Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
178 Cards in this Set
- Front
- Back
|
Why learn basic clinical skills?
|
70% of diagnoses can be made based on history alone. 90% of diagnoses can be made when the physical exam is added.
|
|
|
What are the four types of data collection?
|
1/ complete/classic (traditional history and physical)
2/ episodic 3/ follow-up 4/ emergency |
|
|
"classic" history and physical
|
introductory Information
CC- chief complain HPI- history present of illness PMH- past medical history current health social, occupational, family history functional assessment (ADLs, IADLs) ROS- review of systems PE- physical exam |
|
|
analysis of a symptom
|
OPQRSTU- onset, provocation/palliative, quality/quantity, radiation/relief, severity, time, understanding
|
|
|
PMH
|
general health, childhood illnesses, adult illnesses, obestetric/contraceptive history, psych, accidents/injuries
|
|
|
gravida
|
number of pregnancies, regardless of whether they were carried to term
|
|
|
para
|
number of live births
|
|
|
abortus
|
number of pregnancies that were lost for any reasons, i.e. miscarriages and abortions
|
|
|
current health
|
medications, allergies, habits, screening tests, sleep patterns, exercise/leisure, diet, environmental, use of safety measures
|
|
|
How many generations should a family history include?
|
3!
|
|
|
palpation
|
purpose is to confirm points you noticed during inspection; assess texture, moisture, temperature, organ location and size, masses, pulsations, crepitus, tenderness
|
|
|
Which parts of the hands should you use for fine discriminations, temperature, and vibrations?
|
tips, dorsal, palmar aspects of mcp joints or ulnar surface
|
|
|
What are the four assessment techniques? List in the order of performance.
|
1/ inspection
2/ palpation 3/ percussion 4/ auscultation |
|
|
What is the special case for abdominal exams?
|
Inspect and listen before you touch!
|
|
|
percussion
|
gently tap part of body w/ finger or instrument
|
|
|
When would you directly percuss? When would you indirectly percuss?
|
The only time you directly percuss is when assessing the thorax of a child's sinuses. Indirect percussion for everything else.
|
|
|
sounds via percussion
|
tympani- found in abdomen
resonance- air-filled lung/organ, is normal dullness- dense organs (e.g. liver, spleen) flatness- bone, tumor |
|
|
Which method yields the most physical signs?
|
Inspection: although the least mechanical, it provides an enormous amount of information.
|
|
|
auscultation
|
listening to internal organs of the body
|
|
|
diaphragm v. bell
|
diaphragm- higher pitch sounds v. bell- lower pitch sounds
|
|
|
vital signs
|
-height/weight measurement; head circumference for peds
-temperature -pulse -respiration -BP -pain |
|
|
body mass index (BMI): adults v. peds
|
weight (kg) / height (m)2
*always check if patient has weight problem or CHF peds use percentiles (obese > 95) |
|
|
pulse
|
measures stroke volume
60-100; <60 is bradycardia; >100 is tachycardia assess for rate, rhythm, quality (force), elasticity listen to heart if rhythm is irregular |
|
|
How to rate quality of pulse?
|
1+ thready, e.g. shock
2+ normal pulse 3+ bounding, e.g. s/p exercise |
|
|
influences on temperature
|
1/ diurnal cycle- lowest @ AM, highest @ PM
2/ menstrual cycle- 0.5 increase during ovulation 3/ exercise 4/ age- geriatric is usually one degree > adult |
|
|
respiration
|
infants: 30-40
adults: 10-20 *usually 1/4 of pulse |
|
|
temperature
|
average oral: 37 C or 98.6 F
rectal: 0.5 C or 1F > oral axillary: 0.5 C or 1F < oral tympanic: 0.8 C or 1.4 F > oral |
|
|
BP
|
"pressure of blood against the wall"
systolic pressure- max pressure felt on wall during ventricular systole (when heart contracts) diastolic pressure- elastic recoil/resting pressure during diastole |
|
|
influences on blood pressure
|
age- BP rises as we get older (thickening of artery)
gender- women < men after puberty until menopause race- blacks are 2x HTN than white diurnal- higher in PM higher in obese, during stress, exercise peripheral vascular resistance & elasticity volume/viscosity or circulating blood cardiac output |
|
|
auscultatory gap
|
silent interval that may be present b/w systolic and diastolic pressures
|
|
|
orthostatic hypotension
|
drop in systolic pressure > 20 mmHg
pulse increase >20 bpm *usually occurs when patient is bleeding; should take vitals in supine, sitting, and standing |
|
|
What is the approach for pediatric physicals?
|
QUIET TO ACTIVE
|
|
|
T/F. Adolescents can consent to pregnancy and drug testing.
|
True
|
|
|
What is the approach for adolescents?
|
HEADSSS- home, education, activities, drugs, sexuality, safety, suicide
|
|
|
peds growth curve v. preemies growth curve
|
measure height/weight for every well visit
>dropping off curve is bad; starting out on lower end, but following the curve is not as concerning v. preemie growth charts which corrects for age through age 2 |
|
|
When do you start a new growth chart?
|
after age 2
< 2, measure length- patient is lying down > 2, measure height- patient is standing up measure head circumference until age 2 |
|
|
peds temperature routes/variations
|
*rectal is most accurate
temporal- not accurate under 3 mos tympanic- not accurate under 6 mos |
|
|
peds heart rate
|
apical pulse is the most accurate for children younger than 2
|
|
|
peds BP
|
*start measuring @ age 3
BP will get higher as child gets older HTN if child is >95% in height, weight, age, or gender group |
|
|
bones of face and cranium
|
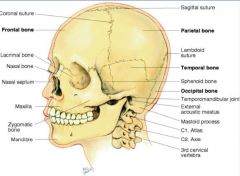
bones unite @ sutures (immovable joints)
cranium is supported by C1-C7 |
|
|
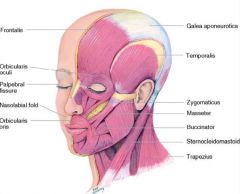
facial muscles
|
|
|
|
acromegaly
|
brow prominent, soft tissues of nose, ears, and lips are enlarged, prominent jaw
*anterior pituitary gland problem |
|
|
fetal alcohol syndrome
|
nose: widen bridge, flat, upturned
|
|
|
bell's palsy
|
*damage to facial nerve- lose movement @ top and bottom of face (e.g. close eyes, raise eyebrows)
patients who are unable to close eyes w/ long term bell's palsy have weight placed so they don't get too dry stroke patients can close/open eyes; raise eyebrows |
|
|
temporomandibular joint
|
below temporal artery, anterior to tragus
*most active joint in body; decrease ROM- arthritis; click- miniscus tear, poor occlusion or synovial swelling |
|
|
When palpating the temporal artery, what are you assessing for?
|
should not feel indurated (hard) or tortuous (wavy)
|
|
|
external eye structures
|

palpebral fissure- opening of upper and lower eye lid
pupil- where light enters iris limbus- border b/w cornea and sclera medial & lateral canthus caruncle- crease of eye |
|
|
anatomy of eye
|
tarsal plate- in lids to give structure/shape
meibomian glands- secrete oily substance to clear dust *conjunctiva- >bulbar- goes over sclera, clear but appears white >palpebral- lines the lids, clear but appears pink |
|
|
What does it mean when you see white on top of the eye when it is open?
|
Eye is protruding! The upper eye lid is more mobile than lower and should be able to cover the iris.
|
|
|
lacrimal apparatus
|
*provides constant irrigation
secretes tears >> puncta >> nasolacrimal sac >> nose |
|
|
What are the three layers of the eye?
|
1/ sclera- outer layer; white; covers iris & pupil
2/ choroid- middle layer; darkly pigmented; extremely vascular- delivers blood to retina 3/ retina- inner layer; visual center |
|
|
ciliary body
|
*controls thickness of lens, produces aqueous humor
bulges out for near objects flattens for far objects |
|
|
compartments of the eye
|
anterior- aqueous humor, how eye gets nutrients and gets rid of waste
posterior- vitreous humor is "gel-like" substance which can clog together to form "floaters" |
|
|
What are the extraocular muscles?
|
straight muscles: superior rectus, inferior rectus, lateral rectus, medial rectus
rotary muscles: superior oblique, inferior oblique *conjugate movement of eye prevents double vision |
|
|
CN VI
|
abducens
innervates lateral rectus (look out to side) |
|
|
CN IV
|
trochlear
innervates superior oblique (look down and in) |
|
|
CN III
|
oculomotor
innervates the rest: superior, medial, and inferior rectus & inferior oblique |
|
|
visual field
|
entire area seen by eye while looking at central point
when using both eyes- binocular, overlap when using one eye- monocular vision |
|
|
visual pathway
|
for image to be seen, light has to hit pupil and be perceived by sensory neurons @ retina
*images are projected upside down and reversed from right to left |
|
|
visual reflexes
|
pupillary light reflex- direct and consensual
light travel through CN II, splits at optic chiasm, sends message to both side of the brain, and response via CN III fixation- when looking straight ahead, fovea/macula is fixated accommodation |
|
|
snellen chart
|
20/50; can read at 20 feet what normal eye can read at 50 feet
20/200; legal blindness |
|
|
myopia v. hyperopia
|
myopia- nearsighted, eye too long
hyperopia- farsighted, eye too short |
|
|
strabismus
|
asymmetrical corneal light reflex
weakness/paralysis of one or more of the extraocular muscles, does not have conjugate vision |
|
|
ptosis
|
one eye drooping more than the other; could be CN or congenital problem
|
|
|
aniscia
|
unequal pupils
|
|
|
optic nerve cut prior to optic chiasm
|
unable to see; cannot get to occipital cortex
|
|
|
optic chiasm cut
|
bitemporal hemianopsia- lose vision in both temporal area
|
|
|
R optic tract cut
|
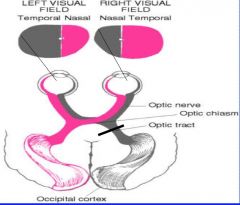
left homonymous hemianopsia- can see temporal w/ R eye and nasal w/ L eye
|
|
|
papilledema
|
inflammation of optic disk (becomes blurry and puffy) due to intracranial pressure
|
|
|
glaucoma
|
increased intraoccular pressure in anterior chamber of eye, cornea will be cloudy
|
|
|
structure of skin
|
epidermis, dermis, subcutaneous layer
|
|
|
epidermis
|
thin, outermost layer, avascular (nourished by dermis)
> stratum corneum- outer most horny cell layer- dead keratin cells > stratum germinativum- inner basal cell layer- living cells: keratin and melanocytes |
|
|
dermis
|
dense connective tissue layer forming the bulk of the skin
>chiefly collagen (resistant to tearing), elastin, hair follicles, glands, vascular |
|
|
subcutaneous layer
|
chiefly adipose tissue- thermal regulation
|
|
|
sweat glands
|
apocrine- active after adolescence, closely associated w/ hair follicles, coarse air, milky secretions, only active during sexual/emotional situations
eccrine- matures by 2 months, transparent secretion, goes directly to epidermis |
|
|
psoriasis
|

skin redness and irritation; most people with psoriasis have thick, red skin with flaky, silver-white patches called scales
|
|
|
pallor
|
loss of color; fear, cold
>anemia? |
|
|
erythema
|
redness of skin; excitement, embarrassment, hot
>localized infection >s/p exercise >poisoning >emotional event |
|
|
raynaud's disease
|
cold temperatures or strong emotions cause blood vessel spasms that block blood flow to the fingers, toes, ears, and nose
|
|
|
jaundice
|
yellowish pigmentation of skin; usually seen in mouth/eye before skin
>liver disease >hepatitis- sclera turns yellow >sickle cell |
|
|
cyanosis
|
decreased perfusion of tissue w/ oxygenated blood: blue
>shock >heart failure >chronic bronchitis |
|
|
vitiligo
|
melanocytes are devoid of color (MJ)
|
|
|
acanthosis nigricans
|
increased pigmentation; seen in adolescent/older adults who are insulin resistant
|
|
|
mongolian spots
|
hyper-pigmentation (blue, black, purple), starts to fade after year 1
common in Black, Asians, Native Americans |
|
|
acne
|
1/ comedonal- black or white heads
2/ pustular |
|
|
Explain the changes in skin in older adults.
|
They have less fat, vessels break easily, less elastin, and longer wound repair
>more wrinkling >senile purpura- easy bruising >xerosis- dry skin >senile lentigines- "liver spots" melanocytes clump together from sun exposure; not cancerous, no treatments |
|
|
edema
|
overaccumulation of interstitial fluid
possible affected system >circulatory >cardiovascular >kidney >lymphatic |
|
|
primary skin lesions
|
macula, patch
papule, plaque nodule, tumor wheal, urticaria vesicle, bulla cyst pustule |
|
|
macule v. patch
|
macule- flat, non palpable change in skin color, up to 1 cm
patch- macule larger than 1 cm |
|
|
papule v. plaque
|
papule- palpable, elevated, solid mass caussed by superficial thickening of epidermis, up to 0.5 cm
plaque- coalescence of papules, larger than 0.5 cm |
|
|
nodule v. tumor
|
nodule- solid, elevated, soft or firm mass less than 1-2 cm
tumor- larger than 1-2 cm, may extend deeper into dermis |
|
|
wheal v. urticaria
|
wheal- superficial, raised, erythematous, transient lesion w/ irregular borders due to localized edema; fluid is held diffusely in the tissues
v. urticaria- wheals coalescing, pruritic |
|
|
vesicles v. bullae
|
vesicle- cirumscribed, superficial elevated cavity; contains free fluid, up to 1 cm
bullae- larger than 1 cm; usually single chambered, thin wall, easily ruptured |
|
|
cyst
|
encapsulated fluid or pus-filled cavity in dermis or subcutaneous layer, larger than 1 cm
|
|
|
pustules
|
circumscribed, superficial, elevated cavity, contains turbid fluid (pus), up to 1 cm
|
|
|
secondary skin lesions
|
crust
scale fissure erosion ulcer excoriation scar atrophic scar lichenification keloid |
|
|
crust
|
thickened dried residue of burst vesicles, pustules or blood; red-brow, honey-colored, or yellow
|
|
|
scaling
|
compact desiccated flakes of skin; visible exfoliation of the dermis; shedding of dead excess keratin cells
|
|
|
fissures
|
linear crack w/ abrupt edges, extends into dermis; dry or moist
|
|
|
erosion v. ulcer
|
erosion- superficial circumscribed loss of epidermis; moist but no bleeding; heals w/o a scar; "stage 2 pressure sore"
ulcer- circumscribed depression extending into dermis; irregular shape; may bleed; scar |
|
|
excoriation
|
scratch mark, superficial
|
|
|
scar
|
replacement of destroyed normal skin tissue by fibrous connective tissue
|
|
|
atrophy
|
depressed skin level >> loss of tissue; thinning of epidermis w/ loss of normal skin resulting in shiny translucent skin
*like a scar, but depressed |
|
|
lichenification
|
thickening/roughening of skin (usually from scratching); results from tightly packed papules
|
|
|
keloid scar
|
hypertrophic; skin level is elevated by excess scar tissue, which is invasive beyond site of original injury
|
|
|
common shapes/configurations of lesions
|
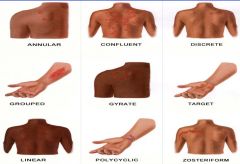
confluent- coalescing (edges overlap)
grouped- multiple lesions (edges don't overlap) gyrate- angled, tunneling (not straight) polycyclic- multiple round lesions zosteriform- following a dermatome |
|
|
vascular lesions
|
petechiae, purpura
ecchymosis cherry angioma spider angioma telangiestasia nevus flammeus "port wine stain" |
|
|
petechiae v. purpura
|
petechiae- red, pin sized macules of blood; < 3 mm
purpura- 0.3 to 1 cm *blood filled lesions do not blanch |
|
|
ecchymosis
|
escape of blood into tissues from ruptured blood vessels; small hemorrhagic spot in skin; non-elevated, blue/purplish patch; > 1 cm
*larger bruise |
|
|
cherry angioma
|
aka Campbell de Morgan spots
bright red papules; benign; common on trunks of middle-aged and elderly |
|
|
spider angioma
|
*if many on trunk, check liver function- possible deficiency; may be normal in children and pregnant women
stellate telangiectases radiating from central palpable feeding vessel |
|
|
telangiectasia
|
permanently dilated and visible vessels in the skin
*can be caused by nifedipine |
|
|
nevus flammeus
|
aka port wine stain, stork bite
present at birth, caused by dilated dermal capillaries; pale pink to purple macules; mostly on face or trunk |
|
|
skin warning signs
|
"ABCDE"
asymmetry border- irregular color- mottled diameter- unusually large (> 6 mm) elevation *enlargement |
|
|
basal cell carcinoma
|
most common malignancy
locally invasive and destructive slow growing, rarely metastasized translucent, dome-shaped papule with overlying telangiectasias |
|
|
actinic keratosis
|
yellowish; can progress into squamous cells
|
|
|
squamous cell carcinoma
|
invasive malignancy; common on head, neck, hands
"sore- heals and opens continuously" |
|
|
melanoma
|
superficial spreading or nodular; can be benign or malignant; usually dark from the pigments produced by melanocytes
|
|
|
What are the two types of hairs?
|
1/ vellus- fine faint hair covers most of body
2/ terminal- eyebrows, scalp, pubic, face, chest |
|
|
What happens to the hair as we get older?
|
Melanin gets replaced by colorless air bubbles, resulting in gray or white hair.
|
|
|
alopecia areata v. alopecia totalis
|
alopecia areata- non-scarring hair loss; usually an immunological phenomenon
alopecia totalis- total hair loss |
|
|
hirsutism
|
excessive hairiness @ sites where terminal hair does not normally occur (hair, face, thigh, abdomen); in women; check for hormones
|
|
|
What happens to nails as we age?
|
Nails are thickened, ridged and split in older adults.
|
|
|
measurement of nail angle
|
check for clubbing; associated w/ cystic fibrosis, cancer, lung disease
|
|
|
external ear structures
|
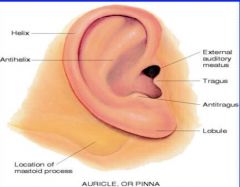
most skin cancer findings are in helix
tragus gets tender during infection |
|
|
anatomy of ear
|
1/ external ear- funnels sound waves to TM
2/ middle ear (MIS)- conducts sound vibrations, reduces amplitude of sound, equalization of air pressure 3/ inner ear- vestibular fx, bony, cochlear |
|
|
Where is the cone of light on the R and L ear on the TM?
|
R 5:00
L 7:00 |
|
|
What is the anatomic/developmental difference in the ears of infants?
|
Their eustachian tubes are shorter, wider, and more horizontal, making them more prone to infection.
|
|
|
otosclerosis
|
abnormal spongy bone growth in middle ear that causes hearing loss; more common in females than males
|
|
|
presbycusis
|
age-related hearing loss; tiny hairs get lost w/ age
|
|
|
What is the most efficient hearing pathway?
|
Air conduction is more efficient than bone conduction.
|
|
|
tinnitus
|
"ear ringing"
|
|
|
weber test
|
place 512 fork in midline of head; ask if sound is louder in one ear than other
|
|
|
rinne test
|
bone conduction- place on mastoid process
air conduction- outer ear |
|
|
Person with normal hearing ...
|
Weber- hear vibration equal bilaterally
Rinne- AC > BC (last longer) |
|
|
Person with conductive hearing lost ...
|
Weber- will lateralize to bad ear
Rinne- BC = AC; BC > AC common causes- fluid, ear wax, damage to ear drum |
|
|
Person with sensorineural loss ...
|
Weber- will lateralize to good ear
Rinne- AC > BC (decreased amount of time, same ratio) or they may not hear at all |
|
|
If pain when palpating mastoid process, what should you consider?
|
otitis media, mastoiditis
|
|
|
If pain when palpating tragus, what should you consider?
|
otitis externa
|
|
|
kiesselbach region
|
anteroinferior part of nasal septum; where four arteries anastomoses
*common site for nose bleeds |
|
|
structures of nasal cavity
|
anterior edge is lined w/ coarse nasal hairs- filters air; remainder is lined w/ ciliated mucous membranes to filter dust and bacteria
|
|
|
T/F. Nasal mucosa is redder than oral mucosa.
|
True; it has a larger blood supply
|
|
|
lateral wall turbinates
|
superior meatus- ethmoid cells
middle meatus- sinuses inferior meatus- tears |
|
|
sinuses
|
air-filled pockets within cranium to lighten weight of skull; we have for pairs of paranasal sinuses
|
|
|
epistaxis
|
nosebleeds
|
|
|
polyps
|
smooth gray nodules; overgrowth of mucosa; result of chronic allergies; non-tender; often removed b/c of breathing/snoring problems
|
|
|
perforated septum
|
cocaine use, excessive use of nasal spray
|
|
|
rhinitis
|
allergic or acute; pale inside; usually clear fluid, if pusy- possible sinus infection
|
|
|
palpate sinuses
|
get underneath sinus and push up
|
|
|
transillumination
|
shoot light through sinus >> red light if sinus is clear
|
|
|
oral cavity structure
|
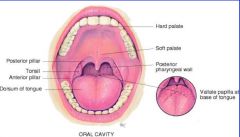
tonsils are b/w posterior and anterior pillar
adult- 32 teeth; children- 20 teeth |
|
|
salivary glands
|
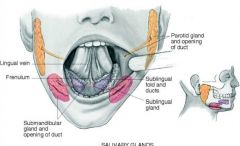
*moistens food
parotid, submandibular, sublingual |
|
|
stenson's duct
|
opening of parotid salivary gland; opposite upper second molar
|
|
|
wharton's duct
|
opening of submandibular salivary glands
|
|
|
normal findings of the mouth
|
fordyce spots- yellow inside cheeks
torus palatinus- roof of mouth scrotal tongue- multiple fissures geographic tongue- areas devoid of papillae |
|
|
CN XII
|
hypoglossal
tongue should protrude midline w/o tremors or deviation; if it does deviate >> will go towards paralyzed side |
|
|
CN X
|
vagus
"AHH" >> soft palate rises up and uvula stays midline |
|
|
grading tonsils
|
1+ visible
2+ halfway b/w pillars and uvula 3+ touching uvula 4+ touching each other |
|
|
viral pharyngitis
|
redness and vascularity of pillars and uvula; pt c/o of sore throat or scratchy throat
|
|
|
bacterial pharyngitis
|
red throat w/ exudate (pus) on tonsil; fever and enlarged cervical nodes; could be streptococcal infection
|
|
|
thyroid gland
|
endocrine gland w/ rich blood supply
thyroid cartilage (Adam's apple) cricoid cartilage isthmus lies over trachea at 2nd or 3rd tracheal ring |
|
|
lymph nodes
|
*removes impurities; @ interstitial tissue; all over body but can only assess them at neck, under the arm, and groin
palpate w/ tip of finger, soft circular motion swollen, tender- infection, inflammation, < 1 cm hard, unmovable- cancer, > 1 cm |
|
|
CN XI
|
spinal accessory; innervates sternomastoid and trapezius muscles (lift up shoulder against pressure)
|
|
|
List all the lymph nodes!
|
preauricular, postauricular, occipital
tonsillar, submandibular, submental superficial cervical, posterior cervical, deep cervical supraclavicular, infraclavicular |
|
|
If patient had the following conditions, where would you expect swollen lymph nodes? (eye infection, ear infection, hair dye, sore throat)
|
eye- preauricular
ear- postauricular, preauricular dye hair- occipital sore throat- tonsillar *always draining towards the heart |
|
|
abnormal trachea
|
if on one side >> collapse lung
if mass is pushing trachea >> bulge in neck |
|
|
When checking for carotid pulse, which parts do you check?
|
Always the lower third or the upper third--there is a sinus in the middle.
Listen for bruit (turbulent blood flow, "whoosh"), can hear if person has 70% occlusion) |
|
|
goiter (enlarged thyroid)
|
thickening throughout neck; could be hyperthyroidism, hypothyroidism, or uthyroidism (normal)
>> always feel for nodules; single nodule is more concerning for cancer |
|
|
T/F. Suture lines may not be palpable at birth.
|
True
|
|
|
fontanels
|
"soft spots"
*anterior- diamond shaped, 2 cm in term infants posterior- triangular shaped, may or may not be palpable |
|
|
Normal fontanels are soft/flat. What does it mean if it is bulging or sunken?
|
swollen- hydrocephaly
sunken- dehydration |
|
|
T/F. Term infant are hyperopic (farsighted) at birth.
|
True
|
|
|
red light reflex (bruchner test)
|
to detect disease processes preventing light from entering/exiting pupil
if cataracts >> will see black spots! |
|
|
leukokoria
|
whitish opacity of pupil w/ absent/partial red reflex
|
|
|
Explain the difference in ear assessment b/w peds and adults.
|
For peds, pull auricle inferiorly.
|
|
|
T/F. Sinuses are fully formed in children.
|
False; the continue to develop throughout childhood.
|
|
|
T/F. Children have larger tonsils than adults.
|
True
|
|
|
ankylglossia
|
shortened lingual frenulum; not usually repaired b/c it doesn't affect speech/feeding
|