Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
54 Cards in this Set
- Front
- Back
|
What divides the airway into upper and lower regions?
|
Cricotracheal junction (from the trachea down is lower respiratory)
|
|
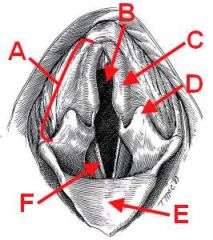
ID the following structures:
|
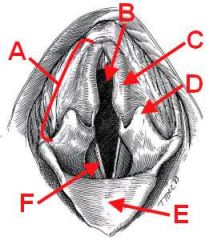
A - Arytenoid
B - Rima Glottis C - Corniculate process D - Cuneiform process E - Epiglottis F - Vocal fold |
|
|
What is the swollen area of the ventral nasal concha known as?
|
Alar fold
|
|
|
How should a NG tube be placed?
|
Initial dorsomedial then direct it ventral along the ventral nasal concha
|
|
|
What is one of the main points of resistance in the upper airway? What structures influence this point?
|
Rima Glottis (affected by motion of arytenoids via Cricoarytenoideus dorsalis)
|
|
|
Which nerve innervates most of the muscles of the larynx?
|
Recurrent laryngeal (Cricothyroideus is innervated by vagus)
|
|
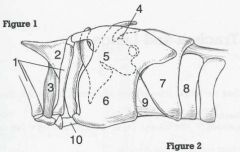
ID 4, 5, 6, and 7
|
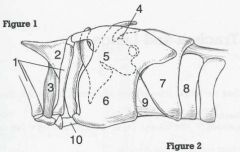
4 - Muscular process
5 - Arytenoid cartilage 6 - Thyroid cartilage 7 - Cricoid cartilage |
|
|
T or F:
Increased inspiratory effort or restrictive breathing = upper airway disease. |
False!
Increased inspiratory effort IS indicative of upper airway disease but restrictive breathing is LOWER airway disease. |
|
|
What are the 4 components of brachycephalic airway syndrome? How is each corrected?
|
Stenotic nares (wedge resection)
Elongated soft palate (Partial staphylectomy) Everted laryngeal saccules (sacculectomy) Hypoplastic trachea (maybe tracheostomy) |
|
|
Which parameter assesses ventilation?
|
PaCO2 (gold standard); also PvCO2 and expired CO2 work
|
|
|
A bulldog with stertor probably has...
|
...brachycephalic airway syndrome
|
|
|
What makes-up the primary palate? The secondary palate?
|
Lips + premaxilla (primary)
hard and soft palates (secondary) |
|
|
T or F:
Surgery of secondary palate defects should delayed until 8 weeks. |
True! Earlier surgery will lead to facial malformation.
|
|
|
What happens in the advanced form of brachycephalic airway syndrome?
|
Complete laryngeal collapse leading to cor pulmonale and R-CHF
|
|
|
What is the most common complication of cleft palate surgery?
|
dehisence
|
|
|
Surgery of the nasal passages and sinuses is always accompanied by...
|
..HEMORRHAGE
|
|
|
What does GOLPP stand for?
|
Geriatric
Onset Laryngeal Paralysis Polyneuropathy |
|
|
Congenital laryngeal paralysis is common in which breeds?
|
Bouviers, Bull Terriers, Rotties, Dalmations, Huskies
|
|
|
What is a common signalment for GOLPP? What are common clinical findings?
|
9yo golden, lab, st. bernard, irish setter
Findings include raspy breathing, hypothyroid |
|
|
Describe paradoxical arytenoid motion.
|
Paralyzed arytenoids move IN on inspiration (should move out normally)
|
|
|
T or F:
Emergency tracheostomy is common in a lar-par emergency! |
False!
Sedate (Ace/Torb), give O2, and cool them down! |
|
|
How is lar-par treated surgically? What is a common complication? What is the prognosis?
|
Tx - unilateral arytenoid lateralization;
30% aspiration pneumonia; 80% do well (pretty good prognosis) |
|
|
Where does the trachealis muscle attach in dogs?
|
On the external surface
|
|
|
What runs alongside (lateral to) the trachea?
|
Carotid sheath (vagosympathetic trunk, internal jugular, carotid, lymphatics); recurrent laryngeal too
|
|
|
What are the types of pneumocytes in the lungs? What is the function of each? Which is most abundant?
|
Type I pneumocytes (most abundant; line alveoli)
Type II pneumocytes (produce surfactant) |
|
|
Where can the pleural cavity be entered without danger of penetrating the lungs?
|
Costodiaphragmatic and costmediastinal recesses
|
|
|
Which muscles can be engaged if the diaphragm fails?
|
External intercostal
Sternocleidomasoid Serratus ventralis Scalenus |
|
|
Which muscles aid in expiration?
|
Transversus thoracis
Internal intercostal Rectus abdominus |
|
|
Where is most resistance during inspiration?
a) nasal b) laryngeal c) small airway |
a) nasal
|
|
|
Where is most resistance during expiration?
a) nasal b) laryngeal c) small airway |
a) nasal
|
|
|
Under what conditions does hemoglobin bind oxygen more?
|
Increased pH
Decreased temperature Decreased DPG Decreased PCO2 |
|
|
Under what conditions does hemoglobin release oxygen more readily?
|
Decreased pH
Increased temperature Increased DPG Increased PCO2 |
|
|
Where is respiration controlled?
|
Medulla
|
|
|
What obstructive respiratory conditions are common in dogs?
|
Stenotic nares
Nasal tumors foreign bodies |
|
|
What obstructive respiratory conditions are common in cats?
|
Rhinitis and sinusitis
|
|
|
Rapid shallow breaths can be evidence of:
a) decreased lung compliance b) obstructive conditions c) pneumothorax d) stenotic nares |
a) decreased lung compliance
c) pneumothorax |
|
|
Anything affecting the pleural cavity or pleural space is considered a _____________ disorder.
|
restrictive
|
|
|
When performing a thoracocentesis, you feel a "scratching" sensation at the end of your needle. What are your next steps?
|
Stop and withdraw a mm or two...that was just the lungs you were on!
|
|
|
What do you do with fluid withdrawn in a thoracocentesis?
|
Measure volume, perform cytology, maybe PCV, total solids, culture
|
|
|
What is the next step on an animal that has persistent pleural effusion?
|
Thoracostomy tube
|
|
|
What is the common signalment for tracheobronchomalacia?
|
Small breed dog with a honking cough
|
|
|
What are some possible complications to surgical tracheal collapse treatment?
|
Tracheal devasculariztaion
Laryngeal paralysis Breakage at thoracic inlet (stent) Inhibition of mucociliary clearance (stent) |
|
|
What are two methods for surgically treating tracheal collapse? What is the prognosis?
|
Stent and cervical support rings:
70% success rate |
|
|
When performing a tracheaostomy, how wide should the horizontal slit be made?
|
no more than 50% of tracheal circumference (more like 30%)
|
|
|
What vein should be noted when performing a tracheostomy?
|
Cranial thyroid vein
|
|
|
What is the signalment for most tracheal tears?
|
Cats, post dental procedure (ET tube trauma)
|
|
|
What are the 2 types of lobectomy?
|
Partial or complete
|
|
|
How much lung can be removed without major complications?
|
Up to 50%
|
|
|
T or F:
The left lung comprises over 50% of overall lung tissue. |
False! This describes the RIGHT lung
|
|
|
Which two dogs typically get lung lobe torsion and which lobe?
|
Narrow, deep-chested dogs (right middle)
Pugs (left cranial) |
|
|
When should a torsed lung lobe be untorsed?
|
NEVER! perform a lobectomy to avoid reperfusion injuries!
|
|
|
What are indications for lobectomy?
|
Neoplasia
Infections Lung lobe torsion |
|
|
What are post lobectomy compensation factors?
|
1) recruitment of existing physiological reserves of diffusing capacity
2) remodeling of alveolar-capillary network 3) new or regenerative alveolar-capillary growth |
|
|
Performing a thoracocentesis on a dog with lung lobe torsion should reveal...
|
...serosanguinous or chylous fluid
|