Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
104 Cards in this Set
- Front
- Back
|
What is Kirby's rule of 20?
|
a list of 20 parameters to evaluate daily in the critically ill animal.
|
|
|
What are the 4 As of fracture repair?
|
Alignment
Apposition Apparatus Activity |
|
|
In fracture scoring, which is worse - low numbers or high numbers? What is the scale?
|
0-3 = low = BAD
8-10 = high = GOOD |
|
|
Low fracture scores are given to...
|
...older dogs with non-reducible fractures and extensive soft tissue damage.
|
|
|
High fracture scores are given to...
|
...young dogs with good fracture load sharing.
|
|
|
What are issues with epiphyseal fracture healing?
|
cartilage does not heal
|
|
|
What are issues with metaphyseal fracture healing?
|
Not really any - good blood supply and softer bone.
|
|
|
What are issues with diaphyseal fracture healing?
|
Limited blood supply and very hard bone
|
|
|
Strain greater than what value inhibits bone healing?
|
>2% strain inhibits bone healing
|
|
|
T or F:
With a properly apposed fracture under compression, there is no bone resorption at the fracture line. |
True!
|
|
|
What are the advantages of compression in fracture repair?
|
increases interfragmentary friction
neutralizes micromotion |
|
|
What are the two types of primary bone healing? How are they different?
|
Contact healing (gap <0.01mm, simultaneous healing and remodeling)
Gap healing (gap <1mm; gap fills with intramembranous bone then remodeled) |
|
|
In secondary bone healing, how much strain do the following tissues tolerate?
Lamellar bone Membranous bone Fibrocartilage Granulation tissue |
Lamellar bone (2%)
Membranous bone (5%) Fibrocartilage (10%) Granulation tissue (100%) |
|
|
What is the reaction of bone to movement?
|
bone resorption
|
|
|
What are the AO principles of fracture stabilization?
|
1) Fracture reduction/fixation to restore normal anatomy
2) Stability/fixation as the fracture requires 3) preserve blood supply & gentle tissue handling 4) early and safe mobilization of the part and patient |
|
|
Which implants counteract bending or angular forces?
|
Plates
IM Pins Interlocking nails External fixation External copation |
|
|
Which implants counteract rotational forces?
|
Wires
Ex fix Plate and screw External copation |
|
|
Which implants counteract shearing or compressive forces?
|
Wires
Ex fix Plate and screw Interlocking nail |
|
|
Force on body protuberances are known as...
|
...distractions
|
|
|
What are some indications for open reduction?
|
Articular fracture
Simple displaced fractures Comminuted fractures (treated by segment alignment and allografts) |
|
|
What are indications for closed fixation?
|
Nondisplaced or incomplete fractures
|
|
|
Which of the following is NOT a method of open fracture reduction?
a) tent pegging b) hanging leg traction c) instrument leverage d) pointed reduction forceps e) cornholing |
b) hanging leg traction
e) cornholing |
|
|
What are the basic biomechanical principles that must be addressed in rigid fracture fixation? How many must be fulfilled?
|
Interfragmentary compression
Rigid bone splinting (fulfill at least 1) |
|
|
What are the two NEVERS associated with IM pin use?
|
NEVER use IM pins alone!
NEVER use an IM pin on the radius |
|
|
What are the two types of threaded Steinman pins? Which type is better?
|
Negative profile (worse, prone to breakage)
Positive profile |
|
|
How should a femoral head capital physeal fracture be fixed?
|
Use 2-3 unthreaded Steinman pins, allowing fixation but continued growth
|
|
|
What is a big fat NEVER DO THIS when fixing a fracture with pins?
|
NEVER have pins cross at the fracture site
|
|
|
An IM pin should fill ___________ % of the medullary canal diameter.
|
60-70%
|
|
|
What is the ONLY manner in which to pin the tibia?
|
Normograde pinning
|
|
|
What is the weakest point of cerclage wire?
|
the knot
|
|
|
What are the cerclage wire application rules?
|
Place wire 0.5cm from fracture ends.
Place 1cm or a full bone diameter between wires. Place wire perpendicular to bone long axis Do NOT put wire in a fracture! |
|
|
What are two ways to hold cerclage in place in conical bone?
|
Notch the bone
Wrap around a place Kirchner wire |
|
|
What are some rules for twisting cerclage wire?
|
Pull and twist simultaneously
Equal tension on each loop arm Do not bend down after twisting (can bend down while twisting) Leave 3 wire wraps |
|
|
T or F:
Cerclage should not be used in oblique fractures >2x the bone width. |
False!
This is when you use cerclage (with an IM pin, of course) |
|
|
When is the pin and tension band technique of fixation used?
|
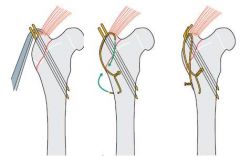
With tuberosity/tendon and ligament attachment avulsion fractures.
|
|
|
What are the 3 types of external fixators?
|
Linear
Free-form Ring or Illizarov |
|
|
What type of cerclage wire knot has the best strength?
|
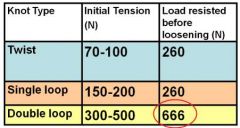
Double loop!!!
It's the devil knot... |
|
|
What are the types of linear ex-fixes? Which is weakest? Strongest?
|
Type 1a (uniplanar - weakest)
Type 1b (multiplanar) Type 2 (uniplanar) Type 3 (multiplanar - strongest) |
|
|
The further away an implant is from a bone...
a) the higher the shear modulus b) the lower the shear modulus c) the higher the bending moment d) the lower the bending moment |
c) the higher the bending moment
|
|
|
When placing an ex fix, what is the greatest number of pins that should be placed in a bone segment?
|
no more than 4
|
|
|
When placing an ex fix, how close can the pins be placed to the fracture ends? The joint?
|
1/2 in (1cm) from each
|
|
|
T or F:
Pins should be placed through both cortices and be no larger than 20-30% of the bone diameter. |
True!
|
|
|
For pin insertion with ex fix you should use...
a) Jacob's Chuck b) Power drill c) Both are appropriate |
b) Power drill
|
|
|
How far should the connecting bar be from the skin?
|
1cm
|
|
|
Where are safe tissue corridors in the humerus?
|
Across the humeral condyles
Proximal-lateral aspect |
|
|
Where on the femur is safe for tissue corridors?
|
Only the lateral femur
|
|
|
Where are safe tissue corridors for the radius for ex fix?
|
Distal 2/3 of the medial aspect.
|
|
|
T or F:
The cranial aspect of the tibia is the only safe route for an ex fix. |
False!
Cranial and medial are both safe! |
|
|
What are important post-op considerations after placing external fixators?
|
Pain meds!
Clean limb/pin sites w/antisceptic and triple abx Expect swelling; add padding under bar Bandage limb cage rest! |
|
|
Choose the correct type of bone screw...
...greater pullout strength. |
cancellous
|
|
|
Choose the correct type of bone screw...
...deep pitch and threads. |
cancellous
|
|
|
Choose the correct type of bone screw...
...greater bending strength. |
cortical
|
|
|
Choose the correct type of bone screw...
...shallow threads and pitch. |
cortical
|
|
|
Screws MUST NOT be greater than ______% of bone diameter.
|
40%
|
|
|
Screws MUST NOT be placed any closer than _____ times the screws width from the fracture edge.
|
2x
|
|
|
Which of the following describe how should a lag screw be placed?
a) perpendicular to bone cortex b) parallel to fracture line c) through both cortices d) perpendicular to the fracture line |
c) through both cortices
d) perpendicular to the fracture line |
|
|
Screws should not be placed in loaded position with which type of fracture?
|
Oblique
|
|
|
Removing part of the fixator to increase weight bearing is known as...
|
...dynamization
|
|
|
What are the 3 goals of plate and screw fixation?
|
anatomical reduction
blood supply preservation stable internal fixation |
|
|
What are the 4 functions of plates (or, the four manners in which they can be placed)? In which ones does the plate take the entire weight bearing load?
|
Neutral
Bridging (wt bearing) Buttressing (weight bearing) Compressing |
|
|
What are the rules to plate placement?
|
Contour plate to bone surface
Screws engage near and far cortex AT LEAST 2 screws on either side of the fracture |
|
|
Which side of the bone is the plate placed on and why?
|
The tension band; this is because steel has more tensile strength than bone
|
|
|
Where should plates be placed on the humerus? The femur?
|
Humerus (cranial/lateral proximally and caudal/medial distal)
Femur (cranial and lateral) |
|
|
Where should plates be placed on the tibia? The radius?
|
Tibia (medial)
Radius (cranial and medial) |
|
|
Which plate type improves blood flow?
|
Limited contact DCP
|
|
|
T or F:
When placing a threaded plate, the screws must be placed perpendicular to the plate. |
Dumb question.
Just know that threaded plates can accept screws with threaded heads (must be placed perpendicular) as well as normal screws (can be placed at an angle). |
|
|
How large should the intermedullary nail be in an interlocking nail fixation?
|
70-80% of medullary cavity
|
|
|
What are the general pre-surgical steps before fracture repair?
|
Stabilize patient
Neuro exam Treat soft tissue injuries first Imaging Place a splint |
|
|
Why perform a neurological exam before surgery?
|
Figure out if nerve issues exist before surgery
|
|
|
How should fractures be stabilized prior to surgery?
|
Splint or Robert-Jones Bandage
|
|
|
How should the humerus be splinted? The femur?
|
Humerus - Spika Splint
Femur - DO NOT SPLINT |
|
|
What are factors impacting the clinical fracture assessment score?
|
Client/patient compliance
Pain level Comfort level |
|
|
What are some factors impacting the biologic fracture assessment score?
|
Age
Health Bone type Injury type Approach type Soft tissue envelope (blood supply) |
|
|
Post op fracture repair care should always include...
|
E collar
Pain meds (10-14d) STRICT rest |
|
|
What does pain at the site of a healed fracture indicate?
|
Its probably really not healed...
|
|
|
T or F:
Bone heals to 100% of its original strength |
True dat beeeeeeyooooooooochh
|
|
|
When should bone allograft be used?
|
Any fx w/open reduction, internal fixation
Dogs >5y Small/toy breeds Osteomyelitis Delayed/non-unions |
|
|
What are indications for taping the muzzle in mandibular fracture repair?
|
TMJ luxation
Vertical ramus fracture Minimally displaced, stable fracture Additional support for other fixes |
|
|
Mandibular wiring should be used with...
|
...symphyseal separations
...interfragmentary wiring |
|
|
T or F:
Acrylic external stabilization can be used for any mandibular fracture type. |
True!
|
|
|
When placing wires or pins in the mandible, what should be avoided?
|
Salivary caruncle
Tooth roots Mandibular canal |
|
|
What should be added to post-op care for mandibular fracture repair surgery in dogs? Cats?
|
Dogs (canned food/gruel; flush w/dilute chlorhex)
Cat (probably feed tube; flush mouth w/saline) |
|
|
Scapular fracture is commonly also associated with...
|
...thoracic trauma (70% concurrence)
|
|
|
How should a humeral IM pin be placed?
|
NORMOGRADE!!!
Start pin lateral to greater tuberosity aim caudal and medial to seat pin in medial epicondylar area |
|
|
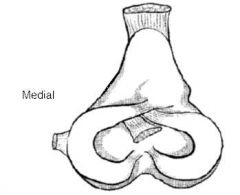
T or F:
The medial humeral condyle is more frequently fractured than the lateral. |
False.
Lateral is smaller and more weight bearing and, thus, more prone to fracture |
|
|
Which type of humeral fracture is like being dealt a big poop sandwich?
|
Dicondylar fractures (Y or T) configuration
|
|
|
When should you cast a radial fracture in a small dog?
|
NEVER! It will cause a nonunion!
|
|
|
T or F:
Fractures of the ulna don't need to be repaired in small to medium breed dogs. |
False!
There are special ulnar fractures requiring repair (styloid avulsion, semilunar notch fracture, olecranon fracture) |
|
|
The most common cause of pelvic fracture is...
|
...vehicular trauma
|
|
|
T or F:
Most patients with pelvic fractures are in shock. |
True! 93%
|
|
|
T or F:
Most patients with pelvic fractures have urinary tract ruptures. |
False! But 39% do so always suspect it...
|
|
|
Which pelvic fractures must be repaired?
|
Weight bearing axis bones (acetabulum, ileal body, SI joint)
Avulsed tuber ischii (racing dogs) Avulsed prepubic tendon |
|
|
In SI luxation repair, how far across the sacrum should the lag screw be placed?
|
At least 60%
|
|
|
What is the shit sandwich in the pelvis when it comes to fracture repair?
|
Acetabular fractures
|
|
|
What radiographic view is helpful in diagnosing capital physeal fractures?
|
Frogleg
|
|
|
What anatomical feature can assist with femoral diaphyseal fracture alignment?
|
Linea aspera (attachment of adductor magnus et brevus)
|
|
|
What is a common complication/sequel to femoral fracture repair in puppies?
|
Quadriceps fibrosis
|
|
|
T or F:
The femur can be pinned normograde or retrograde |
Yup
|
|
Where would an IM pin be placed in this tibia? How should you aim?
|
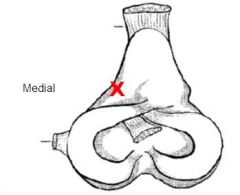
Where the X is (between patellar ligament and MCL); aim slightly laterally
|
|
|
When should retrograde IM pins be placed in the tibia?
|
NEVER NEVER NEVER
|
|
|
What are the weight bearing toes?
|
3 and 4
|
|
|
What are some antibiotics with good bone penetration?
|
Clavamox
Enrofloxacin Clindamycin (mostly bacteriostatic) Chloramphenicol |
|
|
T or F:
Infected bone will still heal as long as vascular supply and rigid stabilization are still present. |
True!
|
|
|
T or F:
A nonunion will not heal without surgery. |
True
|