deficiency Syndrome (AIDS) |
• Caused by human immunodeficiency virus (HIV) transmitted via body fluids—blood, semen, and vaginal secretions • HIV enters the body via – Blood transfusions; blood-contaminated needles; sexual intercourse and oral sex; mother to fetus • HIV – Destroys TH cells à depresses cellular immunity |
|
|
Acquired Immune Deficiency Syndrome (AIDS) |
• HIV multiplies in lymph nodes throughout asymptomatic period, ~10 years if untreated • Symptoms when immune system collapses • Virus also invades brain à dementia • HIV-coated glycoprotein complex attaches to CD4 receptor • HIV enters cell and uses reverse transcriptase to produce DNA from its viral RNA • The DNA copy (a provirus) directs host cell to make viral RNA and proteins, enabling virus to reproduce |
|
|
Acquired Immune Deficiency Syndrome (AIDS) |
• HIV reverse transcriptase à frequent errors; high mutation rate and resistance to drugs • Treatment with antiviral drugs – Fusion inhibitors block HIV's entry into cell – Integrase inhibitors block viral RNA integration into host's DNA – Reverse transcriptase and protease inhibitors inhibit viral replication enzymes – Antiretroviral vaginal gel reduces risk by 50% |
|
|
Autoimmune Diseases |
• Immune system loses ability to distinguish self from foreign • Production of autoantibodies and sensitized TC cells that destroy body tissues • Examples include multiple sclerosis, myasthenia gravis, Graves' disease, type 1 diabetes mellitus, systemic lupus erythematosus (SLE), glomerulonephritis, and rheumatoid arthritis |
|
|
Treatment of Autoimmune Diseases |
• Suppress entire immune system – Anti-inflammatory drugs, e.g., corticosteroids – Blocking cytokine action – Blocking co-stimulatory molecules • Research – Activating regulatory T cells; inducing selftolerance using vaccines; directing antibodies against self-reactive immune cells |
|
|
Mechanisms of Autoimmune Diseases |
• Weakly self-reactive lymphocytes may be activated by – Foreign antigens may resemble self-antigens • Antibodies against foreign antigen may cross-react with self-antigen – New self-antigens may appear, generated by • Gene mutations • Changes in self-antigens by hapten attachment or infectious damage • Release of novel self-antigens by trauma to barrier |
|
|
Hypersensitivities |
• Immune responses to perceived (otherwise harmless) threat cause tissue damage • Different types distinguished by – Their time course – Whether antibodies or T cells involved • Antibodies cause immediate and subacute hypersensitivities • T cells cause delayed hypersensitivity |
|
|
Immediate Hypersensitivity |
• Acute (type I) hypersensitivities (allergies) begin in seconds after contact with allergen • Initial contact is asymptomatic but sensitizes person • Reaction may be local or systemic |
|
|
Immediate Hypersensitivity |
• The mechanism involves IL-4 secreted by TH2 cells • IL-4 stimulates B cells to produce IgE • IgE binds to mast cells and basophils -> flood of histamine release and induced inflammatory response • Later encounter with same allergen à allergic reaction |
|
|
Immediate Hypersensitivities |
• Allergic reactions local or systemic – Local – mast cells of skin and respiratory and gastrointestinal mucosa – Histamines -> blood vessels dilated and leaky -> runny nose, hives, watery eyes • Asthma if allergen inhaled • Antihistamines to control – Systemic response is anaphylactic shock |
|
|
Anaphylactic Shock |
• Systemic response to allergen that directly enters blood and circulates rapidly • Basophils and mast cells enlisted throughout body • Systemic histamine release may cause – Constriction of bronchioles; tongue may swell – Sudden vasodilation and fluid loss from bloodstream may à – Circulatory collapse (hypotensive shock) and death • Treatment: epinephrine |
|
|
Subacute Hypersensitivities |
• Caused by IgM and IgG transferred via blood plasma or serum • Slow onset (1–3 hours) and long duration (10–15 hours) • Cytotoxic (type II) reactions – Antibodies bind to antigens on specific body cells, stimulate phagocytosis and complement-mediated lysis of cellular antigens – Example: mismatched blood transfusion reaction |
|
|
Subacute Hypersensitivities |
• Immune complex (type III) hypersensitivity – Antigens widely distributed in body or blood – Insoluble antigen-antibody complexes form – Complexes cannot be cleared from particular area of body – Intense inflammation, local cell lysis, and cell killing by neutrophils – Example: systemic lupus erythematosus (SLE) |
|
|
Delayed Hypersensitivities (Type IV) |
• Slow onset (one to three days) • Mechanism depends on helper T cells • Cytokine-activated macrophages and cytotoxic T cells cause damage • Example: allergic contact dermatitis (e.g., poison ivy) • Agents act as haptens • TB skin test depends on this reaction |
|
|
Developmental Aspects |
• Immune system stem cells develop in liver and spleen in weeks 1 - 9 • Bone marrow becomes primary source of stem cells later and through adult life • Lymphocyte development continues in bone marrow and thymus |
|
|
Developmental Aspects |
• TH2 lymphocytes predominate in newborn; TH1 system educated as person encounters antigens • Influences on immune system function – Nervous system – depression, emotional stress, and grief impair immune response – Diet – vitamin D required for activation of CD8 cells à TC cells • Vitamin D supplements reduced influenza; deficiency linked to multiple sclerosis |
|
|
Developmental Aspects |
• With age, immune system begins to wane – Greater susceptibility to immunodeficiency and autoimmune diseases – Greater incidence of cancer – Do not know why immune system fails but may be due to atrophy of thymus and decreased production of naive T and B cells |
|
|
What constitutes the body's first line of defense against disease? |
intact skin and mucous membranes
|
|
|
Treatment of an abscess often requires that it be surgically drained because ______. |
the wall of the abscess prevents neutrophils from entering the pus and attacking the pathogens
|
|
|
Which of the following is NOT a nonspecific internal defense against disease? |
T cells
|
|
|
Which defense mechanism results in redness, heat, pain, and swelling? |
inflammation
|
|
|
Which antimicrobial protein is produced by a virus-infected cell? |
interferon
|
|
|
Which of the following is (are) NOT a part of the innate immune defenses? |
T cells
|
|
|
Proinflammatory signals include all of the following, EXCEPT __________. |
antibodies
|
|
|
__________ is the final step of phagocyte mobilization. |
Chemotaxis |
|
|
Which of the following is a role of interferons (IFNs)? |
IFNs help the body combat viral infections.
Interferons (IFNs) are a group of proteins that have antiviral effects. IFNs activate macrophages and mobilize natural killer cells (NK cells) as well. They also have an anticancer role. |
|
|
Which of the following is an effect of complement activation? |
opsonization
Complement proteins stimulate inflammation, serve as opsonins to aid in the phagocytosis of targeted antigens, and facilitate cytolysis. |
|
|
Pyrogens induce __________. |
fever
A pyrogen will induce a fever. Pyro means "heat" and genic means "forming" or "creating." |
|
|
Fever is one of the cardinal signs of inflammation. |
False
|
|
|
With what does our immune system coat pathogens to facilitate their capture and accelerate phagocytosis?
|
opsonins |
|
|
Four (or five) cardinal signs indicate inflammation. What specific sign of inflammation is the result of exudate in the tissue spaces?
|
edema (swelling)
|
|
|
Which of the following inflammatory chemicals is released by mast cells?
|
histamine
|
|
|
Which of the following is NOT one of the cardinal signs of inflammation?
|
vasoconstriction
All inflammatory chemicals dilate, not constrict, local arterioles and make local capillaries leakier. Vasoconstriction is not one of the four (or five) cardinal signs of inflammation. |
|
|
When do neutrophils enter the blood from the red bone marrow, in response to leukocytosis-inducing factors?
|
leukocytosis
|
|
|
What is the main event of chemotaxis?
|
Neutrophils and other WBCs migrate up the gradient of chemotactic agents to the site of injury.
|
|
|
Neutrophils flatten and squeeze between the endothelial cells of the capillary walls during what process?
|
diapedesis |
|
|
What protein can be released by infected cells to help protect cells that have not yet been infected?
|
interferons (IFNs)
|
|
|
How do interferons protect against infection in healthy cells?
|
Interferons block viral reproduction in healthy cells through the production of antiviral proteins.
|
|
|
What is the specific target of interferons?
|
nearby healthy cells
|
|
|
What types of antigen are recognized by T cells? |
processed fragments of protein antigens displayed on surfaces of body cells
T cells can recognize and respond only to processed fragments of protein antigens displayed on the surfaces of body cells (APCs and others). Thus, T cells are best suited for cell-to-cell interactions. They target cells infected by viruses or bacteria, abnormal or cancerous cells, and cells of infused or transplanted foreign tissue. |
|
|
MHC I proteins (major histocompatibility class I proteins) are found on most cells of the body. |
True |
|
|
Which of the following statements does NOT describe the adaptive immune response? |
It occurs immediately after the body is challenged by foreign material. |
|
|
What mobilizes the adaptive defenses and provokes an immune response? |
antigens |
|
|
Which of the following cells engulf antigens and present fragments of them on their own surfaces, where they can be recognized by cells that will deal with them? |
dendritic cells |
|
|
T cells achieve self-tolerance in the __________. |
Thymus
T cells learn and are screened for self-tolerance in the thymus. |
|
|
Which cells mature in the thymus?
|
T cells |
|
|
How does a lymphocyte become immunocompetent?
|
Lymphocytes must be able to recognize their one specific antigen by binding to it.
|
|
|
What are B and T cells called that have not yet been exposed to an antigen?
|
naive
|
|
|
Binding of an eosinophil to an antibody-coated parasitic worm involves binding of the antibody's stem region to a(n) ______. |
plasma membrane protein on the eosinophil's surface |
|
|
Why are children given vaccinations? |
to develop antibodies against various diseases |
|
|
Choose the true statement regarding the primary versus the secondary immune response. |
A primary response results when naïve lymphocytes are activated, while a secondary response is a result of activating memory cells.
A primary immune response is initiated when naïve lymphocytes are exposed to foreign antigens. Since naïve cells are being stimulated, the response is slower to progress than a secondary response in which memory lymphocytes are activated. In addition to being slower than the secondary response, the primary response yields fewer antibodies than a secondary response. Furthermore, primary response antibodies do not bind to antigens as efficiently as the antibodies produced in a secondary response. Lastly, a secondary response tends to last longer than a primary response. |
|
|
__________ immunity protects a baby who is fed breast milk. |
Natural passive
Natural immunity is achieved through natural, non-manmade means. Natural passive immunity occurs when an individual gets antibodies from another source--they are not self-made. In the case of a nursing infant, the process is natural and the baby is protected by antibodies received from the mother. |
|
|
__________ is the most abundant class of antibodies in plasma. |
IgG
IgG is the most abundant class of antibodies in plasma. Additionally, IgG is the only class of antibodies that normally crosses the placenta to protect the baby in utero. |
|
|
__________ are lymphocytes that directly kill virus- infected cells. |
Cytotoxic T cells
Cytotoxic T cells are proficient at killing virus-infected cells. |
|
|
Antigens bound to MHC II activate __________. |
helper T cells
MHC II bound antigens activate helper T cells. |
|
|
Which of the following processes are unique to the respiratory system? |
pulmonary ventilation and external respiration
|
|
|
Which of the following represents all of the processes involved in respiration in the correct order? |
pulmonary ventilation; external respiration; transport of respiratory gases; internal respiration;
|
|
|
Quiet inspiration is __________, and quiet expiration is __________. |
an active process; a passive process
|
|
|
Patients with rhinitis often have "watery eyes" because ______. |
the infection has caused inflammation of the nasolacrimal ducts
The nasolacrimal ducts are a passageway between the lacrimal sac, which lies just medial to the lacrimal canaliculus, and the nasal cavity.
|
|
|
The adenoids normally destroy pathogens because they contain ______. |
lymphocytes
The adenoids (pharyngeal tonsils) are a ring of lymphatic tissue surrounding the entrance to the pharynx. They function to trap inhaled bacteria and facilitate activation of resident lymphocytes.
|
|
|
The tissue(s) and/or cells that may be affected during laryngitis ______. |
All of the listed responses are correct.
Using your textbook or other resource, review the histology of the larynx.
|
|
|
Smoking inhibits cilia by inhibiting the movements of ______. |
dynein molecules
Dynein is a motor protein that moves cilia causing them to bend. Collectively cilia propel other substances (like mucus) across the cell's surface.
|
|
|
Tracheal obstruction by a large piece of food typically involves obstruction of the ______. |
larynx
The larynx is superior to the trachea in the respiratory tract. The laryngeal opening (glottis) is sealed during swallowing by the epiglottis.
|
|
|
During pleurisy, the inflamed parietal pleura of one lung rubs against the inflamed ______. |
visceral pleura of the same lung
Normally the visceral and parietal pleura of one lung glide easily over one another during breathing because they are smooth and lubricated by pleural fluid. During pleurisy, they become rough and friction between the two pleura develops.
|
|
|
Which parts of the respiratory system function as the main sites of gas exchange? |
alveoli
|
|
|
Which of the following is NOT a function of the nasal conchae and mucosa? |
to destroy pathogens entering the nasopharynx
Curved conchae deflect air more than heavier nongaseous particles that hit mucus. Pathogens are trapped, but not necessarily destroyed by mucus. They must either be carried to the stomach for acidic destruction as the mucus is swallowed or dealt with by submucosal leukocytes, such as in tonsils and lymphoid follicles scattered throughout the submucosa.
|
|
|
Which of the following respiratory structures is more commonly known as the "throat"? |
pharynx
The funnel-shaped pharynx connects the nasal cavity and mouth superiorly to the larynx and esophagus inferiorly. Commonly called the throat, the pharynx vaguely resembles a short length of garden hose as it extends from about 13 cm (5 inches) from the base of the skull to the level of the sixth cervical vertebra.
|
|
|
Which of the following is NOT a function of the larynx? |
to assist in taste sensation
Taste receptors are present within the oral cavity and much less so in the pharynx, but do not extend to the larynx.
|
|
|
The __________ is also known as the "guardian of the airways." |
epiglottis
|
|
|
The smallest subdivisions of the lung visible with the naked eye are the __________, which appear to be connected by black carbon in smokers. |
lobules
|
|
|
Systemic venous blood that is to be oxygenated in the lungs is delivered by the __________, and the __________ provide oxygenated systemic blood to lung tissue. |
pulmonary arteries; bronchial arteries
|
|
|
The structures within the respiratory system's conducting zone include the trachea and the paranasal sinuses. |
True |
|
|
The alveoli are also known as alveolar sacs. |
False
|
|
|
Which of the following features characterizes the right lung?
|
presence of a superior, middle, and inferior lobe
|
|
|
Which blood vessels supply oxygenated systemic blood to the lung tissue?
|
bronchial arteries
|
|
|
The indentation on the medial surface of each lung through which pulmonary and systemic blood vessels, bronchi, lymphatic vessels, and nerves enter and leave is called the ___________.
|
hilum
|
|
|
In which region are the palatine tonsils found?
|
oropharynx
|
|
|
Which of the following is NOT a function of the nasal conchae?
|
routing air and food into proper channels
|
|
|
What part of the larynx covers the laryngeal inlet during swallowing to keep food out of the lower respiratory passages?
|
epiglottis |
|
|
During the Valsalva's maneuver, what part of the larynx closes to increase intra-abdominal pressure, such as to help with defecation?
|
glottis
|
|
|
Which cartilage belonging to the larynx anchors the vocal cords?
|
arytenoid cartilages
|
|
|
Which of the following is NOT a function of the larynx?
|
serving as part of the respiratory zone
|
|
|
Since mucus-producing cells and cilia are sparse in the bronchioles and alveoli, how does the body remove microorganisms that make their way into the respiratory zone?
|
alveolar macrophages crawl freely along internal alveolar surfaces
|
|
|
What type of epithelial tissue forms the walls of the alveoli?
|
simple squamous epithelium
|
|
|
Where does gas exchange occur in the respiratory system?
|
alveoli
|
|
|
In pneumothorax, the lung collapses because ______. |
intrapleural pressure is higher than intrapulmonary pressure
Intrapleural pressure (Ppul) is the gas pressure within the pleural cavity, while intrapulmonary pressure (Pip) is the gas pressure within the alveoli. Normally Ppul is less than Pip to maintain lung expansion. If Ppul exceeds Pip, then the lungs collapse.
|
|
|
Which of the following would NOT be involved in causing bronchiolar constriction during an asthma attack? |
adrenal medulla
The adrenal medulla is capable of releasing epinephrine into the bloodstream.
|
|
|
In babies born prematurely, pulmonary surfactant may not be present in adequate amounts ______. |
due to insufficient exocytosis in the type II alveolar cells
Type II alveolar cells make surfactant. Without surfactant, the surface tension created by the water vapor within the alveoli would cause them to collapse.
|
|
|
If the compliance of the thoracic wall is decreased, ______. |
the intrapleural pressure would not decrease normally during inhalation
As the size of the thoracic cavity increases, so does its volume. This causes intrapleural pressure to go below atmospheric pressure so that air (gases) can move into the lungs during inspiration. If the thoracic cavity cannot change its size (volume), then air movement will not occur.
|
|
|
What is the most immediate driving force behind pulmonary ventilation? |
intrapulmonary pressure change
|
|
|
Which of the following is NOT a physical factor that influences pulmonary ventilation? |
partial pressure of oxygen in the air
|
|
|
What is the amount of air that can be exhaled with the greatest possible exhalation after the deepest inhalation called? |
vital capacity
|
|
|
__________, the difference between the intrapulmonary and intrapleural pressures, prevents the lungs from collapsing. |
Transpulmonary pressure
|
|
|
Which form of CO2 transport accounts for the least amount of CO2 transported in blood? |
dissolved in plasma
|
|
|
Which of the following pressures rises and falls with the phases of breathing, but eventually equalizes with the atmospheric pressure?
|
intrapulmonary pressure
|
|
|
Which of the following pressures must remain negative to prevent lung collapse?
|
intrapleural pressure
|
|
|
Calculate the transpulmonary pressure if atmospheric pressure is 755 mm Hg.
|
4 mm Hg
|
|
|
Which of the following gives the relationship between the pressure and volume of a gas?
|
Boyle's law
|
|
|
Which of the following pressure relationships best illustrates when inspiration will occur?
|
Ppul < Patm
|
|
|
Which muscles are activated during normal quiet inspiration?
|
diaphragm and external intercostal muscles
|
|
|
What is the volume of the total amount of exchangeable air for a healthy, young adult male?
|
4800 ml
|
|
|
Which volumes are combined to provide the inspiratory capacity?
|
tidal volume (TV) + inspiratory reserve volume (IRV)
|
|
|
What is the tidal volume of an average adult male or female?
|
500 ml
|
|
|
Which of the following structures would be the LEAST vulnerable to damage caused by oxygen toxicity? |
costal cartilages
Cartilage is normally avascular and receives oxygen by diffusion from surrounding capillaries.
|
|
|
During pneumonia, the lungs become "waterlogged"; this means that within the alveoli there is an abnormal accumulation of ______. |
interstitial fluid
Pneumonia is an infection within the lung tissue often accompanied by inflammation. In response to inflammation, the increased permeability of the respiratory membrane results in increased formation of interstitial fluid that enters the alveoli.
|
|
|
Emphysema can result in an ______. |
All of the listed responses are correct.
-increased level of carbaminohemoglobin -increased level of deoxyhemoglobin -increased likelihood of the skin of Caucasians developing a slightly blue coloration |
|
|
What is ventilation-perfusion coupling? |
matching the amount of gas reaching the alveoli to the blood flow in pulmonary capillaries
|
|
|
Dalton's law of partial pressures states that the total pressure exerted by a mixture of gases is the sum of the pressures exerted independently by each gas in the mixture. |
True
|
|
|
Dalton's law of partial pressures states that when a gas is in contact with a liquid, that gas will dissolve in the liquid in proportion to its partial pressure. |
False
|
|
|
Hypoxia can be caused by ______. |
hyposecretion of erythropoietin
|
|
|
Which of the following is the primary factor in oxygen attachment to, or release from, hemoglobin? |
partial pressure of oxygen
|
|
|
What is the primary form in which carbon dioxide is carried in blood? |
as a bicarbonate ion in plasma
|
|
|
Oxygen is unloaded where it is most needed when blood pH drops, this is a phenomenon known as ___________.
|
the Bohr effect
|
|
|
What is the most common method of carbon dioxide transport?
|
as bicarbonate ions in the plasma
|
|
|
Which of the following qualifies as a fully saturated hemoglobin molecule?
|
hemoglobin is transporting four oxygen molecules |
|
|
Hypocapnia causes ______. |
hypoxia
Hypoxia occurs when to little oxygen is delivered to the tissues. Low carbon dioxide levels stimulate chemoreceptors in the brain and great vessels that signal the respiratory centers of the brain to slow down the respiratory rate. As rate falls, so does the rate of external respiration leading lower oxygen saturation.
|
|
|
What determines the respiratory rhythm in the body? |
medullary respiratory centers
|
|
|
What is the most powerful respiratory stimulant in a healthy person? |
arterial blood carbon dioxide level
|
|
|
Which of the following arterial blood levels is the most powerful respiratory stimulant? |
rising CO2 levels
|
|
|
Which of the following initiates inspiration?
|
ventral respiratory group (VRG)
|
|
|
Which of the following respiratory rates illustrates eupnea for an average, healthy adult at rest?
|
15 breaths per minute
|
|
|
Which of the following modifies and smoothes the respiratory pattern?
|
pontine respiratory centers
|
|
|
Which of the following stimuli is the most powerful respiratory stimulant to increase respiration?
|
rising carbon dioxide levels
|
|
|
Which of the following inhibits the respiration rate?
|
stimulation of stretch receptors in the lungs
|
|
|
Which of the following conditions or scenarios increases the respiratory rate?
|
acidosis
|
|
|
Which form of hypoxia reflects poor O2 delivery resulting from too few RBCs or from RBCs that contain abnormal or too little hemoglobin? |
anemic hypoxia
|
|
|
Emphysema is distinguished by permanent shrinkage of the alveoli. |
False
|
|
|
Although lung cancer is difficult to cure, it is highly preventable. |
True |
|
|
The normal CFTR protein is a membrane channel protein that controls chloride ion flow into and out of cells. The sweat of cystic fibrosis patients has an abnormally high concentration of salt (NaCl) because the presence of faulty CFTR proteins directly causes ______. |
reduced absorption of certain anions from sweat into the sweat duct cells
|
|
|
The functions of the nasal cavity include ________. |
warming, moistening, and filtering the air
|
|
|
The larynx ________. |
contains the apparatus for speech
|
|
|
The wall of the trachea is composed of several tissues. Which is unique to the trachea? |
cartilage rings
|
|
|
The pseudostratified ciliated columnar epithelium of the trachea ________. |
produces mucus to trap dust particles, bacteria, and other debris; sweeps the mucus toward the throat, where it can be expelled or swallowed; and lines the airway that is held open by C-shaped cartilaginous rings
|
|
|
Which lobes of the lungs are found in the apex? |
superior
|
|
|
The medial surface of the left lung has a cavity that accommodates the contents of the mediastinum. It is called the ________. |
cardiac notch
|
|
|
Trace the air flow through the respiratory system starting with the external nares.
|
1. external nares |
|
|
The function of the bronchial tree through the terminal bronchiole is ________; the function of the respiratory bronchiole and alveoli is ________. |
to move air, gas exchange
|
|
|
A respiratory bronchiole can be distinguished from a terminal bronchiole by ________. |
the alveoli that first appear on the respiratory bronchioles
|
|
|
The respiratory membrane includes the ________. |
capillary and alveolar walls and their fused basal laminae |
|
|
Select the pair below that is a correct match of the structure and zone. |
conducting zone, trachea
|
|
|
The inflated lungs of a fresh pluck ________. |
feel like a soft sponge |