Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
169 Cards in this Set
- Front
- Back
|
How does the shape of our spine change from infant to adult?
|
infant is one big kyphosis called a primary curve (probably why they can't support themselves)
|
|
|
What are the lordotic curves that develop called?
|
secondary curves
|
|
|
what are apophyses? Give examples
|
bones in children that will eventually fuse with a parent bone.
examples are tubercles or apophyseal |
|
|
What is an apophyseal joint? Example?
|
a point where two bones join in the spine (example is where the girraffe's cheecks joint with the horns underneath)
|
|
|
What are epiphyses?
|
a growth plate already joined to the original bone
|
|
|
What is lumarization vs sacralization?
Which one is more of a problem? |

when the area between lumar and sacrum become more like the other (within 1 or two vertebrate)
sacralization is worse because you are locking the lumbar in the saccral fusion and limiting mobility. |
|
|
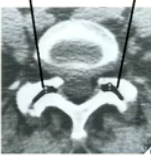
Show the neural arch and vertebral foramen
|
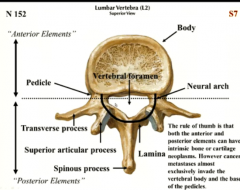
neural arch= black line
|
|
|
Where do the girraffe ears come off of? What are the ears called btw?
|
the laminae
they are articular processes |
|
|
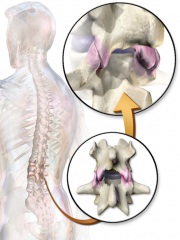
Where do metastases usually form? Why?
|
they can happen anywhere but go to the more vascular areas like the body and the base of the pedicles
|
|
|
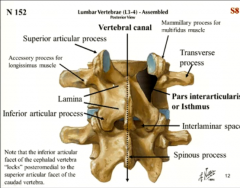
What is the area that goes from the ears to the cheek to make it a smooth transition called?
|
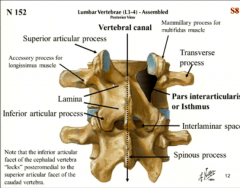
pars interarticularis (part between the articula)
or isthmus |
|
|
What does "isthmus" mean?
|
something connecting two structures (like a pedicle)
|
|
|
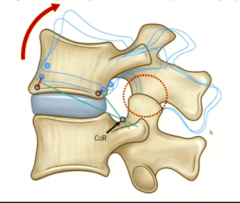
Show the difference between the pars interarticularis and the lamina
|
pars is more horizontal
|
|
|
What happens if this breaks?
|

spondylolithesis
|
|
|
define spondylolithesis
|
slipping of one vertebrate over the other (a bone problem)
|
|
|
What does the cervical vertebrate look like from the top?
|
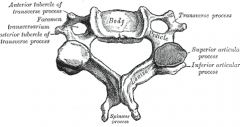
a bug alien
|
|
|
What happens if the pars articularis breaks bilaterally vs unilaterally?
|
bilat- top slips forward or back
uni- rotation |
|
|
What prevents slippage of vertebrae usually?
|
the orientation of the articular facets locking them in.
|
|
|
What common condition would create more force and slippage?
|
obesity
|
|
|
what action do the lumbar vs thoracic vertebrate like?
|
lumbar- f/e
thoracic- rotation |
|
|
What is the Zygapophysial joint?
|
the joint between the articular facets
|
|
|
What type of joint is it?
|
a real synovial joint with a capsule and synovial fluid and everything
|
|
|
What condition do you get with inflammation at this joint?
|
facet joint arthritis
|
|
|
What type of joint is between the vertebral bodies?
|
a cartilaginous symphysis joint
|
|
|
How much movement do they give? Why arer we able to mov our spine so much?
|
not much, but they addd up throughout the column
|
|
|
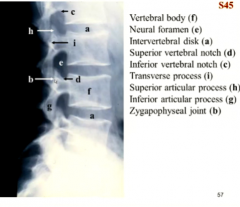
What is the intervertebral foramina bounded by in terms of boney parts?
|

posterior- vertebral body and discs
inferior- top of pedicle of vertebrate below superior- bottom high arch of ertebrate above anterior- apohyseal joints |
|
|
What are the girraffe's neck on bottom and top called?
|

superior and inferior vertebral notches
bottom and top of pedicles |
|
|
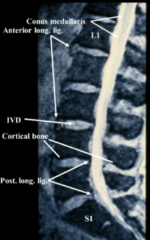
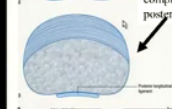
Is the anterior longitudintal ligament one big piece?
|
no, it stops at the discs
|
|
|
Which ligaments of the spine help guard against fexion vs extension?
|
ext- anterior longitudinal
flexion- all the ones behind the body |
|
|
What is different about the zygoapohyseal joints of the cervicals?
|
they are more round and flat
|
|
|
What is the advantages and disadvantages to this?
|
adv- more movements
disadv- more easily injures because not as stabilized |
|
|
WHat happens to the zygo joint from C1 to C7?
|
they transition to be more verticle and facing outward like thoracics
|
|
|
Are they completely horizontal? SHow this.
|
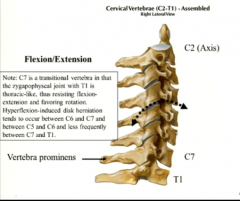
no they point down
|
|
|
What coupling motion in OMM does this explain?
|
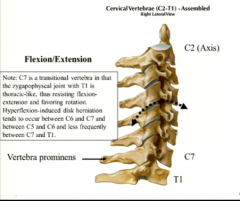
cervicals are always same side rotation and sidebending
|
|
|
At what part of the intervertebral foramen is the cervical disc at? Why is this important?
|
dead center in the foramen, which has implications in myelopathy
|
|
|
Where do you transition the orientation of the facets from thoracic to lumbar?
|
t10-t12
|
|
|
Which vertebrae has the hgihest number of fractures and why?
|
T12 because it is in this vulternable tranistion point. Don't have much protection in either.
|
|
|
Why does it make sense that thoracic vertebrae rotate and lumbars f/e when ribs prevent the rotation and abdomen allows the rotation?
|
you want to protect the spine as much as possible so this limits the free range of motion.
|
|
|
Why is L4-L5 the place for most slipped discs?
|
again, it's the transition region creation a lot of confused mvoement.
|
|
|
How does the vertebral foramen change from cervical to lumbar? Why?
Show a pic! |

cervical- oval and big
thoracic- small and roung lumbar- oval and less big it's the same as for the spinal cord |
|
|
What determine whether it is oval or round? What is this extra space called?
|
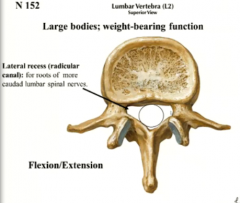
radicular canals or lateral recesses
it is room for thee lumbosacral and cervical enlargements of the anterior horns |
|
|
Why is there a HUGE lateral recess in the lumbar vertebral foramen?
|
because the spinal cord ends here and needs to provide all the LMN for the cauda equina
|
|
|
How can you imagine the topography of the sacrum from the shape of the lumbar?
|
it's crests and valleys are just like fused lumbar vertebrate
|
|
|
What holes does the sacrum still need to have?
|
vertebral foramen and anterior and posterior exits holes for the rami
|
|
|
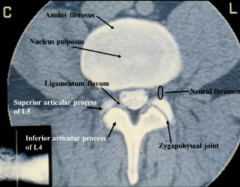
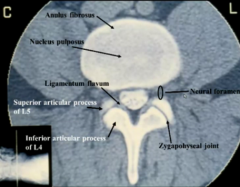
show how thick the annulus fibrosis is around the pulposus.
Is it the same thickness all around? Why does this suck? |
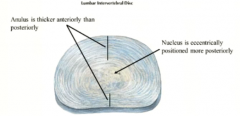
very thick all around
but thinner in the back which is bad because this is where herniations can affect the rami |
|
|
What is the consistency of the nucleus pulposa? how does it change as we age?
|
like toothpaste (semisolid)
it dries up as we age |
|
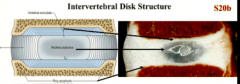
Real pic.
What is that blue part between the disc and the vertebral body? What is that boney protrusion of the body? What is the function of each? |
vertebral end plate- metabolic transiition between vascular body and avascular disc
and ring apophysis- borders the end plate and is a good disc anchor point |
|
|
What is pathologically significant about the ring apophysis?
|
it is the site of osteophyte formation usually and disc failure
|
|
|
What happens if you get end plate degeneration?
|
you also get disc degeneration
|
|
|
How is the vascularization diffeernt for kid's discs?
|
their discs are more vascular. We lose this as we age and rely on end plates.
|
|
|
What is the infectious downside to having an end plate?
|
we can get disc-itis from the vertebral bodies (osteomyelopathies)
|
|
|
What is different about how adults and children get discitis?
|
adults- have to arise from vertebral body infection
children- don'tt necessarily have to involve vertebral body |
|
|
How much of the vertebral body does the anterior longitudinal ligament cover?
|
the anterior 2/3rds (just like the anterior spinal artery)
|
|
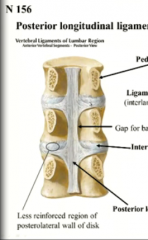
where is the posterior ligament attached? Why doesn't it attach to the back of the body?
|
to the vertebral discs. It is not attached to the back of body because that is where important vessels run.
|
|
|
What 3 things go through the intervertebral foramen? In what proporitons?
|
equally- nerves, fat padding, vessels
|
|
|
What is T1W and T2W?
|
types of MRI viewing
|
|
|
What is white and grey in TW2?
|
fluid is white (hyperdense)
fat is gray |
|
|
What color are the ligaments and why?
|
not much metabolic activity so few free protins so they give a hypodense (dark) signal.
|
|
|
Color of marrow vs outer bone? Why?
|
marrow- more pulpy and metabolically active so lighter than bone
|
|
|
Difference between a MRI and CT that makes MRI longer and more expensive?
|
CT you can pull out what you want from one set of info so you only need to scan once.
MRI- to get TW1 and TW2 you need more info from imaging so you have to scan a bunch of times using all different settings. |
|
|
Would the discs in an MRI show up light or ddark compared to the bodies?
|
light because they have some fluid
|
|
|
What about the spinal cord vs the CSF
|
spinal cord is grey because it has myelin
CSF is white because lots of protons in water |
|
|
How can you determine if there is a tendon or ligament tear on MRI?
|
they wil sgtart attracting fluid and cytokines and become more light.
|
|
|
What color is normal blood on MRI? Why?
|
holy ****, it's black because it moves so fast that the blood you ifused with magnet is already gone by the time the magnet bounces back
|
|
|
How do we fix this?
|
inject gallinium
|
|
|
SHOW A T2w
|
|
|
|
What is grey and white in T1W?
|
fat is white
fluid is grey |
|
|
SHOW T1W
|

|
|
|
mNEMONIC FOR t2w FAT color?
|
I 2 think that FAT is GRREEEYt!
|
|
|
From top to bottom, how do the nerve root length change? SHow.
|
they get longer and longer. in cervical it is at the same level as the horn.
|
|
|
How does the root traction from being so displace affect the vertebral notches as you go down?
animal mnemonic? |
the lower vertebrae have high vertebral notches because of the roots puliling traction.
the necks get higher and higher as you go down the column |
|
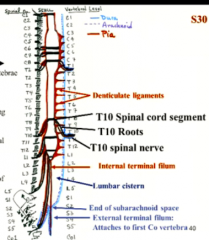
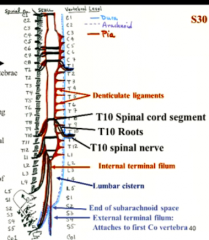
Notice the shape of the meninges and the levels of the denticulate ligaments. what creates the internal vs internal filum terminal.
What level does the CSF end? What about the FT? |
denticulate is C3-L1
internal FT- pia only external FT- all 3 meninges CSF ends at S2 Flium goes all the way to the coccyx |
|
|
What is the leptomeinnges? Meaning?
|
means thin.
This is pia and arachnoiod because they are thin |
|
|
What are packymeninges? Meaning?
|
means thick and grey like elephant skin
this is the dura matters |
|
|
What is the point of the denticulate ligaments? (2)
|
1. anchors the cord to the dura so it doesn't knock around (like a lateral filum terminale)
2. separates dorsal and ventral roots |
|
|
define a spinal cord segment
|
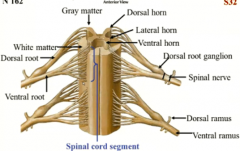
where a bnch of roots come out
|
|
|
If you fx t12, what spianl root is affected and why? (sotry of cheerleader)
|
L5 because roots are all jammed p as you go down the cord.
(cervicals you should check one level up just in case, but more as you go down) |
|
|
what advanage do you get with the vertebral arches being higher at the lumbar?
|

this is where most disc herniations occur due to pressure, so it's good that there is a spacious separation between spinal root and disc
|
|
|
What does the intervertebral foramen look like from a side mri?
|

like an upsidedown teardrop
|
|
why does the vertebral process looke like it is floating?
|
this is a section through the disc so we dont see the pedicles
|
|
|
is fat more or less dense than soft tissue?
|
less
|
|
which verterbrate is on the top vs the bottom? How did you deduce this?
|
remember you are looking from the feet first of all!
check to see if the angle of articultion would allow for rotation smaller lookling one is the horn of the lower vertebrate bigger one is the "cheek" and nose of the higher vertebrate |
|
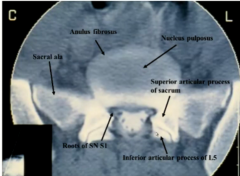
what are we looking at?
|
sacroiliac joint
|
|
|
What shape do the vertebral bodies have axially?
|
like a horseshoe (a blunt one)
|
|

|
|
|

label- where would you put the needle in an LP?
What do the vertebrate on an AP Xray look like? |
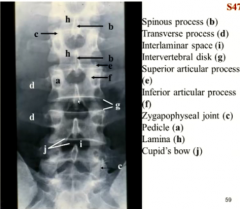
in i- the interlaminar space
an owl. the eyes are the pedicles coming out at you |
|
|
What is responsible for cupid's bow?
|
the fact that the ring apophysis is more there laterally and turns up further on the posterior side of the disc
it's protecting the end plate |
|
|
What pathology do you have with a disturbance in cupid's bow?
|
a rib fracture (I dunno)
|
|
|
show a side view of the ring apophysis responsible for cupid's bow.
|
|
|
|
Do you see cupid's bow everywhere in the column? WHy?
|
only in lumbar because their end plates are larger
|
|
|
why do you use x ray for spine?
|
it is cheap and can tell you if something is moving the bones
|
|
|
rule for interpedicular distance to screen out pathology?
|

line between owl's eyes should be smooth and no less than 20 mm.
|
|
|
How does cupid's bow progress from L1 to L5?
|
get bigger and bigger.
|
|
|
What are two reasons why the transverse processes sppear to be floating on their own?
|
1. fracture
2. they are apophysis and may never have fused |
|

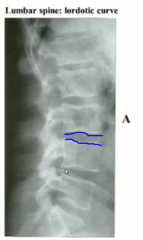
name these lines
|
bodies- vertebral
along the spinous processes- spino |
|
|
What does it mean if you find step offs in those lines?
|
spondylolisthesis (fracture of pars interarticularis)
|
|
|
What should the width between the spinolaminar and posterior vertebral lines be in the cervicals vs lumbar?
|
cervicals- 13 mm
lumbar- 15mm |
|
|
What is the dx if it is less than that?
|
spinal stenosis
|
|
|
What angle does the pt have to be in for an xray to evaluate the pars interarticularis for fx?
|
posterior oblique (catch it AP but pt is rotating to the side)
|
|
|
What is the normal sign you should see in a oblique spinal AP XR? (show it)
|
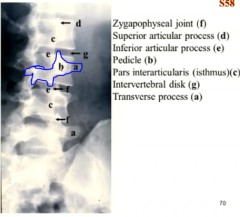
scotty dog sign
|
|
|
What do you know is intact if there is a scotty dog sign?
|
the pars interarticularis
|
|
|
What part of the scotty dog is this? What does it look like if there is a break?
|
the neck. they have a dark collar if there is a break.
|
|
|
How do you name if it is a left or right oblique view?
|
whichever pars articularis is closer to you.
|
|
|
What may be wrong if you stop seeing the pedicles? (eyes of the owl)
*this may be very subtle but mean a lot in XR |
the pedicle could be being eaten away by metastatic disease
|
|
|
What are two ways to see if your spine is rotated in AP XR?
|
Moe pedicle method (better because pedicles are sharper)- see if pedicles are lined up
Cobb spinous process method- line up spinous processes |
|
|
What is dysraphism? WHat spinal deficit is it associated with?
|
incomplete closure of neural tube
spina bifida |
|
|
What other lower spinal abnormality do you get with spina bifida?
|
tethered spinal cord
|
|
|
What dysfunction do you get in this filum terminale synrome? dysfunction of peroneal muscles and urinary and bowel incontinence
|
dysfunction of peroneal muscles and urinary and bowel incontinence
|
|
|
what happens to the meninges as the spinal nerves exit?
|
they exit with the nerves and make the endo/perinerurium CT around the nerves
|
|
|
In tha cadaver, the the arachnoid where is normally is? why?
|
no, it has colapsedonto the pia because there is no more CSF
|
|
|
What are two tests you can do for meningitis?
|
Kernig's and Brudzinski's test
|
|
|
What are these two tests trying to look for essentially?
|
if there is pain when the meninges are stretched.
|
|
|
What is Kernig's vs brudzinski's? Mnemonic?
|
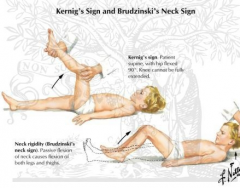
K for kick
Kernig- pt can't extend leg while hip is flexed 90 degrees Brudzinki's- contract legs if neck is flexed. |
|
|
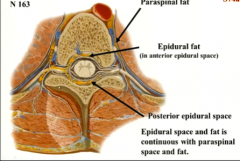
If you do an epidural... where are you injectiong the anesthesia and how does it get to the nerves?
|
in the epidural fat where it the lidocaine will dissolve through the meninges to the nerves
|
|
|
for lumbar epidural, where do you iinject anesthetic?
|
in the subarachnoid
|
|
|
What precautions do you need to take for this?
|
raise the pt's head so it doesn't anesthetize the medulla
|
|
|
show the epidural fat.
|
|
|
|
What is Batson's vertebral venous plexus? Why is it special in spreading infection and metastases?
|

the venous pleuxus draining the spinal cord. it has no valves so things spread easily through them
|
|
|
What is a common infection that can spread to cause infection of the spine?
|
pyelonephritis (the veins also drain the pelvis)
|
|
|
What are two names for infection of the vertebral bodies?
|
septic spodylitis
bacterial osteomyelitis |
|
|
Why do old people get tussive syncope?
|
cough forces blood to veins, veins impinge on dura, CSF pressure raise, can cutt of stuff in the brain with a lot of coughing
|
|
|
What veins of the batson's plexus runs behind the posterior longitudinal ligament?
|
basivertebral vein
|
|
|
Show how the basivertebral vein infiltrates the vertebral body.
|
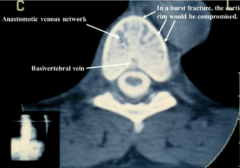
like an oak tree
|
|
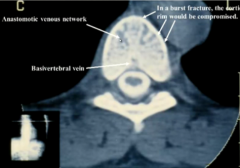
So what is the dark spots in the vertebral body?
|
anastomoses of the veins
|
|
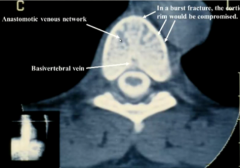
How do you know this sin't a burst fracture?
|
the cortical rim is intact
|
|
|
Where does the anterior spinal artery get it's supply on the top and bottom of the spinal cord.
|
upper 1.3rd- vertebral arteries
lower 2/3rds (T10 down)- artery of adamkiewiez |
|
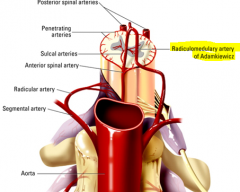
where does the artery of adamkiewics come off of? What vascular pathology would cause it to lose perfusion?
|
the aorta feeding segmental arteries via the spinal rami bundles.
a dissecting aortic aneurysm can compress it |
|
|
Would the whole spinal cord be infarcted in a artery of amdemkiewicz block?
|
no the posterior have their own circulation.
|
|
|
Show what an aortic dissection would look like and which part of the back would be affected.
|
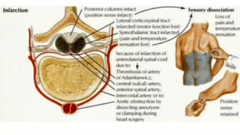
loss of pain and temp and motor control, but not proprioception down from the infarct.
|
|
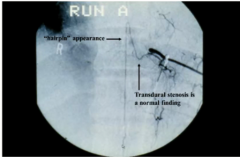
why does the artery of adamkiewicz have a hairpin appearance? What meninges does it need to get through?
|
it needs to follow the nerve root path. Since it originates from the aorta, it must pierce through the dura to get to the anterior spinal artery. (this causes a normal "transdural stenosis"
|
|
|
Is the artery of adamkiewicz bilateral? Why?
|
no it is only to the left cause that is where the aorta is
|
|
|
dissect dys-rapheism
|
dys- abnormality
raphe- seam abnormality in the seam |
|
|
Is spina bifida occulta alway with a tuft of hair?
|
no, but there is some sort of stigmata- it can be a dimple or a port wine stain or pad of fat- this is because of the signalling error
|
|
|
What is neural placode or raphischisis?
|
where the neural tube is open in myelomeningiocele.
raphe-seam schisis- split open |
|
|
What kidney disease can be caused by myelomenigiocele?
|
pyelonephritis
loss of control at bottom of the spine--> no UVJ closing reflex--> infection of kidney |
|
|
What brain abnormality is associated with menigomyeloceles? What implant do they need?
|
CHIARI MALFORMATION
less closure of formane magnum as well ---> brainstem sits too low --> hydrocephalus from blocked CSF ---> must install a shunt |
|
|
What is lemon's sign? What does it indicate and how accurate is it?
Show it |
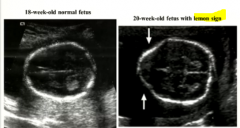
it's the shape of the baby's head in a US before 6 months gestation. It's very accurate for spina bidifa and this Chiari malformations.
|
|
|
What is associated with spina bifida occulta?
|
filum terminale syndrome and lack of peroneal and baldder con trol
|
|
|
Dissect diastemato-myelia
|
diastemato- split
myelia- cord |
|
|
NOW WE TALK ABOUT DISC HERNIATION!
|
MY TYPE OF THIGN!
|
|
|
WHAT IS CONCORDANT PAIN?
|
PAIN upon spinal surgery or anesthsia to let you know you hit the right spot
|
|
|
What is different about the aanulus of the cervical discs?
|
they don't have anterior ring
|
|
|
What spinal levels innervate the disc
|
the one on the same level and the one below, resulting in referred pain with disc disease
|
|
|
What are 2 natural causes of degenerative disc disease?
|
1. loss of fluid in disc
2. cracks in the annulus leading to herniation |
|
|
What are some snowballing consequences of degenerative disc disease?
Show it |
things like the apophyseal joint will start rubbing up on each other look like and form osteophytes or cysts of the synoviial jjoints.
|
|
|
What is the DJD vaccuum phenomenon?
|
a common bubble in the disc left from a dried out pulposus
|
|
|
What is the zygoapophyseal joint innervated by?
|
the current nerve, but mostly the nerve ABOVE
|
|
what is this?
|
vaccuum phenomenon of zygoapophyseal joint
|
|

What is hourglass sign?
imagine what the vertebrate look like here from a top view. |
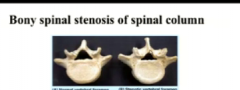
spinal stenosis from osteophytes
(notice no more horseshoe shape) |
|
|
Which ligaments can osteophytes grow on?
|
ligamentum flavun and posterior longitudinal ligament
|
|
|
What is the long vs short term consequence of spinal stenosis? Show pic.
|

short- can fall and poke bones into spinal cord
long- constantly compressed nerves will degenerate |
|
|
Show what kind of posture someone with lumbar spinal stenosis can have? why?
|
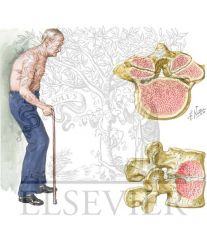
a kyphiosis and bent kneews as they try to shorten the cord by straightneing the lumbar lordosis
|
|
|
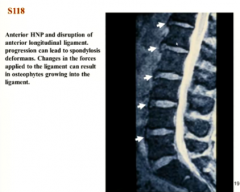
is herniation only out the back?
|
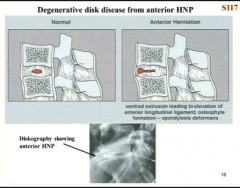
no it can bulge forward or into the vertebral bodies and cause ostephytes there too
|
|
|
Show an MRI of anterior herniation.
|
|
|
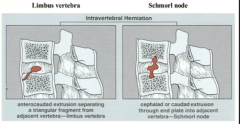
These are some vertebral body disc herniations. Do they cause trouble? What could they look like on an xray?
|
they don;t cause pain, but they can look like metastatic bone disease for fx on xr
|
|
|
Who is prone to getting schmorl nodes? WHy?
|
people with osteoporosis because the cortical bone of the vertebral body is lost
|
|
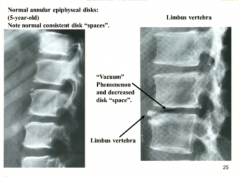
What can look like a limbus vertebra? (dis herniation)
|
the apophysis of young children that haven't fused yet
|
|
|
show the avulsion fx that limbus vertebrae can look like.
|
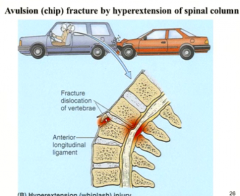
from whiplash
|
|
|
what is an intraspinal herniation?
|
herniation that actuually goes to the spine
|
|
|
what is the most common type?
|
posterolateral
|
|
|
what is th clinical "rule" of posterolateral disc herniation?
|
the nerve affected is named for the vertebrate below it. (works only since majority are in lumbar and cervical)
|
|
|
what side do people lean when they have a disc herniation?
|
usually to the other side to pull the root out from the herniation
|
|
|
what is a test for herniation of cervicals?
|
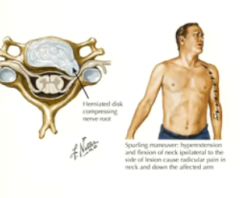
spuling manuever to see if they get radicular pain to one sidewhen the herniation gets exacerbated
|
|
|
what spine abnormality is usually present to correct for a thoracic kyphosis?
|
a compensatory cervical lordosis to keep the head straight
|
|
|
how much calcium can a woman lose during pregnancy?
|
15%, but this is not the strutural part of the vertebrate?
|
|
|
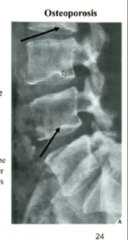
What do vertical striations and empty box sign indicate on vertebral bodies?
how do you identify empty box> |
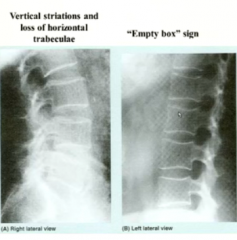
loss of bone in osteoporosis (empty box is worse)
empty box looks like the outside cortical bone is brighter comparatively |
|
|
What injury can arise as a result of osteoporosis of the spine?
|
anterior compression deformities leading to kyphosis
|
|
|
What is the codfish siign?
|
when the disc expands into the vertebral bodies to look like the mouth of a codfish.
indicates the bones are soft from osteoporosis |
|
|
What do DEXA scans tell you?
|
how dense your bone is compared to a 45 year old female.
if you have osteoporosis or osteopenia |
|
|
Which two bones do the DEXA scan look at?
|
lumbar and femoral neck
|