Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
164 Cards in this Set
- Front
- Back
|
What are the types of Seronegative Spondyloarthropathies?
|
PAIR:
- Psoriatic arthritis - Ankylosing spondylitis - Inflammatory bowel disease - Reactive arthritis (Reiter syndrome) |
|
|
What are the characteristics of arthritis in a patient with psoriasis?
|

- Joint pain and stiffness
- Asymmetric and patchy involvement - Dactylitis ("sausage fingers") - "Pencil-in-cup" deformity on x-ray |
|
|
How common is arthritis in patients with psoriasis?
|
1/3 of patients with psoriasis
|
|
|
What disease has the classic presentation of rash, joint pain, and fever?
|
Systemic Lupus Erythematosus
|
|
|
What mnemonic can help you remember the characteristics of Systemic Lupus Erythematosus?
|
RASH OR PAIN:
- Rash (malar or discoid) - Arthritis - Soft tissues / Serositis - Hematologic disorders (eg, cytopenias) - Oral / nasopharyngeal ulcers - Renal disease, Raynaud phenomenon - Photosensitivity, Positive VDRL/RPR - Anti-nuclear antibodies - Immunosuppressants - Neurologic disorders (eg, seizures, psychosis) |
|
|
What are the common causes of death in patients with Systemic Lupus Erythematosus?
|
- Cardiovascular disease
- Infections - Renal disease |
|
|
What kind of cardiac disease is associated with Systemic Lupus Erythematosus?
|
Libman-Sacks Endocarditis: wart-like vegetations on boths ides of valve
|
|
|
What kind of renal disease is associated with Systemic Lupus Erythematosus?
|
Lupus Nephritis (Type III hypersensitivity reaction):
- Nephritic: diffuse proliferative glomerulonephritis - Nephrotic: membranous glomerulonephritis |
|
|
What kinds of antibodies are associated with Systemic Lupus Erythematosus?
|
- Anti-nuclear antibodies (ANA)
- Anti-dsDNA antibodies - Anti-Smith antibodies - Anti-histone antibodies - Anti-cardiolipin antibodies |
|
|
What antibody is sensitive, but not specific for Systemic Lupus Erythematosus?
|
Anti-nuclear antibodies (ANA)
|
|
|
What antibody is specific and indicates a poor prognosis (renal disease) for Systemic Lupus Erythematosus?
|
Anti-dsDNA antibodies
|
|
|
What antibody is specific, but does not offer prognostic information?
|
Anti-Smith antibodies (directed against snRNPs)
|
|
|
What antibody is sensitive for drug-induced lupus?
|
Anti-histone antibodies
|
|
|
What antibody shows false positives for patients with syphilis and prolongs the PTT in patients with Systemic Lupus Erythematosus? Implications?
|
Anti-Cardiolipin antibody
- Pardoxically prolonged PTT, increases risk for arteriovenous thromboembolism |
|
|
What antibody increases the risk of arteriovenous thromboembolism?
|
Anti-cardiolipin antibodies
|
|
|
How is complement affected in Systemic Lupus Erythematosus?
|
Decreased C3, C4, and CH50 due to immune complex formation
|
|
|
How do you treat patients with Systemic Lupus Erythematosus?
|
- NSAIDs
- Steroids - Immunosuppressants - Hydroxychloroquine |
|
|
What mnemonic can help you remember the characteristics of Systemic Lupus Erythematosus?
|
RASH OR PAIN:
- Rash (malar or discoid) - Arthritis - Soft tissues / Serositis - Hematologic disorders (eg, cytopenias) - Oral / nasopharyngeal ulcers - Renal disease, Raynaud phenomenon - Photosensitivity, Positive VDRL/RPR - Anti-nuclear antibodies - Immunosuppressants - Neurologic disorders (eg, seizures, psychosis) |
|
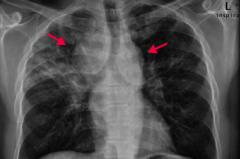
If your patient is a black female with enlarged lymph nodes and bilateral hilar adenopathy or reticular opacities incidentally found on CXR, what diagnosis should you consider? Why?
|
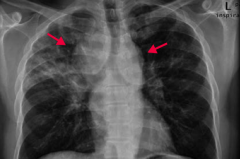
Sarcoidosis
- CXR shows bilateral suprahilar adenopathy (arrows) and right upper lung reticular opacity (often incidental findings on CXR) - Common in black females - Often asymptomatic except for enlarged lymph nodes |
|
|
What is sarcoidosis associated with?
|
- Restrictive lung disease (interstitial fibrosis)
- Erythema nodosum (inflammation of the fat cells under the skin, resulting in tender red nodules or lumps that are usually seen on both shins) - Lupus pernio (chronic raised indurated (hardened) lesion of the skin, often purplish) - Bell palsy - Epithelioid granulomas - Uveitis - Hypercalcemia |
|
|
What are the characteristics of the granulomas in Sarcoidosis?
|
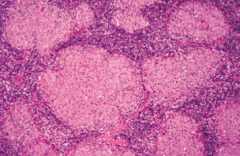
- Non-caseating
- Epithelioid - Contain Schaumann and asteroid bodies |
|
|
What electrolyte abnormality is associated with sarcoidosis? Cause?
|
Hypercalcemia - due to ↑ 1α-hydroxylase-mediated Vitamin D activation in macrophages
|
|
|
How do you treat sarcoidosis?
|
Steroids
|
|
|
What are the characteristics of Sarcoidosis?
|
- Immune-mediated, widespread non-caseating granulomas
- Elevated serum ACE levels - Common in black females - Often asymptomatic except for enlarged lymph nodes - Incidental findings on CXR: bilateral hilar adenopathy and/or reticular opacities |
|
|
What disease can cause present similarly to polymyositis (progressive symmetric proximal muscle weakness) with the addition of malar rash (similar to SLE), Gottron papules (on knuckles), heliotrope (erythematous periorbital) rash, "shawl and face" rash, and/or "mechanic's hands" appearance? What type of inflammation causes this presentation?
|

Dermatomyositis: perimysial inflammation and atrophy with CD4+ T cells
|
|
|
How does Polymyositis compare to Dermatomyositis in terms of location of symptoms?
|

- Polymyositis: symmetric, progressive, proximal muscle weakness, especially in shoulders
- Dermatomyositis: same muscle weakness + malar rash, Gottron papules (knuckles), shawl and face rash |
|
|
What type of inflammation is responsible for Polymyositis and Dermatomyositis?
|
- Polymyositis: endomysial inflammation with CD8+ T cells
- Dermatomyositis: perimysial inflammation and atrophy with CD4+ T cells |
|
|
What lab findings are associated with polymyositis and dermatomyositis?
|
- ↑ CK
- (+) ANA Abs - (+) anti-Jo-1 Abs - (+) anti-SRP Abs - (+) anti-Mi-2 Abs |
|
|
How do you treat a patient with polymyositis or dermatomyositis?
|
Steroids
|
|

What diagnosis should you consider in a patient with puffy and taut skin with an absence of wrinkles? Cause?
|

Scleroderma (systemic sclerosis): excessive fibrosis and collagen deposition throughout the body
|
|
|
Sclerosis can affect what organs?
|
- Skin
- Renal - Pulmonary (most common cause of death) - Cardiovascular - GI |
|
|
Who is more commonly affected by Scleroderma?
|
Females (75%)
|
|
|
What are the two types of Scleroderma (systemic sclerosis)?
|
- Diffuse Scleroderma
- Limited Scleroderma |
|
|
What are the symptoms of diffuse scleroderma? Cause?
|
- Widespread skin involvement, rapid progression
- Early visceral involvement (eg, renal, pulmonary, CV, GI) - Associated with anti-Scl-70 Ab (anti-DNA topoisomerase I antibody) |
|
|
What are the symptoms of limited scleroderma? Cause?
|
- Limited skin involvement confined to fingers and face
- Also with CREST involvement: Calcinosis, Raynaud phenomenon, Esophageal dysmotility, Sclerodactyly, and Telangiectasia - More benign - Associated with anti-Centromere Ab |
|
|
Which antibodies are associated with the two types of Scleroderma?
|
- Diffuse Scleroderma: anti-DNA topoisomerase I antibody
- Limited Scleroderma: anti-Centromere antibody |
|
|
What are the symptoms of CREST involvement? What is it associated with?
|
CREST:
- Calcinosis - Raynaud phenomenon - Esophageal dysmotility - Sclerodactyly - Telangiectasia - Associated with Limited Scleroderma |
|

What type of lesion is this? Characteristics? Other examples?
|

Macule
- Flat lesion with well-circumscribed change in skin color <1 cm - Ex: freckles, labial macule (picture) |
|

What type of lesion is this? Characteristics? Other examples?
|

Patch
- Macule that is >1 cm (flat lesion with well-circumscribed change in skin color) - Ex: large birthmark (congenital nevus) - picture |
|

What type of lesion is this? Characteristics? Other examples?
|

Papule
- Elevated solid skin lesion < 1cm - Ex: mole (nevus) - picture, acne |
|

What type of lesion is this? Characteristics? Other examples?
|

Plaque
- Papule >1 cm (elevated solid skin lesion) - Ex: psoriasis (picture) |
|

What type of lesion is this? Characteristics? Other examples?
|

Vesicle
- Small fluid containing blister <1 cm - Ex: Chickenpox (varicella), Shingles (zoster) |
|

What type of lesion is this? Characteristics? Other examples?
|

Bulla
- Large fluid-containing blister >1cm - Ex: bullous pemphigoid |
|

What type of lesion is this? Characteristics? Other examples?
|

Pustule
- Vesicle containing pus - Ex: pustular psoriasis |
|

What type of lesion is this? Characteristics? Other examples?
|

Wheal
- Transient smooth papule or plaque - Ex: hives (urticaria) |
|

What type of lesion is this? Characteristics? Other examples?
|

Scale
- Flaking off of stratum corneum - Ex: eczema, psoriasis, SCC |
|

What type of lesion is this? Characteristics? Other examples?
|

Crust
- Dry exudate - Ex: impetigo |
|
|
What are the microscopic dermatologic term?
|
- Hyperkeratosis
- Parakeratosis - Spongiosis - Acantholysis - Acanthosis |
|
|
What lesion causes an increased thickness of the stratum corneum? Example?
|
Hyperkeratosis - eg, psoriasis or calluses
|
|
|
What lesion causes hyperkeratosis with retention of nuclei in the stratum corneum? Example?
|
Parakeratosis - eg, psoriasis
|
|
|
What lesion causes an epidermal accumulation of edematous fluid in the intercellular spaces? Example?
|
Spongiosis - eg, eczematous dermatitis
|
|
|
What lesion causes separation of epidermal cells? Example?
|
Acantholysis - eg, pemphigus vulgaris
|
|
|
What lesion causes epidermal hyperplasia (↑ spinosum)? Example?
|
Acanthosis - eg, acanthosis nigricans
|
|
|
What are the characteristics of hyperkeratosis? Examples?
|
Increased thickness of the startum corneum
- Eg, psoriasis and calluses |
|
|
What are the characteristics of parakeratosis? Examples?
|
Hyperkeratosis (↑ thickness of stratum corneum) with retention of nuclei in stratum corneum
- Eg, psoriasis |
|
|
What are the characteristics of spongiosis? Examples?
|
Epidermal accumulation of edematous fluid in intercellular spaces
- Eg, eczematous dermatitis |
|
|
What are the characteristics of acantholysis? Examples?
|
Separation of epidermal cells
- Eg, Pemphigus Vulgaris |
|
|
What are the characteristics of acanthosis? Examples?
|
Epidermal hyperplasia (↑ spinosum)
- Eg, acanthosis nigricans |
|
|
What are the types of pigmented skin disorders?
|
- Albinism
- Melasma (chloasma) - Vitiligo |
|
|
What disorder has a normal melanocyte number with ↓ melanin production? Cause?
|

Albinism
- Due to ↓ tyrosinase activity or defective tyrosine transport - Can also be caused by failure of neural crest cell migration during development |
|
|
What causes Albinism?
|
- Due to ↓ tyrosinase activity or defective tyrosine transport
- Can also be caused by failure of neural crest cell migration during development |
|
|
What is albinism associated with increased risk of?
|
Skin cancer
|
|

What disorder causes hyperpigmentation associated with pregnancy or OCP use?
|

Melasma (Chloasma
|
|

What disorder causes irregular areas of complete depigmentation? Cause?
|

Vitiligo
- Caused by auto-immune destruction of melanocytes |
|
|
What are the common skin disorders?
|
- Verrucae
- Melanocytic nevus - Urticaria - Ephelis - Atopic dermatitis (eczema) - Allergic contact dermatitis - Psoriasis - Seborrheic keratosis |
|

Which common skin disorder causes soft, tan-colored, cauliflower-like papules? Cause?
|

Verrucae / warts - caused by HPV
|
|
|
Which common skin disorder causes epidermal hyperplasia, hyperkeratosis, and koilocytosis?
|
Verrucae / warts
|
|

Which common skin disorder causes condyloma acuminatum on genitals? Cause?
|

Verrucae / warts (caused by HPV)
|
|

What common skin finding is this?
|

Melanocytic Nevus - intradermal nevi are papular
- AKA common mole |
|

What common skin finding is this?
|

Melanocytic Nevus - junctional nevi are flat macules
|
|
|
What can melanocytic nevi lead to?
|
They are benign, but melanoma can arise in congenital or atypical moles
|
|

What common skin finding is this? Cause?
|

Urticaria / hives - pruritic wheals form after mast cell degranulation
|
|
|
How is urticaria characterized?
|

Superficial dermal edema and lymphatic channel dilation, leading to pruritic wheals
|
|

What common skin finding is this? Cause?
|

Ephelis - freckles
- Normal number of melanocytes, with ↑ melanin pigment |
|

What common skin finding is this? Cause?
|

Atopic Dermatitis (Eczema)
- Pruritic eruption, commonly on skin flexures |
|
|
What is the other name for Atopic Dermatitis? What is it associated with?
|
Eczema
- Associated with other atopic diseases: asthma, allergic rhinitis |
|
|
What is the typical location of Atopic Dermatitis (Eczema)?
|

- Usually starts on face in infancy (G)
- Often appears in antecubital fossae thereafter (H) |
|

What common skin finding is this? Cause?
|

Atopic Dermatitis (Eczema)
- Pruritic eruption, commonly on skin flexures |
|

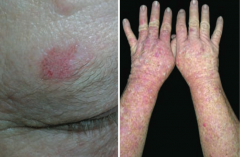
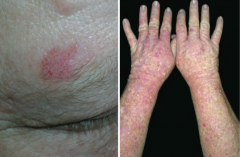
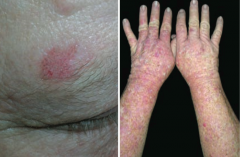
What common skin finding is this? Cause?
|

Allergic Contact Dermatitis
- Type IV hypersensitivity reaction - Follows exposure to allergen - Lesions occur at site of contact (eg, NICKEL) |
|

What common skin finding is this? Cause?
|

Allergic Contact Dermatitis
- Type IV hypersensitivity reaction - Follows exposure to allergen - Lesions occur at site of contact (eg, NEOMYCIN) |
|
|
What are common allergens that cause allergic contact dermatitis? What type of reaction?
|
- Nickel
- Poison Ivy - Neomycin - Causes a type IV hypersensitivity reaction |
|

What common skin finding causes papules and plaques with silver scaling, especially on the knees and elbows?
|

Psoriasis
|
|

What common skin finding is this? What sign is this arrow pointing at?
|

Psoriasis
- Auspitz sign - pinpoint bleeding spots from exposure of dermal papillae when scales are scraped off |
|
|
What are the skin findings in psoriasis?
|
- Papules and plaques with silvery scaling (K), especially on knees and elbows
- Acanthosis (epidermal hyperplasia, ↑ spinosum) with parakeratotic scaling (nuclei still in stratum corneum) - ↑ Stratum spinosum and ↓ stratum granulosum - Auspitz sign: pinpoint bleeding spots from exposure of dermal papillae when scales are scraped off - Can be associated with nail pitting and psoriatic arthritis |
|

What common skin finding appears as a flat, greasy, pigmented squamous epithelial proliferation with keratin-filled cysts and has an appearance of being "stuck on"? Cause? Where do these lesions occur?
|

Seborrheic Keratosis
- Occurs on head, trunk, and extremities |
|

What common skin finding appears as a flat, greasy, pigmented squamous epithelial proliferation with keratin-filled cysts and has an appearance of being "stuck on"? Cause? Where do these lesions occur?
|

Seborrheic Keratosis
- Occurs on head, trunk, and extremities |
|

What common skin finding appears as a flat, greasy, pigmented squamous epithelial proliferation with keratin-filled cysts and has an appearance of being "stuck on"? Cause? Where do these lesions occur?
|

Seborrheic Keratosis
- Occurs on head, trunk, and extremities |
|
|
What is a common benign neoplasm of older persons?
|

Seborrheic Keratosis
|
|

What is the name of the sign for the sudden appearance of multiple seborrheic keratoses? What does this indicate?
|

Leser-Trélat Sign: indicates an underlying malignancy (eg, GI, lymphoid)
|
|
|
What are the types of infectious skin disorders?
|
- Impetigo
- Cellulitis - Necrotizing Fasciitis - Staphylococcal Scalded Skin Syndrome - Hairy Leukoplakia |
|

What skin disorder is characterized by "honey-colored crusting"? Most common causes?
|

Impetigo
- Usually from S. aureus or S. pyogenes |
|
|
What kind of infection is Impetigo? Characteristics?
|

- Very superficial skin infection
- Usually from S. aureus or S. pyogenes - Highly contagious - Honey-colored crusting |
|

What skin disorder is this? Most common causes?
|

Bullous Impetigo - has bullae and is usually caused by S. aureus
|
|

What skin disorder is this? Most common causes?
|

Cellulitis
- Acute, painful, spreading infection of dermis and subcutaneous tissues - Usually from S. pyogenes or S. aureus |
|
|
What often precipitates a Cellulitis infection?
|

Often starts with a break in the skin from trauma or another infection
|
|

What skin disorder causes bullae and a purple color to the skin? Most common causes?
|

Necrotizing Fasciitis
- Deeper tissue injury, usually from anaerobic bacter or S. pyogenes - Flesh eating bacteria |
|

What does Necrotizing Fasciitis lead to?
|

Results in crepitus from methane and CO2 production
|
|

What skin disorder causes fever and generalized erythematous rash with sloughing of the upper layers of the epidermis that heals completely? Cause?
|

Staphylococcal Scalded Skin Syndrome
- Exotoxin destroys the keratinocyte attachments in the stratum GRANULOSUM only |
|
|
What happens if a patient is exposed to a staphylococcal exotoxin that can destroy keratinocyte attachments to the stratum granulosum?
|

Staphylococcal Scalded Skin Syndrome
- Fever - Generalized erythematous rash - Sloughing of layers of epidermis - Heals completely - Seen in newborns and children |
|

What skin disorder causes white, painless plaques on the tongue that cannot be scraped off? Most common cause?
|

Hairy Leukoplakia
- EBV mediated - Occurs in HIV positive patients |
|
|
Who gets Hairy Leukoplakia? Appearance?
|

- Seen in HIV-positive patients with EBV
- Causes a white, painless plaque on the tongue that cannot be scraped off |
|
|
What are the blistering skin disorders?
|
- Pemphigus vulgaris
- Bullous pemphigoid - Dermatitis herpetiformis - Erythema multiforme - Stevens-Johnson Syndrome |
|
|
What skin disorder is caused by IgG antibody against desmoglein (component of desmosomes)?
|
Pemphigus Vulgaris
|
|
|
What skin disorder is caused by IgG antibody against hemidesmosomes?
|
Bullous Pemphigoid (think: antibodies are "BULLOW" the epidermis)
|
|

Which skin disorder causes flaccid intraepidermal bullae and affects the oral mucosa? Cause?
|

Pemphigus Vulgaris
- Auto-immune: IgG antibody against desmoglein (part of desmosomes) - Caused by acantholysis (keratinocytes in stratum spinosum are connected by desmosomes) |
|
|
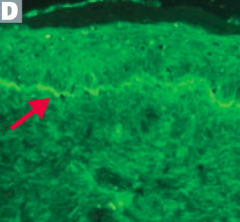
How can you diagnose Pemphigus Vulgaris?
|
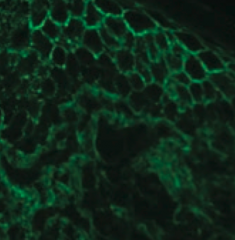
- Immunofluorescence reveals Abs (IgG against Desmoglein) against epidermal cells in a reticular (net-like) pattern
- Nikolsky sign (+) - separation of epidermis upon manual stroking of skin |
|

Which skin disorder causes tense blisters on the skin but spares the oral mucosa? Cause?
|

Bullous Pemphigoid
- Auto-immune: IgG against hemidesmosomes |
|
|
How can you diagnose Bullous Pemphigoid?
|
- Immunofluorescence reveals linear pattern at epidermal-dermal junction
- Tense blisters contain eosinophils - Nikolsky sign (-) = separation of epidermis upon manual stroking of skin |
|

Which skin disorder causes pruritic papules, vesicles, and bullae (often on the elbows)? Cause / associations?
|

Dermatitis Herpetiformis
- Deposits of IgA at the tips of the dermal papillae - Associated with celiac disease |
|
|
Which skin disorder is associated with infections, drugs , cancers, and auto-immune diseases?
|
Erythema Multiforme
|
|
|
What infections can cause Erythema Multiforme?
|

- Mycoplasma pneumoniae
- HSV |
|
|
What drugs can cause Erythema Multiforme?
|
- Sulfa drugs
- β-lactams - Phenytoin |
|
|
What type of lesions are associated with Erythema Multiforme?
|

- Macules
- Papules - Vesicles - Target lesions (look like targets with multiple rings and a dusky center showing epithelial disruption) |
|
|
What skin disorder is characterized by fever, bulla, necrosis, sloughing of skin, and a high mortality rate?
|
Stevens Johnson Syndrome
|
|
|
Are mucus membranes affected in Stevens Johnson Syndrome?
|

Yes - typically at least 2 mucus membranes are involved
|
|
|
In what skin disorders ma you see target lesions?
|
- Erythema Multiforme
- Stevens Johnson Syndrome |
|
|
What is the more severe form of Stevens Johnson Syndrome? How do you distinguish them?
|

Toxic Epidermal Necrolysis
- >30% of the body surface area is affected |
|

Which skin disorder is associated with a hyperpigmented, velvety thickening of the skin? Cause?
|

Acanthosis Nigricans
- Epidermal hyperplasia - Associated with hyperinsulinemia (eg, diabetes, obesity, Cushing syndrome) and visceral malignancies (eg, gastric adenocarcinoma) |
|
|
What skin changes occur in Acanthosis Nigricans?
|

Epidermal hyperplasia causes symmetrical, hyperpigmented, velvety thickening of skin, especially on neck or in axilla
|
|

What premalignant lesion is caused by sun exposure, leading to a small, rough, erythamtous or brownish papule or plaque? What can it progress to?
|
Actinic Keratosis: risk of squamous cell carcinoma is proportional to degree of epithelial dysplasia
|
|
|
What is the appearance of the skin changes in Actinic Keratosis?
|
Small, rough, erythematous or brownish papules or plaques
|
|
|
What is there a risk of if you have Actinic Keratosis? What determines risk?
|
Risk of squamous cell carcinoma is proportional to degree of epithelial dysplasia
|
|

What is the skin disorder characterized by painful inflammatory lesions of the subcutaneous fat, usually on the anterior shins? Possible causes?
|

Erythema Nodosum
- Often idiopathic - Can be associated with sarcoidosis, coccidioidomycosis, histoplasmosis, TB, streptococcal infections, leprosy, and Crohn disease |
|
|
What is the appearance of Erythema Nodosum?
|

Painful, inflammatory lesions of subcutaneous fat, usually on anterior shins
|
|

What can cause Erythema Nodosum?
|
- Often idiopathic
- Can be associated with sarcoidosis, coccidioidomycosis, histoplasmosis, TB, streptococcal infections, leprosy, and Crohn disease |
|
|
Which skin disorder is associated with the 6 P's: pruritic, purple, polygonal planar papules and plaques?
|

Lichen Planus
|
|
|
Which skin disorder manifests as Wickham striae (reticular white lines) on mucosal surfaces? What is it associated with?
|
Lichen Planus
- Associated with Hepatitis C |
|
|
Which skin disorder is associated with a sawtooth infiltrate of lymphocytes at the dermal-epidermal junction?
|
Lichen Planus
|
|
|
What are the features of Lichen Planus?
|

6 P's:
- Pruritic - Purple - Polygonal Planar Papules and Plaques Mucosal involvement manifests as Wickham striae (reticular white lines) Sawtooth infiltrate of lymphocytes at dermal-epidermal junction Associated with Hepatitis C |
|
|
Which skin disorder is known as a "Herald patch" followed days later by a "Christmas tree" distribution of plaques with a collarette scale? How long does this last?
|

Pityriasis Rosea
- Self-resolves in 6-8 weeks |
|

What is this finding? What is it a sign of?
|

Herald Patch - sign of Pityriasis Rosea
|
|

What is this finding? What is it a sign of?
|

Christmas tree distribution - sign of Pityriasis Rosea
|
|
|
What causes a sunburn?
|
Acute cutaneous inflammatory reaction due to excessive UV irradiation
|
|
|
What is the mechanism of damage causing sunburn?
|
Causes DNA mutations, inducing apoptosis of keratinocytes
|
|
|
What are the types of UV rays? How do they differ in the skin changes they cause?
|
- UVA: causes tanning and photoaging
- UVB: causes sunburn |
|
|
What are the potential complications of sunburns?
|
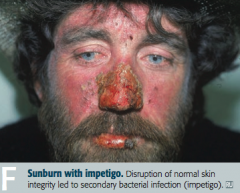
- Impetigo
- Skin cancers: basal cell carcinoma, squamous cell carcinoma, and melanoma |
|
|
What are the types of skin cancers?
|
- Basal cell carcinoma
- Squamous cell carcinoma - Melanoma |
|
|
What is the most common skin cancer?
|
Basal Cell Carcinoma
|
|

What kind of skin lesion is this? Characteristic appearance?
|

Basal Cell Carcinoma
- Pink, pearly nodules - Commonly with telangiectasias, rolled borders, and central crusting or ulceration |
|

What kind of skin lesion is this? Characteristic appearance?
|

Basal Cell Carcinoma
- Non-healing ulcer with infiltrating growth |
|

What kind of skin lesion is this? Characteristic appearance?
|

Basal Cell Carcinoma
- Scaling plaque (superficial BCC) |
|
|
What is the classic histologic appearance of a Basal Cell Carcinoma?
|
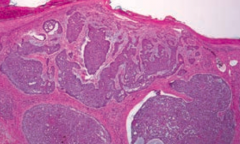
- Palisading nuclei
- Nests of basaloid cells in dermis |
|
|
Where are most Basal Cell Carcinomas located?
|
Found in sun-exposed areas of body
|
|
|
What is the prognosis of Basal Cell Carcinoma?
|
Locally invasive, but almost never metastasizes
|
|
|
How can Basal Cell Carcinomas appear?
|

- Pink pearly nodules, commonly with telangiectasis, rolled borders, and central crusting or ulceration
- Also can appear as non-healing ulcers with infiltrating growth - Scaling plaque (superficial) |
|
|
What is the second most common skin cancer?
|
Squamous Cell Carcinoma
|
|
|
What is Squamous Cell Carcinoma associated with?
|
- Excessive exposure to sunlight
- Immunosuppression - Occasionally arsenic exposure |
|
|
What are the most common locations for Squamous Cell Carcinoma?
|
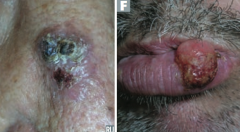
- Face
- Lower lip - Ears - Hands |
|
|
What is the prognosis of Squamous Cell Carcinoma?
|
Locally invasive, but may spread to lymph nodes and will rarely metastasize
|
|
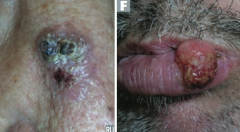
Which type of skin cancer causes ulcerative red lesions with frequent scales, and is associated with chronic draining sinuses?
|
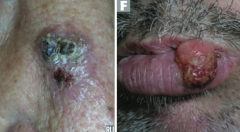
Squamous Cell Carcinoma
|
|
|
What does Squamous Cell Carcinoma look like histologically?
|
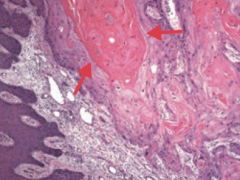
Keratin pearls
|
|
|
What is the name of the scaly plaque, that is a precursor to Squamous Cell Carcinoma?
|
Actinic Keratosis
|
|
|
What is the name of the Squamous Cell Carcinoma variant that grows rapidly and may regress spontaneously? Timeline?
|

Keratoacanthoma: grows rapidly over 4-6 weeks and regresses over months
|
|
|
Which type of skin cancer has a significant risk for metastasis? What determine the risk of this?
|
Melanoma - depth of tumor correlates with risk of metastasis
|
|
|
What tumor marker is there for Melanoma?
|
S-100 tumor marker
|
|
|
What is Melanoma associated with?
|
- Sunlight exposure
- Fair-skinned persons are at ↑ risk |
|
|
What are the key things to look for when evaluating a patient you think may have a Melanoma?
|
ABCDEs:
- Asymmetry - Border irregularity - Color variation - Diameter >6 mm - Evolution over time |
|
|
What are the types of Melanoma?
|

- Superficial spreading melanoma (I)
- Nodular melanoma (J) - Lentigo maligna melanoma (K) - Acrolentiginous melanoma (L) |
|

What skin lesion is this?
|

Superficial Spreading Melanoma
|
|

What skin lesion is this?
|

Nodular Melanoma
|
|

What skin lesion is this?
|

Lentigo Maligna Melanoma
|
|

What skin lesion is this?
|

Acrolentiginous Melanoma
|
|
|
What genetic abnormality often drives melanoma?
|
BRAF kinase activating mutation (V600E)
|
|
|
How do you treat Melanoma?
|
- Primary treatment: excision with appropriately wide margins
- Metastatic or unresectable melanoma in patients with BRAF V600E mutation may benefit from Vemurafenib, a BRAF kinase inhibitor |