Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
90 Cards in this Set
- Front
- Back
|
What is the most common location for leukocyte extravasation?
|
Post-capillary venules (sites of tissue injury and inflammation)
|
|
|
What are the four steps of leukocyte extravasation?
|
1. Margination and rolling
2. Tight-binding 3. Diapedesis 4. Migration |
|
|
What mediates the first step of leukocyte extravasation?
|
Margination and Rolling:
- E-selectin binds Sialyl-Lewis - P-selectin binds Sialyl-Lewis - GlyCAM-1, CD34 bind L-selectin |
|
|
What mediates the second step of leukocyte extravasation, after margination and rolling?
|
Tight-Binding
- ICAM-1 (CD54) binds CD11/18 integrins (LFA-1, Mac-1) - VCAM-1 (CD106) binds VLA-4 integrin |
|
|
What mediates the third step of leukocyte extravasation, after tight-binding?
|
Diapedesis - leukocyte travels between endothelial cells and exits blood vessel
- PECAM-1 (CD31) binds PECAM-1 (CD31) |
|
|
What mediates the fourth step of leukocyte extravasation, after diapedesis?
|
Migration - leukocyte travels through interstitium to site of injury or infection guided by chemotactic signals
|
|
|
What chemotactic products are release in response to bacteria to stimulate leukocyte migration?
|
- C5a
- IL-8 - LTB4 - Kallikrein - Platelet-actvating factor |
|
|
What mediates margination and rolling in leukocyte extravasation?
|
Vasculature / stroma:
- E-selectin - P-selectin - GlyCAM-1, CD34 Leukocyte: - Sialyl-Lewis - L-selectin |
|
|
What mediates tight binding in leukocyte extravasation?
|
Vasculature / stroma:
- ICAM-1 (CD54) - VCAM-1 (CD106) Leukocyte: - CD11/18 integrins (LFA-1, Mac-1) - VLA-4 integrin |
|
|
What is the term for when a leukocyte travels between endothelial cells to exit a blood vessel?
|
Diapedesis
|
|
|
What mediates diapedesis in leukocyte extravasation?
|
PECAM-1 (CD31) on both vasculature/stroma and leukocytes
|
|
|
How do free radicals damage cells?
|
- Lipid peroxidation
- Protein modification - DNA breakage |
|
|
What can initiate free radical damage?
|
- Radiation exposure (eg, cancer therapy)
- Metabolism of drugs (phase I) - Redox reactions - Nitric oxide - Transition metals - Leukocyte oxidative burst |
|
|
What enzymes can eliminate free radicals?
|
- Catalase
- Superoxide dismutase - Glutathione peroxidase |
|
|
Besides enzymes, what else can eliminate free radicals?
|
- Spontaneous decay
- Antioxidants (eg, vitamins A, C, and E) |
|
|
What pathologies are caused by free radical injury?
|
- Retinopathy of prematurity
- Bronchopulmonary dysplasia - Carbon tetrachloride, leading to liver necrosis (fatty change) - Acetaminophen overdose (fulminant hepatitis, renal papillary necrosis) - Iron overload (hemochromatosis) - Reperfusion injury (eg, superoxide), especially after thrombolytic therapy |
|
|
What free radical damage is associated with prematurity?
|
Retinopathy
|
|
|
How can the lungs be affected by free radical damage?
|
Bronchopulmonary Dysplasia
|
|
|
What are the effects of carbon tetrachloride?
|
Free radical damage → liver necrosis (fatty change)
|
|
|
What are the free radical effects of acetaminophen overdose?
|
Overdose → fulminant hepatitis and renal papillary necrosis
|
|
|
What mediates reperfusion injury?
|
Superoxide, especially after thrombolytic therapy
|
|
|
What is the most common pulmonary complication after exposure to fire?
|
Inhalation Injury:
- Inhalation of products of combustion (eg, carbon particles, toxic fumes) → chemical tracheobronchitis, edema, and pneumonia |
|
|
How long does it take for wound healing to get a majority of the tensile strength back to the tissue? What percentage of tensile strength?
|
Takes ~3 months following wound formation to get 70-80% of the tensile strength back (little additional strength will be regained after that)
|
|
|
What are the pathologic types of scars?
|
- Hypertrophic scars
- Keloid scars |
|
|
Which type of scar has greater collagen synthesis?
|
- Keloid Scars: ↑↑↑ collagen synthesis
- Hypertrophic Scars: ↑ collagen synthesis |
|
|
What is the arrangement of collagen in hypertrophic vs keloid scars?
|
- Hypertrophic: parallel collagen
- Keloid: disorganized collagen |
|
|
What is the extent of a hypertrophic vs keloid scars?
|
- Hypertrophic: confined to borders of original wound
- Keloid: extends beyond the borders of the original wound |
|
|
Do hypertrophic scars tend to recur following resection? vs keloid scars?
|
- Hypertrophic scars infrequently recur following resection
- Keloid scars frequently recur following resection |
|

What types of scars are these? Characteristics?
|

Keloid Scars
- ↑ collagen synthesis - Parallel collagen arrangement - Scar is confined to borders of original wound - Infrequently recurs following resection |
|

What types of scars are these? Characteristics?
|

Keloid Scars
- ↑↑↑ collagen synthesis - Disorganized collagen arrangement - Scar extends beyond the borders of the original wound - Frequently recurs following resection |
|
|
Who is at higher risk for keloid scars?
|
African-Americans
|
|
|
What are the tissue mediators of wound healing?
|
- PDGF
- FGF - EGF - TGF-β - Metalloproteinases |
|
|
What is the source of PDGF? Function?
|
PDGF is secreted by activated platelets and macrophages
- Induces vascular remodeling and smooth muscle cell migration - Stimulates fibroblast growth for collagen synthesis |
|
|
What is the function of FGF?
|
Stimulates all aspects of angiogenesis
|
|
|
What is the function of EGF?
|
Stimulates cell growth via tyrosine kinases (eg, EGFR as expressed by ERBB2)
|
|
|
What is the function of TGF-β?
|
- Angiogenesis
- Fibrosis - Cell cycle arrest |
|
|
What is the function of metalloproteinases?
|
Tissue remodeling
|
|
|
What factor induces vascular remodeling and smooth muscle cell migration?
|
PDGF (from activated platelets and macrophages)
|
|
|
What factor stimulates fibroblast growth for collagen synthesis?
|
PDGF (from activated platelets and macrophages)
|
|
|
What factor stimulates all aspects of angiogenesis?
|
FGF
|
|
|
What factor stimulates cell growth via tyrosine kinases?
|
EGF - via EGFR, as expressed by ERBB2
|
|
|
What enzyme is involved in tissue remodeling?
|
Metalloproteinases
|
|
|
What are the phases of wound healing?
|
1. Inflammatory (immediate)
2. Proliferative (2-3 days after wound) 3. Remodeling (1 week after wound) |
|
|
What is the immediate phase of wound healing? Mediators?
|
Inflammatory Phase
- Mediated by platelets, neutrophils, macrophages |
|
|
What is the phase of wound healing that occurs 2-3 days after a wound? Mediators?
|
Proliferative Phase
- Fibroblasts - Myofibroblasts - Endothelial cells - Keratinocytes - Macrophages |
|
|
What is the phase of wound healing that occurs 1 week after a wound? Mediators?
|
Remodeling Phase
- Fibroblasts |
|
|
What are the characteristics of the inflammatory phase of wound healing?
|
Immediately after wound:
- Clot formation - ↑ Vessel permeability and neutrophil migration into tissues - Macrophages clear debris 2 days later |
|
|
What are the characteristics of the proliferative phase of wound healing?
|
2-3 days after wound
- Deposition of granulation tissue and collagen - Angiogenesis - Epithelial cell proliferation - Dissolution of clot - Wound contraction (mediated by myofibroblasts) |
|
|
What are the characteristics of the remodeling phase of wound healing?
|
1 week after wound
- Type III collagen replaced by type I collagen - Increased tensile strength of tissue |
|
|
What bugs/pathologies can cause granulomas?
|
- Bartonella henselae (cat scratch)
- Berylliosis - Churg-Strauss syndrome - Crohn disease - Francisella tularensis - Fungal infections (eg, histoplasmosis, blastomycosis) - Granulomatosis with polyangiitis (Wegener) - Listeria monocytogenes (granulomatosis infantisepticemia) - M. leprae (leprosy; Hansen disease) - M. tuberculosis - Treponema pallidum (tertiary syphilis) - Sarcoidosis - Schistosomiasis |
|
|
What mediates the formation of a granuloma?
|
- Th1 cells secrete γ-interferon, activating macrophages
- Macrophages release TNF-α, which induces and maintains granuloma formation |
|
|
What can the side effects of anti-TNF drugs be?
|
Cause sequestering granulomas to breakdown, leading to disseminated disease
(TNF-α maintains granuloma formation) |
|
|
Which mediator activates macrophages? Source?
|
γ-Interferon from Th1 cells
|
|
|
What mediator from macrophages induces and maintains granuloma formation?
|
TNF-α
|
|
|
What do you need to check for before starting anti-TNF therapy? Why?
|
Latent Tuberculosis
- Anti-TNF drugs can cause sequestering granulomas to breakdown, leading to disseminated disease |
|
|
Which is thicker/thinner: exudate or transudate?
|
- Exudate (thick)
- Transudate (thin) |
|
|
What are the contents of an exudate?
|
- Cellular
- Protein rich |
|
|
What are the contents of an transudate?
|
- Hypocellular
- Protein-poor |
|
|
What is the relative specific gravity in an exudate vs transudate?
|
- Exudate: >1.020 (thick)
- Transudate: <1.012 (thin) |
|
|
What can cause an exudate?
|
- Lymphatic obstruction
- Inflammation / infection - Malignancy |
|
|
What can cause a transudate?
|
- ↑ Hydrostatic pressure (eg, CHF)
- ↓ Oncotic pressure (eg, cirrhosis) - Na+ retention |
|
|
What is the Erythrocyte Sedimentation Rate a reflection of?
|
- Products of inflammation (eg, fibrinogen) coat RBCs and cause aggregation
- When aggregated, RBCs fall at a faster rate within the test tube |
|
|
What can cause increased ESR?
|
- Most anemias
- Infections - Inflammation (eg, temporal arteritis) - Cancer (eg, multiple myeloma) - Pregnancy - Autoimmune disorders (eg, SLE) |
|
|
What can cause decreased ESR?
|
- Sickle cell (altered shape)
- Polycythemia (↑ RBCs "dilute" aggregation factors) - CHF (unknown) |
|
|
What is one of the leading causes of fatality from toxicologic agents in children?
|
Iron poisoning
|
|
|
What is the mechanism of iron poisoning?
|
Cell death due to peroxidation of membrane lipids
|
|
|
What are the acute symptoms of iron poisoning?
|
- Nausea
- Vomiting - Gastric bleeding - Lethargy |
|
|
What are the chronic symptoms of iron poisoning?
|
- Metabolic acidosis
- Scarring leading to GI obstruction |
|
|
How do you treat a patient with iron poisoning?
|
Chelation:
- IV deferoxamine - Oral deferasirox Dialysis |
|
|
What is the term for the abnormal aggregation of proteins (or their fragments) into β-pleated sheet structures? Implications?
|
Amyloidosis → damage and apoptosis
|
|
|
What are the common types of Amyloidsosi?
|
- AL (primary)
- AA (secondary) - Dialysis-related - Heritable - Age-related (senile) systemic - Organ specific |
|
|
What causes AL (primary) amyloidosis? Associated with?
|
- Deposition of proteins from Ig Light chains
- Can occur as a plasma cell disorder or associated with multiple myeloma |
|
|
What are the extent of the effects of AL (primary) amyloidosis?
|
Often affects multiple organ systems, including:
- Renal (nephrotic syndrome) - Cardiac (restrictive cardiomyopathy, arrhythmia) - Hematologic (easy bruising) - GI (hepatomegaly) - Neurologic (neuropathy) |
|
|
What causes AA (secondary) amyloidosis? Associated with?
|
Seen with chronic conditions:
- Rheumatoid arthritis - IBD - Spondyloarthropathy - Protracted infection Often multisystem |
|
|
What is AA (secondary) amyloidosis composed of?
|
Fibrils composed of serum Amyloid A
|
|
|
What are the extent of the effects of AA (secondary) amyloidosis?
|
Often multisystem involvement like AL amyloidosis
|
|
|
How does dialysis relate to amyloidosis?
|
Dialysis-Related Amyloidosis:
- Fibrils composed of β2-microglobulin in patients with ESRD and/or on long-term dialysis |
|
|
How might dialysis-related amyloidosis present?
|
Carpal tunnel syndrome
|
|
|
What is the amyloidosis in patients on dialysis composed of?
|
β2-microglobulin
|
|
|
What are the characteristics of heritable amyloidosis? Cause?
|
Heterogenous group of disorders
- Example is ATTR neurologic / cardiac amyloidosis due to transthyretin (TTR or prealbumin) gene mutation |
|
|
What causes age-related (senile) systemic amyloidosis?
|
Deposition of normal (wild-type) transthyretin (TTR) in myocardium and other sites
|
|
|
How does the rate of cardiac dysfunction compare in age-related amyloidosis and AL amyloidosis?
|
Age-related amyloidosis has a slower progression of cardiac dysfunction relative to AL amyloidosis
|
|
|
What is the most important form of organ-specific amyloidosis? Cause?
|
Alzheimer Disease
- Deposition of amyloid-β protein cleaved from amyloid precursor protein (APP) |
|
|
What type of amyloidosis is associated with T2DM? Cause?
|
Islet Amyloid Polypeptide (IAPP) - type of organ-specific amyloidosis
- Commonly seen in T2DM - Caused by deposition of amylin in pancreatic islets |
|
|
What type of disease is caused by deposition of amylin in the pancreatic islets?
|
Islet Amyloid Polypeptide (IAPP) - organ-specific amyloidosis commonly seen in patients with T2DM
|
|
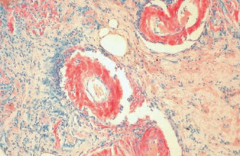
What does this image show?
|
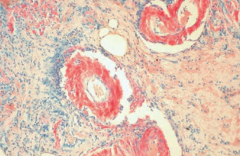
Amyloidosis:
- Congo red stain shows amyloid deposits within vessel walls |
|
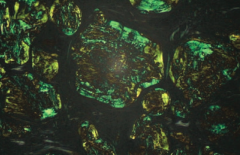
What does this image show?
|
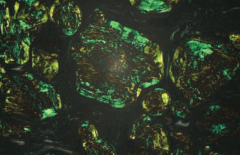
Amyloidosis
- Congo red stain shows apple green birefringence under polarized light |
|
|
What is the name of the yellow-brown "wear and tear" pigment associated with normal aging?
|

Lipofuscin
- Macrophages with granular yellow-brown pigment |
|
|
What is the cause of Lipofuscin deposition in macrophages?
|
Formed by oxidation and polymerization of auto-phagocytosed organellar membranes
|
|
|
Where will you find Lipofuscin in an autopsy of an elderly person?
|
- Heart
- Liver - Kidney - Eye - Other organs |