![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
28 Cards in this Set
- Front
- Back

|
Exanthematous Drug Eruptions - Pink maculesthat appear in a symmetric distribution on the trunk and upper extremities,progressively becoming confluent and sometimes slightly palpable Treatment: - Discontinue offending medication - Supportive Care: - Topical antipruritics, corticosteroids, bland emollients, oral antihistamines May persist up to 4 weeks after drug is D/C |
|

|
Urticaria (hives) - Transient erythematous, edematous pruritic papules and plaqueswith central pallor - Duration: 24 hours, if > 24 hrs think urticarial vasculitis Treatment - Withdrawal of causative agent - Antihistamines |
|

|
Urticaria (hives) - Transient erythematous, edematous pruritic papules and plaques with central pallor - Duration: 24 hours, if > 24 hrs think urticarial vasculitis Treatment: -Withdrawal of causative agent - Antihistamines |
|

|
Angioedema - Possible anaphylactic symptom Treatment - Immediate discontinuation of causative agent - Epinephrine - Possible hospitalization and system steroids |
|

|
Phototoxicity - Light + Drug = Cutaneous inflammation - Exaggeratedsunburn - Followed by hyperpigmentation Treatment - Discontinue medication, or dose it at bedtime - Decrease sun exposure or dosage of drug Medications that cause phototoxic Rxs - Tetracyclines- doxycycline, demeclocycline - NSAIDs- naproxen - Fluoroquinolones - Antiarrhythmics- amiodarone, quinidine - Diuretics: Furosemide, Thiazides - Psoralens - Phenothiazines - chlorpromazine - St. John's wort |
|

|
Phytophotodermatitis - Phototoxic reaction characterized by linearerythematous streaks occurring about 1 day after skin contact with plantscontaining furocoumarins and exposureto UVR: - Celery - Limes - Parsley - Figs |
|
|
Photoallergic Eruption Treatment - Drug withdrawal - Cool compress - Topical steroids - Broad spectrum Sunscreen - Sun Avoidance - Mild emollients - Mild analgesics Meds that cause photo allergic RXns - Sunscreens - Fragrances - Antimicrobial agents - NSAIDs - Antiarrhythmics - Antifungal - Antimalarial - Antimicrobials |
|
|
Meds that cause photoallergic RXns |
- Sunscreens - Fragrances - Antimicrobial agents - NSAIDs - Antiarrhythmics - Antifungal - Antimalarial - Antimicrobials |
|

|
Erythema Multiforme - skin-directed immune reaction that occurs in thesetting of infection in certain ‘predisposed’ patients (HSV, mycoplasma) - Target lesions most often onextremities (palms and soles) but may also be on trunk or face, or some mucosal involvement Treatment - Episodes usually last 2 weeks and heal without scarring - Topical: antiseptics for eroded skin - Systemic: Suppressive antiviral therapy (HSV), antihistamines, possibly corticosteroids - Prophylactic: Acyclovir or Valacyclovir |
|
|
Erythema Multiforme |
|

|
Erythema Multiforme |
|
|
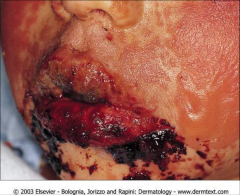
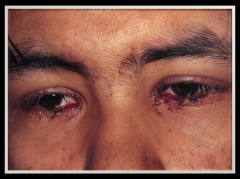
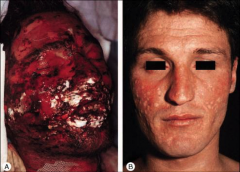
Stevens-JohnsonSyndrome Characteristics: - widespreadmucosal involvement in addition to areas of blistering and epidermal detachment(<10 %) - Positive Nikolsky Sign - Painful! - Occurs 7-21days after initiation of drug - Mortality = 1-5% Treatment: - D/C drug use - Supportive care in burn unit Complications - Fluid Loss, electrolyte imbalance, infections |
|

|
Stevens-JohnsonSyndrome |
|
|
Stevens-JohnsonSyndrome |
|

|
Stevens-Johnson Syndrome |
|

|
Stevens-Johnson Syndrome |
|

|
Stevens-Johnson Syndrome |
|
|
Medications that cause Stevens-Johnson Syndrome (SJS) |
- Allopurinol - NSAIDs - Antibiotics - Anticonvulsants |
|
|
Toxic Epidermal Necrolysis (TEN) - Similar to SJS but more widespread, > 30% BSA - Positive Nikolsky Sign - Mortality 25-35% Treatment - STOP THE OFFENDING MEDICATION - Supportive care in burn unit |
|

|
Toxic Epidermal Necrolysis |
|

|
Exfoliative Erythroderma - AKA Red Man syndrome - Diffuse erythema followed by desquamation Treatment: - Stop the medication - Antihistamines if itchy Drugs Associated with Erythroderma - Allopurinol - Beta-lactam antibiotics - Carbamazepine/oxcarbazepine - Gold - Phenobarbital - Phenytoins - Sulfasalazine - Sulfonamides - Zalcitabine |
|

|
Exfoliative Erythroderma |
|

|
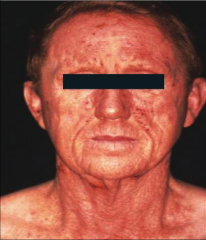
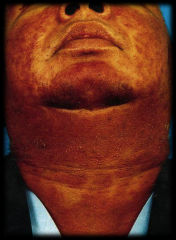
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS)
- Facial Edema is common and is a hallmark of DRESS - Most common visceral involvement is liver Treatment - Systemic Corticosteroids (LONG TAPER) - Withdrawal of offending drug (rash may persist months after withdrawal) |
|
|
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) |
|

|
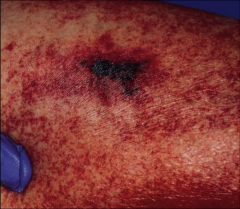
Fixed Drug Eruption - Solitary well-circumscribed erythematous, "dusky" merciless that evil into plaques or bullae - Most common on face, genitalia - Develop 1-2 weeks after first exposure - Areas may burn or itch - Eruption appears in the same spot each time the drug is taken. - Most commonly due: - Sulfonamides (in laxatives) - Antibiotics (tetracyclines) - NSAIDs - Barbiturates Treatment: - Stop the drug - Supportive care |
|
|
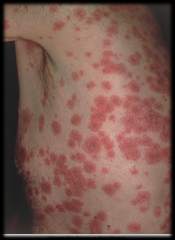
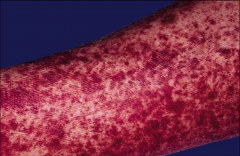
Vasculitis - Clinical: Palpable purpura - most oftenlower extremities - Complicationsinclude involvement of kidney, liver, GI tract, joints, and CNS - May be life threatening Treatment - Stop the drug |
|
|
Vasculitis - Clinical: Palpable purpura |
|

|
Vasculitis - Clinical: Palpable purpura |