Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
99 Cards in this Set
- Front
- Back
|
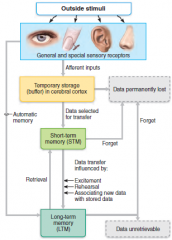
Functional Areas of the Cerebral Cortex
|
The three types of functional areas are:
Motor areas – control voluntary movement Primary (somatic) motor cortex Premotor cortex Broca’s area Frontal eye field Sensory areas – conscious awareness of sensation Primary somatosensory cortex Somatosensory association cortex Visual and auditory areas Olfactory, gustatory, and vestibular cortices Association areas – integrate diverse information Prefrontal cortex Language areas General (common) interpretation area Visceral association area |
|
|
Cerebral Cortex: Motor Areas
primary motor area |

Primary Motor Cortex
Located in the precentral gyrus Pyramidal cells whose axons make up the corticospinal tracts Allows conscious control of precise, skilled, voluntary movements |
|
|
Cerebral Cortex: Motor Areas
premotor cortex (planning) |

Premotor Cortex
Located anterior to the precentral gyrus Controls learned, repetitious, or patterned motor skills Coordinates simultaneous or sequential actions Involved in the planning of movements |
|
|
Cerebral Cortex: Motor Areas
Frontal eye field |

Frontal eye field
Located anterior to the premotor cortex and superior to Broca’s area Controls voluntary eye movement |
|
|
Prefrontal Cortex
|

Working memory for spatial tasks
Executive area for task management Working memory for object recall tasks solving complex, multitask problems Located in the anterior portion of the frontal lobe Involved with intellect, cognition, recall, and personality Necessary for judgment, reasoning, persistence, and conscience |
|
|
Language Areas
Cerebral Cortex: Association Areas |

Located in a large area surrounding the left (or language-dominant) lateral sulcus
Major parts and functions: Wernicke’s area –sounding out unfamiliar words Broca’s area – speech preparation and production Lateral prefrontal cortex – language comprehension and word analysis Lateral and ventral temporal lobe – coordinate auditory and visual aspects of language |
|
|
Cerebral Cortex: Motor Areas
broca's area |

Broca’s area
Located anterior to the inferior region of the premotor area Present in one hemisphere (usually the left) A motor speech area that directs muscles of the tongue Is active as one prepares to speak |
|
|
Visceral Association Area
|

Located in the cortex of the insula
Involved in conscious perception of visceral sensations Visceral - Pertaining to an internal organ of the body or the inner part of a structure. |
|
|
General (Common) Interpretation Area
Cerebral Cortex: Association Areas |

Ill-defined region including parts of the temporal, parietal, and occipital lobes
Found in one hemisphere, usually the left Integrates incoming signals into a single thought Involved in processing spatial relationships |
|
|
Cerebral Cortex: Sensory areas
Primary somatosensory cortex |

PrImary Somatosensory Cortex
Located in the postcentral gyrus, this area: Receives information from the skin and skeletal muscles Exhibits spatial discrimination |
|
|
Cerebral Cortex: Sensory area
somatosensory association cortex |
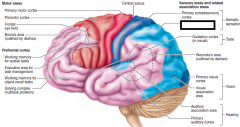
Somatosensory Association Cortex
Located posterior to the primary somatosensory cortex Integrates sensory information Forms comprehensive understanding of the stimulus Determines size, texture, and relationship of parts |
|
|
gustatory cortex
|

the gustatory cortex is the area that handles tastes. It is the brain structure that relays information about the type of taste in addition to information about a taste's intensity.
|
|
|
Wernicke's area
|

the region of the brain where SPOKEN language is understood
- Language Comprehension - Semantic Processing - Language Recognition - Language Interpretation |
|
|
primary visual cortex
|

Primary visual (striate) cortex
Seen on the extreme posterior tip of the occipital lobe Most of it is buried in the calcarine sulcus Receives visual information from the retinas |
|
|
visual association area
|
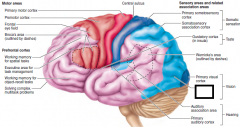
Surrounds the primary visual cortex
Interprets visual stimuli (e.g., color, form, and movement) |
|
|
auditory association area
|

Auditory association area
Located posterior to the primary auditory cortex Stores memories of sounds and permits perception of sounds Wernicke’s area |
|
|
primary auditory cortex
|

Primary auditory cortex
Located at the superior margin of the temporal lobe Receives information related to pitch, rhythm, and loudness |
|
|
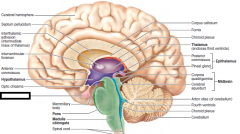
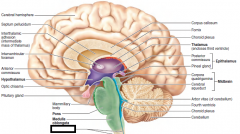
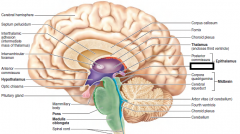
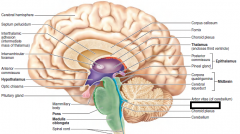
Hypothalamus
|
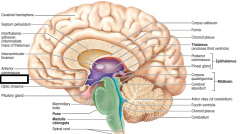
Hypothalamic Function
- Regulates blood pressure, - rate and force of heartbeat, - digestive tract motility, - rate and depth of breathing - other visceral activities - Perception of pleasure, fear, and rage - Maintains normal body temperature - Regulates feelings of hunger and satiety - Regulates sleep and the sleep cycle Endocrine Functions of the Hypothalamus - Releasing hormones control secretion of hormones by the anterior pituitary - The supraoptic and paraventricular nuclei produce ADH and oxytocin Mammillary bodies - Small, paired nuclei bulging anteriorly from the hypothalamus - Relay station for olfactory pathways Infundibulum – stalk of the hypothalamus; connects to the pituitary gland - Main visceral control center of the body |
|
|
optic chiasma
|
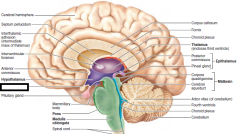
an X-shaped structure formed by the crossing of the optic nerves in the brain. The optic nerve connects the brain to the eye.
|
|
|
pituitary gland
|
controls hormones and helps turn food to energy.
|
|
|
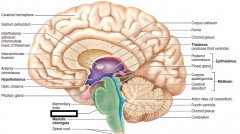
mammillary body
|
Mammillary bodies
Small, paired nuclei bulging anteriorly from the hypothalamus Relay station for olfactory pathways |
|
|
pons
|
Pons
Relay impulses between the motor cortex and the cerebellum Bulging brainstem region between the midbrain and the medulla oblongata Forms part of the anterior wall of the fourth ventricle Fibers of the pons: Connect higher brain centers and the spinal cord Origin of cranial nerves V (trigeminal), VI (abducens), and VII (facial) Contains nuclei of the reticular formation |
|
|
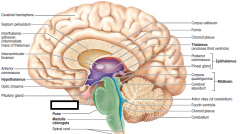
medulla oblongata
|
Most inferior part of the brain stem
Cranial nerves X, XI, and XII are associated with the medulla Vestibular nuclear complex – synapses that mediate and maintain equilibrium Ascending sensory tract nuclei, including nucleus cuneatus and nucleus gracilis Cardiovascular control center – adjusts force and rate of heart contraction Respiratory centers – control rate and depth of breathing Additional centers – regulate vomiting, hiccuping, swallowing, coughing, and sneezing |
|
|
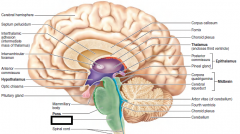
spinal cord
|
CNS tissue is enclosed within the vertebral column from the foramen magnum to L1
Provides two-way communication to and from the brain Protected by bone, meninges, and CSF Epidural space – space between the vertebrae and the dural sheath (dura mater) filled with fat and a network of veins |
|
|
**corpus callosum
|
Connects the left and right sides of the brain allowing communication between hemispheres. Transfers motor, sensory, and cognitive information between the brain hemispheres.
involved in several functions of the body including: - Communication Between Brain Hemispheres - Eye Movement - Maintaining the Balance of Arousal and Attention - Tactile Localization Commissural fibers connect corresponding gray areas of the two hemispheres. These commissures allow the two hemispheres to function as a coordinated whole. Females have a larger corpus callosum, and gender differences are seen in the language and auditory areas of the cerebral cortex |
|
|
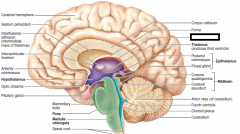
choroid plexus
|
Epithalamus
Most dorsal portion of the diencephalon; forms roof of the third ventricle Choroid Plexuses Clusters of capillaries that form tissue fluid filters, which hang from the roof of each ventricle Have ion pumps that allow them to alter ion concentrations of the CSF Help cleanse CSF by removing wastes Choroid plexus – a structure that secretes cerebral spinal fluid (CSF) |
|
|
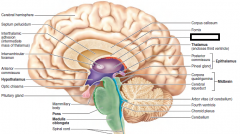
thalamus(encloses third ventricle)
|
Thalamic Function
controls sensory integration and motor integration. Receives sensory information and relays it to the cerebral cortex. The cerebral cortex also sends information to the thalamus which then transmits this information to other parts of the brain and the brain stem. -Sensual afferent impulses converge and synapse in the thalamus -Impulses of similar function are sorted out, edited, and relayed as a group -All inputs ascending to the cerebral cortex pass through the thalamus -Mediates sensation, motor activities, cortical arousal, learning, and memory |
|
|
pineal gland
|
Epithalamus
Most dorsal portion of the diencephalon; forms roof of the third ventricle Pineal gland – extends from the posterior border and secretes melatonin Melatonin – a hormone involved with sleep regulation, sleep-wake cycles, and mood |
|
|
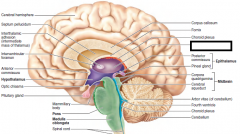
corpora quadrigemina
|
|
|
|
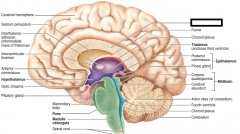
cerebral aqueduct
|
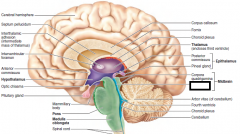
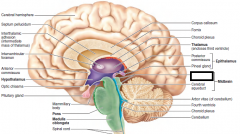
Midbrain structures include:
Cerebral aqueduct aka Mesencephalon – hollow tube that connects the third and fourth ventricles |
|
|
arbor vitae
|
Arbor vitae – distinctive treelike pattern of the cerebellar white matter
|
|
|
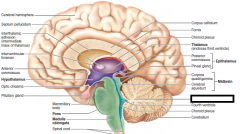
fourth ventricle
|
aka Metencephalon and myelencephalon
|
|
|
empty
|
|
|
|
cerebellum
|
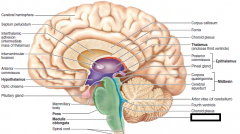
Cerebellar Cognitive Function
Plays a role in language and problem solving Recognizes and predicts sequences of events Provides precise timing and appropriate patterns of skeletal muscle contraction Cerebellar activity occurs subconsciously Cerebellar Processing Cerebellum receives impulses of the intent to initiate voluntary muscle contraction Proprioceptors and visual signals “inform” the cerebellum of the body’s condition Cerebellar cortex calculates the best way to perform a movement A “blueprint” of coordinated movement is sent to the cerebral motor cortex |
|
|
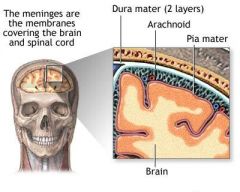
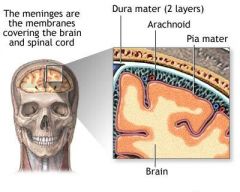
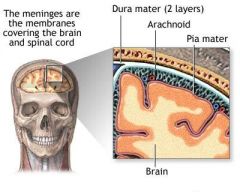
Meninges
|
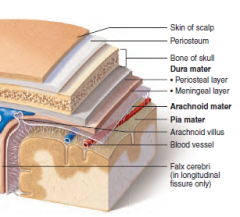
Three connective tissue membranes lie external to the CNS – dura mater, arachnoid mater, and pia mater
Functions of the meninges Cover and protect the CNS Protect blood vessels and enclose venous sinuses Contain cerebrospinal fluid (CSF) Form partitions within the skull |
|
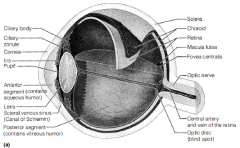
Function of parts of the eye?
|
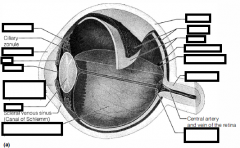
The sclera protects the eye and anchors extrinsic muscles
The cornea lets light enter the eye Vascular Tunic: - Choroid region - Supplies blood to all eye tunics - Ciliary Body - Anchors the suspensory ligament that holds the lens in place - Iris - colored part that Regulates the amount of light entering the eye --- Pupil – central opening of the iris changes due to light/mood. Sensory Tunic: Retina A delicate two-layered membrane Pigmented layer – the outer layer that absorbs light and prevents its scattering Neural layer, which contains: Photoreceptors that transduce light energy Bipolar cells and ganglion cells Amacrine and horizontal cells Ganglion cell axons: Run along the inner surface of the retina Leave the eye as the optic nerve The optic disc: Is the site where the optic nerve leaves the eye Lacks photoreceptors (the blind spot) Rods: Respond to dim light Are used for peripheral vision Cones: Respond to bright light Have high-acuity color vision Are found in the macula lutea Are concentrated in the fovea centralis vitreous humor in posterior(to lens) segment; Transmits light Supports the posterior surface of the lens Holds the neural retina firmly against the pigmented layer Contributes to intraocular pressure Aqueous humor A plasmalike fluid that fills the anterior(to lens) segment Drains via the canal of Schlemm Supports, nourishes, and removes wastes Lens A biconvex, transparent, flexible, avascular structure that Allows precise focusing of light onto the retina and Is composed of epithelium and lens fibers |
|
Where are different pitches processed?
|
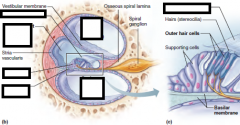
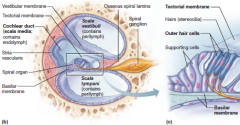
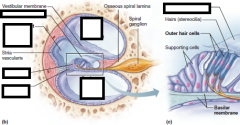
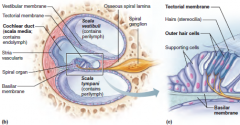
Basilar membrane
Pitch is perceived by: The primary auditory cortex Cochlear nuclei Loudness is perceived by: Varying thresholds of cochlear cells The number of cells stimulated |
|
What are the fluids of the inner ear?
|
|
|
Extrinsic eye muscle movement
|
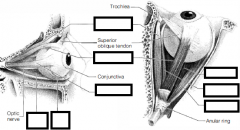
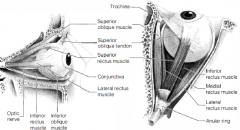
Lateral moves eye laterally,
Medial moves eye medially. Superior elevates , turns medially inferior depresses, turns medially Inferior oblique - Elevates eye and turns it laterally Superior oblique - Depresses eye and turns it laterally |
|

Receptors and structures for hearing?
Hearing, Static/dynamic eq.? |

MACULAE -equilibrium
Organ of Corti - hearing receptor The Vestibule(static equilibrium/gravity) Suspended in its perilymph are two sacs: the saccule and utricle The saccule extends into the cochlea The utricle extends into the semicircular canals These sacs: House equilibrium RECEPTORS called maculae Respond to gravity and changes in the position of the head The Semicircular Canals(Dynamic equilibrium/movement) Membranous semicircular ducts line each canal and communicate with the utricle The ampulla is the swollen end of each canal and it houses equilibrium RECEPTORS in a region called the crista ampullaris These receptors respond to angular movements of the head The Cochlea(hearing) Coils around a bony pillar called the modiolus Contains the cochlear duct, which ends at the cochlear apex Contains the organ of Corti (hearing receptor) |
|
|
Brain Stem
|
Brain Stem
Consists of three regions – midbrain, pons, and medulla oblongata Controls automatic behaviors necessary for survival such as: - heart rate - breathing - digesting foods - sleeping. It is the lowest, most primitive area of the human brain. |
|
|
Brain Lobes and function
|
The FRONTAL lobe associated with reasoning, motor skills, higher level cognition, and expressive language. At the back of the frontal lobe lies the motor cortex which utilizes information from other lobes to carry out body movements. Damage to the frontal lobe can lead to changes in sexual habits, socialization, and attention as well as increased risk-taking.
The PARIETAL lobe is associated with processing tactile sensory information such as pressure, touch, and pain. The somatosensory cortex is in this lobe and is essential to the processing of the body's senses. Damage to the parietal lobe can result in problems with verbal memory, an impaired ability to control eye gaze and problems with language. The TEMPORAL lobe isalso the location of the primary auditory cortex, which interprets sounds and the language. Contains the hippocampus which is associated with formation of memories. Damage to the temporal lobe can lead to problems with memory, speech perception, and language skills. The occipital lobe is associated with interpreting visual stimuli and information. The primary visual cortex, which receives and interprets information from the retinas. Damage to this lobe can cause visual problems such as difficulty recognizing objects, an inability to identify colors, and trouble recognizing words. |
|
|
Seratonin
|
Plays a role in sleep, appetite, nausea, migraine headaches, and regulating mood. Drugs that block
its uptake (Prozac) relieve anxiety and depression. Activity blocked by LSD and enhanced by ecstasy (MDMA). Mainly inhibitory Indirect action via second messengers Secreted by CNS: brain stem, especially midbrain; hypothalamus; limbic system; cerebellum; pineal gland; spinal cord |
|
|
Melatonin
|
a sleep-inducing signal and antioxidant; and,
along with hypothalamic nuclei, helps regulate the sleep-wake cycle. The epithalamus includes the pineal gland, which secretes the hormone melatonin. |
|
|
Dopamine
|
A “feel good” neurotransmitter. Release enhanced by l-dopa and amphetamines; reuptake blocked
by cocaine. Deficient in Parkinson’s disease; dopamine neurotransmission increases in schizophrenia. Excitatory or inhibitory depending on the receptor type Secreted by CNS: substantia nigra of midbrain; hypothalamus; the principal neurotransmitter of indirect motor pathways PNS: some sympathetic ganglia |
|
|
Epinephrine
|
A “feel good” neurotransmitter. Release enhanced by amphetamines; removal from synapse blocked
by tricyclic antidepressants [amitriptyline (Elavil) and others] and cocaine. Brain levels reduced by reserpine (an antihypertensive drug), leading to depression. Excitatory or inhibitory depending on receptor type Secreted by CNS: brain stem, particularly in the locus coeruleus of the midbrain; limbic system; some areas of cerebral cortex PNS: main neurotransmitter of postganglionic neurons in the sympathetic nervous system |
|
|
Parkinson’s disease
|
– degeneration of the dopamine-releasing neurons of the substantia nigra
|
|
|
Huntington's Disease
|
Mutant huntingtin protein accumulates in brain cells and the tissue dies, leading to massive degeneration of the basal nuclei and later of the cerebral cortex.
Usually treated with drugs that BLOCK, rather than enhance, dopamine’s effects. |
|
|
cerebrovascular accidents (stroke)
|
Experimental evidence indicates that glutamate, an excitatory neurotransmitter also involved in learning and memory, may be a culprit. Normally, glutamate binding to NMDA receptors opens NMDA channels that allow Ca to enter the stimulated neuron. After brain injury, neurons deprived
of oxygen begin to disintegrate, unleashing the cellular equivalent of “buckets” of glutamate. Under these conditions, glutamate acts as an excitotoxin, literally exciting surrounding cells to death. |
|
|
Dura Mater
|
Leathery, strong meninx composed of two fibrous connective tissue layers
The two layers separate in certain areas and form dural sinuses Dura Mater Three dural septa extend inward and limit excessive movement of the brain Falx cerebri – fold that dips into the longitudinal fissure Falx cerebelli – runs along the vermis of the cerebellum Tentorium cerebelli – horizontal dural fold extends into the transverse fissure |
|
|
Arachnoid Mater
|
The middle meninx, which forms a loose brain covering
It is separated from the dura mater by the subdural space Beneath the arachnoid is a wide subarachnoid space filled with CSF and large blood vessels Arachnoid villi protrude superiorly and permit CSF to be absorbed into venous blood |
|
|
Pia Mater
|
Pia Mater
Deep meninx composed of delicate connective tissue that clings tightly to the brain |
|
|
Cerebrospinal Fluid (CSF)
|
Watery solution similar in composition to blood plasma
Contains less protein and different ion concentrations than plasma Forms a liquid cushion that gives buoyancy to the CNS organs Prevents the brain from crushing under its own weight Protects the CNS from blows and other trauma Nourishes the brain and carries chemical signals throughout it |
|
|
Blood-Brain Barrier
|
Protective mechanism that helps maintain a stable environment for the brain
Bloodborne substances are separated from neurons by: Continuous endothelium of capillary walls Relatively thick basal lamina Bulbous feet of astrocytes Blood-Brain Barrier: Functions Selective barrier that allows nutrients to pass freely Is ineffective against substances that can diffuse through plasma membranes Absent in some areas (vomiting center and the hypothalamus), allowing these areas to monitor the chemical composition of the blood Stress increases the ability of chemicals to pass through the blood-brain barrier |
|
|
Concussion vs Contusion
|
A concussion is an alteration in brain function, usually temporary, following a blow to the head. The victim may be dizzy or lose consciousness. Although typically mild and short-lived, even a seemingly mild concussion can be damaging, and multiple concussions over time produce cumulative damage.
Contusion - More serious concussions can bruise the brain and cause permanent neurological damage. In cortical contusions, the individual may remain conscious. Severebrain stem contusions always cause coma, lasting from hours to a lifetime because of injury to the reticular activating system. |
|
|
Hemorrhage
subdural or subarachnoid |
bleeding from ruptured vessels into those spaces.
Individuals who are initially lucid and then deteriorate neurologically are hemorrhaging intracranially. - Blood accumulating in the skull increases intracranial pressure and compresses brain tissue. - If the pressure forces the brain stem inferiorly through the foramen magnum, control of blood pressure, heart rate, and respiration is lost. Intracranial hemorrhages are treated by surgically removing the hematoma |
|
|
Cerebral Edema
|
SWELLING OF THE BRAIN
Another consequence of traumatic head injury is. At best, cerebral edema aggravates the injury. At worst, it can be fatal in and of itself. |
|
|
What is a stroke?
Most common causes of CVAs? % that die? What happens to survivors |
Cerebrovascular Accidents (Strokes)
1. Caused when blood circulation to the brain is blocked and brain tissue dies 2. Most commonly caused by blockage of a cerebral artery(clot) Other causes include compression of the brain by hemorrhage or edema, and atherosclerosis 3. 15 percent die shortly after the stroke. 4. Survivors: - typically paralyzed on one side of the body. - Sensory deficits or difficulty understanding or vocalizing speech. - Some recover part of their lost faculties, because undamaged neurons sprout new branches that spread into the injured area and take over some lost functions. |
|
|
What does an EEG measure?
|
An electroencephalogram (EEG) records continuous electrical activity of brain function
|
|
|
Types of Brain Waves
|
- Alpha waves (8–13 Hz)– (awake but relaxed) regular and rhythmic, low-amplitude, slow, synchronous waves indicating an “idling” brain
- Beta waves(14–30 Hz) – (awake, alert) rhythmic, more irregular waves occurring during the awake and mentally alert state(concentrating) - Theta waves(4–7 Hz) – more irregular than alpha waves; common in children,uncommon in awake adults but may appear when concentrating. - Delta waves(4 Hz or less) – high-amplitude waves seen in deep sleep and when reticular activating system is damped. In awake adults, they indicate brain damage |
|
|
Low vs High amplitude
|
Alpha waves = low = awake/relaxed
Delta waves = high = sleep The amplitude of brain waves reflects the synchronous activity of many neurons and not the degree of electrical activity of individual neurons |
|
|
What changes brain waves?
|
- Change with age, sensory stimuli, brain disease, and the chemical state of the body
- EEGs used to diagnose and localize brain lesions, tumors, infarcts, infections, abscesses, and epileptic lesions - A flat EEG (no electrical activity) is clinical evidence of death |
|
|
Clinical consciousness
|
Clinical consciousness is defined on a continuum that grades levels of behavior:
(1) alertness, (2) drowsiness or lethargy (which proceeds to sleep), (3) stupor, and (4) coma -------------------------------------------------------------------- Encompasses perception of sensation, voluntary initiation and control of movement, and capabilities associated with higher mental processing Involves simultaneous activity of large areas of the cerebral cortex Is superimposed on other types of neural activity |
|
|
Conscious vs Unconscious
|
Conscious = aware
Unconscious = not aware Sleep is defined as a state of partial unconsciousness from which a person can be aroused by stimulation. |
|
|
What is fainting?
What is a coma? |
A brief loss of consciousness is called fainting or syncope. Most often, syncope indicates inadequate cerebral blood flow due to low blood pressure, as might follow hemorrhage or sudden emotional
stress. Significant unresponsiveness to sensory stimuli for an extended period is called coma. Coma is not deep sleep. During sleep, the brain remains active and oxygen consumption resembles that of the waking state. In coma patients, oxygen use is always below normal resting levels. Factors that can induce coma include: (1) blows to the head that cause widespread cerebral or brain stem trauma, (2) tumorsor infections that invade the brain stem, (3) metabolic disturbances such as hypoglycemia (abnormally low blood sugar levels), (4) drug overdose, (5) liver or kidney failure. |
|
|
Two major types of sleep?
|
NREM stages (first 30-45 min of sleep):
Stage 1 – eyes are closed and relaxation begins; the EEG shows alpha waves; one can be easily aroused Stage 2 – EEG pattern is irregular with sleep spindles (high-voltage wave bursts); arousal is more difficult Stage 3 – sleep deepens; theta and delta waves appear; vital signs decline; dreaming is common Stage 4 – EEG pattern is dominated by delta waves; skeletal muscles are relaxed; arousal is difficult Characteristics of REM sleep: - occurs after the fourth NREM stage has been achieved EEG pattern reverts through the NREM stages to the stage 1 pattern Vital signs increase Skeletal muscles (except ocular muscles) are inhibited Most dreaming takes place |
|
|
During sleep:
- When do you have nightmares? - Dreams? - When does the digestive system increase its functions? - Sleepwalking? |
1. Most nightmares and night terrors occur during NREM stages 3 and 4
2. Most dreaming occurs during REM sleep. 3.??????????????????????????? 4. NREM stage 4 |
|
|
In your life, how long do you spend sleeping?
Who spends the most time sleeping?(newborns, adults, elderly) |
1. 1/3???
2. Newborns(16hrs) Adults(7.5-8.5hrs) elderly(less) |
|
|
Why is sleep important?
|
Importance of Sleep
Slow-wave sleep is presumed to be the restorative stage Those deprived of REM sleep become moody and depressed "We dream to forget." REM sleep may be a reverse learning process where superfluous information is purged from the brain Daily sleep requirements decline with age |
|
|
What is Narcolepsy?
Insomnia? Sleep Apnea? |
Sleep Disorders
Narcolepsy – lapsing abruptly into sleep from the awake state Insomnia – chronic inability to obtain the amount or quality of sleep needed Sleep apnea – temporary cessation of breathing during sleep --------------------------------------------------------------------- Cells in the hypothalamus that secrete peptides called orexins (a wake-up chemical; also called hypocretins) are selectively destroyed in patients with narcolepsy. True insomnia often reflects normal age-related changes, but perhaps the most common cause is psychological disturbance. Obstructive sleep apnea occurs when loss of muscle tone during sleep allows excess fatty tissue or other structural abnormalities to block the upper airway. It is associated with obesity and made worse by alcohol and other depressants. |
|
|
What are the 2 types of memory?
|
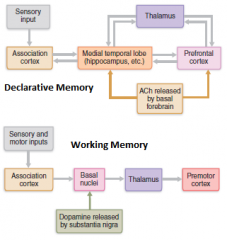
Fact (declarative) memory:
- Entails learning explicit information - Is related to our conscious thoughts and our language ability - Is stored with the context in which it was learned Skill Memory Skill memory is less conscious than fact memory and involves motor activity - It is acquired through practice - Skill memories do not retain the context in which they were learned --------------------------------------------------------------------- Fact memory involves the following brain areas: Hippocampus and the amygdala, both limbic system structures Specific areas of the thalamus and hypothalamus of the diencephalon Ventromedial prefrontal cortex and the basal forebrain Skill memory involves: Corpus striatum – mediates the automatic connections between a stimulus and a motor response Portion of the brain receiving the stimulus Premotor and motor cortex |
|
|
What affects memory acquisition?
(memory consolidation?) |
■ Emotional state. We learn best when we are alert, motivated, surprised, and aroused. Norepinephrine, a neurotransmitter involved in memory processing of emotionally charged events, is released when we are excited/stressed.
■ Rehearsal. Rehearsing or repeating the material enhances memory. ■ Association. Tying “new” information to “old” information already stored in LTM ■ Automatic memory. Not all impressions that become part of LTM are consciously formed. A student concentrating on a lecturer’s speech may record an automatic memory of the pattern of the lecturer’s tie. NMDA receptors (calcium channels), activated by depolarization and glutamate binding, play a major role in long-term potentiation (LTP). The calcium influx that follows NMDA receptor activation mobilizes enzymes that mediate events necessary for memory formation. Ach for declarative Dopamine for procedural |
|
|
3 ways PNS receptors are classified
|
1. STIMULUS TYPE:
Mechanoreceptors – respond to touch, pressure, vibration, stretch, and itch Thermoreceptors – sensitive to changes in temperature Photoreceptors – respond to light energy (e.g., retina) Chemoreceptors – respond to chemicals (e.g., smell, taste, changes in blood chemistry) Nociceptors – sensitive to pain-causing stimuli 2. LOCATION: Exteroceptors - Respond to stimuli arising outside the body - Found near the body surface - Sensitive to touch, pressure, pain, and temperature - Include the special sense organs Interoceptors - Respond to stimuli arising within the body - Found in internal viscera and blood vessels - Sensitive to chemical changes, stretch, and temperature changes Proprioceptors - Respond to degree of stretch of the organs they occupy - Found in skeletal muscles, tendons, joints, ligaments, and connective tissue coverings of bones and muscles - Constantly “advise” the brain of one’s movements Receptor Classification by Structural Complexity 3. STRUCTURE: Complex receptors are special sense organs Most receptors are simple and include: - encapsulated -- Meissner’s corpuscles (tactile corpuscles) -- Pacinian corpuscles (lamellated corpuscles) -- Muscle spindles, Golgi tendon organs, and Ruffini’s corpuscles -- Joint kinesthetic receptors - unencapsulated -- Free dendritic nerve endings: Respond chiefly to temperature and pain -- Merkel (tactile) discs -- Hair follicle receptorS |
|
|
Corpuscles, what STIMULI they pick up.
|
Structure receptors
Simple Receptors: Encapsulated Meissner’s corpuscles (tactile corpuscles) - L: Exteroceptors S: Mechanoreceptors (light pressure, discriminative touch, vibration of low frequency); rapidly adapting Pacinian corpuscles (lamellated corpuscles) L: Exteroceptors, interoceptors, and some proprioceptors S: Mechanoreceptors (deep pressure, stretch, vibration of high frequency); rapidly adapting Muscle spindles, Golgi tendon organs, and Ruffini’s corpuscles L: Exteroceptors and proprioceptors S: Mechanoreceptors (deep pressure and stretch); slowly or nonadapting Joint kinesthetic receptors L: Proprioceptors S: Mechanoreceptors and nociceptors |
|
|
Inborn vs learned reflex
|
Pain reflex vs driving instinct.
An inborn (intrinsic) reflex is a rapid, predictable motor response to a stimulus. It is unlearned, unpremeditated, and involuntary, and is built into our neural anatomy. a learned (acquired) reflex, results from practice or repetition. |
|
|
Purpose of stretching(stretch reflex?)
|
The stretch reflex makes sure that the muscle stays at that length
Operation of the Muscle Spindles Stretching the muscles activates the muscle spindle There is an increased rate of action potential in Ia fibers Contracting the muscle reduces tension on the muscle spindle There is a decreased rate of action potential on Ia fibers |
|
|
Most popular clinical reflex?
|
the patellar or knee-jerk reflex
a stretch reflex that helps keep your knees from buckling when you are standing upright. As your knees begin to buckle and the quadriceps lengthens, the stretch reflex causes the quadriceps to contract without your having to think about it. |
|
|
Parts of Reflex Arc?
Changes seen with aging? |

There are 5 components of a reflex arc
Receptor – site of stimulus Sensory neuron – transmits the afferent impulse to the CNS Integration center – either monosynaptic or polysynaptic region within the CNS Motor neuron – conducts efferent impulses from the integration center to an effector Effector – muscle fiber or gland that responds to the efferent impulse Reflexes slow with age. Physical changes in nerve fibers slow the speed of conduction. And the parts of the brain involved in motor control lose cells over time. |
|
|
Myopia
Hyperopia Presbyopia Astigmatism Cause? |
1. Nearsightedness - “short vision” occurs when distant objects focus in front of the retina, rather than on it. The eye is too LONG.
2. farsightedness,“far vision” occurs when the parallel light rays from distant objects focus behind the retina. The eye is too SHORT. 3. The lens is non accommodating, a condition known as presbyopia, literally “old person’s vision. 4. astigmatism "not a point" - Unequal curvatures in different parts of the cornea or lens leads to blurry images. Accommodation is the process that increases the refractory power of the lens. The ciliary muscles contract, pulling the ciliary body anteriorly toward the pupil and inward, releasing tension in the ciliary zonule. |
|
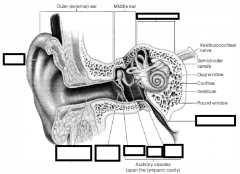
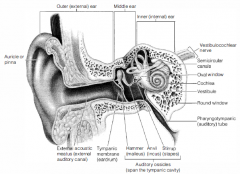
Parts of external, middle and inner ear?
|
|
|
|
Pathway of nerve fibers of eye
|
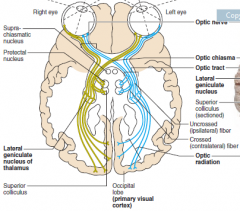
Visual Pathways
Axons of retinal ganglion cells form the optic nerve Medial fibers of the optic nerve decussate at the optic chiasm Most fibers of the optic tracts continue to the lateral geniculate body of the thalamus Other optic tract fibers end in superior colliculi (initiating visual reflexes) and pretectal nuclei (involved with pupillary reflexes) Optic radiations travel from the thalamus to the visual cortex Some nerve fibers send tracts to the midbrain ending in the superior colliculi A small subset of visual fibers contain melanopsin (circadian pigment) which: Mediates papillary light reflexes Sets daily biorhythms |
|
|
Pathway of sound
|
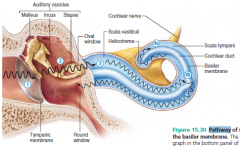
1 Sound waves vibrate the tympanic membrane.
2 Auditory ossicles vibrate. Pressure is ampli ed. 3 Pressure waves created by the stapes pushing on the oval window move through uid in the scala vestibuli. 4a Sounds with frequencies below hearing travel through the helicotrema and do not excite hair cells. 4b Sounds in the hearing range go through the cochlear duct, vibrating the basilar membrane and de ecting hairs on inner hair cells. |
|
|
Pathway of nerve fibers of ear
|
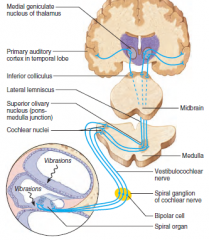
Auditory Pathway to the Brain
Impulses from the cochlea pass via the spiral ganglion to the cochlear nuclei From there, impulses are sent to the: Superior olivary nucleus Inferior colliculus (auditory reflex center) From there, impulses pass to the auditory cortex Auditory pathways decussate so that both cortices receive input from both ears |
|
|
Rhodospin
|
Rhodopsin is a biological pigment in photoreceptor cells of the retina that is responsible for the first events in the perception of light. Rhodopsins are extremely sensitive to light, enabling vision in low-light conditions.
Exposed to light, the pigment immediately photobleaches, and it takes about 45 minutes to regenerate fully in humans. |
|
|
Dark adaptation?
|
Adaptation
Adaptation to bright light (going from dark to light) involves: Dramatic decreases in retinal sensitivity – rod function is lost Switching from the rod to the cone system – visual acuity is gained Adaptation to dark is the reverse Cones stop functioning in low light Rhodopsin accumulates in the dark and retinal sensitivity is restored |
|
|
Where is sound processed?
|

Auditory Processing
Pitch is perceived by: The primary auditory cortex Cochlear nuclei Loudness is perceived by: Varying thresholds of cochlear cells The number of cells stimulated Localization is perceived by superior olivary nuclei that determine sound |
|
|
Where is vision processed
|

visual processing extends well forward into the temporal, parietal, and frontal lobes via two parallel streams:
■ The “what” processing stream extends through the ventral part of the temporal lobe ■ The “where” processing stream takes a dorsal path through the parietal cortex all the way to the postcentral gyrus and uses information from the primary visual cortex to assess the location of objects in space. Output from both these regions then passes to the frontal cortex, which uses that information to direct activities that, among other things, can guide movements such as reaching for a juicy peach. |
|
|
Balance and Orientation nerve Pathways
|
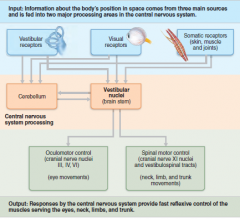
There are three modes of input for balance and orientation
Vestibular receptors Visual receptors Somatic receptors These receptors allow our body to respond reflexively |
|
|
What substances can we taste/smell?
|
Olfactory neurons are excited by volatile chemicals that bind to receptors in the olfactory cilia
Taste: - Umani - bitter, sweet etc. Their chemoreceptors respond to chemicals in aqueous solution Taste – to substances dissolved in saliva Smell – to substances dissolved in fluids of the nasal membranes |
|
|
Where on the tongue are tastes processed?
|
|
|
|
Night Blindness
Causes/symptoms? |
poor vision at night or in dimly lit environments. Although the term “night blindness” implies that you cannot see at night, this is not the case
nearsightedness: blurred vision when looking at faraway objects cataracts: a clouding of the eye’s lens retinitis pigmentosa: when dark pigment collects in your retina, creating tunnel vision Usher syndrome: a genetic condition that affects both hearing and vision |
|
|
Color Blindness
Causes/symptoms? |
the difficulty or inability to distinguish colors caused by problems with the color-sensing pigments in the eye. The majority of people who are colorblind cannot distinguish between red and green. Distinguishing yellows and blues may also be problematic. If you are completely colorblind (achromatopsia), you see only in gray or black and white.
|
|
|
Detached Retina
Causes/symptoms? |
Retinal detachment will cause a sudden defect in vision.
- darkness - In extremes, only a small hole of vision remains - If slight, a blind spot - floaters, little dark spots that float across the eye - flashes of light. serious eye disorder in which the retina separates from the underlying tissue layers. Scarring or shrinkage of the vitreous (substance comprising the insides of the eye) can pull the retina inward. Small tears in the retina allow liquid to seep behind the retina and push it forward. Injury to the eye can loosen the retina. Trauma is the most common cause of retinal detachment in children, although it is comparatively unusual in the adult population. Bleeding behind the retina, most often due to diabetic retinopathy or injury, can push it forward. Retinal detachment may be spontaneous. This occurs more often in the elderly or in very nearsighted (myopic) eyes. Cataract surgery causes retinal detachment 2% of the time. Myopia. Diabetes. Congenital factors (those that people are born with). Family history of retinal problems. High blood pressure. Stress. Tumors. |
|
|
Macula Degeneration
Causes/symptoms? |
the progressive deterioration of the macula, the light-sensitive cells of the central retina, at the back of the eye. As these macular cells malfunction and die, central vision becomes gray, hazy, or distorted, and eventually is lost. Peripheral (away from the center) vision is unaffected
|
|
|
Conduction Deafness
Causes/symptoms? |
hearing loss or impairment resulting from interference with the transmission of sound waves to the organ of Corti
|
|
|
Glaucoma
Causes/symptoms? |
Glaucoma is a condition that causes damage to your eye's optic nerve and gets worse over time. It's often associated with a buildup of pressure inside the eye
Less common causes of glaucoma include a blunt or chemical injury to the eye, severe eye infection, blockage of blood vessels in the eye, inflammatory conditions of the eye, and occasionally eye surgery to correct another condition. can cause blindness |
|
|
Otitis Media
Causes/symptoms? |
the middle ear (behind the eardrum) gets inflamed and fills with fluid
In older children and adults, symptoms include earache, hearing problems, fullness or pressure in the ear, fever, drainage from the ear, dizziness and loss of balance, and nausea or vomiting. Symptoms without pain or fever can also mean that there’s fluid in the ear and should be looked into. |
|
|
Menier's Syndrome
Causes/symptoms? |
a disorder of the inner ear
Recurring episodes of vertigo. and vomiting. Hearing loss. Ringing in the ear (tinnitus). Feeling of fullness in the ear Causes: Improper fluid drainage, perhaps because of a blockage or anatomic abnormality Abnormal immune response Allergies Viral infection Genetic predisposition Head trauma Migraines |
|
|
Neurosensory deafness
Causes/symptoms? |
Causes
Although sensorineural hearing loss is considered an idiopathic (no known cause) condition, researchers believe that other factors besides age (as in presbycusis), hereditary (as in hearing loss at birth and later in life) and environmental and physical factors (as in trauma-induced problems, tumors, noise damage and drug-induced hearing loss) may play a role in hearing loss. These factors include: Viral infections such as influenza, rubeola, rubella, mumps, herpes simplex and CMV. Vascular diseases such as leukemia and sickle cell anemia Autoimmune diseases such as lupus and temporal arteritis Symptoms In babies with congenital deafness, failure to respond to sounds In babies with congenital deafness, no baby babbling or other baby noises Sounds heard are quieter, distorted and less clear High tones are less audible The sounds "s", "f", and "z" are not heard Speech may be difficult to understand if there is background noise Tinnitus Vertigo (dizziness and loss of balance) |