![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
424 Cards in this Set
- Front
- Back
|
Anatomy + function of the pharynx:
a) Throat= b) walls composed of c)function of the pharynx d) communicates with: (5) e) muscular mechanisms guarding opening |
a) pharynx + larynx
b) bony + fibromuscular walls c) pathway for air + food, pharyngeal mm control the pharyngeal phase of swallowing, sneezing/coughing, vomiting, speech d) nasal chambers, pharyngotympanic tubes, oral cavity, larynx + oesophagus e) palatal+salpingopharyngeal muscles at the pharyngeal ostium of the eustachian tube, soft palate + sphincter muscles of the nasopharyngeal isthmus, base of the tongue and palatoglossal folds, aryepigllotic folds forming the first of the triple sphincters of the larynx, the cricopharyngeal sphincter |
|
|
Sensory receptors of the pharynx (3)
|
somatic sensation- touch, pain, temp, special taste
afferent receptors- reflexes of swallowing and vomiting sensation in dehydration is referred to pharynx |
|
|
Divisions of the pharynx
|
nasopharynx
oropharynx hypopharynx |
|
|
Nasopharynx:
a) postero/superior aspect b) inferior limit c) contents |
a) skull base + clivus
b) horizontal like from the hard palate to the posterior wall of the nasopharynx c) adenoidal tissue, eustachian tube orifice (connects to middle ear) |
|
|
Oropharynx:
a) upper limit b) anterior seperation c)contents |
a)horizontal line from posterior hard palate and hyoid bone posteriorly
b)anterior faucal pillar of the palatine tonsil + circumvillate papillae which separates posterior 1/3 of the tongue c)soft palate, uvula, anterior and posteriorfaucal pillar + palatine tonsil + posterior 1/3 of tongue |
|
|
Hypopharynx:
a)lower limit b) 3 regions c) functions (2) |
a) cricoid cartilage
b) piriform foassae, postcricoid space, posterior pharyngeal wall c) channel for food, resonance chamber for voice production |
|
|
Divisions of the larynx (3)
|
glottis
supraglottis subglottis |
|
|
What is the glottis?
|
region between upper and lower limits of the vocal cords, including the anterior and posterior commisures
|
|
|
supraglottis
|
from the vocal cords to the level of the hyoid bone
|
|
|
subglottis
|
region below the vocal cords to the level of the cricoid cartilage
|
|
|
functions of the larynx
|
protection of the lower airway
generation of cough + expulsion of matter from airway production of sound vibration for voice |
|
|
cricoid cartilage
|
lower anatomical landmark of the larynx
seperates pharynx from oesophagus and larynx from trachea adults: C6, child slightly higher |
|
|
Glottic larynx contains:
|
true vocal cords
anterior commisure |
|
|
Supraglottic larynx contains
|
epiglottis
false vocal cords ayepiglottic folds arytenoid cartilage |
|
|
Epithelium of the larynx
|
ciliated columnar epithelium except over vocal cords which is covered in squamous epithlium
|
|
|
Voice
|
energy causes mucosa of the ventricular folds to vibrate, vocal fold close and vibrate (adducted position) to produce sound
|
|
|
Vocal fold attatchment
|
anterior) thryoid cartilage
posterior) arytenoid cartilage |
|
|
intrinsic laryngeal muscles function
|
1) abduction for respiration
2) adduction for lower airway protection, coughing and phonation |
|
|
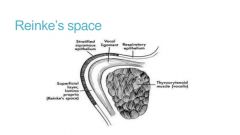
Layered structure of the vocal folds (3)
|
1)epithelium= surface layer
2Reinke space= gel layer between epithlium and ligament allowing oscillation of the epithelial layer supero-inferiorly 3)vocal ligament |
|
|
vocal muscles
|
superficial vocalis mm
deep thyroarytenoid mm |
|
|
Sound production:
a) speech frequency b)measurement of sound intensity + determination c)vowel production by d) consonant production by e) normal voice production requires |
a) adult male= 110 hz, female= 190 hz, child=300 hz, soprano=1000 hz
b) dB, determined by subglottic pressure c) vocal cord vibration d)air 'squirted' through narrowings in the vocal tract e) coordinated vibration of the vocal folds, adequate subglottic pressure from lungs, shaping of the vocal tract and control by brain |
|
|
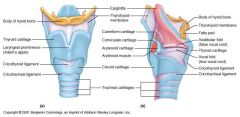
larynx anatomy
|
|
|
reinke's space
|
|
|
Definitions in voice disorders:
a) dysphonia b)dysarthria c)dysphasia d)hoarseness |
a) impairment of voice/difficulty speaking (hoarseness)
b)imperfect articulation of speech - disturbance of muscular control or incoordination c)sensory=impairment of speech/verbal comprehension, expressive= impairment of speech and verbal production (brain injury) d)percieved rough, harsh or breathy quality to voice |
|
|
Questions to ask in voice disorders:
a) risk b)other c) voice use/abuse/lifestyle d)duration of problem |
=smoker, difficulty breathing/swallowing, family history of throat/laryngeal cancer, pain or reffered otalgia, neck lump -> refer on '2 week cancer wait'
b) URTI symptoms c)occupation, social, tea/coffee/cola/water, do they eat regularly late at night, spicy/fatty foods, hertburn/indigestion/acid regurg/throat clearing/coughing/choking episodes d) if >6/52 refer for laryngeal examination, if risk of cancer '2 week wait' |
|
|
ways to visualize the larynx
|
flexible endoscope (fibreoptic)- inspection from nasal cavity to larynx
rigid endoscope - for examining fold structure and function stroboscopic light- allows observation of mucosal motion |
|
|
Types of voice disorder
|
structual/neoplastic
inflammatory neuromuscular muscle tension imbalance |
|
|
Structtal/neoplastic causes of voice disorders:
a)benign b)malignant |
a) nodules, polyps, Reinke's oedema, cysts
b)carcinoma |
|
|
inflammatory causes of voice disorders:
a)infectious b)non-infectious |
a)viral/bacterial/fungal
b)Extra-oesophageal reflux, allergies (rare) |
|
|
Neuromuscular causes of voice disorders:
a) underactive b) overactive |
a) recurrent laryngeal nn palsy, myaesthenia(rare)
b)spasmodic dysphonia (rare) |
|
|
Muscle tension imbalance causes of voice disorders:
a)primary b)secondary |
a)vocal demands/strain, occupational with inadequate vocal skills, psychogenic-anxiety/conversation dysphonia/puberphonia/mutational voice disorder, presbylaryngis, gender identity
b)inflammation from post infection, strucutal/neoplastic, neuromuscular, breathing disorders, postural abnormalities, congenital laryngeak anatomical abnormalities |
|
|
Laryngeal carcinoma- symptoms + signs
|
- consider in pts with persistent hoarseness >6 weeks
-hoarseness/change in voice, unexplained neck lump, pain in head/neck region, referred otalgia (normal otoscopy), difficulty swallowing, inspiratory stridor, haemoptysis - raised thickened, irregular mass with leukoplakia (white patch) and redness -airway narrowing +/- vocal cord fixation, cervical lymphadenopathy on examination |
|
|
larygneal carcinoma treatment
|
partial or total laryngectomy
radiotherapy |
|
|
nodules - 'singers nodes'
a) causes b)symptoms + signs c) treatment |
a) voice abuse, shouting, talking above background noise, reflux, boys=girls, adults <40 greater incidence in women
b)husky voice that worsens with use, loss of higher range, perilaryngeal discomfort, bilateral swellings in mid-membranous vocal fold giving hourglass appearence c)voice therapy surgical resection if unresponsive |
|
|
vocal polyps:
a)causes b)symptoms c)signs d)treatment |
a) shouting when suffering with a cold or reflux, men>women
b)husky voice worsening with use, may be deeper, voice cuts out during speaking, choking episodes if very large c)unilateral grey/haemorragic swelling in mid-membranous portion of vocal fold, smooth edge d) surgical excision,edical treatment of reflux with PPI/alginates, voice therapy, excision may be needed to exclude malignancy |
|
|
Reinke's oedema:
a)causes b)symptoms c)signs d)treatment |
a) smoking, a lot of talking, reflux
b) deep pitched gravelly voice- women mistaken for men on phone, choking episodes if severe c) usually bilateral, grey/erythematous swellings along whole of membranous portion of vocal fold d)stop smoking, surgical reduction of polypoid swelling, medical treatment of reflux, voice therapy |
|
|
vocal cysts:
a)causes b)symptoms c)signs d)treatment |
a) unknown, some develop after inflammation, some congenital, 2 types= mucous retention cysts or epidermoid cysts, men=women
b) husky voice, pitch break, loss of range of voice, increased effort to produce voice c)unilateral nodular swelling or localised bulge or stiffness of vocal fold d) voice therapy for reduction of secondary muscle tension, surgical excision |
|
|
Laryngitis causes:
|
viral- URTI, recurrent respiratory papillomatosis (RRP) due to HPV
bacterial-rare fungal- candida secondary to steroid inhalers/immunosuppression |
|
|
larygnitis- symptoms
a) acute viral/bacterial b)fungal c)RRP |
a)hoarse/croaky voice, aphonia if severe, pain on using voice, coughing or swallowing, irritant paroxysmal coughing, other symptoms of URTI
b)same as above without URTI c)affects infants and children who tend to be aggressive, severe dysphonia, airway problems, adults less aggressive but dysphonia |
|
|
laryngitis -signs
a)viral/bacterial b)papillomas c) candida |
a)erythematous/sloughy vocal folds
b) 'jelly tots'- multiple, raised erythematous lesions on the vocal folds and anywhere in the larynx c) white spots of leukoplakia |
|
|
laryngitis- treatment
a) acute viral/bacterial b)RRP |
a) self limiting: voice rest, analgesia, fluid hydration, steam inhalationm, cough suppressants, occasionaly abx needed
b)surgical excisions with laser or microdebrider |
|
|
Non infectious laryngitis causes:
|
extra oesophageal 'silent' reflux
allergies (rare) |
|
|
Non infectious laryngitis symptoms:
|
variable huskiness
voice worsens with use loss of higher range of voice associated throat symptoms: chronic throat clearing, cough, excessive mucous in the throat, choking episodes, globus sensation, difficulty swallowing food or pills (no true dysphagia) - only 40% have heartburn (silent) |
|
|
Non infectious laryngitis signs:
|
general erythema
oedema of vocal folds + larynx |
|
|
Non infectious laryngitis treatment:
|
vocal hygeine and dietary advice
PPI -2 X daily before breakfast and evening meal for a min of 2 months +/- alginates and H2 antagonists |
|
|
Neuromuscular voice disorder- Recurrent laryngeal nerve palsy or paresis: causes:
|
- miscellaneous=35%
- surgical trauma=23% (10% thyroidectomy) - malignant disease =22% (Ca bronchus- 10.6%, Ca thyroid-3.5%, Ca oesophagus- 1.8%) -idiopathic- 16% - neurological disorders- 4% |
|
|
Recurrent laryngeal nerve palsy or paresis: symptoms
|
- weak voice
- tires on prolonged talking - perilaryngeal discomfort - choking with fluids - higher pitched voice - diplophonia (two tone voice) - weak 'bovine' cough - Typical history: onset related to specific event |
|
|
Recurrent laryngeal nerve palsy or paresis: signs
|
- Immobile vocal cord: left side (75%), right side (15%), both sides (10%)
- listen to voice -listen to cough - check for other cranial nn lesions |
|
|
Recurrent laryngeal nerve palsy or paresis: investigations:
|
-CXR: exclude mediastinal mass
- CT scan: skull base to mid thorax- check for lesions along path of nerve - Ba swallow- of oesophageal lesion or aspiration suspected |
|
|
Recurrent laryngeal nerve palsy or paresis: treatment
|
None- await spontaneous recovery (up to a yr)
voice therapy- encourages compensation Vocal cord medialisation: injection (materials: synthetic polymer, collagen, autologous fat, fascia, hydroxyapatite), thyroplasty (laryngeal framework surgery- implant placed in cartilage alongside vocal cord to push cord closer to the middle) |
|
|
Muscle tension imbalace (dysphonia)- abnormal biomechanics:
Primary causes |
Excessive tension of the laryngeal muscles/imbalance of pull (synergists and antagonists)
- multifactorial aetiologies: stress, anxiety, depression, conversion disorders, neck/back problems, poor vocal hygeine, lifestyle/dietary |
|
|
Muscle tension imbalace (dysphonia)- abnormal biomechanics:
Lifestyle factors- primary cause: |
- talking above background noise for a long time
- having to project voice for long periods - working in dusty, smoky, noisy environments or where poor acoustics - not drinking enough fluids: water - too much tea, coffee, cola - eating late at night, large fatty meals - poor acoustic environments for working |
|
|
Muscle tension imbalace (dysphonia)- abnormal biomechanics:
secondary causes: |
Excessive tension required to overcome a deficiency in the voice producing mechanism- poor respiratory function, structural defect of vocal fold, nasal blockage affecting resonance
|
|
|
Muscle tension imbalace (dysphonia): symptoms
|
- variable hoarseness/huskiness- worsening with use
- may be deeper or higher than expected for age and sex - voice unstable, perilaryngeal soreness, dryness/uncomfortable sensation in throat |
|
|
Muscle tension imbalance (dysphonia): signs
|
-voice may be croaky/husky/breathy/bizarre/aphonic (no voice)
-variable voice quality (sometimes normal) - cough often normal, even when voice aphonic - vocal folds normal in appearance and movement -> may be constriction of the false cords or sphincteric closure where vocal folds disapear from view below false cords |
|

|
vocal cords:
true cords false cords aryentoid cartilage |
|
|
Muscle tension imbalace (dysphonia): treatment
|
vocal hygiene + lifestyle advice
voice therapy address underlying causative factors |
|
|
Tonsilitis: causes-
|
Commonly viral
Bacterial: group A beta haemolytic streptococci, streptococcus pneumonia, haemolytic influenza, |
|
|
Tonsilitis: symptoms
|
severe pain for >48hrs on swallowing
pain referred to ears headache- children may have abdo pain |
|
|
Tonsilitis: diagnosis
|
patient feels ill, pyrexial, sore throat, enlarged tonsils, white or yellow slough on tonsil surface, lymphadenitis, enlarge jugular digastric glands
|
|
|
Tonsilitis: treatment
|
hydration and analgesia, antibiotics of questionable benefit- usually co-amoxiclav, tonsillectomy for recurrent cases
|
|
|
Requirements for tonsillectomy for recurrent cases:
|
2 year or greater history of 4-5 attacks per year
|
|
|
Tonsilitis: complications
|
Peritonsillar abscess (Quincy) should be drained, parapharngeal abscess life threatening therefore urgent referral
|
|
|
Peritonsillar abscess (Quincy)- what?
|
complication of tonsilitis/infectious mononucleosis, consists of pus between tonsillar capsule and lateral pharyngeal wall
|
|
|
peritonsillar abscess- organisms:
|
strep pyogenes, staph aureus, h. influenzae, anaerobes
|
|
|
Peritonsillar abscess history:
|
severe throat pain (may be unilateral), fever, drooling of saliva, foul smelling breath, swallowing painful, trismus, 'hot potato voice', earache, neck stiffness
|
|
|
Peritonsillar abscess- management:
|
-Needle aspiration, incision and drainage- quincy tonsillectomy- SURGERY ESSENTIAL
-Iv abx: penicillin, cephalosporins, amoxicillin + clauvanic acid, cindamycin |
|
|
Tonsillitis- differential diagnosis:
|
- acute pharyngitis (viral or bacterial)
- infectious mononucleosis (usually young adults)- slough on tonsil is adherent, long-lasting lethargy + enlarged spleen |
|
|
Large tonsils
|
-sizes vary biologically
- large if causing functional symptoms: dysphagia, snoring |
|
|
Large adenoids
|
Adenoids regress with age, pathological enlargement obstructs nasal secretions pathway into pharynx, drips down nose causing anterior vestibulitis, obstructs nasal airway
adenoidectomy: for sleep apnoea/snoring, recurrent glue ear (bacterial reservoir) |
|
|
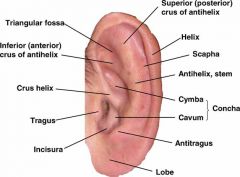
outer ear |
|
|
Otitis media with effusion/glue ear/secretory otitis media- disease of what part of ear? |
Disease of the middle ear mucosa from poor ventilation |
|
|
Glue ear (OME) results in- |
sterile collection of fluid in middle ear cleft (mucus glycoproteins,mucins + serous fluid), causing a conductive deafness of 10-40dB and a flat tympanogram, yellow discolouration of the tympanic membrane |
|
|
Glue ear affects |
children- 70-80% following an URTI, cleft palate, downs syndrome and mucociliary function disorder childrenb most susceptible |
|
|
Glue ear outcome |
Normally spontaneous resolution, review @ 3/12, 50% will improve, if glue ear persists insert tympanotomy tube (grommets) to aerate middle ear, antibiotics have a marginbal effect- decongestants and antihistamines serve no benefit |
|
|
Glue ear decision to treat based on: |
adverse effects of hearing loss, social + educational speech deficits, repeated attacks of acute otitis media or development of ear drum sequalae. Adenoidectomy may reduce recurrence risk but isn't performed at first insertion |
|
|
Unilateral glue ear in adults- exclude: |
Carcinoma of the postnasal space causing Eustachian tube orifice obstruction |
|
|
Grommet extrusion |
Sponanteous: on average 9 months can persist for 2 yrs |
|
|
Complication of recurrent glue ear |
thinning of tympanic membrane, retraction pockets, collapse of membrane. 20% children require re-insertion of grommets |
|
|
Acute suppurative otitis media: what? |
bacterial infection of the middle ear, pus forms, inflamed tympanic membrane bulges outwards (painful), tympanic membrane can rupture and pus and blood drain to EAM |
|
|
Time taken for tympanic membrane to heal after rupture |
4-5 days |
|
|
Acute suppurative otitis media:: symptoms |
otalgia + relief on rupture of TM, conductive deafness, pyrexia, tenderness over the mastoid bone, red bulging tympanic membrane or mucoid discharge in EAM if membrane has ruptured |
|
|
Bacteria causing Acute suppurative otitis media: |
strep pneumoniae, h.influenzae, morxella catarrhalis, group a streptoccoi, staph aureus |
|
|
Acute suppurative otitis media: treatment |
Analgesia, First line-co-amoxiclav (augmentin, myringotomy if conditions fails to resolve/ facial nn palsy.complications |
|
|
myringotomy |
incision in the tympanic membrane to relieve fluid build up in the middle ear |
|
|
Acute suppurative otitis media: complications |
brain absces- potentially fatal |
|
|
cholestaetoma |
protrusion of meatal skin into the middle ear |
|
|
cholestaetoma-aetiology: |
protrusion of meatal skin into the middle ear produces keratising squamous epithelium, anaerobic bacteria colonoise and produce a foul smelling purulent discharge |
|
|
cholestaetoma-symptoms: |
foul smelling discharge, conductive hearing loss, attic retraction filled with squamous debris, discharging attic perforation |
|
|
cholestaetoma-complications: |
cholesteatoma erodes through orricles causing conductive deafness of 50db or more, protrusion to semicircular canal causing vertigo, into the facial nerve canal causing facial palsy, into the cochlear causing sensorineural deafness, through the roof (tegmen) into brain causing intracranial abscess/sepsis, into the sigmoid sinus causing it to thrombose |
|
|
cholestaetoma:treatment |
suregery-remove cholestaetoma sac through mastoid surgery |
|
|
retraction pockets |
indrawing of the tympanic membrane, self-cleansing, if debris accumulates becomes cholesteatoma |
|
|
tympanosclerosis |
calcification of a collagenous scar from previous infection/trauma, may be asymptommatic, may cause conductive deafness ~50dB and obliterate the middle ear |
|
|
otosclerosis -what |
familial dominant condition with incomplete penetration oten presents in pregnant women- spongy bone formation around the oval window and growth to fuse with the stapes causing a conductive deafness, usually bilateral causing tinnitus and positional vertigo |
|
|
otosclerosis- treatment |
stapedectomy=replacement of stapes with prosthesis or hearing aid to return hearing to normal- pts choice, surgery carries small risk of sensorineural deafness |
|
|
Chronic suppurative otitis media- what |
disease of middle ear mucosa- repeat infections, mucosa hypersecretory and hypertrophic, micro abscesses, inflammatory cell infiltrates +/- perforation, chronic odourless discharge from clear to mucopus, conductive deafness |
|
|
Chronic suppurative otitis media- treatment |
Short term: antibiotics and steroid ear drop to help settle infection- middle ear disease- myringoplasty, mastoid involvement (confirmed by CT) - cortical mastoidectomy + myringoplasty beware of intracranial sepsis |
|
|
Trauma to head- results in |
skull base fractures |
|
|
haemotympanum -what |
blood in middle ear, appears red/blue, conductive loss ~30dB |
|
|
haemotympanum- treatment |
spontaneous resolution- blood reabsrobed + healing of TM, may be CSF leak which usually heals spontaneously and can cause 'watery rhinitis' |
|
|
ossicular fracture/disruption- symtpms |
hearing loss ~50dB, non resolving, explore when blood resorbed, if delayed the displaced ossicles may be resorbed temporal bone fractures
|
|
|
congential conductive deafness |
rare genetic cause |
|
|
Intracranial complication of temporal bone infection |
Brain abscess- pus + region of encephalitis in cerebrum or cerebellum, otogenic brain abscess- solitory lesion in temporal lobe or cerebellum |
|
|
otogenic brain abscess -epidemiology |
can occur at any age, 1/3 have ENT cause in children, originates from venous thrombophlebitis |
|
|
otogenic brain abscess- mortality |
10% |
|
|
otogoneic brain abscess- organisms |
most common = gram-ve bacilli ,aerobes, anearobes, mixed cultures |
|
|
intracranial brain abscess- symptoms |
systemic effects of infection- malaise, pyrexia, raised intracranial pressure-headache drowsiness, confusion, impaired consciousness, papilloedema,focal signs - eg hemiparesis depending where the lesion is - SUSPECT IN ANYONE WITH EAR SEPSIS |
|
|
Intracranial brain abscess- management |
Surgery-drain abscess through burr hole , treatment with IV antibiotics- penicillin, metronidazole + often a 3rd, ENT surgery to remove cholesatoma (probable) and radical mastoidectomy performed |
|
|
Extradural abscess- what |
pus, granulation tissue or effusion- usually asymptommatic and found on mastoidectomy- can cause sigmoid sinus thrombosis/phlebitis + ottic hydrocephalus |
|
|
Sigmoid sinus thrombophlebitis-formation |
Localised phlebitis-muralthrombus formation-occlusion or propgation to IJV where it can present as swelling in neck- can become infected to cause septicaemia |
|
|
Sigmoid sinus thrombophlebitis- symptoms |
general malaise, headache, spiking fever, rigors and increased ICP, post auricular oedema of acute mastoiditis (if mastoid emissary vv blocks off)- anticoagulant treatment |
|
|
Subdural abscess |
well circumscribed collection of pus, walled off from remaining subdural space |
|
|
Meningitis |
bacterial infection causing inflammation of the meninges and CSF- 86% of these have had atleast 1 episode of ASOM, cholesteatomas can cause by direct extension |
|
|
common virsues causing acute otitis media |
respiratory syncytialvirus (RSV), influenza A and B viruses and rhinoviruses |
|
|
Rinne's test a) what b)screens for what |
a) compares air conduction to bone conduction using tuning
b)conductive hearing loss |
|
|
Rinne's test- a)normal result b)abnormal result |
a) air>bone= positive Rinne b) bone>air= negative Rinne, conductive deficit if bone can be heard louder than air, sensorineural if neither can be heard - can be given false result through bone conduction to other normal ear so conduct weber test |
|
|
Weber test |
base of the vibrating tuning fork is placed on the glabella, pt asked which ear they hear it loudest in or if its equal |
|
|
Weber results: a) normal b)abnormal |
a) heard symmetrical and equally in both ears b)sound heard louder on one side |
|
|
Weber test abormal result- explain |
If heard louder on one side= conductive loss on that side or sensorineural loss on opposite side (sound transmitted to better cochlea) |
|
|
Audiogram a) shows b) axis |
a) type and degree of hearing loss (conductive or sensorineural) b)x=frequency (pitch) - Hz 250,500,1kHz, 8kHz, y= intensity (loudness) dB |
|
|
Audiogram- intensity range |
0dB to 20dB = Normal range -21dB to 40 dB = Mild hearing loss 41 dB to 55 dB = Moderate hearing loss 56 dB to 70 dB = Moderately Severe hearing loss 71 dB to 90 dB = Severe hearing loss > 90 dB = Profound hearing loss |
|
|
masking |
It means presenting a constant noise to the nontest ear. It is done to prevent nontest ear from detecting the sound presented to the test ear by crossover |
|
|
conductive hearing loss on audiogram |
audiogram shows normal bone conduction thresholds while the air conduction thresholds show a hearing loss greater than 20db, difference of at least 10 db between the air and bone conduction thresholds |
|
|
conductive hearing loss- causes: |
Wax, glue ear, otitis media, perforation of the tympanic membrane, or ossicular abnormalities |
|
|
Sensorineural Hearing loss on audiogram- |
air and bone conduction thresholds are above 20db. The difference between the air and bone conduction threshold is less than 10db |
|
|
sensorineural HL- causes |
Presbyacusis, Menieres disease, noise-induced hearing loss, Acoustic neuroma |
|
|
Mixed Hearing Loss on audiogram |
Both the air and bone conduction thresholds are above 20db but the difference between the air and bone conduction threshold is more than 10db |
|
|
tympanommetry- what |
Tympanometry is a method of assessing the status of the middle ear. The compliance (inverse of stiffness) of the tympano-ossicular system is charted against various pressure changes.X axis shows the pressure gradient. Y axis shows the compliance. |
|
|
Type A tympanogram |
Tent shaped, located between -100 to +50 (normal at 0)- NORMAL |
|
|
Type B tympanogram A) appearence b) indicates |
a) flat, horizontal trace line b) indicating fluid in the middle ear (in the presence of normal ear canal Volume), If the ear canal volume is large and the curve is Type B, it indicates a perforated tympanic membrane |
|
|
Type C tympanogram a) appearence b) indicates |
a) Is tent shaped but is located at pressures more negative than -100mm b) indicates negative pressure in the middle ear seen in Eustachian tube dysfunction. |
|
|
Presbyacusis a)what b)symptoms c)when |
a) hearing loss due to aging from wear and tear on outer hair cells - most common cause of sensorineural deafness b) bilateral and symmetrical hearing loss, insidious onset c) 50yrs condisidered lower limit |
|
|
Presbyacusis on audiometry |
high frequency hearing loss, can't hear constonants which are crucial for understanding speech |
|
|
Presbyacusis- symptoms |
person knows people are speaking but can't understand whats being said, words merge into one, muffled speech- funciton well on one to one basis, can't hear in background noise, tinnitus may be present |
|
|
Presbyacusis- risk factors |
noise exposure, smoking, ototoxic meds, fhx,m high bmi, htn, vasc disease, alcohol |
|
|
presbyacusis- treatment |
Hearing aids give a substantial improvement in hearing, explain the hearing loss problems to the pt and their relatives |
|
|
Presbyacusis: causes a) intrinsic factors b) extrinsic factors |
a)neuronal loss, loss of cochlear outer hair cells, atrophy of the highly vascular stria in the lateral cochlear wall, oxidative stress/DNA damage b)noise, ototoxic medication, diet |
|
|
Ototoxic meds- |
aminoglycosides, cisplatin, loop diuretics, NSAIDs |
|
|
Acoustic neuroma-what: |
benign tumours arising from the auditory nerve, morbidity and mortality related to tumour size |
|
|
acoustic neuroma- symptoms: |
unilateral hearing loss or tinnitus, fluctuatung hearing, subtle balance disturbance- most patients present to neuro symptoms (and large tumours) rather than hearing loss |
|
|
acoustic neuromas- risk factors |
neurofibromatosis, high dose ionising radiation |
|
|
acoustic neuromas- investigations |
pure tone audiometry, MRI/CT scanning |
|
|
large acoustic neuroma- symptoms |
facial pain/numbness if involving the trigeminal nn, earache, ataxia- cerebellar compression, brainstem compression- hydrovephalus, vision loss |
|
|
acoustic neuroma- treatment |
Small tumours- removal with preservation of the facial nn Gamma-knife: single large dose of radiation in one surgery - for tumours >3.5cm |
|
|
Sudden sensorineural hearing loss- causes |
acoustic neuroma, Wegners granulomatosis (vasculitis) |
|
|
Sudden sensorineural hearing loss- management |
Early- bed rest, vasodilators, carbogen (5% CO2 and 95% O2), steroids= pred 40mg for 5 days Late:exclude acoustic neuroma |
|
|
Sudden sensorineural hearing loss- prognosis |
low frequency losses recover better than higher freq losses, vertigo is an unfavourable factor |
|
|
Noise induced hearing loss- temporary |
prolonged noise exposure causes temporary threshold shift within 2 hrs exposure |
|
|
noise induced hearing loss- permanent |
permenant threshold shift |
|
|
noise induced hearing loss- on audiogram |
notch at 4khz,6kxz and less commonly 3 kHz - gradual involvement of lower freq |
|
|
diagnosis of noise induced hearing loss: |
requires history of noise exposure, bilateral hearing loss |
|
|
non organic hearing loss |
those in pursuit of compensation, teenagers |
|
|
Hearing aids work by |
amplifying sound into the ear canal by an earpiece |
|
|
Bone anchored hearing aids a) who uses b)how does it work |
a) those unable to use conventional hearing aids due to loss of shape of canal or chronic infection b)titanium screw in temporal bone and attachment by bone conduction to the cochlear |
|
|
cochlear implants a) what b)indication |
a)implantation of electrodes into the cochlear to stimulate the auditory nerve b) bilateral profound sensorineural deafness |
|
|
perilymph fistula |
abnormal connection in oval or round window connecting the inner ear to the middle ear allowing perilymph leakage into the middle ear |
|
|
symptoms of barotrauma (sudden pressure change) and perilymph fistula (barotrauma can lead to perilymph fistula) |
sensorineural hearing loss, tinnitus, vertigo |
|
|
perilymph fistula-treatment |
surgical repair as a matter of urgency |
|
|
Longitudanal temporal bone fracture a) percentage of temp bone fractures b)involves which structures c)hearing loss |
a)80% b) EAM and middle ear roof c)conductive loss due to ossicular disolcation/ haemotympanum/ tympanic membrane rupture |
|
|
Transverse temporal bone fracture a)percentage b)involves which structures c)symptoms d) tx |
a)20% b) bony labyrinth c) sensorineural hearing loss, vertigo, facial nerve palsy (30%)- delayed paralysis recover spontaneously d) early surgical decompression improves long term chance of recovery |
|
|
Ear manifestations of AIDs: a) external ear b)middle ear c)inner ear |
a) Kaposi's sarcome, fungal otitis externa, necrotizing 'malignant' otitis b) acute and serous otitis media, mastoiditis, most common in paediatric AIDs C) Sensorineural hearing loss (neuropathy of auditory nerve), iatrogenic (vincristine, antifungal agents), Hearing loss progresses with disease. Exclude neurosyphilis |
|
|
Ototoxic group of drugs |
Aminoglycosides, diuretics (furesmide), salicylates and chemotherapeutic agents. monitor serium levels and serial audiometry |
|
|
Glomus tumour- what |
Arise from non-chromaffin paraganglionic tissue, in the neck glomus cells give rise to carotid body tumours. rare and benign tumours |
|
|
Glomus tumour- symptoms |
tinnitus- synchronous with the pulse beat, hearing loss - conductive or sensorineural, facial paralysis, paralysis of CN 9-12, vertigo, ataxia, headaches (small no present with phaechromocytoma like picture) |
|
|
Glomus- examination |
pulsatile red/blue mass behind the ear drum (setting sun) and audible bruit over the temporal bone, facial paralysis, paralysis of CN 9-12 |
|
|
Glomus- treatment |
surgery, radiation therapy or combination |
|
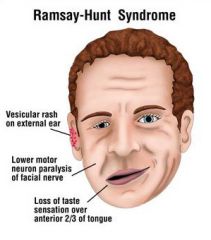
Herpes zooster oticus (Ramsay Hunt Syndrome)- symptoms |
Intense, deep pain within the ear, may radiate to pinna, followed a few days later by a vesicular eruption on the pinna + external ear |
|
|
Ramsay hunt syndrome- signs |
Vesicular rash on pinna and external ear and soft palate and anterior 2/3 of tongue causing loss of taste. sensorineural deafness, vertigo, facial nn paralysis on ipsilateral side, ipsilateral hearing/balance problems, hyperacusis |
|
|
ramsay hunt syndrome |
Early treatment (within 7 days of onset) with antiviral acyclovir + prednisolone improves prognosis and reduces the likelihood of post herpetic neuralgia |
|
|
Subjective (intrinsic) tinnitus |
hallucination of noises in the head or ears - occurs on its own or in association with vertigo and hearing loss. Short burst <15 mins are physiological and due to outer hair cell activation |
|
|
Obhective (extrinsic) tinnitus |
Noise in the head or ears that can be heard by others eg clicking of the soft palate in palatal myoclonus and vascular bruits |
|
|
Causes of intrinsic tinnitus |
drugs, labyrinthitis, trauma, vascular, presbyacusis, meniere's, noise, otosclerosis |
|
|
Management a) bilateral tinitus b)unilateral tinitus |
a) reasurrance, coping strategies eg masking with environmental noise- radio, ipod, night time sedation, tinnitus maskers b) investigation. often begins in one ear then occurs in other |
|
|
Trauma to pinna' 'cauliflower ear' a) causes b)pathogenesis |
a) contact sports-boxing/rugby b) Bleeding, vascularising perichondrium is stripped from the underlying cartilage of the external ear, cartilage can become ischaemic causing perichondritis, necrosis and atrophy, cosmetic distortion of the pinna |
|
|
Perichondrial haematoma of the pinna a) treatment |
drainage under local anaesthetic, after drainage a wick/corregated drain inserted and pressure dressing applied as haematoma has a tendancy to reform, prophylactic antibiotics |
|
|
Perichondrial haematoma- treatment when a pressure dressing cannot be tolerated |
sutures through full thickness of the ear + tied over dental rolls |
|
|
Middle ear trauma a) causes b) result of trauma c) result of large shock wave |
a) poking things in ear, accidental or due to sudden pressure changes (barotrauma)- following a loud explosion, noise or slap across the ear b) rupture of the tympanic membrane- 10-20dB conductive HL + irregular edge , disruption/fracture of the ossicular chain eg stapes crura- associated conductive hearing loss of 50-60dB |
|
|
result of large shock wave to middle ear |
c) disruption of Reissner's membrane + severe sensorineural hearing loss |
|
|
Acoustic trauma a) results from b) characteristic hearing loss c) risk factors |
a) small arms gunfire, explosions/blast injuries, long term noise exposure over 85dB b) hearing loss more marked at 4KHz c) susceptibility of the cochlea to noise induced hearing loss has a genetic component |
|
|
Temporary threshold shift |
Acute noise exposure damaging the outer hair cells, thought to be reversible + returns to normal within 24hrs, tinnitus experienced |
|
|
Skull base fracture of the petrous temporal bone- symptoms and signs |
haemotympanum- drum appears purple, conductive hearing loss, external auditory canal may appear stenosed, CSF leakage (more likely in transverse fracture) |
|
|
Skull base fracture- treatment |
Antibiotic cover, surgical decompression if nerve palsy |
|
|
Transverse fractures (20%) a) result from b) symptoms c) Ix d) later complications e) other complications |
a) frontal or occipital blows b) sensorineural hearing loss (often pass through labyrinth or IAM), vertigo, facial nerve palsy, nystagmus (if cochlear damage) c) urgent CT to define site of injury d) delayed nerve palsy due to oedema and bruising around the nerve - managed with high dose systemic steroids d) CSF leak, may present as rhinorrhea, vertigo |
|
|
Minor head trauma (no fracture) a) symptoms b) time to resolve |
a) labyrinthine concussion - tinnitus, vertigo, permenant hearing loss and BPPV (rotation induced by placing the ear down) b) usually within 2 yrs- 1/4 of pts have persistant trouble |
|
|
Otitis externa a) what b) 3 types |
a) inflammation of the outer ear: auricle, external auditory canal + outer surface of the ear drum b) diffuse, furuncle, malignant |
|
|
Diffuse otitis externa a) what b)types |
a)Generalised inflammation of the ear canal - eam b) generalised skin condition: eczema, psoriasis, seborrhoeic dermatitis, localised skin condition: trauma, cotton buds, instrumentation, scratching with dirty nails, putting head under water |
|
|
Diffuse otitis externa a) infective causes b)non-infective causes |
a)Bacterial- pseudomonas (secondary colonisation), staph aureus, fungal: candida, aspergillus, viral: herpes zooster b) allergic/irritant- shampoos, ear drops, neurodermatitis as part of an anxiety disorder resulting in itching/scratching/eczema cycle |
|
|
Diffuse otitis externa: a) symptoms b)signs |
a)itchiness, irritation, pain and swelling, ottorhoea, deafness due to occlusion of EAM b) pain on moving pinna/ inserting aural speculum to examine ear, otorrhoea, enlarged pre and post auricular or deep cervical LN's |
|
|
Diffuse otitis externa: types of ottorhea |
Bacterial- pus + debris in EAM, fungal- dry or wet debris looking like blotting paper, or yellow/black spores (aspergillus flavum or niger), viral- vesicles around introitus of EAM (herpes zooster), soft palate, or haemorrhagic vesicles on tympanic membrane - thin + watery discharge nb if mucus is present- must be from middle ear, EAM doesn't contain any mucus secreting glands |
|
|
Diffuse otitis externa: treatment |
analgesia, aural toilet, topical medication, systemic antibiotics for gross cellulitis |
|
|
Diffuse otitis externa: Topical treatments |
Antibiotics/steroid ear drops- gent + hydrocortisone, astringents- aluminium acetate, anti-infective drops - locorten vioform- acetic acid eardrops protective against bacteria and fungal infection, ribon gauze wick or pope otowick helps drops reach deeper in EAM |
|
|
Furuncle otitis externa a) what b)signs c) treatments |
a) painful infection of a hair follicle on the outer 1/3 of the EAM - usually due to staph b) red swelling from an aspect of the outer wall of the EAM bulging into the meatus c) analgesia, astringents (glycerin + ichthammol) |
|
|
astringents |
agents which cause contraction or shrinkage of tissues and dry up secretions |
|
|
malignant otitis externa a) what b) cause c) risk factors d)signs and symptoms |
a) aggressive form of otitis externa, not cancerous b)pseudomonnas aeruginosa c) diabetics, immunocompromised, old age d) spreads to bone causing osteitis, severe pain, 7,9,10,11 CN palsies as it spread across skull base- pain, headache, oedema, exudate |
|
|
malignant otitis externa- treatment |
High dose IV antibiotics, oral and topical antibiotics for 6-8 weeks |
|
|
Acute otitis media- infection of the middle ear- causes |
50% viral origin, bacterial: strep pneumoniae, haem influenzae, moraxella catarrhalis |
|
|
Acute otitis media- a)symptoms b) examination c) treatment |
a)hearing loss, pain, otorrhea when TM bursts, pyrexia, systemic upset b) red bulging TM, ruptured TM c) amoxicillin first line, myringotomy if condition fails to resolve or facial nerve palsy- brain abscess= potentially fatal complication |
|
|
Mastoid bone a) what b)relations c) structures |
a) extension of petrous temporal bone of the skull, honeycomb appearence, communicated with tympanic cavity through petrous temporal bone b)superior- middle cranial fossa, posterior- post cranial fossa (could be spread to cause meningitis or cerebral abscess) c) facial nerve canal, sigmoid sinus, lateral sinus |
|
|
acute mastoiditis- typical history |
AOM that fails to resolve, persistant otalgia, ottorhoea and hearing loss, unilateral headache- cause for concern as could indicate intracranial complication, pt systemically unwell, canal full of pus, polyp may be seen thought tympanic membrane, sagging of the postero-superior canal wall + tenderness over bone above ear canal (McEwen's triangle), oedamatous + erythematous skin and pinna pushed forward- red and boggy |
|
|
Acute mastoiditis- treatment |
early- high dose IV abx if not resolved in 48hrs/ complications arise- subperiosteal abscess, facial nerve palsy, labyrinthitis, petrositis (CN 5+6 nn palsy) then cortical mastoidectomy |
|
|
Trauma to the facial bones and nose: parts of the face |
orbit= pear shaped, zygoma= floor and lateral wall of the orbit + zygomatic arch |
|
|
'Blow out' fracture= |
orbital floor +/- medial wall |
|
|
History of facial trauma |
manner of injury, CSF leak, pre or post traumatic amnesia, clear airway, other injuries, periorbital swelling should not stop you testing the pupil reflexes + vision |
|
|
Nasal reduction: a) when assesed |
a)5-10 days after the injury when the swelling has reduced |
|
|
Septal haematoma a) cause b) appearence c) consequences d) treatment |
a) bleeding underneath the mucoperichondrium b) soft bluish bulge either side of the septum causing blockage of nasal air passages, feels soft on examination c) usually infection, septal abscess, necrosis of the cartilage, collapse of the nasal bridge and 'saddle deformity' d) drain haematoma as a matter or urgency, broad spectrum antibiotics covering staphylococci for at least 1 days |
|
|
Summary of management of nasal trauma: |
Exclude a head injury + other injuries, exclude a septal haematoma, exclude a zygomatic or middle 3rd fracture, exclude a csf leak, exclude a blow out fracture of the orbit |
|
|
If diplopia + facial trauma: a) exclude b) pathogenesis |
a)blow out fracture or zygomatic fracture b) blow compressing orbital contents, herniation of orbital fat through damaged orbital floor confirmed by ct, trapped inferior rectus causing diplopia |
|
|
Signs of a zygomatic fracture |
1) diplopia 2) subconjunctival haemorrage withour a posterior limit 3) infraorbital nerve anaesthesia 4) an infraorbital 'step' on palpation 5) trismus 6) deformity of the zygomatic prominence |
|
|
Periorbital swelling which crackles when palpated or increases in size when the pt blows their nose is due to |
surgical emphysema- results from fronto ethmoidal fracture |
|
|
Dural tear associated with: |
aerocele (air in cerebral vault/brain), immeadiate repair indicated |
|
|
CSF leak in closed injuries: a) management b) CSF |
a) conservative under supervision, pt nursed at 30 degrees head up, no nose blowing, prophylactic antibiotic b) test for presence of beta- transferrin as more traditional glucose testing is inadequate |
|
|
Compound nasal injuries- management: |
1) cleaning 2) tetanus prophylaxis 3) antibiotic cover 4) closure of the skin defect 5) review at 5-10 days to consider nasal reduction |
|
|
Severe nasal laceration: management |
primary reconstruction when pt is fit for surgery, for full-thickness cuts closure with mucosa-cartilage- Sc tissue skin using 5/0 monofilament (Nylon) |
|
|
Management of: a) depression of the frontal bone b) fracture of the posterior wall c)zygomatic fractures d)fractured nose |
a) Elevation b) left unless there is an aerocele or persistant CSF leak c) XRAY, often fluid level in the maxillary sinus usually due to blood from epistaxis- alerts to zygomatic fracture d) must be reduced within 14 days of injury |
|
|
Important features of the examination after facial trauma: |
Rhinorrhea, epistaxis, CSF leak- clear unilateral watery discharge, septal haematoma/haemorrhage |
|
|
Rhinoplasty |
Needed if nose is not reduced in first 14 days after injury, appointment 5-10 days after injry, after this osetotomies carried out through 2mm stab incisions either side of nose |
|
|
Reduction of nasal fractures |
in outpatients under local anaesthetic (or general), may need intranasal pack to support if bones are very unstable |
|
|
Complications of nasal fracture |
septal haematoma/septal abscess, septal perforation, deformity, bent septum with obstruction, anosmia, CSF leak, adhesions between turbinate mucosa and septum |
|
|
Management: a) adhesions b) septal perforation consequences |
a) reconstruction of the bony and cartilagenous architecture + nasal splinting to prevent severe obstruction b) altered air flow, turbinate hypertrophy, sensation of nasal obstruction, crusting + bleeding |
|
|
Nose picking: a) presentation b) management c) complications |
a) recurrent epistaxis of vestibulitis, rawness of little's area, crusting, vare are of pale cartilage b) sniffing vaseline from the end of the little finger adjacent to the anterior nasal septum c) septal perforation |
|
|
Barotrauma to the sinuses: a) when b) symptoms c) treatment |
a) following sudden decompresion in an aircraft, diving or after URTI which has interefered with patency of sinus ostia b) immeadiate severe pain as negative intra sinus pressure strip off the the mucoperiostium from the bone causing development of a haematoma prone to infection c) antibiotics, decongestants and analgesics |
|
|
Epistaxis: a) in children arise from b) in adults c) causes |
a) retrocollumnar vein at the anterior end of Little's area b) anterior septum- prominent vessels seen, or lateral nasal wall posteriorly c) idiopathic, following URTI or allergic rhinitis, nose picking + crusting, facial and nasal trauma and rarely tumours, RARE- angiofibroma causes severe unilateral epistaxis in teenage boys |
|
|
Epistaxis: a) risk factors b) first aid |
a) HTN, anticoagulants, hereditary haemorragic telangectasia (abnormal capillaries in GI, resp and urogenital tract), coagulopathis- VWD, leukaemia, DIC b) lean forward + pinch fleshy part of the nose for 10 mins, spit out blood and apply ice pack to nasal bridge or back of the neck |
|
|
Epistaxis resuscitation |
- measure the amount of blood loss, pulse + BP, - seat the patient in case of vasovagal attack, -iV access, iv fluid, fbc, coag screen, group and save, - clot removed via anaeasthetic + vasoconstrictor spray applied cophenylococaine or 5% cocaine, - if bleeding point can be seen, cauterise with silver nitrate (on a stick) or bipolar diathermy, - anterior pack- vaseline, merocel or bismuth and iodine parafin paste (BIPP) pack inserted into nasal cavity, - posterior ballon- foley urinary catheter inserted + left for 36-48hrs - broad spec abx to prevent infection - on pack removal antiseptic cream to reduce adhesion formation - topical injection of injectable transexamic acid |
|
|
Epistaxis in bleeding diatheses insert: |
calcium alginate pack (Kalostat)- less traumatising |
|
|
If packing failure: |
-theatre for packing, insertion of postnasal pack + septal surgery, - failure then artierial ligation - sphenpalatine artery pr ext carotid in neck + anterior ethmoidal artery also effective |
|
|
Pharyngitis (infected,sore throat) symptoms |
usually trivial and self-limiting, dry sore throat in mornings, no general malaise, nocturnal nasal obstruction, coryza- throat swabs only in persistant/atypical cases |
|
|
Pharyngitis- viral agents |
adenovirus, EBV, enteroviruses, cytomegalovirus, rare: HSV |
|
|
Pharyngitis- bacterial agents |
beta- haemolytic streptococcus, pneumococcus |
|
|
Pharyngitis- main fungal agent |
Candida, associated with steroid asthma sprays, dentures, immunosuppression- AIDs, radiotherapy encompassing the oral cavity/oropharynx |
|
|
Follicular tonsilitis- symptoms |
sore throat, pain on swallowing, enlarged erythematous tonsils with 'white spots' (exudates from tonsilar crypts), systemic illness, fever, malaise, cervical lymphadenopathy + halitosis |
|
|
Follicular tonsilitis- bacterial agents |
beta haemolytic streptococcus group a (c and g less common), cornybacterium diptheriae |
|
|
Follicular tonsilitis- treatment |
analgesics + antipyretics, usually self limiting + resolution within 5 days, antibiotics- penicillin shortens course by 1-3 days- give if: marked systemic features, unilateral peritonsilitis, increased risk from acute infection (IC)- give ertythromycin if pen allergic |
|
|
when is tonsillectomy indicated? |
recurrent tonsilitis- at least 5 episodes per yr for 2 yrs or more or missing a signifigant time off school |
|
|
Glandular fever (EBV) - Symptoms |
sore throat, pain on swallowing, enlargered erythematous tonsils covered in white/grey exudate, systemic illness with fever, malaise, marked cervical and generalised lymphadenopathy, unwell pt with nasal congestion amd sterterous breathing, hepatosplenomegaly, atypical mononuclear cells on blood film diagnosis- positive monospot or paul bunnell test |
|
|
Glandular fever- treatment |
bed rest, hydration, analgesics, antipyretics and oral steroids (severe cases if there is airway obstruction) |
|
|
Quinsy - peritonsillar abscess: symptoms |
+/- past history of tonsilitis- can develop out of acute tonsilitis, pus and bulging in soft tissues superolateral to the tonsil displacing it inferomedially, severe unilateral tonsillar pain, odynophagia, trismus, referred otalgia, generally malaise and fever, hot potato voice, drooling |
|
|
Qunisy- treatment |
drainage of abscess, antibiotics, analgesia, antipyretics and fluids, tonsillectomy if quinsy returns |
|
|
Head + neck malignant tumours: |
-oral cavity, pharynx, paranasal sinuses, nasal cavity, larynx, salivary glands, thyroid tumours - 6th most common cause of cancer world wide - more common: men and older people |
|
|
Head + neck malignancy: risk factors for SCC: |
smokers- pipe smokers and those who hold cigarettes between their lips for a long time, alcohol drinkers, sun exposure, tobacco or betel nut chewing, pahn, breathing in chemicals and hardwood dusts (nose and sinuses), leukoplakia- condition becomes cancerous in 1/3 pts |
|
|
Head + neck cancer pathology: |
most SCC, lymphoma, salivary gland tumours (adenoid, cystic, mucoepidermoid, acinic cell), thyroid (papillary, medullary, anaplastic carcinomas), sarcomas, undifferentiated carcinomas |
|
|
Head + neck cancer: presentation |
persistant pain in throat (beware: unilateral for >4 weeks), odynophagia, dysphagia, persistant hoarseness/voice change, referred pain to the ear, bleeding in the mouth or throat, enlarging neck node, persistant ulceration, leukoplakia or erythroplakia nb any white/red oral lesion that doesn't heal in 2 weeks should be evaluated + considered for biopsy weight loss- unusual unless secondary to dysphagia |
|
|
Other symptoms of h+ n cancers: |
lump/thickening in oral soft tissues, soreness or feeling that something is stuck in the throat, difficulty chewing/opening mouth, difficulty moving the tongue, numbness of the tongue or other parts of the mouth, swelling of the jaw that causes dentures to fit poorly/be uncomfortable symptoms for >2 weeks see GP |
|
|
H+N Cancers: diagnosis: |
history, examination by fibreoptic endoscopy, FNAC in clinic on neck nodes/lumps, CT/MRI from skill base to thoracic inlet, CXR/CT chest, blood tests, ECG, assesement of nutritional status, biopsy under GA |
|
|
Tumours of the oropharynx: a) incidence b)age c)sex d)aetiological factors e)histology |
a) 6-8/million per year b) 50-70yrs, increasing incidence of younger pts (30-40yrs) c) male:female of 5-8:1, increasing in women d) smoking, alcohol abuse, betel-nut chewing, radiation, iron deficiency anaemia, HPV infection e) mainly SCC-90%, NHL-8%, minor salivary gland tumours-2% usually on palate |
|
|
Tumours of the oropharynx: a) presenting symptoms b)sub sites |
a) sore throat, odynophagia, dysphagia, otalgia, bleeding, change of voice, trismus, weight loss, mass in neck b) tonsils/lateral pharyngeal wall (60%), tongue base (25%), palate (10%), posterior pharyngeal wall (5%) |
|
|
Hypopharyngeal tumours a) incidence b) age c) sex d) aetiological factors |
a) 10-20/million/year b) increasing incidence with age c)more common in males, apart from postcricoid (females) d)smoking, alcohol abuse, betel nut chewing, iron deficiency anaemia, HPV infection |
|
|
Hypopharyngeal tumours e) histology f) Presenting symptoms g) sub sites |
e) almost exclusively SCC f) sore throat, odynophagia, dysphagia, otalgia, haemoptysis, hoarseness, stridor, weight loss (advanced cases), neck mass (45% have metastatic disease at presentation) g) piriform sinuses- 70%, posterior pharyngeal wall 25%, postcricoid area -5% |
|
|
Larygneal cancer: a) incidence b)age c) sex d) aetiological factors |
a) 40/million/year b)rare <45yrs, increasing incidence with age c) male-female, 4:1, increasing in females, scotland (2:1) d)smoking, alcohol abuse, previous neck radiation |
|
|
Larygneal cancer: f) histology g) presenting symptoms h) sub sites |
f)95%- SCC, minor salivary gland tumours, neuroendocrine tumours, sarcomas g)change of voice/hoarseness, dyspnoea/stridor, pain/odynophagia, dysphagia, neck mass h) glottis/true vocal cords (50%), supraglottis (false vocal cords, epiglottis + aryepiglottic folds)- 40%, subglottis (lower edge of cricoid cartilage) - 5% |
|
|
Staging- |
TNM Staging, stage 1 cancer are small, localised + usually curable- stage 2,3,4- locall advanced or spread to local lymph nodes/distant mets |
|
|
Surgery for malignancy |
-transoral surgery using carbon dioxide laser under microscopic guidance -neck dissection- radical= ipsilateral LN, spinal acc nn, IJV + SCM |
|
|
Head and neck cancers: treatment |
- surgery - total laryngectomy leaving laryngeal stoma + valve for speech, - radiation- SCC highly sensitive to radiotherapy - chemo- limited role |
|
|
Minor salivary glands |
600-1000, beneath the mucosa of the upper aerodigestive tract + named according to position- around the oral cavity and oropharynx eg- palatal, buccal, labial, tongue, tonsilar |
|
|
Major salivary glands - 3 paired structures |
parotid, submandibular, sublingual - situated outside the oral cavity- connected via a series of ducts |
|
|
Parotid gland a) which nerve enters and divides b) opening of the duct c) secretomotor supply from, via d)type of saliva produced |
a) facial nerve enters posterior pole and divides gland into superficial (80) and deep lobes (20%) b) second upper molar tooth c) glossopharyngeal nerve via the tympanic plexus in the middle ear d) entirely serous saliva |
|
|
Relations of the parotid gland: a) posterior b) anterior c) superior |
a) zygoma/tympanic bone/ cartilagenous external ear canal/ stylomastoid fossa/ mastoid process/ upper quarter of sternocleiodomastoid mm b) posterior half of masseter c) zygomatic arch |
|
|
Structures within the gland: |
-Facial nerve + 5 branches: temporal, zygomatic, buccal, mandibular, cervical - retromandibular vv - ext carotid aa- divides into terminal superficial temporal and maxillary arteries - variable no of lymph nodes in superficial lobe (<20) - Parotid duct (Stenson's duct)- through buccinator mm- anterior border of masseter- 2nd upper molar tooth |
|
|
Parotid gland innervation: |
secretomotor fibers: from inferior salivary nucleus + otic ganglion (glossopharyngeal nn via tympanic plexus of middle ear) sympathetic fibers: from superior cervical ganglion via neural plexuses around aa |
|
|
Submandibular gland: a) type of saliva produced b) location + relationship |
a) serous + mucous b)Triangular space: mylohyoid mm + mandible + roofed by deep cervical fascia, marginal mandibular branch of facial nerve superficially, lingual and hypoglossal nn near deep surgace, facial aa enters submandibular triangle under posterior border of digastric mm |
|
|
Submandibular gland: a) duct b) exit c) secretomotor fibers d)sympathetic fibers |
a) Wharton's duct from middle of deep surface b) lingual frenulum c) from lingual nerve via chorda tympani of facial nerve from the superior salivary nucleus d)from superior cervical ganglion via neural plexuses around facial aa - hypoglossal |
|
|
Sublingual gland: a) location b)nn supply c) drainage d) saliva produced |
a) floor of the mouth, distal to deep lobe of submandibular gland, marginal mandibular nn overlies b) lingual nn + hypoglossal nn c) many small ducts drain to floor of mouth + wharton's duct d) mucus saliva |
|
|
Cells of origin of salivary gland neoplasms |
Reserve cells- found in intercalated and excretory duct systems - have the capacity to differentiate into different duct cell types |
|
|
Physiology of the salivary ducts |
Serous/mucus cells clump together to form acini, acini are surrounded by myoepithelial cells which are drained by short intercalated ducts, these drain into striated ducts then excretory ducts before exiting into main ducts |
|
|
Physiology of the salivary glands- fluid secretion |
Acini- basal secretion of fluid (water, Na, K, Cl, HCO3, proteins- amylase, mucins, IgA) Striated and excretory ducts- active secretion and exchange of ions (Na for K) |
|
|
Amount of saliva produced in 24hrs |
1-1.5L - Basal saliva excretion and autonomic control via neurotransmitters |
|
|
Salivary stimuli: |
smell, taste- acid and sugar, sweet, salt, psychic stimuli eg the thought + sight of food and images of food, chewing and mastication, parasympathomimetic drugs eg pilocarpine |
|
|
Causes of xerostomia (dry mouth): |
Depression, anxiety, Drugs with antimuscarinic activity: atropine, hyoscine, ipratropium, TCAs, monamine oxidase inhibitors, phenothiazides, orphenadrine+ benhexol (and related antiparkinson drugs), antihistamines Drugs with sympathomimetic activity: 'cold cures' and decongestants eg ephedrine, phenylpropylamine, bronchodilators eg isoprenaline, apetite suppressants Sjogren's syndrome radiotherapy to head/neck region |
|
|
Non-neoplastic, non-salivary swelling: |
Hypertrophy of the masseter, ageing, neuromas, anuerysms, cysts within the parotid, lymphadenopathy due to otitis externa, skin/scalp infections, dental infections, lymph nodes, Ludwig's angina, parapharyngeal space tumours, mandibular tumours, mastoiditis causing subperiosteal abscess and drainage into upper neck behind parotid tail |
|
|
Viral parotitis: causes |
-mumps, caused by paramyxovirus, most common cause of bilateral parotid enlargement. signs: systemic upset, swelling and pain due to stretching of parotid capsule treat: analgesia + hydration - HIV: Cystic enlargement of the major salivary glands |
|
|
Bacterial parotitis: a) presentation b) causes c) treatment d) may be due to: |
a) painful, swollen gland, pyrexia and systemic upset, pus may be visible coming from opening of duct in mouth. of submandibular glands: swollen tissues at the floor of the mouth b) often staphylococcal infection c)high dose anx, rehydration, oral hygeine, citrus moutwash (sialogogue) to increase flow of saliva d) TB - drug treatment required- actinomycosis |
|
|
a)Fungal parotitis: b) other parotitis |
a) candidiasis- rare- immunosuppressed b) sarcoid, drugs- dextroprphoxyphene |
|
|
Sialectasis: a) what b) prior event to c) majority affect which gland |
a)Dilatation + stenosis + necrosis of acini forming cysts b)initial event in sialiathisis c) submandibular gland - 85%, can occur in parotid |
|
|
Sialithiasis: a) what b) presentation c) examination d) investigation e) treatment |
a) formation of calculi within the salivary glands b)postprandial swelling/pain + repeated infections c)tender, swollen, if migrated to duct may be palpated on floor of the mouth d) CT/Xray, sialogram e) conservative management with oral fluids and sialogogues as small stones may pass spontaneously, surgical excision if problematic duct/gland |
|
|
Sjogren's syndrome: a) classification b) immunological deficit |
a) primary (sicca complex= xeropthalmia, xerostomia), secondary with other autoimmune conditions, benign lymphoepithelial lesions, aggressive lymphocytic behaviour b)loss of suppresor t cell activity |
|
|
Sjogren's syndrome: symptoms |
xeropthalmia, xerostomia, glossitis, dental caries (tooth decay), keratoconjunctivitis, secondary candidiasis, stomatitis, dry vagina, 40% have parotid enlargement and increased chance of development of lymphoma |
|
|
Sjogren's syndrome:: investigations |
HLA A1, A8,DR3, Antigens: ssa, ssb Schirmer's test for lacrimation, Carlsson-Crittenden test for salivary flow, diagnostic test = labial biopsy |
|
|
Benign tumours: a) location b) percentage benign parotid tumours c) percentage benign submandibular tumours d) percentage benign minor salivary gland tumours |
a) 80% salivary tumours parotid b) 80% parotid tumours benign c) 60% submandibular tumours benign d) 30% minor salivary tumours benign - all minor salivary tumours away from mouth/opropharyn are malignant |
|
|
Benign tumours: a) incidence b) sex c) age d)aetiology e)pathology f) what |
a) 1/100,000 b) female preponderance c)adults, rare in children + usually malignant d) unknown, previous radiation may be a factor e) from reserve (stem cells) of intercalated + excretory ducts f) pleomorphic adenoma, warthin's tumour, other adenomas |
|
|
Pleopmorphic adenomas: a) % of benign tumours b) origin c) histology d) presentation |
a) 60-70% b) intercalated ducts of reserve cells c) usually in superficial lobe or tail of parotid, macroscopically: gray/blue surface, soft myomatous, cystic lobulated d) slow- growing painless mass, not usually facial nn palsy , smooth sc swelling with no skin attatchment |
|
|
Pleopmorphic adenomas: a) investigations b)treatment c) prognosis |
a) US or CT, FNAC b) superficial parotidectomy with a cuff of tumour or occasionally total c) If incomplete margins will recurr, if PA left malignant change can occur |
|
|
Warthin's tumour/adenolymphoma a) percentage b) from c) sex d) presentation e) hist f) tx |
a) 2-6% b) origin= parotid LN c) males- 8:1 >40yrs d) soft cystic mass in parotid tail, may be bilateral e) papillary elements lining cystic spaces e) excision: partial or total |
|
|
Tumours of variable malignancy (2) |
mucoepidermoid carcinoma, acinic cell (2-4% of parotid tumours) |
|
|
Mucoepidermoid carcinoma a) origin b) features c) histology d) treatment e) prognosis |
a) epithelial cells of interlobular + intralobular ducts b) prevelance greatest in 5th dacde, female (2-4:1), range of malignancy from low to high and local spread to LN, lungs, bone and brain c)well differentiated: well circumscribed, cut surfaces show cystic dilatations + mucus material. cell types: mucin secreting, epidermoid, intermediate d)low grade= local resection + prolonged follow up, high grade= radical resection and adjuvant chemo e) 30% recurrence rate, 15 yr cure rate= 50% for low grade, 25% for high grade |
|
|
Acinic cell (2-4% parotid tumours): a) originates b)features c) histology d) treatment e) prognosis |
a) reserve cells b) 99% in parotid gland, middle aged and elderly, slow growth, can occur in children, females, can occur bilaterally c) large layer of dense fibrous tissue, cellular, basophillic cytoplasm, lymphoid infiltrate d)local resection and facial nerve preservation, prolonged follow up e) Behaves as low grade tumours- 35% tendancy of local recurrence, 10% metastasise to LN, 55% cure rate at 15yrs |
|
|
Adenoid cystic carcinoma- |
-commonest malignant salivary tumour- 14%, 2% parotid, 16% submandibular, 28% sublingual, 13% minor salivary glands |
|
|
Adenoid cystic carcinoma: a) who b) features c) histology d) treatment |
a) 40-60yrs b) slow growth, perineural infiltration - presentation to pain and palsies c) well circumscribed, large layer of dense fibrous tissue same colour and consistency as normal tissue, cribriform cell pattern d) wide local resection sometimes facial nn sacrificed, role of radiotherapy controversial |
|
|
Adenoid cystic carcinoma: prognosis |
Long term= poor but surivival is usually for years, 15yr survival= 10-26%, local recurrence= 50% - bone, liver, lung- distant mets = prolonged survival |
|
|
Carcioma ex pleomorphic adenoma a) interval of time of presentation from pleomorphic adenoma b)presentation |
a) 10-15yrs b) pain + palsy |
|
|
Adenocarcinoma a) % of salivary neoplasms b) prognosis |
a) 2.5-4% b) highly malignant, poor prognosis: 10% = 5yr survival |
|
|
Lymphoma: 40% of non-epithelial salivary tumours |
- commonest= NHL - 5th-7th decade - some associated with a beign lymphoepithelial lesion - present: firm, rapidly elnarging mass, occasional LN mets, diagnosis= open biopsy -Tx: dependant on histological stage and subtyoe |
|
|
Metastases of salivary gland tumours: |
Local skin: melanoma, SCC Distant: lung, breast, kidney |
|
|
Signs suggestive of malignancy in salivary gland tumours: |
hardness, fixation, tenderness, infiltration of surrounding structures (facial nn, lymph nodes), overlying skin ulceration, cranial nn palsy |
|
|
facial nn palsy+ salivary gland mass= |
malignancy |
|
|
Symptoms of salivary gland tumours: |
most are slow growing painless mass, parotid= discrete mass usually in tail, submandibular= diffuse enlargement of gland, sublingual= palpable fullness on floor of the mouth, minor salivary glands- painless masses, usually floor of the mouth, laryngeal salivary tumours can cause airway obstruction, dysphagia, hoarseness, pain can occur with beign or malignant tumours |
|
|
Functions of the balance/vestibular system: |
1) Keep standing + avoid injury despite movement of the individual +/- surroundings 2) maintenance of visual fixation despite movement of head/body/surroundings |
|
|
Sensory inputs to balance |
proprioceptors, vision, labyrinth |
|
|
Nystagmus- what? |
Involuntary, conjugated rhythmic to and fro movement of the eyes - clinical sign of vestibular abnormality |
|
|
Directions of: a) peripheral vestibular nystagmus b) sign of a central lesion |
a) horizontally or rotatory b) vertical nystagmus or nystagmus that changes direction |
|
|
Physiological nystagmus |
Present in most individuals when the iris moves past the punctum of the lacrimal sac |
|
|
Labyrinth function nystagmus- direction: |
Away from the affected ear |
|
|
Cerebellar lesion nystagmus- direction: |
Ipsilateral nystagmus |
|
|
Degrees of nystagmus: a) 3rd degree b) 2nd degree c) 1st degree |
eg for sudden total vestibular failure of right ear: a) nystagmus to left, front and right b) after a few days...nystagmus to left and front c) after a few weeks...nystagmuys to the left |
|
|
Long term prognosis for nystagmus: |
CNS compensation, damage to labyrinth is permenant, 2st degree nystagmus can be initiated by abolising optic inputs. Reduced caloric response= failure to induce nystagmus by irritating ear canal with warm/cool water above and below body temp |
|
|
Outline of the components of the vestibular system: |
Labyrinth + eyes + somatosensors -> vestibular nuclei + brain stem Cerebellum -> vestibular nuclei + brain stem |
|
|
Central causes: CNS lesion |
1) SOL- infratentorial tumours, cerebellopntine angle tumours 2) Degenerative disease- MS, cerebellar degen 3)Post trauma: head injury 4) Intoxication: alcohol, barbiturates 5)Vascular processes: vertebrobasilar ischaemia |
|
|
Other central causes: |
1) basilar migraine: TIA's 2) presbystasis: in elderly, lasts seconds, worse on movement, no LOC/nausea/vomiting, spontaneous improvement |
|
|
Central causes: presentation: |
varies ataxia unsteadiness imbalance, usually gradual onset central vertigo: not associated with nausea/vomiting, hearing loss or tinitus other S+S of cerebellar or brainstem lesions |
|
|
Vertigo: what, types, accompanying symptoms |
Hallucination of movement, horizontal/rotatory or vertical, symptoms accompanying= nausea, vomting, pallor, diarrohea |
|
|
Cardiovascular causes - vertigo: |
Vaso-vagal, carotid sinus syndrome, postural hypotension, hypertension, cardiac arrhythmias, drugs, hyperventilation |
|
|
Cardiovascular causes- presentation: |
syncope, light-headedness, vague unsteadiness- due to global ischaemia, blackouts (+/- LOC) - Never associated with peripheral causes, fainting/feeling light headed after standing for a long time eg 20 mins |
|
|
Peipheral vestibular vertigo a) what b) assoc features c) cochlear involvement indicated by |
a) sudden episodes of vertigo b) nausea and vomiting c) hearing loss + tinnitus |
|
|
BPPV- CAUSE |
Spontaneous, occasionally follows head injury |
|
|
BPPV- History: |
Middle aged/older pt, recurrent episodes of vertigo, vertigo sudden in onset and associated with particular movements eg turning in bed, looking up, associated with nausea and vomiting on head movement, lasts mins, no otological symptoms |
|
|
BPPV- examination: |
-Dix-Hallpike manouvre- positive test reproduces BPPV symptoms and nystagmus- pt lies flat and examiner supports head turning it through 30 degrees and inclines downwards - shows fatiguability in 30-40secs vertigo + nystagmus disapear -> if no fatigue look for central cause - Latent period- before onset of nystagmus/vertigo - Adaptation: lessens on consecutive testing - ENT+ neuro exam normal |
|
|
BBPV- treatment: |
Reassurance as settles spontaneously, positioning manouvres= Epley's + Cawthorne Cooksley to spend of vestibular compensation- rarely surgery of the posterior semicircular canal |
|
|
Meniere's disease- a triad of: |
Vertigo (recurrent- 10 mins to 24hrs), tinnitus, sensorineural hearing loss |
|
|
Meniere's history of attacks: |
Preceeded by a feeling of fullness in affected ear + sudden onset vertigo. Prostrating + associated with nausea and vomiting, progressive sensorineural hearing loss with attacks, low freq tinnitus, horizontal nystagmus, tuning fork show SNHL on affected side, ENT + neuro exam otherwise normal NB Rule out acoustic neuroma particularly in unilateral sx + otosyphilis |
|
|
Meniere's disease: causes: |
distention of membranous labyrinth/endolymphatic hydrops |
|
|
Meniere's - treatment: |
- natural history is towards spontaneous resolution in 70% of pts |
|
|
Meniere's treatment in medical acute phase: |
vestibular sedatives eg diazepam, antiemetics- phenothiazides, vertigo- cinnarizine 30 mg tds (stugeron)- if fails beta histine 16mg tds |
|
|
Meniere's treatment- surgery |
For resistant cases uncontrolled by medical therapy, ablation destroying affected labyrinth- intratympanic gentamicin (chemical neuronectomy), endolymphatic sac decompression, vestibular nn section, labyrinthectomy ( last option- hearing lost) |
|
|
Meniere's prophylaxis: |
Cinnarizine and beta histine hydrochloride, salt and caffeine restriction, diuretics |
|
|
Benign vestibulopathy: a) cause b) history c) treatment |
a)unknown b)clustered attacks of vertigo in middle aged person, similar to meniere's without tinitus and SNHL, condition resolves in 2 yrs, idipathic c)reasurre, cawthorne- cooksley exercises, spontaneous improvement over 12-24 months |
|
|
Acute labyrinthine failure: a) cause b) history |
a) idiopathic/viral/local vascular occlusion/autoimmune, fracture of temporal bone through labyrinth, post surgery, due to bacterial labyrinthitis- secondary to otitis media/ cholesteatoma b) Any age, sudden attacks of deafness, sever vertigo, nause and vomiting, vertigo is prostrating and pt is confined to bed, audiogram: profound SNHL, distressed pt unable to move, nystagmus, 10 days- 3 week course- vertigo improves SNHL doesn't |
|
|
Acute labyrinthine failure: treatment |
Admit- symptom relief of vertigo: IV fluids, antiemetics, vestibular sedatives, plasma expanders IV, inhlaed carbogen to improve blood supply. Incase of autoimmune cause- steroids + cyclophosphamide |
|
|
Vestibular neuronitis: inflammation of the vestibular part of CN VIII causing vertigo- similar symptoms to labyrinthitis a) cause b) history c) treatment |
a) viral aetiology b)sudden onset vertigo, nausea, vomiting, nystagmus, no hearing loss or tinnitus, lasts a few days, bed ridden, GP managed, occurs in small epidemics c)symptommatic- vestibular sedatives/antiemetics |
|
|
Drug induced a) drugs b) history |
a) aminoglycosides, chemo, AD's, sedatives in elderly b) often not recognised until pt stops taking drugs |
|
|
Migranous vertigo: a) what b) tx |
a) peripheral vertigo associated with migranes at the time of the attack (uncommon) or occuring in migarine sufferers b) amytriptyline 10-25mg nocte |
|
|
Rhinosinusitis |
Inflammatory process of the mucosa of the nose and sinuses (frequently inflmmation of whole of URT) |
|
|
Classifying rhinosinusitis: |
acute: symptoms <4 weeks sub- acute: 4-12 weeks chronic: > 12 weeks |
|
|
Factors contributing to chronic rhinosinusitis: |
bacterial, allergy, infection, mucocilliary impairement, swelling of the mucosa, anatomical variations |
|
|
Sinuses (4 paired structures): |
Frontal Ant + post ethmoidal Sphenoid Maxillary |
|
|
Drainage of the sinuses: a) frontal, ant ethmoidal + maxillary b) sphenoids c) post.ethmoidal d) nasolacrimal duct |
a) middle meatus b) sphenoethmoidal recess in superior meatus c) superior meatus d) inferior meatus |
|
|
Acute rhinosinusitis: sinuses most commonly affected in order |
1) maxillary 2) ethmoid 3) frontal 4) sphenoid |
|
|
Acute rhinosinusitis: pathology |
Mostly follows URTI- involves respiratory epithelium + paranasal sinuses- infection= hyperaemia + oedema of mucosa + blockage of sinus drainage- stasis predisposes to secondary bacterial infection: strep pneumoniase + h influenzae |
|
|
Acute rhinosinusitis: clinical features: |
Facial pain, headache, nasal obs, anosmia/cachosmia, halitosis, systemic upset, malaise, pyrexia, rhinorrhea with pus |
|
|
Acute frontal sinusitis: |
Pain above the eye, tenderness of the supraoribital margin, frontal headache especially on bending, infection spread easily to orbit, blindness can occur, can spread to cranial cavity causing extradural/intracranial abscess -> aggressive treatment with broad spectrum Abx + decongestants, if pt is slow to recover surgical drainage required |
|
|
Maxillary rhinosinusitis: |
Pain in cheek or upper teeth, tends to be unilateral |
|
|
Sphenoid infection |
retrorbital pain, or pain at the vertex of the head, pain can be referred to temporal region or whole head |
|
|
Tenderness on the first or second upper molar |
Sinusitis of dental origin |
|
|
Periorbital swelling |
May be presenting feature in ethmoidal sinus infection- May be due to periorbital cellulitis or abscess- serious - sight in jeopardy - IV abx and drainage - CT scan to demonstrate any intraorbital pus |
|
|
Rhinosinusitis- on examination: |
inflamed/oedematous nasal mucosa + mucopurulent secretions in the nasal cavity or posterior oropharynx |
|
|
Rhinosinusitis - investigations: |
Diagnosis is usually made on clinical history, Xray shows sinus opacificaion CT scan shows the extent of disease |
|
|
Treatment: rhinosinusitis |
-Analgesics, -team inhalation, -decongestant- xylometazoline spray- not for >5 days to avoid rhinitis medicamentosa (damage of the nasal vascualture resulting in rebound congestion + chronic nasal obstruction) - antibiotics - 3% difference in cure rate only - severe cases where symptoms >5 days- antibiotics recommended |
|
|
Treatment: acute maxillary sinusitis |
penicillin/amoxicillin for 7-14 days - check for resistance after 5 days |
|
|
Surgical treatment: rhinosinusitis |
If progressive pain: maxilliary sinus washout or trephining (making a hole) in the frontal sinus |
|
|
Symtoms of rhinosinusitis complications: |
periorbital cellulitis, severe headaches, focal neuro signs and symptoms of meningitis |
|
|
Chronic rhinosinusitis: pathology |
Staph aureus, coagulase negative staphylococcus, anaerobic and gram-negative bacteria predominate. Hypertrophic mucosa, secretions, eosinophila but no evidence of allergy
|
|
|
Chronic rhinosinusitis: Clinical features
|
Duration>12 weeks, Nasal obstruction, discoloured discharge (nasal or postnasal), anosmia/cachosmia, intermittent frontal pain, painless, but pain exacerbation on URTI, when flying, purulent secretions around the clock- examination: mucosal swelling, inflammation and dsicharge, nasal polyps, red and senstive inferior turbinate |
|
|
Allergic rhinitis: clinical symptoms: |
nasal obstruction, hyposmia, nasal irritation, sneezing, yellow nasal mucus due to eosinophil staining, pale swollenturbinates occasinally red mucosa - yellow secretions in late onset asthma - green secretions - chronic infective rhinosinusitis |
|
|
Treatment: chronic rhinosinusitis: |
Course of broad spectrum oral antibiotics eg co-amoxiclav, clindamycin or a combination of metronidazole + penicillin is given for at least 3 weeks, Topical nasal steroids: betamethasone drops, given for 2 months followed by a steroid nasal spray - take nasal drops when lying off a bed hanging upside down - can be continued > 8 weeks if there is an improvement Nasal douching Treat co-existing pathology- allergic rhinitis, nasal polyps, - allergen avoidance, antihistamines, oral steroids |
|
|
Referal for surgical treatment for chronic rhinosinusitis: |
If no improvement after 8 weeks of medical therapy, nasendoscopy, CT scan with a view to surgery. Functional endoscopic sinus surgery (FESS)- Drainage pathways of sinuses cleared- 91% improvement rate, may need to continue topical nasal medication after surgery as often its a systemic disease affecting the lining |
|
|
Commonest cause of facial pain: a) is b) symptoms c) treatment |
a) midfacial segment pain b) symmetrical sensation of pressure sometimes described as blockage, but no airway impairement, tension type headache c) low dose amytriptylline- takes 6 weeks to work and needs 6 months of treatment |
|
|
Nasal douching: a) what b) procedure c) after douching |
a) 1/2 teaspoon salt, 1/2 teaspoon sugar, 1/2 teaspoon bicarb of soda in 2 pints of boiled water left to cool b) block off one nostril with a finger and sniff/squeeze up the solution into the other nostril allowing it to run out after c) take nasal drops/sprays after douching |
|
|
Complications of infective sinusitis: |
1) chronic sinusitis 2) osteomyelitis 3) peri-orbital cellulitis + orbital abscess- commonest serious complication, direct/blood bourne spread, ethmoid sinus seperated from orbit by thin bone 4) facial cellulitis 5) mucoceles |
|
|
Management of peri-orbital cellulitis/orbital abscess: |
- High dose IV antibiotics + obs - monitor colour vision, visual acuity, eye movements, CT scan may be required |
|
|
Mucocele: a) what b) presentation c) treatment |
a) late complication of acute sinusitis, collections of sterile mucus occupying an obstructed sinus - especially frontal and ethmoidal b) facial swelling, visual disturbances due to displacement of eye/2ndy infection c) endoscopic surgical drainage |
|
|
Intracranial complications of rhinosinusitis: |
meningitis- most common cavernous sinus thrombosis brain abscesses extradural abscess subdural abscess |
|
|
Cavernous sinus thrombosis: a) pathology b) symptoms c)signs d) treatment |
a) spreading thrombophlebitis from frontal/ethmoidal/sphenoid sinuses, decreased venous return from eye b) swelling of the orbit, congestion of retinal vessels, fever + rigors, severe headache, reduced LOC, cerebral irritation c) 3rd, 4th, 6h nerve palsy- opthalmoplegia, parasethesia of opth + max division of 5th, symptoms may become bilateral d) high dose Abx - still high associated mortality |
|
|
Brain abscess secondary to frontal sinusitis: a) symptoms b) treatment |
a) change in personality, headaches, grand mal convulsion b) neurosurgical drainage/aspiration |
|
|
Extradural abscess- secondary to frontal sinusitis: a) investigation b)treatment |
a) CT scan shows a dehiscence of the posterior wall of the frontal sinus b)drainage of the frontal sinus |
|
|
Subdural abscess: secondary to frontal sinusitis: a) symptoms b)prognosis |
a) general malaise, headache, neck stiffness, signs of raised intracranial pressure - examination + CT b) poor |
|
|
Croup= laryngotracheobronchitis a) what b) causative organisms c) symptoms |
a) diffuse inflammation of the airway- oedema and vascular engorgement, particularly of subglottis, affects larynx in children 6 months to 3yrs b) parainfluenza, RSV, adenoviruses, rhinoviruses c) worse at night, lasts 3-7days, follows low grade resp tract infection, stridor, deterioration of child and toxicity, brassy cough like bark of dog, recession signals significant subglottic oedema and life threatening |
|
|
Croup- examination- look for: |
inspiratoruy stridor, retractions, air entry, cyanosis, LOC |
|
|
Croup- management based on modified Wesley croup score: a) <3- mild b)4-8-mod c)>8-severe |
a)supportive treatment at home b)hospital treatment- observation, nebulised racemic adrenaline, systemic steroids (dex single dose), +/- abx c) heliox (helium + oxygen), nebulised racemic adrenaline, systemic steroids (dex/pred/budesonide), intubation, +/- antibiotics |
|
|
Acute epiglottitis: a) causative agent b) pathology c) cardinal features in children |
a) Haemophius influenzae type b, HiB b) marked erythema and oedema of the epiglottis, often extending to the larynx c) Starts as URTI, child unwell, toxic, lethargic + febrile, young children drool as they have difficulty swallowing, stridor can develop rapidly and be followed by respiratory arrest |
|
|
Acute epiglottitis: in adults |
Severe sore throat, pain on swallowing, hot potato voice |
|
|
Acute epiglottitis- management to avoid airway obstruction: |
- don't upset the child - don't try to examine the throat - don't send for xrays - sit patient up |
|
|
Acute epiglottitis- management in suspected cases: |
direct laryngoscopy, endotracheal intubation for 3-4days after gas induction, blood culturesm heliox, Iv antibiotics- ceftrixone, IV steriods |
|
|
Rare infective conditions involving the larynx: |
Recurrent respiratory papillomatosis (HPV virus), TB, diptheria (cornybacterium diptheriae), herpes |
|
|
Laryngeal trauma: a) eg b) signs c) management |
a) car accidents where neck hits steering wheel/dashboard, stab wounds, kick boxing b) stridor= bad sign, referral should be madebut delayed laryngeal oedema can also occur, neck bruising, surgical emphysema indicated breech in resp airway in neck/mediastinum c) compromised airway- intubate/tracheostomy, antibiotics to prevent perichondritis, smoke inhlatation injuries can result in delayed laryngeal oedema, chest xray and min 24hrs observation |
|
|
Tracheostomy- indications: Obstruction in the voice box eg |
epiglottitis, benign/cancerous growths, anaphylaxis, inhaled objects, obstructive sleep apnoea |
|
|
Tracheostomy- other indications: |
Swelling of the tissues after major surgery, allowing easier removal of secretions from the airway + preventing scarring scarring from long term artifical ventilation, preventing overspill of secretions into lungs, providing alternate means of air entry after laryngectomy- end tracheostomy |
|
|
End tracheostomy: |
Part of laryngectomy, open end of the trachea is sutured to the edge of the skin in the lower neck seperating the lower airway from the upper airway - stoma formed - artificial humidification eg filters attatched over stoma |
|
|
Tracheostomy: Risks + complications- |
Early- tube displacement, blocked tube from secretions/clot, pneumothorax, surgical emphysema. Late- tracheocutaneous fistula on removal, tracheoesophgeal fistula, tracheal stenosis |
|
|
Stridor: a) define b) level of narrowing of the air passages |
a) noisy breathing b)inspiratory stridor- laryngeal level expiratory stridor- wheeze of asthma (bronchi/bronchioles), mixed inspiratory + expiratory stridor= tracheal or laryngeal and lower airways |
|
|
Stertor- what: |
noises produced at level of oro/nasopharynx ie snoring |
|
|
Causes of stridor: a) congenital b) acquired |
a) laryngomalacia, vocal cord palsy, vocal cord web, subglottic stenosis b) trauma, foreign body, angioedema, epiglottitis, croup, vocal cord palsy, laryngeal carcinomas, subglottic stenosis, laryngeal papillomata, large laryngeal polyps/cysts, external compresion eg thyroid mass |
|
|
Stridor- management: |
basic history, first aid, assess severity of stridor, improve + secure airway as necessary, investigate and treat underlying cause as necessary |
|
|
Stridor- assessment of severity: |
Mild- only on exertion/deep inspiration mod- audible all the time but able to hold a normal conversation, has to talk in short phrases, severe- only able to get odd words out as concentrating on breathing, unable to talk, using acc mm of respiration, cyanosed, respiratory arrest |
|
|
Managing airway obstruction - first aid measures: |
-Resp arrest- clear mouth + oropharynx of vomit, dentures or foreign bodies by suction or sweeping the airway with a gloved finger - if cyanosed + still breathing give heliox - Using brown IV cannulae- atatch syringe - palpate thryroid cartilage- find cricothyroid groove beneath lower edge of thyroid cartilage- insert cannula through cricothyroid membrane- aspirate air with syringe to confirm in lumen - remove syringe and place high flow oxygen/heliox over cannula |
|
|
Snoring- what: |
Vibration and partial collapse of the lax upper airway in sleep eg soft palate across posterior pharyngeal wall or nasopharyngeal or tongue base obstruction |
|
|
Obstructive sleep apnoea a) complete b) partial |
a) cessation of airflow in sleep lasting >10 secs
b) =hypopnoae= 10 second period where ventilation is reduced by more than 50% |
|
|
Causes of sleep apnoea: |
central- neurological obstructive- most common combination |
|
|
OSA- prognosis: |
Increased mortality from cardiovascular causes- up to 23 times increased risk of a cardiac event + RTAs due to falling asleep |
|
|
OSA- risk factors: |
Obesity- collar size >17 inches, more common in in men with fat distributede over neck + chest, sedatives eg alcohol/AD's exacerbate the problem, smokers, middle age |
|
|
OSA- pathophysiology: |
Mm relaxation in the deep stages of sleep in the upper airway causing complete airway collapse, decreased oxyhaemaglobin and increased CO2, changes detected by chemoreceptors causing increased central stimulation + arousal and restoring mm tone of the airway to increase oxyhb levels |
|
|
OSA- presentation: |
Obese males, heavyt snorers in the lighter stages of sleep, 'stop breathing' during sleep as reported by partners, pt doesn't feel rested, headaches, falling asleep at inapropriate times, chronic OSA- cardio complications, HTN, cor pulmonale/RHF |
|
|
ENT causes of OSA: |
Dental occlusion- retrognathia/midface hypoplasia, nasal obstruction- septal deviation/polyps/rhinitis, oropharyngeal obs- tonsillar enlargement, lax soft palate, pharynx- excessive fat deposition/ collapse on inspiration |
|
|
OSA- investigations: |
Polysomnography- gold standard, pt admitted to sleep lab, EEG, EMG, ECG, airflow at nose and lips, abdo + chest movements, 02 sats. Sleep nasoendoscopy: for snoring or mild OSA prior to surgical intervention - pt lighted sedated and nasoendoscopy pinpoints the site of collapse |
|
|
OSA- general management: |
Loose weight, correct ENT abnormalities |
|
|
OSA- management of moderate to severe OSA: |
CPAP overnight via nasal mask- keeps airway inflated, reverses tiredness and cardio SE's, 50% compliance. Mandibular advancement appliances: dental splints worn at night which advance the mandible in a jaw thrust to pull the tongue base + soft palate away from the pharyngeal wall |
|
|
OSA- surgery: a) for b) explain c) severe OSA |
a) snoring + mild OSA b) EG Laser assisted uvuloplasty- uvelo pharyngopalatoplasty produces scarring of the soft palate- increases stiffness- decreases vibration + reomval of tonsils c) if pts can't tolerate CPAP tracheostomy may be required |
|
|
OSA in children: a) cause b) presentation c) diagnosis d) management |
a)adeno-tonsillar hypertrophy, maxillary/mandibular disproportion, children with NM disorders b)parents concerned about child stopping breathing in sleep, may present with bed wetting, daytime hyperactivity, night sweating, conduct disorders c) clinical examination, sleep study d) adeno-tonsillectomy |
|
|
Facial nerve: a) exit b) Branches |
a) from pons/medulle b) Motor root = facial nerve proper- innervates the mm of facial expression Nervus intermedius- carries taste, parasympathetic + somatic sensory fibers 1- Greater petrosal nerve= secretormotor fibers to salivary glands of head + neck except parotid- from sup salivary nucleus 2- nn to stapedius mm- 3- chorda tympani - taste fibers from anterior tongue |
|
|
Greater petrosal nerve supplies: |
taste fibers from the palate, preganglionic parasymp fibers to lacrimal gland, secretomotor fibers to parotid |
|
|
Branch to the stapedius mm |
motor part of stapedius reflex- prevents excess movement due to loud noise |
|
|
Chorda tymapni |
taste fibers from the tongue via the lingual nerve- joins the vagus and glossopharyngeal nn |
|
|
Postauricular nn- |
motor mm of the ear, occipital belly of occipitofrontalis |
|
|
All branches of facial nn: |
Greatr petrosal nn, branch to stapedius mm, chorda tympani, postauricular nn, branches to posterior belly of the digastric + stylohyoid mm |
|
|
Intrapetrous course of the facial nn |
1) posterior cranial fossa 2) IAM 3) Petrous temporal bone- medial surface of the middle ear 4) first genu- nn turns posteriorly at geniculate ganglion 5) 2nd genu- nn turns again to travel inferiorly through mastoid bone 6) exits skull at stylomastoid foramen 7) enters parotid gland |
|
|
Terminal branches of the facial nn: |
Tempral, zygomatic, buccal, marginal mandibular, cervical |
|
|
Cutaneous branches of the facial nn: |
With auricular branch of vagu- supplies both sides of the pinna + EAM + tympanic membrane, fibers carried in nn intermedius with CN8- pharyngeal pathology is associated with otalgia |
|
|
Facial nn palsy- mainfestations: |
facial mm weakness- UMN= damage above facial nn nucleus, sparing of the movement of the forehead mm LMN- total facial weakness |
|
|
Scale for assessing facial weakness: |
House Brackmann- scale: 1- normal 2- slight weakness 3- obvious weakness, not disfiguring 4- severe reduction in movement, incomplete eye closure 5- asymmetry at rest, motion barely perceptible 6- asymmetry at rest and no facial movement |
|
|
Facial nn palsy- symptoms: |
Eye closure, drooling, hyperacusis, deafness, ottorhea, otalgia, vertigo, tinnitus, CVA, MS, GB, infection, sarcoid, skull base injuries, stab injuries, signs of ear infection/trauma, parotid mass, oral cavity vesicles/palatal weakness/displaced tonsil |
|
|
Facial nn palsy- investigations: |
pure tone audiogram, stapedial refleexes, electroneurography, MRI/CT |
|
|
Conditions causing facial nn palsy in children: |
- Moebius syndrome: bilateral 6,7 and uni or bilateral 12th nn palsy - Hemifacial microsmia: unilateral 7th-Acquired: forceps delivery, Herpes zooster virus, acute ottitis media |
|
|
Conditions causing facial nn palsy in adults in children: |
Peripheral: trauma, iatrogenic (parotid/submandibular gland surgery), tumours eg malignant parotid + lymphoma, inflammatory parotid- sarcoidosis Middle ear: iatrogenic: mastoid surgery, ear surgery, infection: cholesteatoma, acute otitis media, mastoiditis, herpes zooster, tumours: SCC, rhabdomyosarcoma, glomus jugulare or glomud tympanicum Petrous temporal bone: trauma: transverse skull fractures, tumours: SCC, mets, cholesteatoma Intracranial: tumours: acoustic neuromas, facial nn neuromas, meningioma, carcinomatous meningitis, iatrogenic: skull base surgery, vascular: stroke, neuro: MS |
|
|
Bell's palsy: what |
Idiopathic LMN palsy of CN7, incidence 20/10,000. Taverner's criteria: 1)acute onset: few hrs, complaint of aching 2) hemi facial 3) no CNS pathology or ear pathology |
|
|
Bell's palsy- presentation: |
Weakness of mm of facial expression and eye closure, facial sag- drawn to opposite eye on smiling, voluntary eye closure may not be possible, facial numbness, drooling of saliva, hyperacusis, change in taste, speech difficulty, decreased crying of tears, ocular complications eg corneal ulceration |
|
|
Bell's palsy- management + course: |
- usually resolves in <2 months, 90% pts have full return of facial nn function - oral steroids speed up recovery - oral prednisolone 60mg daily and weaned off over 2 weeks - aciclovir to treat HSV - eye care: hypromellose drops + larcrilube, eye tape - surgical decompression if unlikely to recover spontaneously |
|
|
Ramsay Hunt syndrome: cause |
Herpes zooster otticus, caused by reactivation of VZV in geniculate ganglion, common in immunosuppressed + elderly |
|
|
Ramsay Hunt syndrome: |
- facial palsy, often severe and irreversible, early treatment with high dose antivirals improves prognosis - Facial + ear pain often preceeds palsy - vesicles: ear canal, pinna + soft palate - other cranial nerve involvement: +/- sensorineural deafness, +/- tinnitus, +/- vertigo, +/- taste |
|
|
Ramsay Hunt syndrome: |
- eye care
- steroids- pred- 60mg - antivirals- acyclovir |
|
|
Facial paralysis due to parotid disease: |
Stretch injury due to disturbance in vasa nervorum - causes temporary facial nn weakness which will return to normal- advise eye protection/ drops/ opthalmic ointment |
|
|
Surgery for permenant facial nn weakness |
Facial slings using fascia lata of thigh suspended from corner of mouth to zygomatic arch |
|
|
Midline neck masses: |
submental lymphadenopathy, plunging ranula, thyroglossal cyst, thyroid mass |
|
|
Lateral neck masses: |
salivary gland enlargement, branchial cyst, cystic hygroma, carotid body tumour, lymphadenopathy, thyroid mass |
|
|
Branchial cysts: a) what b)Presentation c)diagnosis d)management |
a) Closure of upper and lower parts of 2nd branchial cleft but failure of fusion in the middle b) late adolesence/early adulthood, aysymtommatic/smooth swellings emerging from upper SCM, may present 2ndy to infection after resp infection as hot and tender masses c) US scan- irregular areas sampled by FNAC d) surgical excision under GA |
|
|
Thyroglossal cysts: a) what b) presentation c) diagnosis d) management |
a) residual cells from descent of thyroid gland which may form cystic lesions in adulthood b) in 2nd decade as a midline swelling, may be asymptommatic + present 2ndry to infection, lesion attatched to tongue base + elevates on protrusion c) US= diagnostic, if doubt FNAC d) if symptommatic- surgical excision including removal of body of hyoid to prevent recurrence (cyst occurs below hyoid) |
|
|
Thyroid cancer a) risk factors b) history c)examination d) diagnosis |
a) female, exposure to ionising radiation, fhx of thyroid cancer b)rapid growth, hoarseness c) hard, fixed texture, cervical lymphadeonpathy, vocal cord paralysis d) FNAC under US guidance, features on US scan: microcalcification, irregularity, haphazard vascularity, lymphadenopathy. Markers includes: increased calcitonin (medullary thyroid ca) |
|
|
Thyroid cancer- histological types + prevelance: |
1) papillary thyroid ca- 80% 2)follicular- 10% 3) medullary- 7% 4) undifferentiated - Anaplastic 2% |