![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
11 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
What is the difference between pancytopenia & aplastic anaemia? |
Pancytopenia is reduction of all three cell lines. Aplastic anaemia is Pancytopenia due to bone marrow hypoplasia. |
|
|
|
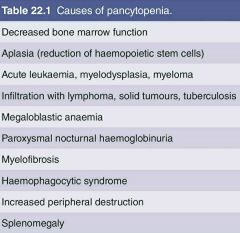
Causes for Pancytopenia |
|
|
|
|
Causes for Aplastic anaemia |
Primary- congenital fanconi & non-fanconi types Idiopathic acquired Secondary- Ionising radiation Chemicals Drugs Viruses ( Non-A, Non-B, non-C, non-G hepatitis, EBV ) Autoimmune disease eg-SLE Transfusion associated GVHD Thymoma ( more in red cell aplasia ) |
Primary & secondary |
|
|
Pathogenesis of Aplastic anaemia |
Reduction of haemopoietic pluripotential stem cells With Fault in remaining stem cells Or Immune process against remaining stem cells, Making them unable to proliferate and differentiate.. |
|
|
|
Congenital - Fanconi type inheritance |
Autosomal recessive 16 genes involved |
|
|
|
Fanconi anaemia features |
Growth retardation Skeletal defects ( absent radii/ thumbs, microcephaly ) Renal defects (pelvic / horse shoe kidney ) Skin ( areas of hyper / hypopigmentation ) Learning disability |
|
|
|
What is the most common type of Aplastic anaemia? |
Idiopathic acquired Aplastic anaemia 2/3 of all aplastic |
Thought to be autoimmune |
|
|
Criteria for aplastic anaemia |
1. Hg less than 10g/dl Macrocytic or normocytic normochromic 2.Neutrophils less than 1.5 x 10 9 3.Platelet count less than 50 x 10 9 At least 2 of above with, 4.no abnormal blood cells in peripheral blood film 5.marrow hypoplasia with around 75% fat infiltrate |
|
|
|
What is paroxysmal nocturnal haemoglobinuria |
* acquired x chromosome gene mutation * defects in phospatidylinositol glycan protein class A (PIG-A) *PIG-A necessary to make GPI anchor *GPI linked proteins absent in all cells from mutated stem cells Eg- CD 55 DAF decay activating factor CD 59 MIRL membrane inhibitor of reactive lysis * If above proteins absent, RBC are sensitive to lysis by complement *chronic intravascular haemolysis |
Pathogenesis |
|
|
What is the clinical triad in Paroxysmal nocturnal haemoglobinuria? |
*Chronic intravascular haemolysis *Venous thrombosis (recurrent thrombosis of large vessels eg- hepatic, mesenteric causing ab.pain , hepatic) *Bone marrow failure Other features *Haemosiderinuria -may worsen anaemia due to ion defficiency *haptoglobulins absent *free Hb -damage kidney -remove NO from smooth muscles causing dysphagia & pulmonary hypertension *arterial thrombosis eg-MI, CVA |
|
|
|
What is the classification of pure red cell aplasia? |

|
Acute, transient Chronic congenital Chronic acquired |