![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
39 Cards in this Set
- Front
- Back
|
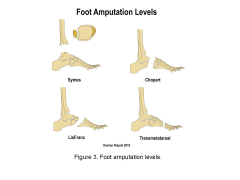
A 65-year-old diabetic male with forefoot gangrene is evaluated for possible amputation. When discussing the amputation levels with the patient, which of the following should be noted to require the greatest increase in energy expenditure for ambulation? 1. Syme amputation 2. Unilateral transtibial amputation 3. Transfemoral amputation 4. Bilateral transtibial amputations 5. Through the knee amputation |
A transfemoral level amputation requires the greatest increase in energy expenditure of the amputation levels given, and a Syme amputation the least. The authors found that that posterior tibial artery Doppler examination is predictive of healing in the Syme amputation performed on diabetics, and that furthermore, diabetics can attain a functional level of ambulation with a Syme amputation.ANS3 |
|

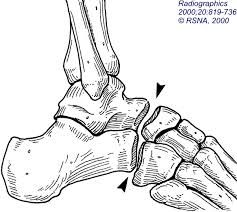
Figure A shows a below the knee amputation performed in a diabetic patient with significant vascular disease. Removal of the "dog ears", indicated by the red arrows, could cause direct damage to what vasculature leading to flap necrosis? 1. Anterior tibial artery 2. Saphenous and sural arteries 3. Posterior tibial artery 4. Peroneal artery 5. Lower popliteal artery |

"Dog ears" at the edge of a long posterior flap BKA incision are typically left intact because removal risks posterior flap blood supply. |
|
|
most common complication with chopart amputation most common technique to prevent it from recurring? |
equinus deformity to prevent do Achilles lengthening and transferred tibialis anterior tendon |
|
|
most common complication with Lisfranc amputation most common technique to prevent it from occurring? |
equina varus deformity prevented by keeping peroneus brevis tendon attached and it occurs because of unopposed pull posterior tibialis tendon and gastric soleus complex |
|
|
most important for success with a symes amputation and most important laboratory tests to ensure healing of the amputation? |
must have a stable heel pad and must have a patent posterior tibialis artery |
|
|
most common complication with an amputation pediatric patient and most common technique to prevent? |
overgrowth, knee disarticulation or cartilaginous cap to prevent overgrowth |
|
|
best predictor of wound healing after amputation? |
albumin level greater than 3.0 |
|
|
what are the minimal values necessary for wound parenting healing when comparing albumin, transient transcutaneous oxygen tension, total lymphocyte count, ABIs and toe pressures |
3.0/30//15/0.45 /40 |
|
|
what are the energy expenditure is when comparing amputations at different levels for example bilateral transfemoral amputations, transfemoral amputation, bilateral knee amputations, transtibial amputation, bilateral transtibial amputations, symes amputation |
bilateral transfemoral amputationequals 200 Bilateral knee disarticulation equals 120 Transfemoral amputation equals 70/100 Bilateral transtibial amputation equals 40 transtibial amputation 25/40 SYMES amputation equals 15
|
|
|
In addition to lengthening the Achilles, transfer of which tendon is most important for functional ambulation after performing a Chopart amputation of the foot? 1. peroneus brevis 2. peroneus longus 3. tibialis anterior 4. tibialis posterior 5. flexor hallucis longus |
The partial foot amputation through the talonavicular and calcaneocuboid joints is also known as the Chopart amputation. The Chopart amputation may result in significant equinovarus deformity with anterior weight bearing through the scar line, predisposing to skin breakdown over time. Therefore, lengthening of the Achilles tendon and transfer of the tibialis anterior to the talar neck should also be performed in conjunction with this disarticulation.ans3 |
|
|

|
|
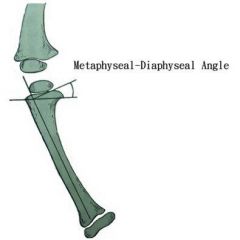
if pediatric patient 3 years of age presents to the office with metaphyseal diaphyseal angle of 16° what is the treatment and what is the classification |

a child less than 3 with stage I and 2 is treated with a brace K AFO |
|
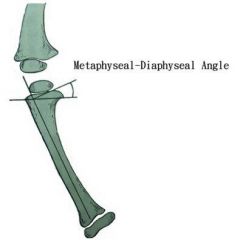
pediatric patient who is 4 years old presents to the office with an metaphyseal diaphyseal angle of 16° what is the treatment and what is the classification? |

a child greater than 3 years of age with a stage II or 1 is treated with proximal tibia fibula valgus osteotomy and overcorrection of 10-15° of valgus |
|
|
if a pediatric patient 3 years of age presents to the office withmetaphyseal diaphyseal angle of 20° was a treatment was a classification? |
the child is greater than 3 years of age with stage III or 5 the treatment is proximal tibia and fibula valgus osteotomy with correction 10-15° of valgus |
|

if a child 2 years of age presents with a congenital bar across the physis what is the treatment? |
excision of the bar and epiphysial lysis If the physeal bar is greater than 50% consider hemiepiphyseal lysis |
|
|
A valgus producing proximal tibial osteotomy with 10 degrees of overcorrection is the most appropriate treatment for which of the following patients with tibia vara? 1. A 4-year-old obese child with Blount's disease, Langenskiöld stage IV 2. An 18-month-old child with a proximal tibia metaphyseal-diaphyseal angle of 11 degrees 3. A 2-year-old obese child with Blount's disease, Langenskiöld stage II disease 4. A 5-year-old child with untreated renal osteodystrophy and a proximal tibia metaphyseal-diaphyseal angle of 16 degrees 5. A 8-year-old child with distal femoral varus a lateral distal femoral angle of 95 degrees |
children who are too old for bracing, morbidly obese, and have advanced Blount's disease (Langenskiöld stages IV, V, or VI) are candidates for proximal tibial osteotomy. Furthermore, it has been shown that overcorrection of the deformity can lead to decreased recurrence rates. Incorrect Answers: ans1 |
|
|
A 32-month-old male with severe infantile Blounts disease has been treated with full time bracing for the past year. At most recent follow-up, the varus deformity of his bilateral legs has worsened despite compliance with bracing. What treatment is now recommended? 1. Observation, discontinuation of bracing 2. Observation, continuation of full-time bracing 3. Bilateral proximal tibial osteotomies 4. Bilateral distal femur osteotomies 5. Bilateral proximal tibial medial hemiepiphysiodesis
|
The clinical scenario is consistent for a child with Infantile Blount’s disease who is < 3 year of age BUT has failed the first line of treatment which is bracing. At this time bilateral proximal tibial osteotomies is the most appropriate treatment. ncorrect Answers: |
|

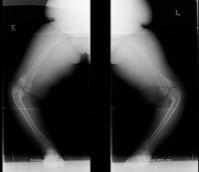
A 30-month-old boy has worsening bilateral bowleg deformities, and radiographs are shown in Figure A. The most appropriate initial management should consist of which of the following? 1. Observation 2. Full-time bracing with knee-ankle-foot orthoses 3. Night-time bracing with knee-ankle-foot orthoses 4. Proximal tibia/fibula valgus osteotomy with bar resection 5. Proximal tibia/fibula valgus osteotomy with hemiepiphysiodesis |
initial management of infantile Blount's disease in children less than 3 years old consists of full time bracing with a knee-ankle-foot orthosis. |
|
|
what kind of anesthesia leads to increased difficulty with fluoroscopic identification during pelvic and spinal procedures? |
nitrous oxide with increase gases abdominal distention |
|
|
what is the most common complication with interscalene regional block? |
sensorimotor neuropathy |
|
when an interscalene regional block is performed where is the brachial plexus found for injection? |
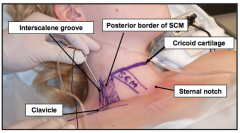
the groove between the anterior and middle scalene muscles at the level of the cricoid cartilage |
|
|
was difference between epidural anesthesia and spinal anesthesia? |
spinal anesthesia as a single injection and epidural anesthesia isan indwelling catheter |
|
|
|
|
|
what kind of anesthesia would be given for procedures around the medial aspect of the knee leg and ankle/ |
saphenous nerve block |
|
|
A surgeon recommends an interscalene regional block to a patient undergoing shoulder arthroscopy. When asked about potential complications, which of the following is most likely to occur? 1. Persistent motor neuropathy 2. Sensory neuropathy 3. Complex regional pain syndrome 4. Pneumothorax 5. Cardiac arrythmia and arrest |
Sensory neuropathy is the most common complication seen with interscalene regional block. |
|
|
regarding the SF 36 what is this outcome measurement tool used to compare and what is the differentiate? |
the SF 36 is used to compare the relative burden of disease and differentiate health benefits produced from different treatments |
|
|
in the SF 36 the burden of disease fracture 8 categories what are they?
|
|
|
|
the harris hip score is based on what 4 categories? |
|
|
|
one of the 5 categories for the following ankle outcome score and what clinical conditions are commonly used in patient's?
|
|
|
|
what is the constant shoulder outcomes score includes 4 variables ? |
|
|
|
UCLA shoulder score which consist of 5 pain, function, active forward flexion, strength of forward flexion, satisfaction of the patient what is a maximal score? |
maximal score 35" excellent results is score greater than 27 |
|
|
what is the Oswestry disability index used for? |
the patient's permanent functional disability and this considering the gold standard for lower back functional outcome tool |
|

A 45-year-old male trauma patient presents with multiple extremity injuries including the foot injury shown in Figure A. The foot fracture is treated surgically, and heals without any initial complications. At a minimum of 12 months, this patient will be expected to have which of the following scores compared to a matched polytrauma patient without a foot injury? 1. Lower mean Short Form 36 (SF-36) score 2. Higher mean score on the AAOS lower limb and foot and ankle outcomes questionnaire 3. Equivalent score on the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) 4. Lower Constant score 5. Higher score on the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)
|
Turchin et al assessed the outcome of two groups of matched polytrauma patients, with the only difference being the presence of a foot injury in Group 1. They used three outcome tools, SF-36, WOMAC, and Modified Boston Children's Hospital Grading System to evaluate the the two groups at a minimum of 2 years from injury. The foot injury group, including all types of foot fractures, had a poor outcome when using any of these measures. Turchin concludes that “Foot injuries cause significant disability to multiply injured patients. More attention should be given to these injuries, and more aggressive management should be considered to improve the outcome of this group of multiply injured patients.” ans1 |
|
|
what compressive neuropathy result in motor deficits only with no sensory changes? |
A AIN compressive neuropathy |
|
|
where is the most common cause of AIN compressive neuropathy at the elbow? |
the tenderness as of the deep head of the pronator teres |
|
|
the patient presents with bilateral weakness of grip and pinch, unable to make the capital okay sign, weakness with resisted pronation at the elbow maximally flexed
|
|
|
|
patient presents to the office note pain but has weakness of grip and pinch, unable to make the okay sign and weakness with pronation what is the diagnosis? |
the diagnosis AIN nerve palsy |
|

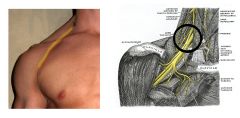
A 34-year-old seamstress was diagnosed with Parsonage-Turner brachial neuritis in the right upper extremity 1 month ago. She has weak forearm pronation with the elbow in the flexed position. She denies any current sensory changes. A clinical image of her hands attempting to make a clenched fist are shown in Figure A. Which of the following most likely represents her diagnosis and treatment? 1. Anterior interosseous nerve syndrome treated with observation 2. Posterior interosseous nerve syndrome with release of the Arcade of Frohse 3. Pronator syndrome with surgical release of the lacertus fibrosis 4. Anterior interosseous nerve syndrome with surgical release of Gantzer's muscle 5. Posterior interosseous nerve syndrome treated with observation
|
This patient presents with anterior interosseous nerve (AIN) syndrome and is often seen in conjunction with brachial neuritis (Parsonage-Turner Syndrome). ans1 |
|
|
what muscles are affected and found to be abnormal by EMG with AIN nerve palsy and how to test each of these muscles |
|