Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
449 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
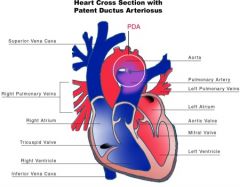
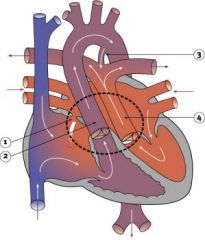
patent ductus arteriosus is failure of the fetal ductus arteriosus (artery connecting the aorta and pulmonary artery) to close within the first week of life. The continued patency of this vessel allows blood to flow from the higher pressure pulmonary artery, causing a left-to-right shunt
|
What is this?
|
defects with increased pulmonary blood flow
L-to-R |
|
What is this?
|
Tetralogy of Fallot
|
1. ventricular septal defect
2. pulmonic stenosis 3. overiding aorta 4. right ventricular hypertrophy |
|
|
What are the 2 classifications of congenital heart disease?
|
Acyanotic & Cyanotic
|
|
|
|
What is responsible for Acyanotic?
|
-increased pulmonary blood flow
-obstruction to blood flow from ventricles |
|
|
|
What defects cause increased pulmonary blood flow?
[Acyanotic] |
-Atrial septal defect
-Ventricular septal defect -Patent Ductus Arteriosus* -Atrioventricular canal |
|
|
|
What defects cause obstruction to blood flow from ventricles?
[Acyanotic] |
-Coarction of aorta*
-Aortic Stenosis -Pulmonic Stenosis |
|
|
|
What happens with cyanotic?
|
-decrease of pulmonary blood flow
-mixed blood flow |
|
|
|
What defects cause a decrease in blood flow?
|
-Tetraology of Fallot*
-Triscuspid atresia |
|
|
|
What defects cause mixed blood flow?
|
-Transposition of great arteries*
-total anomalous pulmonary venous return -truncus arteriosus -hypoplastic left heart syndrome |
|
|
|
Nutritional state:
|
failure to thrive or poor weight gain is associated with heart disease
|
|
|
|
Color:
|
-cyanosis is a common feature of congenital heart disease, and pallor is asscociated with poor perfusion.
|
|
|
|
Chest deformities:
|
An enlarged heart sometimes distorts the chest configuration
|
|
|
|
Unusual pulsations:
|
visible pulsations of the neck veins are seen in some patients.
|
|
|
|
Respiratory excursion:
|
this refers to the ease or difficulty of respiration (tachypnea, dyspnea, presence of expiratory grunt)
|
|
|
|
Clubbing of fingers:
|
this is assoicated with cyanosis
|
|
|
|
chest:
|
palpation and percussion: these maneuvers help discert heart size and other characteristics (thrills) associated with heart disease
|
|
|
|
heart rate and rhythm:
|
-listen for fast heart rates (tachycardia), slow heart rate (bradycardia), or irregular rhythms
-character of heart sounds: listen for distinct or muffled sounds, murmmurs, and additional heart sounds |
|
|
|
What are causes of CHD?
|
-infections; Rubella
-radiation -metabolic disorders; diabetes, PKU -drugs; alcohol -peripheral conditions; increased maternal age, premature birth, high altitude |
|
|
|
Common Pathology of CHD:
|
-anatomic defect: VSD, ASD, PDA
-hemodynamic alteration: Right to Left shunt-cyanotic Left to right shunt-acyanotic -altered tissue oxygenation: characterized as cyanotic or acyanotic defects based on systemic effects. |
|
|
|
What is Patent Ductus Arteriosus?
|
Failure of the fetal ductus arteriosus (artery connecting the aorta and pulmonary artery) to close within the first weeks of life. The continued patency of this vessel allows blood to flow from the higher pressure aorta to the lower pressure pulmonary artery, causing a left-to-right shunt
|
Acyanotic
[increase in pulmonary blood flow] |
|
|
Pathophysiology:
|
The additional blood is recirculated through the lungs and returned to the left atrium and left ventricle. The effect of this altered circulation is increased workload on the left side of the heart, increased pulmonary vascular congestion and possibly resistance, and pontentially increased right ventricular pressure and hypertrophy.
|
|
|
|
What are the clinical manifestations?
|
Patients may be asymptomatic or show signs of CHF. There is a characteristic machinery-like murmur. A widened pulse pressure and bounding pulses result from runoff of blood from the aorta to the pulmonary artery. Patients are at risk for bacterial endocarditis and pulmonary vascular obstructive disease in later life from chronic excessive pulmonary blood flow.
|
|
|
|
Medical Management:
|
-administration of indoethacin (prostaglandin inhibitor) has proved sucessful in closing a patent ductus in premature infants and some newborns
|
|
|
|
Surgical Management:
|
surgical litigation of the patent vessel via a left thoracotomy
|
|
|
|
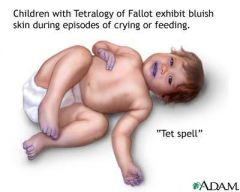
What is Tetralogy of Fallot?
|
Includes four defects:
1. ventricular septal defect 2. pulmonic stenosis 3. overiding aorta 4. right ventricular hypertrophy |
cyanotic
[decrease in pulmonary blood flow] |
|
|
What are the clinical manifestations of Tetralogy of Fallot?
|
Infants: some infants may be acutely cyanotic at birth; others have mild cyanosis that progresses over the first year of life as the pulmonic stenosis worsens. There is a characteristic murmur. There may be acute episodes of cyanosis and hypoxia, called blue spells or tet spells. Anoxic spells occur when the infant's oxygen requirements exceed the blood supply, usually during crying or after feeding.
|
|
|
|
Interventions:
|
-knee chest position
-meds; morphine, oxygen |
|
|
|
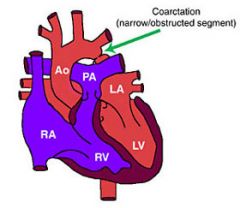
What is Coarction of the Aorta?
|
Localized narrowing near the insertion of the ductus arteriosus, resulting in increased pressure proximal to the defect (head and upper extremities) and decreased pressure distal to the obstruction (body and lower extremities)
|
Acyanotic
[obstruction of blood flow from ventricles] |
|
|
What are the clinical manifestations of COA?
|
may be high blood pressure, bounding pulses in arms, weak or absent femoral pulses, and cool lower extremities with lower blood pressure.
|
|
|
|
Medications:
|
-reduce the severity of CHF: Digoxin, Lasix, Alddactone
|
|
|
|
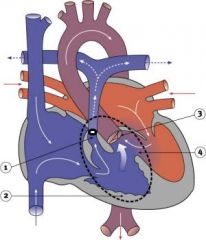
What is Transposition of the great arteries?
|
The pulmonary artery leaves the left ventricle, and the aorta exits from the right ventricle, with no communication between the systemic and pulmonary circulations.
|
Cyanotic
[mixed blood flow] |
|
|
Pathophysiology:
|
Associated defects such as septal defects such as septal defects or patent ductus arteriosus (PDA) must be present to permit blood to enter the systemic circulation and/or the pulmonary circulation for mixing of saturated and desaturated blood.
|
|
|
|
Assessment Findings:
|
-cyanosis from birth and tachypnea (worsen w/ crying)
-gallop rythm -tachycardia -dyspnea -hepatomegaly -cardiomegaly -murmurs of ASD,VSD,PDA, loud S2 -diminished exercise tolerance -fatigue -clubbing |
|
|
|
Medical Management:
Medications- |
Prostaglandin E to temporarily increase blood mixing if systemic and pulmonary mixing is inadequate
|
|
|
|
What is Rheumatic Fever?
|
-an inflammatory disease that occurs after infection with group A ß-hemolytic streptococcal pharyngitis
-it involves the joints, skin, brain, serous surfaces, and heart |
|
|
|
What is the most signifigant complication of RF?
|
cardiac valve damage (referred to as rheumatic heart disease)
|
|
|
|
Major Manifestations:
|
Carditis-tachycardia our of proportion to degree of fever, cardiomegaly, muffled heart sounds, pericardial friction rub, chest pain
polyarthritis-swollen, hot, red painful joints, after 1-3 days affects different joints, favors large joints-knees, elbows, hips, shoulders, wrists erythema marginatum-erythematous macules with clear center and wavy, well-demarcated border, transitory, nonpruritic, primarily affects trunk and extremities (inner surfaces) chorea-sudden aimless, irregular movements of extremites, involuntary facial grimaces, speech disturbances, emotional lability, muscle weakness; muscle movement exaggerated by anxiety and attempts at fine motor activity; relieved by rest subcutaneous nodes: nontender swelling, located over bony prominences, may persist for some time, then gradually resolve |
|
|
|
Minor Manifestations:
|
Arthalgia
Fever |
|
|
|
Collaboration Care:
|
-Eradicate hemolytic strep
-prevent permanent cardiac damage -palliation of symptoms -prevent recurrence -penicillin is the drug of choice, with erythromycin as a substitute in penicillin-senstive children -Salicylates are used to control the infammatory process, especially in the joints and reduce the fever and discomfort |
|
|
|
Children who have had acute RF are susceptible to recurent RF:
|
-should be followed medicaly for at least 5 years
-children and families must be aware of the need for continuing antibotic prophylaxis for dental work, infection, and invasive procedures |
|
|
|
Interventions during home care are primarily concerned with:
|
providing rest and adequate nutrition
|
|
|
|
One of the most disturbing and frustrating manifestation of the disease is:
|
chorea-the onset is gradual and may occur weeks to months after the illness; it sometimes occurs in children who have not been dx w/ RF
|
|
|
|
What is Endocarditis?
|
An infection of the valves and inner lining of the heart.
-especially affects children with valvular abnormalities, prosthetic valves, recent cardiac surgery with invasive lines, and rheumatic heart disease with valve involvement |
|
|
|
Pathophysiology:
|
organsims may enter the bloodstream from any site of localized infection; most common portals of entry are oral from dental work, UTI, cardiac surgery
|
|
|
|
Clinical Manifestations:
|
onset usually insidious
-unexplained fever (low grade and intermittent) -anorexia -malaise -weight loss characteristic findings caused by extracardiac emboli formation: splinter hemorrhages (thin black lines) under the nails, osler nodes (red, painful intradermal nodes found on pads of phalanges), Janeway lesions (painless hemorrhagic areas on palms and soles), petechiae on oral mucous membranes may be present: congestive heart failure, cardiac dysrhythmias, new murmur or change in previously existing one |
|
|
|
Therapeutic Management:
|
Treatment should be instituted immediately and consists of administration of high doses of appropriate antibiotics intravenously for 2 to 8 weeks
|
|
|
|
Prevention:
|
Involves administration of prophylactic antibiotic therapy 1 hour before procedures known to increase the risk of entry of organisms.
|
|
|
|
Acyanotic: obstruction to blood flow from ventricles
|
Coarction of the Aorta
|
|
|
|
Cyanotic: Mixed blood flow
|
Transposition of the Great Vessels
|
|
|
|
Abnormal oening between the atria, allowing blood from the higher pressure left atrium to flow into the lower pressure right atrium.
|
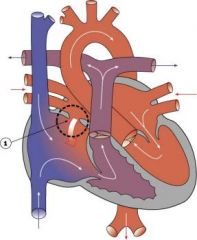
Atrial Septal Defect (ASD)
|
Defects with increased pulmonary blood flow
ACYANOTIC |
|
|
Pathophysiology:
|
Because left atrial pressure slightly exceeds right atrial pressure, blood flows from the left to the right atrium, causing an increased flow of oxygenated blood into the right side of the heart.
-Despite the low pressure difference, a high rate of flow can still occur because of low pulmonary vascular resistance and the greater distensibillity of the right atrium, which further reduced flow resistance. |
|
|
|
Clinical Manifestations:
|
Patients may be asymptomatic. They may develop congestive heart failure. There is characteristic murmur. Patients are at risk for atrial dysrhythmias (probably caused by atrial enlargement and stretching of conduction fibers) and pulmonary vascular obstructive disease and emboli formation later in life from chronic increased pulmonary blood flow
|
|
|
|
The liquid, fatty fluid that precedes mother milk is called
|
Colostrum
|
|
|
|
Important because
|
High in nutrition and natural antibodies
|
|
|
|
Breast Cancer mostly found what part of breast
|
Upper outer quadrant
|
|
|
|
Cancer causing stuff is called
|
Tetrogenic Agents
|
|
|
|
Diabetes caused by insulin resistance, mostly obese people get it
|
Type 2 Diabetes
|
|
|
|
Name some causes of congenital heart disease (CHD)
|
Infections (rubella), radiation, metabolic disorders, drugs/alcohol, peripheral conditions (maternal age. Premature etc.)
|
|
|
|
BPH is
|
Benign prostatic hyperplasia
|
|
|
|
Procedure to fix
|
turp
|
|
|
|
A heart disease caused by a fistula between left and right atrium
|
ASD (atrial Septal defect) YOU HEAR A MURMUR!
|
|
|
|
Cyanotic or a cyanotic
|
Acyanotic (mixed blood but with some o2)
|
|
|
|
A heart disease caused by a fistula between aorta and the pulmonary artery is called
|
PDA patent ductus arteriosus
|
|
|
|
Cyanotic or a cyanotic
|
Acyanotic (mixed blood but with some o2)
|
|
|
|
A heart disease caused by a fistula between left and right ventrical is called
|
VSD Ventricular Septal defect. MOST COMMON!
|
|
|
|
Cyanotic or a cyanotic
|
Acyanotic (mixed blood but with some o2)
|
|
|
|
Congenital heart disease: 4 things wrong, kid often squats ……..
|
Tetralogy of Fallot
|
None
|
|
|
Cyanotic or a cyanotic
|
Cyanotic
|
|
|
|
Congenital heart disease: aorta and pulmonary artery are interchanged and there is a atrial fistula
|
Transposition of the great vessels
|
|
|
|
Cyanotic or a cyanotic
|
Cyanotic
|
|
|
|
Obstruction of blood leaving the heart, acyanotic, can be
|
Coarctation of the aorta
|
|
|
|
Lack of o2 to heart resulting in ischemia of heart muscle is called
|
Myocardial Infarction
|
|
|
|
s/s acyanotic
|
Cool to touch
|
|
|
|
s/s cyanotic
|
Blue lips and cool to touch
|
|
|
|
Name some nursing diagnosis related to heart disease
|
-altered nutrition
-altered growth -ineffective family coping |
None
|
|
|
A possible heart disease related to URI (strep)
|
Rheumatic fever
|
|
|
|
Infection of the heart valves and lining is called
|
Bacterial endocarditis
|
|
|
|
Male sex hormone
|
Testosterone
|
|
|
|
Artificial detour of ureters from kidney to intestines to bypass bladder is called
|
Ileal Conduit
|
|
|
|
Dialysis through a semi permeable intestinal membrane is called
|
Peritoneal Dialysis
|
|
|
|
How long is the post partum period
|
6 weeks, 42 days
|
|
|
|
Jaundice is caused by
|
Too much bilirubin
|
|
|
|
And treated with
|
Uv light
|
|
|
|
Neonatal period is
|
4 weeks
|
|
|
|
When is Apgar score performed
|
1-5 minutes after birth
|
|
|
|
Good score is
|
7-10
|
|
|
|
4-6 means
|
Moderate resuscitative efforts
|
|
|
|
What medication is administered
|
Vitamin K, eye antibiotic, Hep if parents agree
|
|
|
|
Site of injections is
|
Vastus lateralis
|
|
|
|
Can you put it in IV
|
NO
|
|
|
|
Vitamin K because
|
Baby does not have enough clotting factor
|
|
|
|
Eye medication because
|
Ophthalmia neonatorum (infection gonorhorreal/chlamydial)
|
|
|
|
Circumcision care
|
Check for bleeding/infection, prevent diaper to touch penis (fold it). No Vaseline with plastabell
|
|
|
|
First feeding not larger than
|
1 oz/30cc
|
|
|
|
First feeding can be
|
Breast milk/sterile water/formula/sterile glucose
|
|
|
|
First milk is called
|
Colostrum
|
|
|
|
When does discharge planning start
|
At admission
|
|
|
|
Engorgement is
|
Feeling of tension in breast
|
|
|
|
Cured by
|
Feeding baby
|
|
|
|
If no breastfeeding
|
Do not touch/irritate
|
|
|
|
After pains are caused by
|
Uterine cramps
|
|
|
|
Last normally not longer than
|
48 hours
|
|
|
|
The process where the reproductive organs return to normal size after the baby is born is called
|
Involution
|
|
|
|
Discharge from uterus during postpartum is called
|
Lochia
|
|
|
|
If red (1/3 days post partum)
|
Lochia rubra (ruby red)
|
|
|
|
If pink or brown (3-10 days post partum)
|
Lochia Serosa
|
|
|
|
If white after 10-14 days
|
Lochia Alba
|
|
|
|
Top of uterus is called
|
fundus
|
|
|
|
Nägele's rule is
|
subtracting 3 months and adding 7 days and 1 year if appropriate to the first day of a pregnant woman's last menstrual period
|
|
|
|
Fertilization takes place in the
|
Ampulla
|
|
|
|
Pregnancy lasts
|
280 days/ 40 weeks
|
|
|
|
Low amniotic fluid could mean
|
Renal problems for baby
|
|
|
|
Rh test is called
|
Coombs test
|
|
|
|
5 digit system is
|
1. Gravida
2. Term 3. Para 4. Abortion 5. Living children |
None
|
|
|
Supine hypertension caused by
|
Laying supine for a while, pressure on descending aorta and Vena Cava: lay on side for a while will help
|
|
|
|
Anemia if
|
Hgb is = or smaller than 11
|
|
|
|
Interventions during labor
|
-emotional support
-supportive environment -physical care to provide comfort/hygiene -explain procedures -Identify everything that will interfere with labor (voiding, privacy, moving, ambulation etc.) -Encourage verbalization of fears etc. monitor progress of labor |
None
|
|
|
Rupture of the fetal membranes is called
|
Amniotomy can be AROM/SROM
|
|
|
|
Withdrawal of amniotic fluid from the sac for testing is called
|
amniocentesis
|
|
|
|
Time from conception to delivery is called
|
gestation
|
|
|
|
Other word for pregnant woman, relates to # of pregnancies
|
Gravida
|
|
|
|
And if a woman is more than one time pregnant
|
multigravida
|
|
|
|
never delivered a baby
|
Nullipara
|
|
|
|
Para is
|
Past pregnancy continued to viable period, twins count as one para
|
|
|
|
So primapara is
|
Woman who had one pregnancy and delivered after the period of viability
|
|
|
|
GTPAL
|
Gravida, Term, Para, Abortion, living children
|
|
|
|
Normal term
|
38-42 weeks
|
|
|
|
Post term is
|
More than 40 weeks
|
|
|
|
complications
|
Maternal weight loss
Decreased uterine seize Decreased amniotic sac (kidney problems baby) Large infant Postpartum hemorrhage and infection |
None
|
|
|
preterm
|
Under 37 weeks
|
|
|
|
complications
|
LBW, inadequate lung development
|
|
|
|
Lightning means
|
Decreased abdominal distention due to uterine and fetal descent (2-3 weeks before delivery)
|
|
|
|
The appearance of the fetal scalp at the vaginal orifice in childbirth is called
|
crowning
|
|
|
|
The process of the cervix/cervical canal thinning and shortening is called
|
Effacement
|
|
|
|
The process of the cervix/cervical canal expanding or enlarging from 0-10cm is called
|
Dilatation
|
|
|
|
Position of the fetus head in the true pelvis (-3-+3) is called
|
Station (0 = engaged)
|
|
|
|
IUGR means
|
Intro-uterine growth restriction (lack of oxygen, smoking, drugs, placenta previa)
|
|
|
|
Neonate is
|
First 28 days of life
|
|
|
|
Chadwicks sign is
|
purple color of vaginal walls
|
|
|
|
Possible signs of pregnancy are
|
-absence of menstruation
-breast tenderness -nausea/vomiting |
None
|
|
|
Probable signs
|
Pregnancy test/Chadwicks, Goodells and Hegar’s signs
|
|
|
|
Positive signs
|
Ultrasound/FHR
|
|
|
|
Quickening means
|
First movement (feels like gas, 4th month)
|
|
|
|
With cephalic birth, what part of head first?
|
vertex
|
|
|
|
Surgical incision of the perineum during delivery is called
|
Episiotomy
|
|
|
|
Normal FHR
|
110-180
|
|
|
|
Three stages of delivery are
|
First: - dilation
- early latent phase - mid/active phase - transitional phase (most dramatic) second : delivery, usual 30 minutes to 3 hours Third stage: delivery of placenta (2 to 20 minutes) |
None
|
|
|
Nursing assessment stage
|
Membrane status
True/false contraction Color of amniotic fluid if ruptured Vaginal exam for effacement, dilatation, presentation, position, station |
None
|
|
|
Nursing interventions during labor include
|
- providing support to mother and supporter
- maintain a supportive environment - giving physical care to provide comfort - explain all procedures - identify everything that may interfere with labor (voiding, privacy, moving) - provide encouragement - encourage verbalization of fears and concerns - continually monitor progress of labor |
None
|
|
|
The first thing the nurse does after the water breaks
|
Check FHR (because umbilical cord could be under pressure
|
None
|
|
|
Early decelerations: nursing intervention
|
Position change (not benign)
|
|
|
|
Early decelerations: what causes it
|
Head compression, means baby is in position!
|
|
|
|
Variable decelerations: nursing intervention
|
Position change (not benign)
|
|
|
|
Variable decelerations can point to
|
Cord compression
|
|
|
|
Late decelerations: nursing intervention
|
02 mask (8-10 liters)
|
|
|
|
How does the fetus adapt to birth stress
|
FHR goes up
|
None
|
|
|
Pushing/breathing during contractions…how
|
At beginning of contraction two cleansing breaths, at peak of contraction push, with breathing, at end of contraction two more cleansing breaths
|
|
|
|
Contra-indications for epidural
|
- allergy
- maternal refuse - antepartum hemorrhage - bleeding disorder/anti coagulant therapy - infections at the injection site - maternal hypotension |
None
|
|
|
First stage of labor: cervix open in three stages:
|
Latent 0-3 cm contractions 5-30 minutes apart 30-45 sec long
|
|
|
|
*Risk Factors for CAD
|
Modifiable:
Cholesterol, elevated serum lipids (LDL/HDL), smoking, weight, stress, HTN, DM Non-Modifiable: -age, race, gender, family hx; (genetics) |
None
|
|
|
Angina
|
Angina is defined as “An oppressive pain in the chest that is caused by inadequate blood flow and oxygenation to the heart muscle.”
|
|
|
|
Which diabetes: weight gain, blurred vision, slow to heal, UTI’s, spontaneous abortion
|
Type2
|
|
|
|
What is the leading undiagnosed cause of depression and suicide in the elderly???
|
Myxedema (long hypothyroidism)
|
|
|
|
s/s of hypothyroidism
|
Everything is slow: weak heart, depressed, constipation, high LDL, dry skin, thick tongue, croaky voice, cold skin, cold intolerant
|
|
|
|
Severe or long standing hypothyroidism is called
|
Myxedema
|
|
|
|
s/s
|
Non pitting edema, especially in hands, feet, subclavicular fossae, slurred speech, hoarseness
|
|
|
|
What can happen if Myxedema is severe
|
Coma : hypothermia, hypoventilation, lactic acidosis, hypotension
|
|
|
|
What can provoke this
|
Narcotics or sedatives
|
|
|
|
Most common cause of hypothyroidism
|
Atrophy of the thyroid gland or in developing countries: lack of iodine in diet
|
|
|
|
How do you care for someone with hypothyroidism: assessment
|
- weight gain
- mental changes - slurred speech - cold intolerance - thick, dry skin - constipation - Dyspnea |
None
|
|
|
How do you care for someone with hypothyroidism: diagnosis
|
- hypothermia
- imbalanced nutrition (more than required) hypometabolism - constipation - activity intolerance (low metabolism) - disturbed thought process (diminished cerebral bloodflow) activity intolerance (low metabolism) |
None
|
|
|
What is the most common cause of hyperthyroidism
|
Graves disease
|
|
|
|
What is Graves’ disease
|
Autoimmune disease marked by thyroid enlargement and excessive thyroid hormone secretion
|
|
|
|
What age and sex are most affected by hyperthyroidism?
|
women age 30-50
|
|
|
|
What is Thyrotoxicocis
|
It refers to the physiologic effects of hypermetabolism that results from excess circulating levels of T4 T3 or both
|
|
|
|
s/s of hyperthyroidism
|
Hypermetabolic, no sleep, weight loss, palpations, SOB,
|
|
|
|
Treatment for hyperthyroidism is
|
Radioactive iodine, irradiation of gland, Propranolol, surgery
|
|
|
|
A thyroid disease with as a sign goiter
|
Graves disease
|
|
|
|
How do you take care of someone with hyperthyroidism: assessment
|
objective: hyperthermia, palpitations, exopthalmos, blinking, diaphoretic, thin nails, thick velvety skin, clubbing, tachypnea, tachycardia, bounding pulse, increased bowel sounds
VS : HTN |
None
|
|
|
How do you take care of someone with hyperthyroidism: diagnosis
|
- imbalanced nutrition (less than body requirement): hypermetabolism
|
|
|
|
How do you take care of someone with hyperthyroidism: interventions
|
normal hyperthyroidism is home care but if they have acute Thyrotoxicocis:
- place patient in cool quit room - change bed linens regularly if diaphoresis - encourage exercise - restrict visitors who upset patient - establish a supportive, trusting environment |
None
|
|
|
Thyroid storm is
|
Extreme hyperthyroidism on persons with undiagnosed or undertreated thyroid disease (because of stress/trauma)
|
|
|
|
Other name is
|
Thyrotoxic crisis
|
|
|
|
s/s
|
Dehydration, tachycardia, heart failure, HYPERTHERMIA, agitation, delirium, fever : EMERGENCY
|
|
|
|
An autoimmune diseases: not enough cortisol but also associated with Hashimoto’s disease, pernicious anemia, idiopathic hypoparathyroidism
|
Addison’s disease
|
|
|
|
What is wrong?
|
Addison's disease is a severe or total deficiency of the hormones made in the adrenal cortex, caused by a destruction of the adrenal cortex
|
|
|
|
What hormones are produced in adrenal glands
|
cortisol and aldosterone
|
|
|
|
s/s
|
Weakness, fatigue, anorexia, hypoglycemia
|
|
|
|
electrolytes
|
Na down, K up so beware of Hyponatremia and hyperkalemia
|
|
|
|
Treatment:
|
Add corticoidsteroids and salt to diet
|
|
|
|
How do you take care of someone with Addison’s …assessment
|
- vital signs
- fluid volume deficit - electrolyte imbalances (N & K) - daily weights - understanding of medication |
None
|
|
|
Remember Addison’s and salt
|
ADDisons ADD salt
|
|
|
|
A disease caused by increased levels of cortisol is called
|
Cushing’s disease
|
|
|
|
How do you take care of someone with Addison’s …..?diagnosis
|
risk for imbalanced nutrition: less than body requirement (loss of appetite)
|
None
|
|
|
How do you take care of someone with Addison’s …interventions
|
- avoid stress
- I/O daily weights - Teach: medication compliance - Keep quit , safe, low stress environment - Give medications |
None
|
|
|
3 kinds of diabetes are
|
- DM I
- DM II - gestational diabetes |
None
|
|
|
Characteristics of type 1
|
- abrupt onset
- primary defect of Beta cells - always insulin dependent - prone to develop Ketoacidosis - affects mostly teens - decrease in size and number of Islet cells |
None
|
|
|
Type two is caused by
|
insulin resistance
|
|
|
|
characteristics
|
- no ketosis/Ketoacidosis
- insidious onset - usually not insulin dependent - mostly after 40 years - often obese |
None
|
|
|
What race/group is most likely to get type 1
|
Caucasian (western Europe)
|
|
|
|
What race/group is most likely to get type 2
|
Native American, Hispanics
|
|
|
|
Which one is linked to lower economic status
|
Type 2
|
|
|
|
What does the lack of insulin do to your body
|
- glucose is not taken in by hepatic and skeletal muscles
- glucose accumulates in blood and spills in urine - fluid shifts : dehydration, thirst, blurred vision - breakdown of fat & protein: weight loss: ketosis METABOLIC ACIDOSIS |
None
|
|
|
Which diabetes: confusion, weight loss, ketone bodies in blood, paresthesia
|
Type 1
|
|
|
|
What can happen to nails of people with diabetes
|
Harden, yellow
|
|
|
|
Diagnosed with diabetes if
|
Blood level glucose over 126 x 2 readings
|
|
|
|
Diabetes: weird behavior can be sign of
|
Hypoglycemia treat with glucose
|
|
|
|
Treatment of type 1 is
|
Insulin
|
|
|
|
What adrenal disease: NA up.
|
Cushing’s (water retention)…cushion …..
|
|
|
|
What adrenal disease: NA down
|
Addison’s ….add salt………………….
|
|
|
|
Treatment of type II
|
Insulin sensitizers / insulin/ diet/ exercise
|
|
|
|
s/s of hypoglycemia
|
Irritable, hunger, fatigue, vision problems, pallor, tremor, anxiety, confusion, poor judgment seizure, coma
|
|
|
|
If you doubt between hypo and hyper treat like
|
Hypo
|
|
|
|
Acetone breath, malaise, dry mouth could be sign of
|
Diabetic Ketoacidosis
|
|
|
|
Treat it with
|
Insulin, IV fluids and might need dialysis
|
|
|
|
A diabetic coma with sever dehydration BG level 600-200 could be
|
Hyperosmolar hyperglycemic non-ketotic syndrome (HHNKS)
|
|
|
|
Could happen to
|
Diabetes II, undiagnosed, too much sugar
|
|
|
|
Night time hypoglycemia with morning hyperglycemia released to epinephrine and GH is called
|
Somogyi phenomenon
|
|
|
|
treat
|
Night time snack or less insulin
|
|
|
|
And same thing without night time hypoglycemia is
|
Dawn phenomenon
|
|
|
|
treat
|
Pm insulin
|
|
|
|
Most common complication of diabetes is
|
Diabetic neuropathy: may be reversible
|
|
|
|
s/s
|
Wrist drop, paresthesia, amyotrophy
|
|
|
|
Vascular disease related to long high glucose levels
|
Microvascular disease
|
|
|
|
Can progress in
|
Microangiopathy (hypoxia/ischemia )
|
|
|
|
Blurred vision, spots on retina can be
|
Diabetic retinopathy
|
|
|
|
Proteinuria with diabetes can be sign of
|
Diabetic nephropathy
|
|
|
|
More common in type
|
1
|
|
|
|
Macrovascular disease most common in type
|
2
|
|
|
|
Related to
|
Obesity: CVA, MI, atherosclerosis
|
|
|
|
Leading cause of amputations is
|
Peripheral vascular disease (peripheral…end of limb)
|
|
|
|
What are the different insulin types?
|
- rapid acting (Lispro/Humalog)
- short acting (regular, R) - intermediate lasting (NPH) - long lasting (Humulin U) - premixed combinations of NPH/regular |
None
|
|
|
What is the only kind you can administer IV
|
REGULAR
|
|
|
|
What is an insulin reaction?
|
It is another name for hypoglycemia or they mean that you get a little redness/swelling at the injection site
|
|
|
|
How do you give insulin correctly
|
Clean skin, give in abdomen, 2 inch right/left off belly button, check right amount/type, and test blood glucose first if needed.
|
|
|
|
DKA is
|
Diabetic ketoacidosis is a complication of diabetes caused by the buildup of by-products of fat metabolism (ketones), which occurs when glucose is not available as a fuel source for the body.
|
|
|
|
s/s DKA
|
Frequent urination or frequent thirst for a day or more
|
|
|
|
Treatment of DKA
|
The goal of treatment is to correct the elevated blood glucose level by giving additional insulin, and to replace fluids lost through excessive urination and vomiting. If ketoacidosis is severe, hospitalization is required to control the condition. Insulin replacement will be given, fluid and electrolytes will be replaced, and the cause of the condition (such as infection) will be identified and treated.
|
|
|
|
Nursing assessment for DKA and HHNS are
|
- bloodglucose and count, PH of blood, urinalysis
- physical exam, heart, respiration, LOC |
None
|
|
|
Nursing interventions for DKA and HHNS are
|
- insulin!!!! Regular through IV if possible
- Fluid replacement (more in DKA) - Electrolyte replacement (K) - Assessment for mental status - Record I/O - Asses bloodglucose - ECG monitoring - Asses respiratory status - PH les than 7: administer sodium bicarbonate |
None
|
|
|
HHNS what is it
|
Hyperosmolar Hyperglycemic Nonketotic Syndrome, or HHNS, is a serious condition most frequently seen in older person it occurs more often in people with type 2. HHNS is usually brought on by something else, such as an illness or infection. In HHNS, blood sugar levels rise, and the body tries to get rid of the excess sugar by passing it into the urine. The body makes lots of urine at first, and the patient has to go to the bathroom more often. Polydipsia because of the urination!
|
|
|
|
Physical findings in these patients
|
Blood sugar level over 600 mg/dl
|
|
|
|
How does it differ from DKS
|
The difference between DKS and HHNS is that
|
|
|
|
Hyperglycemia s/s
|
Polyphagia (frequent hunger, especially pronounced hunger)
|
|
|
|
Normal bloodglucose is
|
70-105, some say 80-100 mg/dl
|
|
|
|
Critical levels are
|
<50 or >400 mg/dl
|
|
|
|
Hypoglycemic s/s
|
Mild Signs Include:
Headache, hunger, sweating, nervousness, problems staying focused, mood changes, and weakness. Moderate Signs Include: Heavy sweating, increasing weakness, heart palpitations, memory loss, double vision, problems walking, and numbness in the area of the mouth and (possibly) the fingers. Severe Signs Include: Seizures, fainting, muscle twitching, and passing urine unexpectedly. |
None
|
|
|
The two types of DM I are
|
- immune mediated (viral or infection, triggers antibodies against insulin and destroy insulin producing cells, symptoms appear after 90% is destroyed)
- non-immune (more common in Asian, African-American) |
None
|
|
|
Prone to develop
|
Ketoacidosis
|
|
|
|
Nursing management related to stroke
|
maintain stable or improve LOC
attain maximum physical function attain maximum self care-abilities and skills maintain stable body functions (bladder control) maximize communication abilities maintain adequate nutrition avoid complications maintain effective personal and family coping |
None
|
|
|
s/s hemorrhaging stroke
|
worst headache ever
|
|
|
|
Modifiable risk factors for stroke
|
HTN (#1)
High serum lipids Smoking Alcohol Diabetes heart disease Obesity Oral contraceptives |
None
|
|
|
Other word for stroke
|
cerebrovascular accident (CVA),[
|
|
|
|
s/s Ischemic stroke
|
- muscle weakness (hemiplegia)
- numbness - reduction in sensory or vibratory sensation - In most cases, the symptoms affect only one side of the body. The defect in the brain is usually on the opposite side of the body - altered smell, taste, hearing, or vision (total or partial) - drooping of eyelid (ptosis) and weakness of ocular muscles - decreased reflexes: gag, swallow, pupil reactivity to light - decreased sensation and muscle weakness of the face - balance problems and nystagmus - altered breathing and heart rate weakness in sternocleidomastoid muscle (SCM) with inability to turn head to one side |
None
|
|
|
assessment
|
See above, watch for HTN, respiratory distress, difficulty swallowing, incontinence, nausea, vomiting vertigo
|
|
|
|
So priority
|
- airway /oximetry/o2
- CT scan - Risk for falling - Remove dentures - Elevate HOB - Ischemic: anticoagulants - Siderails |
None
|
|
|
ongoing
|
- Glasgow coma scale
- VS - Motor/sensory functions - Pupil reaction - O2 - Cardiac rhythm - Reassure family |
None
|
|
|
What is Myasthenia gravis
|
a neuromuscular disease leading to fluctuating weakness and fatiguability. At about 14 cases per 100,000 (in the U.S.), it is one of the lesser known autoimmune disorders. The antigens and basic disorder mechanisms are known. Weakness is caused by circulating antibodies that block acetylcholine receptors or the MuSK protein at the post-synaptic neuromuscular junction, inhibiting the stimulative effect of the neurotransmitter acetylcholine. Myasthenia is treated with immunosuppression, cholinesterase inhibitors and, in selected cases, thymectomy.
|
|
|
|
Primary manifestation is
|
Fluctuating weakness (goes away with rest)
|
|
|
|
Often first seen at
|
Eyes (eyelids)
|
None
|
|
|
Other visible things
|
Difficulty swallowing, speaking, breathing
|
|
|
|
Chronic?
|
Yes but with exacerbations and remissions
|
|
|
|
Nursing assessment
|
- severity determined by fatigability
- coping abilities - understanding disorder - RR, O2, ABG, pulmonary function test - Respiratory distress |
None
|
|
|
Nursing diagnosis
|
- ineffective breathing pattern (weak intercostal muscles)
- ineffective airway clearance (impaired cough and gag reflex) - impaired verbal communication (weakness of mouth, larynx, lips) - impaired nutrition (less: swallowing is hard) - disturbed sensory perception (visual: eyelids droop) - activity intolerance (muscle weakness) - disturbed body image |
None
|
|
|
What is in the Glasgow Coma scale
|
Best Eyes
Best Verbal response Best motor |
None
|
|
|
15 is
|
best
|
|
|
|
8 or less is
|
Coma (8=intubate)
|
|
|
|
3 is
|
death
|
|
|
|
Respiration: cycles of hyperventilation and apnea
|
Cheyne Stokes
|
|
|
|
Cushing triad indicates
|
ICP
|
|
|
|
Cushing triad is
|
Signs of increased intracranial pressure:
|
|
|
|
Rising temperature could mean
|
Increased metabolic rate of the brain (dysfunction of hypothalamus or brainstem)
|
|
|
|
ICP can be caused by
|
Trauma, hemorrhage, tumors, hydrocephalus, edema, inflammation
|
|
|
|
Earliest indication of ICP is
|
Declining LOC (tired, weak, headache)
|
|
|
|
Other s/s
|
Headache, Abnormal respirations , Widening pulse pressure
|
|
|
|
Interventions
|
- prevent hypoxia: makes ICP worse (CO2 widens veins: more pressure)
- elevate HOB 30-40% - prevent flexion of hips and neck - mechanical ventilation if needed to keep Paco2 30-35 - prevent shivering (maintain body temperature) - lower environmental stimuli (dark room/low visitors, quiet) |
None
|
|
|
a syndrome of massive imbalanced reflex sympathetic discharge occurring in patients with spinal cord injury (SCI) above the splanchnic sympathetic outflow (T5-T6) started sympathetic visceral sign
|
Autonomic dysreflexia or Hyperreflexia
|
|
|
|
What happens
|
Episodes of hypertension, sweating, slow heart beat and severe headaches may occur spontaneously in these patients, with variable severity. Treatment is aimed at controlling the blood pressure and the associated symptoms.
|
|
|
|
Interventions
|
- Blood pressure and pulse measurement
- Investigation of systemic causes of autonomic dysreflexia - Urinary catheterization - Nonpharmacologic management of elevated blood pressure through lateral tilt or upright positioning and loosening clothing or constrictive devices - Pharmacologic management for elevated blood pressure (nitropatch etc) - Management of symptomatic hypotension (leg elevation, intravenous fluids, adrenergic agonists such as norepinephrine) - Patient and caregiver education about autonomic dysreflexia |
None
|
|
|
Emergency interventions with spinal injury
|
AIRWAY FIRST
|
|
|
|
What is spinal shock
|
a temporary, sudden condition following transection of the spinal cord that is characterized by muscular flaccidity and loss of motor reflexes in all parts of the body below the point of transection
|
|
|
|
spinal shock: what happens to muscles
|
- paralyzed
- flaccid - reflexes are absent |
None
|
|
|
Spinal shock ends when
|
Reflexes return
|
|
|
|
Encephalitis is
|
an acute inflammation of the brain, commonly caused by a viral infection. Brain damage occurs as the inflamed brain pushes against the skull, and can lead to death. Patients with encephalitis suffer from fever, headache, vomiting, confusion, drowsiness and photophobia. The patients could also suffer from weakness, seizure, and less commonly, stiffness of the neck.
|
None
|
|
|
Meningitis
|
is the inflammation of the membranes (meninges) covering the brain, usually due to bacterial infections elsewhere in body that has spread into the blood and into the cerebrospinal fluid (CSF).
|
|
|
|
Parkinson’s disease is
|
is a degenerative disorder of the central nervous system that affects the control of muscles, and so may affect movement, speech and posture. The primary symptoms are the results of excessive muscle contraction, normally caused by the insufficient formation and action of dopamine, which is produced in the dopaminergic neurons of the brain.
|
|
|
|
s/s
|
It is often characterized by muscle rigidity, tremor, a slowing of physical movement (bradykinesia). (2 of the 3=diagnosis)
|
|
|
|
Typical complications
|
- dysphagia
- pneumonia - UTI’s - Skin breakdown |
None
|
|
|
Typical drug
|
Levodopa/Sinemet
|
|
|
|
Important nutritional factors
|
Fibers/roughage
|
|
|
|
Nursing goals of Parkinson’s
|
- maximize neurological function
- maintain independence ADL as long as possible - optimize psychosocial well being |
None
|
|
|
Nursing diagnosis
|
- impaired physical mobility
- impaired verbal communication - imbalanced nutrition: less - deficient diversional activities |
None
|
|
|
Nursing interventions
|
- assist with ambulation
- Rom exercises - Teach walking etc - Allow enough time for communication - Encourage deep breaths before speaking - Alternatives for communication (pictures etc) - Watch for aspiration - Soft food, thickener - Provide diversional activities |
None
|
|
|
What is Alzheimer’s
|
is a neurodegenerative disease characterized by progressive cognitive deterioration together with declining activities of daily living and neuropsychiatric symptoms or behavioral changes. It is the most common cause of dementia.
|
|
|
|
Nursing goals for care giver
|
- Reduce stress
- Maintain personal health - Cope with long term effects on caregiver |
None
|
|
|
Interventions
|
- Coping enhancement: social and community interventions, support groups
- Anticipatory guidance: teach what to expect to patient and family - Cognitive stimulation: remind on where and when, exercise mind etc - Fall preventions: remove small rugs, get good lights in hallways, bedside urinal etc. - Assist with bathing etc The list is endless see page 1592/93/95 |
None
|
|
|
Legal description of blindness
|
Best visual acuity w/ corrective lenses in the better eye of 20/200 or less or visual acuity of <20 degrees of the visual field in the better eye
|
|
|
|
Assessment of eye
|
- pupils round and equal, reacting to light
- sclera is white - cornea is transparent - red reflex with ophthalmoscope |
None
|
|
|
Cataracts are
|
Opacity of the lens that distorts image projected on retina, can cause blindness
|
|
|
|
After cataract surgery
|
- avoid rubbing/straining
- avoid rapid eye movements - avoid sneezing/coughing - wipe fluids with sterile cottonball from inner side to outside of eye - use eye shield at hospital |
None
|
|
|
Glaucoma is
|
Increased intraocular pressure due to inadequate drainage of aqueous humor from the canal of Schlemm or overproduction of aqueous humor.
|
|
|
|
Interventions acute glaucoma
|
- administer medication
- prepare for peripheral iridectomy |
None
|
|
|
Breast cancer acute interventions
|
- knowledge deficit
- fear - body image |
None
|
|
|
What about arm after mastectomy
|
- exercise !, watch for lymphedema
|
|
|
|
CAD is
|
Coronary artery disease
|
|
|
|
Modifiable risk factors CAD
|
- cholesterol
- serum lipids (LDL/HDL) - smoking -weight - stress -HTN - DM |
None
|
|
|
Non-modifiable risk factors
|
- age
- race - gender - family |
None
|
|
|
Ischemia is
|
is a restriction in blood supply, generally due to factors in the blood vessels, with resultant damage or dysfunction of tissue.
|
|
|
|
Infarction is
|
necrosis of tissue due to upstream obstruction of its arterial blood supply. It is the culmination of ischemia.
|
|
|
|
ACS is
|
Acute coronary syndrome
|
|
|
|
Angina is
|
Oppressive pain in the chest that is caused by inadequate bloodflow and oxygenation of the heart muscle
|
None
|
|
|
Most common complication of MI
|
arrhythmias
|
|
|
|
Nursing diagnosis CAD
|
- pain
- ineffective tissue perfusion - anxiety - activity intolerance - ineffective therapeutic regimen management |
None
|
|
|
Main risk factors MI
|
- CAD
- DM - HTN - Age |
None
|
|
|
s/s right CHF
|
Edema in extremities
|
|
|
|
s/s left CHF
|
Pulmonary edema/SOB starts left, goes right!
|
|
|
|
Nursing diagnosis CHF
|
- activity intolerance
- excess fluid volume - disturbed sleep pattern - impaired gas exchange - anxiety - deficient knowledge |
None
|
|
|
Drug of choice for pain with pulmonary edema is morphine because
|
Decrease preload and Afterload and relief of pain/anxiety
|
|
|
|
Check what labs when pt is on diuretics
|
Potassium
|
|
|
|
Modifiable risk factors for HTN
|
- sodium in diet
- alcohol - smoke - DM - Serum lipids - obesity |
None
|
|
|
Non-modifiable risk factors for HTN
|
- age
- gender - race - family hx |
None
|
|
|
Main risk factors for HTN
|
- ethnicity
- sedentary lifestyle - socioeconomic status - stress |
None
|
|
|
Complications of HTN to what organs
|
- brain (stroke)
- heart (CAD) - kidneys - eyes |
None
|
|
|
Diagnostic studies for HTN
|
- hx and physical
- BP measure in both arms |
None
|
|
|
tips
|
Use arm with highest reading as main arm to measure and let pt rest before measurement
|
|
|
|
Nursing diagnosis HTN
|
- ineffective health management
- anxiety - sexual dysfunction - ineffective therapeutic regimen - disturbed body image (after amputation) |
None
|
|
|
Risk factors for PAD are
|
- smoking
- Hyperlipidemia - hypertension - DM - Age over 40hyperjomocystinemia |
None
|
|
|
The pain in muscles that is gone after resting is called
|
Intermittent claudication
|
|
|
|
Is it reproducible?
|
Yes
|
|
|
|
Other s/s
|
Skin shiny, no hair, low peripheral pulses, feet can get red, pain with exercise
|
|
|
|
Important nutritional/lifestyle advice
|
- diet low in cholesterol (less than 200 mg/day)
- decrease intake of saturated fat - use soy instead of animal proteins - exercise at least 3 x 30 minutes a week - stop smoking |
None
|
|
|
What to asses
|
- DM
- Smoking - Hypertension - Hyperlipidemia - Obesity |
None
|
|
|
Important interventions after acute PAD (peripheral artery disease)
|
- Avoid knee-flexed position (except exercise)
- Turn patient regular - Check pulses - check sensitivity of extremity |
None
|
|
|
2 kinds of thrombosis in extremities
|
- deep vein
- superficial |
None
|
|
|
Directly after DVT important
|
Bedrest, leg up, heparin to prevent cloths to travel through body
|
|
|
|
Blood test Heparin
|
Ptt
|
|
|
|
Blood test Coumadin
|
Pt
|
|
|
|
Typical s/s anemia include
|
- palpitations
- Dyspnea - Diaphoresis - Jaundice - Pallor - Pruritus - Increased HR - Systolic murmurs - Angina - MI - CHF |
None
|
|
|
Common anemia of elderly
|
Iron deficient anemia
|
|
|
|
Cobalamin is
|
Vitamin b 12
|
|
|
|
In a severely anemic patient, the nurse would expect to find
|
Dyspnea and tachycardia.
|
|
|
|
What is the definition of GFR?
|
The definition of GFR is the volume of fluid filtered from the renal glomerular capillaries into the Bowman's capsule per unit time
|
|
|
|
How is it measured
|
Creatinine clearance is used to measure GFR.
|
|
|
|
Cystitis
|
(inflammation of the bladder) it is a lower urinary infection
|
None
|
|
|
Pyelonephritis
|
(inflammation of the kidney) is an upper urinary infection
|
|
|
|
Urethritis
|
(inflammation of the urethra) is a lower urinary infection
|
|
|
|
What is the difference between a complicated and uncomplicated UTI?
|
Uncomplicated (simple) infections occur in healthy urinary tracts and do not spread to other parts of the body. They usually go away readily with treatment.
|
|
|
|
Most common calculi is
|
Calcium oxalate
|
|
|
|
Best prevention
|
Drink enough / A diet low in protein, nitrogen and sodium intake.
|
|
|
|
s/s of calculi are
|
Abdominal flank pain
Hematuria Renal colic Nausea/vomiting |
None
|
|
|
Nursing care for urinary tract calculi
|
- prevention of stones occurring (drink fluids)
- dietary restrictions teaching (purines/oxalates) - turn immobile pt Q 2h - pain management/medication - monitor urine PH, I/O - strain urine to catch stone |
None
|
|
|
Difference between lower and upper UTI is
|
Upper is kidney and ureters
|
|
|
|
Order of assessment of the abdomen is
|
1. Inspect
2. Auscultate 3. Percuss 4. Palpate |
None
|
|
|
More woman than man have UTI why
|
Shorter urethra
|
|
|
|
Preventative measures are
|
- wipe front to back
- drink a lot - urinate after intercourse - sterile procedure catheters etc - empty bladder completely - empty bowl regularly - drink cranberry juice |
None
|
|
|
s/s UTI
|
A strong urge to urinate that cannot be delayed which is followed by a sharp pain or burning sensation in the urethra when the urine is released. Most often very little urine is released and the urine that is released may be tinged with blood. The urge to urinate recurs quickly and soreness may occur in the lower abdomen, back, or sides. Urine can smell or look different.
|
|
|
|
Most common bacterial agent in UTI is
|
E-coli
|
|
|
|
What is different with the elderly
|
Signs are the same as others but:
Patient can be confused Unexplained low-grade fever Change in odor or appearance of urine |
None
|
|
|
Advantage of hemodialysis
|
- Rapid fluid removal
- Rapid removal of urea and creatinine - Effective K removal - Less protein loss Home dialysis possible |
None
|
|
|
Disadvantage of hemodialysis
|
- Vascular access problems
- Dietary and fluid restrictions - Extensive equipment needed - Hypotension during procedure - Surgery for access placement - Specially trained personnel needed - Self image problems with access |
None
|
|
|
Advantage of peritoneal dialysis
|
- less diet restrictions
- less complicated - short training - home dialysis possible - good for diabetic patient |
None
|
|
|
Disadvantage of peritoneal dialysis
|
- Peritonitis
- Protein loss - Self image problems - Hyperlipidemia - Surgery for placement - Catheter can migrate |
None
|
|
|
What are some nutritional considerations for the patient in CRF on hemodialysis
|
- no protein restriction (protein is lost in dialysis)
- eat enough carb and fat - fibers in diet (often constipated) - no potassium/sodium rich foods - Iron supplements |
None
|
|
|
s/s appendicitis
|
Pain (RLQ)/anorexia/nausea/vomiting
|
|
|
|
Nursing management appendicitis
|
Before surgery: NPO, no laxatives/ice pack
|
|
|
|
Erickson: infant
|
Trust vs mistrust
|
|
|
|
Erickson: toddler
|
Autonomy vs. shame and doubt
|
|
|
|
Erickson school aged kid
|
Industry vs. inferiority
|
|
|
|
Erickson adolescent
|
Identity vs. role confusion
|
|
|
|
Major roles of pediatric nursing is
|
Promotion of wellness and disease prevention
|
|
|
|
Other factors
|
- metabolism
- sleep and rest - speech and communication |
None
|
|
|
Young child has to go to hospital, how long before hand will you tell
|
2-3 days before
|
|
|
|
Nephrotic syndrome is
|
Nephrotic syndrome is a disorder where the kidneys have been damaged, causing them to leak protein from the blood into the urine. It is a fairly benign disease when it occurs in childhood.
|
|
|
|
s/s of nephrotic syndrome
|
Proteinuria, hypoalbuminemia ,Hyperlipidemia
|
|
|
|
Nursing diagnoses
|
- risk for fluid deficit/excess
- altered nutrition - risk for impaired skin integrity - activity intolerance - body image disturbance |
None
|
|
|
Nursing assessment
|
- daily weights
- I/O - Urine tests - Measure abdomen - Asses for pallor, edema, fatigue |
None
|
|
|
treatment
|
Bed rest, corticosteroids (edema), good nutrition, increased activity if possible, family teaching
|
|
|
|
Glomerulonephritis (GN) is bacterial, viral or parasitic pathogens),
|
a primary or secondary autoimmune renal disease characterized by inflammation of the glomeruli. It may be asymptomatic, or present with hematuria and/or proteinuria (blood resp. protein in the urine
|
|
|
|
Most common in children
|
Acute poststreptococcal glomerulonephritis
|
|
|
|
Gender/age?
|
More boys than girls: school age
|
|
|
|
s/s
|
- irritable, fatigue, lethargic
- pallor, high BP, weight gain - Oliguria, hematuria - Hx of strep infection |
None
|
|
|
Urine lab
|
Elevated BUN & creatinine levels
|
|
|
|
Nursing diagnosis
|
- fluid volume excess
- activity intolerance - altered patterns of urinary elimination - altered family process |
None
|
|
|
Assessment
|
- vitals
- fluid status, electrolytes - complications? |
None
|
|
|
Nursing management;
|
- Administer medication (calcium channel blockers, B-blockers, ACE blockers if condition is severe
- Antibiotics - Anticonvulsants - Diet with no added salt |
None
|
|
|
If edema/hypertensive?
|
Sodium restrictions
|
|
|
|
Nursing care
|
- quiet play activities
- refer to social services - teaching: stress, complications, home care, diet, medications |
None
|
|
|
Wilms tumor is
|
Wilms tumor is a neoplasm of the kidneys that typically occurs in children. It is also known as a nephroblastoma
|
|
|
|
Important
|
Do NOT palpate abdomen
|
|
|
|
Important after surgery
|
Deep breathing etc
|
|
|
|
Family care
|
- shock to family
- asses understanding - provide support - allow to express feelings - play therapy regarding kids attitude to surgery |
None
|
|
|
Barlow maneuver is
|
Flex legs breast
|
|
|
|
Hypospadias is
|
Meatus below the glans
|
|
|
|
Epispadias is
|
Meatus on dorsal surface of penis
|
|
|
|
What is cystic fibrosis
|
A common hereditary disease that affects the entire body, causing progressive disability and early death. Difficulty breathing is the most common symptom and results from frequent lung infections, which are treated, though not always cured, by antibiotics and other medications. A multitude of other symptoms, including sinus infections, poor growth, diarrhea and infertility, result from the effects of CF on other parts of the body
|
|
|
|
Further more
|
Increased viscosity of mucous secretions
|
|
|
|
What electrolytes are involved
|
Chloride and Sodium
|
|
|
|
test
|
Sweat test
|
|
|
|
Why not possible on babies
|
Not enough sweat
|
|
|
|
s/s
|
- abdominal distention/ vomiting/ failure to pass stools
- dehydration/large bulky stools (stinky) - weight loss/ wheezing/coughs - salty skin |
None
|
|
|
At assessment you find a firm, olive like, movable mass in the RUQ of a baby, what could that be?
|
Pyloric Stenosis
|
|
|
|
What is Retinoblastoma?
|
-most common congenital malignant intraocular tumor of childhood primarily in children younger than 5 years
|
|
|
|
What causes Retinoblastoma?
|
caused by a mutation in a gene and my occur sporadically or be inherited -develops when the mutated gene is unable to produce the natural signals to stop the growth of retinal cells
|
|
|
|
What is Conjunctivitis?
|
Inflammation of the conjunctiva from virus or bacteria
|
|
|
|
What are the clinical manifestations?
|
red, blood vessels swollen -sticky, with a discharge, which is worse in the morning -itchy or painful
|
|
|
|
Therapeutic Management/ Nursing Care:
|
-bacterial is treated with antibiotic
|
|
|
|
What is Otitis Media?
|
Inflammation/infection of the middle ear
|
|
|
|
Who is at risk?
|
smokers in the house -bottle fed babies
|
|
|
|
Otitis Media and infant feeding methods
|
-Breastfed infants have a lower incidence than formula-fed infants. Breastfeeding may protect infants against respiratory viruses and allergy because breast milk contains secretory immunoglobulin Ig A, which limits the exposure of the eustachian tube and middle ear mucosa to microbial pathogens and foreign proteins. Reflux of milk up the eustachian tubes is also less likely to occur in breastfed infants because of the semivertical positioning during breastfeeding
|
|
|
|
What is a myringotmy?
|
-A surgical incision of the eardrum, may be necessary to alleviate the severe pain on Acute Otitis Media
|
|
|
|
Types of Head Injury: Concussion-
|
-most common, transient and reversible neuronal dysfunction, with instantaneous loss awareness
|
|
|
|
Types of Head Injury: Contusion-
|
visible bruising and tearing of cerebral tissue
|
|
|
|
What is Spina Bifida?
|
Myelomeningocele is a complex malformation of the spinal cord, nerve roots, meninges, vertebral bodies, and skin.
|
|
|
|
What is a neural tube defect?
|
NTDs constitute the largest group of congenital anomomalies that is consistent with multifactorial inheritance.
|
|
|
|
What is spina bifida oculta?
|
refers to a defect that is not visible externally. It occurs most commonly in the lumbosacral area (L5 and S1) SB occulta may not be apparent unless there are associated cutaneous manifestations or neuromuscular disturbances.
|
|
|
|
What is spina bifida cystica?
|
Refers to a visible defect with an external saclike protrusion. -The two major forms of SB cystica are Meningocele, which encases meninges and spinal fluid but no neural elements, and Myelomeningocele, which contains meninges, spinal fluid, and nerves
|
|
|
|
Is it possible to detect SB prenatally?
|
yes, fetal ultrasound and elevated concentrations of alpha-fetoprotein (AFP), a fetal specific gamma-globulin, in amniotic fluid may indicate presence of ancephaly or myelomeningocele.
|
|
|
|
Nursing Care:
|
sterile, moist covering with normal saline
|
|
|
|
Prevention:
|
the widespread use of folic acid of childbearing age is expected to significantly decrease the incidence of SB.
|
|
|
|
Nursing management of DVT includes
|
foot of bed elevated and bed rest
|
|
|
|
What is lightening and when does it usually occur…
|
when baby drops into pelvis, about 1-2 wks before delivery
|
|
|
|
The RN teaches pt. with diverticulosis to include what in diet…
|
increase fiber, increase fluids, and bulk laxatives
|
|
|
|
Name 2 to 3 causes of DKA…
|
infection, illness, stress
|
|
|
|
20. Quadriplegic with diaphoresis, flushed face, BP of 230/100, Pulse: 40, what complication should be suspected…
|
autonomic dysreflexia
|
|
|
|
A maternity cycle is divided into 3 periods, intrapartum begins and ends when..
|
onset of labor to delivery of placenta
|
|
|
|
Hemoglobin of 8.2 , what nursing care is essential…
|
assess for tachycardia, hypotension and O2 sat
|
|
|
|
What labs should be monitored with MI is suspected…
|
CK-MB, troponin- both elevated. Troponin is predictive of MI
|
|
|
|
.A woman pregnant with 2 girls, 1 boy, 1 miscarriage, what is G/P…
|
G 5, P 3
|
|
|
|
RN teaching adolescent with history of seizures about medicines should reinforce avoiding what with meds…
|
alcohol
|
|
|
|
4 s/s of hypothyroidism…
|
wt. gain, decrease in VS, constipation, decrease concentration, dry brittle nails
|
|
|
|
A common serious complication of rheumatic fever…
|
cardiac valve damage
|
|
|
|
What is the proper method to perform fundal check on a patient postpartum…
|
use 1 hand to support the lower portion of uterus
|
|
|
|
Following upper endoscopy, an essential, very important assessment of will include…
|
gag reflex prior to admin of anything PO
|
|
|
|
Mother entered 2nd stage of labor. Stage begins with complete dilation of the cervix and ends with…
|
delivery of the baby
|
|
|
|
To prevent reoccurrence of renal calculi, RN teaches…
|
maintain fluid intake (2000-3000)
|
|
|
|
. After removal of Wilm’s tumor what tx are required…
|
chemotherapy and radiation
|
|
|
|
3 chronic complications associated with DM…
|
retinopathy, PVD, CAD, neuropathy, renal disease
|
|
|
|
2 Risk Factors of glaucoma…
|
Family history, increased intraocular pressure, age (45-65
|
|
|
|
8 hours following delivery of baby, the assessment of fundus should be…
|
firm and at umbilicus
|
|
|
|
Pregnant woman asks about sexual activity, the nurse states only reason to avoid sexual activity would be…
|
vaginal bleeding
|
|
|
|
. Name 2 important complications after a heart cath that the nurse should be alert for…
|
bleeding and cardiac arrhythmias
|
|
|
|
Pt’s cervix is dilated 9cm and 80% effaced, membranes just ruptured, 1st intervention…
|
assess FHR and then assess amount and color of fluid
|
|
|
|
State 3 facts about colostrums…
|
slightly yellow, antibodies, high protein, high fat
|
None
|
|
|
.To assess AV fistula patency, the RN will…
|
feel the thrill, hear the bruit
|
|
|
|
Stages of vaginal discharge during postpartum
|
Rubra, serosa, and alba (know the length of each stage)
|
|
|
|
A client recalls smelling unpleasant odor prior to a seizure…
|
aura
|
|
|
|
4 s/s of hypoglycemia…
|
sweating, nausea, hunger, confusion, cool/pale skin
|
|
|
|
If a patient is experiencing laryngeal stridor and cramps in the hand, the RN suspects…
|
hypocalcemia
|
|
|
|
When comparing CVA with a TIA, the RN understands that….
|
TIA is intermittent while CVA is spontaneous
|
|