Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
772 Cards in this Set
- Front
- Back
|
A 24yo complains of a stuffy nose in the aftermath of a viral cold of 5 days duration. he has taken a nasal spray for self- treatment for the past 3 days and has noted that the stuffiness has become bilateral and now interferes with his sleep. Tx? (3 together)
|
1. Discontinue the present spray
2. use Inhaled Glucocorticoids briefly 3. Humidification (the Sx are due to "Rhinitis Medicamentosa": rebound bogginess caused by local tissue refractory effects due to a topical decongestant; produces opposite effect of the medication) |
|
|
Q002. A 15yo patient has recurrent nose bleeds on the left side. Dx?; Tx?
|
A002. Dx: Anterior Epistaxis; Tx: cauterize with Silver Nitrate
|
|
|
Q003. what virus has the greatest possibility to lead to Otitis Media?
|
virus → RSV
the most common bacterial pathogens found in AOM are Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis. |
|
|
Q004. You have a new 52yo male patient without any recent medical records. What are the (2) main tests to screen for CV disease?; (2) for cancer?; (2) immunizations?
|
A004. CV:; 1. Blood Pressure (every visit);; 2. Lipid Profile Cancer:; 1. Fecal Occult Blood;; 2. Prostate exam Immunizations:; 1. Tetanus (if not had in 10 years);; 2. Influenza vaccine (in fall months)
|
|
|
Q005. when should a patient be screened for an abdominal aortic anneurism?; what test?
|
A005. at age 65 or over; by an Ultrasound
|
|
|
Q006. If there is no History of a Td (tetnus and diphtheria), what is the dosage schedule?
|
A006. 2 injections of vaccine at least 4 weeks apart;; followed by a third 6-12 months later;; normal boosters every 10 years
|
|
|
Q007. what is the schedule for the pneumococcal vaccine?
|
A007. at age 65 unless the patient has a chronic disease. with chronic disease, give vaccination then a one-time revaccination 5 years later
|
|
|
Q008. Tx for acute exacerbation of COPD with coughing green and without fever?; (3 together)
|

A008. 1. Antibiotics; 2. Bronchodilators; 3. Corticosteroids
|
|
|
Q009. what are the PFT levels for Stage I of COPD?; Name (2) med Tx and classes
|

Stage I: FEV1/FVC < 70%; FEV1 > 80%
Tx: Short-acting inhaled Bronchodilators; 1. Beta2 agonist: Albuterol or 2. Anticholinergic: Ipratropium |
|
|
Q010. what are the PFT levels for Stage II of COPD?; Name (2) additional med Tx and classes
|

Stage II: FEV1/FVC < 70%; FEV1 50 - 80%
Tx: ADD a Long-acting inhaled Bronchodilator; 1. Beta2-agonist: Salmeterol or; 2. Anticholinergic: Tiotropium; (still use short-acting PRN) |
|
|
Q011. what are the PFT levels for Stage III of COPD?; Name additional med Tx
|

Stage III: FEV1/FVC < 70%; FEV1 30 - 50%
Tx: Add inhaled steroids |
|
|
what are the PFT levels for Stage IV of COPD?
Name additional Tx for this stage |

Stage IV: FEV1/FVC < 70%; FEV1 < 30%;
Tx: add oxygen therapy |
|
|
Q013. A 45yo man presents with a sudden onset of monoarticular, nontraumatic join pain. He is an alcoholic and takes HCTZ for his HTN. Dx?; Tx for acute attacks? (2 possible); Maintenance therapy? (3 possible)
|
Dx: Gout
Acute attacks: 1. Colchicine; 2. NSAIDs (not aspirin) Maintenance: 1. Alkalinization of urine; 2. Probenicid; 3. Allopurinol |
|
|
Q014. Chronic inflammation (as in RA) predisposes the joint to infection by what organism?; In active young adults?; what (2) tests should be done with both?
|
Chronic: Staph Aureus
Young adults: N. Gonorrhea Tests: 1. Joint culture 2. Blood culture (also urethral swab if positive for gonorrhea) |
|
Q015. A child has a few painful, swollen joints with prolonged morning stiffness. He also has uveitis and a negative rheumatoid factor. Dx?
|
A015. Juvenile RA; (rheumatoid factor is often negative in children. Key is the Uveitis)
|
|
|
Dx: Joint pain with "pannus"; Unique joint affected?; Tx for symptomatic relief?; Tx for bad flare-ups?; other meds used and class? (4)
|
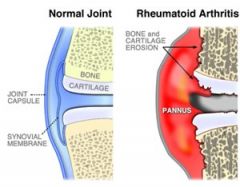
Rheumatoid Arthritis (MCP effected)
Symptomatic Tx: NSAIDs Bad flare: Corticosteroids Other meds: 1. DMARDS (Methotrexate, Sulfsalazine) 2. Anti-cytokines (Infliximab, Etanercept) |
|
|
Q017. Main Sx of a septic joint that distinguishes it
|
A017. Limited ROM
|
|
|
Q018. what are (3) bugs seen in a HIV patient joint?
|
A018. 1. Pneumococcal; 2. Salmonella; 3. H. Influenza
|
|
|
Q019. What valvular repair surgery is assoc with highest mortality?
|
A019. Mitral Valve replacement
|
|
|
Q020. on exam a 59yo woman has a new low-pitched, rumbling, diastolic murmur that is heard loudest at the apex. Dx?
|
A020. Rheumatic Heart Disease
|
|
|
Q021. MC complication of Mitral Stenosis
|
A021. Systemic Embolization; (LA is rgeatly enlarged with MS causing A-fib and leading to a 80% increase in systemic emboli)
|
|
|
Q022. MC complication of Aortic Stenosis
|
A022. Syncope
|
|
|
Q023. How do you differentiate a Paroxysmal Atrial Tachycardia from an AV nodal Reentry Tachycardia?
|
A023. Carotid massage; (no effect on PAT, but can convert AVNRT)
|
|

what is the physiologic first goal of treatment of an acute A-fib?
|

Reduce Ventricular response (rate control)
(reduce rate with Digoxin, Beta-blocker or Ca channel blocker) |
|

What is the rule for anticoagulation therapy for A-fib?
|
Should be Anticoagulated (Warfarin) if rate continued for > 2 days
|
|
|
what does the pattern of a QS in leads II, III and AVF indicate?
|
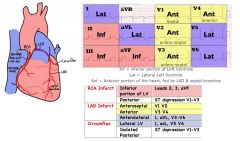
Previous Inferior MI
|
|
|
Crescendo-decrescendo murmur that decreases with squatting
|

Hypertrophic Cardiomyopathy; (IHSS)
|
|
|
What does Insipration and squatting do to blood?
|

Increases venous return
|
|
|
Q029. What does Expiration and standing do to blood?
|
A029. Decreases Venous return
|
|
|
Q030. what murmur is increased with squatting?
|
A030. Mitral regurg
|
|
|
MCC of peripheral emboli?; 2nd MCC?
|
1. A-fib
2. MI |
|
|
Q032. MCC of an Ascending Aortic Aneurysm
|
A032. Cystic Medial Necrosis; (or syphillis)
|
|
|
Q033. MCC of a Descending Aortic Aneurysm
|
A033. Atherosclerosis
|
|
|
Medication for mild Claudication that increases RBC flexibility
|
Pentoxifylline (Pentoxil/Pentopak/Trental)
MOA: reduces blood viscosity & improves RBC flexibility, microcirculatory flow & tissue oxygen concentrations. improvement in RBC flexibility appears to be due to inhibition of phosphodiesterase & a result increase in cAMP in RBCs |
|
|
Q035. What are the (3) main risk factors for the rupture of an AAA?
|
A035. 1. HTN; 2. Large Diameter of AAA; 3. COPD
|
|
|
Q036. what symptom must be present when diagnosing Otitis Media?
|
A036. Conductive hearing loss in affected ear
|
|
|
What is the defining characteristic of Malignant Otitis Externa?
|
Osteomyelitis of the bony canal
Skull base osteomyelitis, also known as malignant otitis externa or necrotizing otitis externa (NOE), is a bacterial infection of the EAC and skull base. This disease process is most frequently seen in elderly diabetics and immunocompromised patients. It most commonly begins as an external otitis that progresses to involve the temporal bone, and may progress to fatal meningitis, sepsis, and death if unrecognized or untreated. Treatment: Long-term parenteral antibiotics are the treatment of choice. Aminoglycosides (eg, tobramycin) and antipseudomonal -lactam antibiotics, including piperacillin, ticarcillin, or ceftazidime, may be used. Some physicians recommend the use of outpatient fluoroquinolones such as ciprofloxacin or ofloxacin; however, this is appropriate only for patients with early presentations who can be followed up closely. Control of hyperglycemia and immunosuppression is necessary to maximize treatment. Surgical debridement may be necessary to remove necrotic tissue. |
|
|
Q038. Dx:; Conductive hearing loss in patient with an otherwise normal exam
|
A038. Otosclerosis
|
|
|
(2) Sx that differentiate Mononucleosis from Strep Pharyngitis
|
Mono:
1. Non-Tender Lymph nodes 2. No Fever |
|
|
Q040. What is the children's mean age at the eruption of the last if the deciduous teeth?
|
A040. 27 months; (starts at about 7 months)
|
|
|
Q041. MC bug of oral cellulitis
|
A041. Beta-hemolytic Strep Pyogenes
|
|
|
Q042. Dx:; Abrupt and severe HA in Occipital area and Upper Neck; HTN; confusion; No cervical spine tenderness
|
A042. Subarachnoid aneurysm; (note lack of cervical tenderness)
|
|
|
Q043. 60yo man has 1 week History of mild HA accompanied by pain in his jaw with chewing. He denies any visual change, BP is normal, take no meds, exam is otherwise normal; Dx?; Next step?
|
A043. Dx: Temporal Arteritis (does not always present with eye problem; jaw pain is more common); Next step: Sedimentation Rate
|
|
|
Q044. MC presenting Sx of Intracerebral AV malformation
|
A044. Intracranial Hemorrhage; (more then HA, seizure, etc)
|
|
|
What is eye problem is most often assoc with crossed-eyes (Esotropia)?
|
Hyperopia; (farsightedness)
|
|
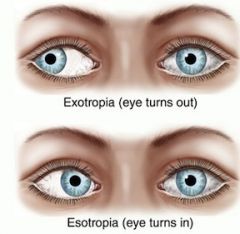
Q046. What eye problem is most often assoc with lateral gaze or "cock-eyed" (Exotropia)?
|
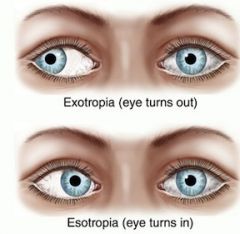
A046. Myopia; (nearsightedness)
|
|
|
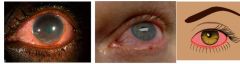
With respect to "red eye" a speedy diagnosis is urgent because of the possibility of what eye problem?
What is a specific finding for this problem? |
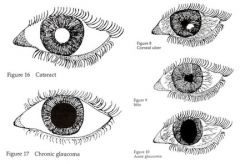
Acute-angle Glaucoma
sign: Ipsilateral Dilated Pupil |
|
|
patient presents with a red eye, ipsilateral miotic pupil and photophobia
What's the likely dx? |
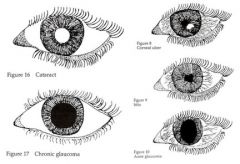
Iritis
|
|
|
Q049. A 45yo obese mother of 5 children complains of HA. Her bp is normal and fundoscopy reveals papilledema. A lumbar tap shows an Increased CSF pressure, but otherwise normal. A CT comes back normal. Dx?
|
A049. Pseudotumor Cerebri; (assoc with use of Vitamin A, oral contraceptives, and tetracycline)
|
|
|
MC type of ankle sprain?; MC ligament injured?
|
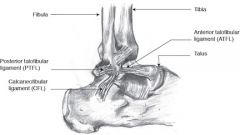
Sprain: Inversion of ankle that is Plantar Flexed
Ligament injured: Anterior Talofibular ligament |
|
|
What are the Ottawa Ankle Rules used to rule out?
What are the (2) main rules? |
Ottawa Ankle Rules used to rule out:
1. Malleolar fracture 2. Mid-foot fracture note: use these rules to determine whether patient needs an ankle xray Rules: 1. Unable to bear weight immediately or during the exam 2. Bony tenderness over the distal Medial or Lateral Malleolus |
|
|
Difference b/t Sprain and Strain?
|
Sprain: Ligament stretch/tear
STrain: TENDON stretch/tear |
|
|
Q053. what is the MCC of stiff or painful joint following a sprain?
|
A053. Inadequate rehabilitation
|
|
|
Describe the "Empty Can test"; What does it test?
|
Empty can test → arm abducted, elbows extended, thumbs pointing down, patient elevates arm against resistance
tests: Supraspinatus (for rotator cuff injury) |
|
|
Q055. Describe the "Lift-off Test"; What does it test?
|
A055. LOT: patient places dorsum of hand on lumbar back and attempts to lift hand off of back; tests: Subscapularis (rotator cuff injury)
|
|
|
Q056. Definition:; 1. A small blister <0.5cm; 2. A blister >0.5cm
|
A056. 1. Vesicle; 2. Bulla (pleural: bullae)
|
|
|
Q057. Definition:; a discoloration of the skin that is neither raised nor depressed
|
A057. Macule
|
|
|
Q058. MC type of Melanoma
|
A058. Superficial Spreading Melanoma
|
|
|
Q059. MC type of Melanoma in elderly
|
A059. Lentigo Maligna; (although least common of the four types)
|
|
|
Q060. MC type of Melanoma in African Americans and Asians
|
A060. Acral Lentiginous Melanoma
|
|
|
Q061. Most aggressive type of Melanoma
|
A061. Nodular Melanoma
|
|
|
A 25yo woman complains of vaginal itching and burning. The pH of the vaginal discharge is 4. Dx?
|
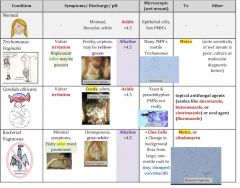
Candida; (Trich, BV and Candida cause 90% of all vaginal Sx; both Trich and BV have a pH > 4.5)
|
|
|
Q063. A previously healthy 26yo man presents with abdominal cramping and fever for 2 days. He has 10 stools in last 24 hours. The specimen has blood and WBC. Dx?
|
A063. Shigellosis; (inflammatory process...food poisoning does not have WBC)
|
|
|
Q064. A 30yo obese woman presents with RUQ pain, slight fever, myalgias, fatigue and anorexia for 2 weeks that has increasingly become worse. Now she also has N/V and she is mildly jaundiced. LFTs show inc AST/ALT and total and conjugated billirubin and blood shows a mild elevation of WBC. Dx?; Initial step? (2 together)
|
A064. Hepatitis initial step:; 1. Continue oral fluids and bed rest; 2. order Hepatitis profile to determine type
|
|
|
Q065. a 76yo patient has a Hb of 7 and dec MCV, inc TIBC and dec Ferritin. Cause of Anemia?
|
A065. Iron Deficiency Anemia; (usually bowel-related bleed at that age)
|
|
|
Q066. What is the first line of therapy for Acne patients?; What is reserved for severe Acne?
|
A066. first: Tretinoin (Retin-A); severe: Isotretinoin (Accutane)
|
|
|
Q067. Which MCV anemia causes neurological Sx?; What Dx is it most commonly assoc with?
|
A067. B-12 deficiency; MC assoc with: Pernicious Anemia
|
|
|
Q068. How can you tell the difference b/t bleeding from colon cancer vs bleeding from diverticulosis by CBC?
|
A068. Colon CA: Microcytic, Hypochromic anemia; Diverticulosis: RBC indices are normal (both have decreased Hb)
|
|
|
Q069. First Dx test for possible Diverticulitis?
|
A069. CT Scan; (colonoscopy and barium enema could possibly cause perforation)
|
|
|
Q070. What is the first Tx for recurrent Otitis Media?
|
A070. Antibiotics for the acute otitis and then prophylactic Abx for 6 months; (tube placement for those who fail this suppressive therapy)
|
|
|
Q071. After a patient is treated for H. pylori and is asymptomatic, what is the next step?
|
A071. Endoscopy (EGD); (to confirm that the ulcer did not represent a gastric CA)
|
|
|
Q072. A 23yo woman complains of the room spinning and on exam has vertical nystagmus unaffected by position. What should she be tested for?
|
A072. test for: Multiple Sclerosis; (with MRI of the brain)
|
|
|
Q073. If there is a patient undergoing a vascular surgery, what pre- surgical test besides a CBC, CMP and x-ray should be performed?
|
A073. Cardiac Stress Test; (vascular surgery is a high risk for cocomitant CAD)
|
|
|
Q074. when should a child be screened for high cholesterol?; (2)
|
A074. At Age 2 if there is a family History of CV disease in parent/grandparent at age < 55 or; parental History of hypercholesterolemia
|
|
|
Q075. what other virus is most like the Sx of mononucleosis?
|
A075. CMV
|
|
|
Q076. A 10yo with asthma begins to wake from sleep about once a week. He is currently taking albuterol. what meds should he now take given the new Sx?
|
A076. 1. Long-Acting Beta-Agonist; 2. Inhaled Steroid
|
|
|
Q077. a 45yo has come into the office for the second time with HTN. Aside from the bloodwork, what (2) lab tests should be performed on this visit?
|
A077. 1. ECG; 2. CXR
|
|
|
Q078. *92 y/o with inc RBC count, inc platelet, most likely CLL; What is the next step?
|
A078. Observation
|
|
|
Q079. *pt with inc WBC count and inc RBC; what is the mechanism for erythrocytosis?
|
A079. abnormal Stem Cell Proliferation
|
|
|
Q080. *pt with lung cancer has hyponatremia with dec osmolarity; Next step?
|
A080. Water restriction
|
|
|
Q081. *Dx:; Asymptomatic 18 y/o with symmetric t-wave inversion on v1-v3
|
A081. Juvenile pattern of T-wave inversion
|
|
|
Q082. *Pt with tender 2 month duration nodule in RUQ; US shows cysytic mass. Next step?
|
A082. Aspiration of cyst
|
|
|
Q083. *Pt with chronic alcoholic abuse present with positive Romberg test (eyes open good balance, eyes closed loses balance). Next step?
|
A083. Check B-12 level
|
|
|
Q084. *Pt with non-blanching purpura on buttocks and legs. If you were to biopsy, what would you see?
|
A084. IgA
|
|
|
Q085. *Pt with irregularly irregular heart rate >24 hours; Next step? (2)
|
A085. 1. Rate control (beta-blocker or Calcium blocker); 2. Anticoagulate with Warfarin for 3 weeks before electrical Cardioversion (less then 24 hours can cardiovert electrically or with IV Procainamide)
|
|
|
Q086. *MC type of kidney stone?
|
A086. Calcium Oxalate
|
|
|
Q087. *Pt with sickle cell anemia(normocytic). what do you give as a supplement?
|
A087. Folate supplements
|
|
|
Q088. *What is the mechanism of damage behind ototoxicity from Aminoglycosides?
|
A088. Inner ear damage (to vestibular and cochlear apparatus)
|
|
|
Q089. *Pt with upper neuron CN 7 damage (forehead is OK but left face is drooping) and pt has dizziness, loss of balance, rhinitis. Dx?
|
A089. Acoustic Neuroma
|
|
|
Q090. *Pt with FH of stroke at age 55, BP 160/102, LDL 140 (overall ratio is OK), sedentary, obese. What is the most probable cause of a stroke?
|
A090. Hypertension
|
|
|
Q091. (2) Possible Tx for Barrett's esophagus
|
A091. 1. Esophagectomy; 2. Photodynamic therapy
|
|
|
Q092. *Pt with accentuated S2, bilateral edema, normal ejection fraction. What is the cause?
|
A092. Primary Pulmonary HTN
|
|
|
Q093. Pt with cirrhosis, non-bleedning varices, and other findings. Which med is the best for long term use?
|
A093. Propranolol (for varices)
|
|
|
Q094. First test to order when suspecting PCOS?
|
A094. US of the pelvis
|
|
|
Q095. *Pt with headache, low grade fever, joint pain and muscle pain. What is the next step?
|
A095. ESR (to rule-out Temporal Arteritis)
|
|
|
Q096. *Pt went to woods, rash with center clearing and joint pain. Drug Tx? (2 possible)
|
A096. 1. Doxycycline; 2. Amoxicillin (Penicillin or Cephalosporins if cardiac or neural involvement)
|
|
|
Q097. Dx:; Patient has joint pain in various joints without any positive lab results
|
A097. Degenerative Joint Disease (otherwise known as OA)
|
|
|
Q098. What can be used in both adults and children for up to 8 weeks as daily prophylaxis during an Influenza outbreak?
|
A098. Amantidine
|
|
|
Q099. Treatment for a 10 cm enlarging hematoma adjacent to the episiotomy site in a baby who you delivered 6 hours ago
|
A099. removal of the sutures and clots, and ligating the bleeding sites
|
|
|
Q100. Common cause of Retinal Detachment
|
A100. Posterior detachment of the Vitreous; Vitreous detachment is very common after age 60 and occurs frequently in younger persons with myopia. The separation of the posterior aspect of the vitreous from the retina exerts traction on the retina, with the attendant risks of a retinal tear and detachment. Symptoms of retinal detachment may include light flashes(photopsia), a sudden appearance or increase in “floaters,” or peripheral visual field loss, any of whichshould prompt an ophthalmology referral. Cataract surgery can result in premature shrinkage of the vitreous and thereby poses an increased risk, but vitreous detachment resulting from other processes is more common. Hyphema, glaucoma, and diabetic retinopathy are not specific risk factors for retinal detachment.
|
|
|
Q101. Treatment of choice for a 4 year old with suspected Pertussis?
|
A101. Erythromycin, Azithromycin, or Clarithromycin
|
|
|
Q102. What vitamin has been shown to reduce the risk of falling in the elderly?
|
A102. Vitamin D
|
|
|
Q103. What is an effective treatment for Bulimia nervosa?
|
A103. Fluoxetine; A number of placebo-controlled, double-blind trials have demonstrated the effectiveness of a variety of antidepressants in the treatment of bulimia nervosa. Fluoxetine has FDA approval for this indication. The other agents are not used for treating bulimia.
|
|
|
Q104. The Health Insurance Portability and Accountability Act (HIPAA); A)sets a federal minimum on the protection of privacy; B)requires that privacy notices be acknowledged and signed at eachofficevisit; C)allows the patient to inspect and obtain a copy of his/her record without exception; D)requires privacy notices prior to giving emergency care
|
A104. ANSWER: A; HIPAA regulations set a minimum standard for privacy protection. Privacy notices must be provided at the first delivery of health services, and written acknowledgement is encouraged but not required. Exceptions to patient inspections include psychotherapy notes and instances where disclosure is likely to cause substantial harm to the patient or another individual in the judgment of a licensed health professional. Although it is not necessary to provide patients with a privacy notice at the time of rendering emergency care, it is required that patients be provided with a privacy notice after the emergency has ended.
|
|
|
Q105. What is the most common cause of visual loss in children?
|
A105. Amblyopia = Amblyopia refers to diminished vision in either one or both eyes, for which no cause can be discovered upon examination of the eye. ★ - Amblyopia is the medical term used when the vision in one of the eyes is reduced because the eye and the brain are not working together properly. ★ - The eye itself looks normal, but it is not being used normally because the brain is favoring the other eye. ★ - This condition is also sometimes called lazy eye ★ - Evaluation of visual symptoms in children canbe challenging, but is important for identifying correctableconditions.Amblyopia, or“lazy eye,”is the most common cause of visual loss, with a prevalence of 2% inchildhood. ★ - It isoftenrelated to strabismus, in which the image from one eye is suppressed in order toeliminate diplopia. ★ - Iritis is unusual and may have minimal symptoms; it isfrequently associated withjuvenile rheumatoid arthritis. ★ - Glaucoma does occur in children, oftenaftercataract surgery. ★ - Eye trauma isrelatively common, especially in boys. ★ - They may sustain abrasions, foreign bodiesandpenetrating injuries. ★- Conjunctivitis will usually resolv
|
|
|
Q106. What tumor marker is used to detect the recurrence of colon cancer?
|
A106. CEA; Carcinoembryonic antigen (CEA) is a marker for colon, esophageal, and hepatic cancers. It is expressed innormal mucosal cells and is overexpressed in adenocarcinoma, especially colon cancer. Though not specific for colon cancer, levels above 10 ng/mL are rarely due to benign disease. CEA levels typically return tonormal within 4–6 weeks after successful surgical resection. CEA elevation occurs in nearly half of patientswith a normal preoperative CEA level that have cancer recurrence.
|
|
|
Q107. Tumor marker for Ovarian Cancer?
|
A107. CA-125
|
|
|
Q108. What levels are elevated in PCOS?
|
A108. Testosterone; LH and FSH (usually 3:1); This patient presented with classic symptoms of polycystic ovary syndrome (PCOS)—oligomenorrhea, infertility, hirsutism, and acne—reflecting hyperandrogenic anovulation. The underlying pathophysiology of PCOS includes insulin resistance leading to increased ovarian androgen production. LH and FSH levels are often elevated in PCOS, with the LH:FSH ratio often being greater than 3:1. Prolactin is usually normal, although mild elevations are possible.
|
|
|
Q109. What is the most effective drug used for the treatment of Alcohol dependence?
|
A109. Naltrexone (ReVia); * opioid receptor antagonist
|
|
|
Q110. What method most reliably detects a ureteral stone?
|
A110. Helical CT scan of the abdomen and pelvis without contrast; An unenhanced helical CT scanof the abdomen and pelvis is the best study for confirming the diagnosis of a urinary tract stone in a patient with acute flank pain, supplanting the former gold standard, intravenous pyelography. A CT scan may also reveal other pathology, such as appendicitis, diverticulitis, or abdominalaortic aneurysm. Although abdominal ultrasonography has a very high specificity, it is still not better than CT, and its sensitivity is much lower; thus, its use is usually confined to pregnant patients with a suspected stone. Plain abdominal radiographs may show the stone if it is radiopaque, and are useful for following patients with radiopaque stones. CT will reveal a radiopaque stone. While most patients with stones will have hematuria, its absence does not rule out a stone.
|
|
|
Q111. What method has been shown to prolong survival in cases of COPD?
|
A111. oxygen therapy
|
|
|
Q112. Radiologic evaluation of the cervical spine shows an air- fluid level in the Sphenoid sinus. What facial fracture would this be consistent with?
|
A112. Basilar Skull Fracture
|
|
|
Q113. Facial fracture associated with double vision, fluid in the Maxillary sinus, an air-fluid level in the maxillary sinus, and diplopia?
|
A113. Orbital floor fractures
|
|
|
Q114. Facial fractures more visible in Towne's view and have characteristic swelling and lateral orbital bruising
|
A114. Zygomatic arch fractures
|
|
|
Q115. Facial fractures associated with dental misalignment or bleeding
|
A115. Mandible fractures
|
|
|
Q116. Which vitamin reverses the effect of Warfarin?
|
A116. Vitamin K
|
|
|
Q117. What class of antihypertensives may help preserve bone mineral density?
|
A117. HCTZ
|
|
|
Q118. What drug would be used for first-line treatment of OCD with a depressive episode?
|
A118. Fluoxetine or other SSRI's; Escitalopram; Sertraline (Zoloft); Paroxetine (Paxil); Clonazepam would be 2nd line
|
|
|
Q119. Pain during rest and exercise and the presence of swelling and soreness behind the knee and in the calf is found in those with?
|
A119. Baker's cysts
|
|
|
Q120. What finding would support the diagnostic impression of peripheral vascular disease?
|
A120. Treadmill arterial flow studies showing a 20-mm HG decrease in ankle systolic blood pressure immediately following exercise
|
|
|
Q121. Read question 31 on Exam Book 1
|
A121. -
|
|
|
Q122. What medications are most effective for Restless Leg Syndrome?
|
A122. Carbidopa/Levodopa (Sinemet); or Ropinirole (Requip)or Pramipexole (Mirapex); Dopamine agonists used in Parkinson's disease
|
|
|
Q123. What are the key factors in the diagnosis of Streptococcal pharyngitis?
|
A123. 1. fever > 100.4; 2. Tonsillar exudates; 3. Anterior Cervical LAD; 4. absence of cough
|
|
|
Q124. Imiquimod (Aldara) is approved by the FDA for the treatment of what?
|
A124. External genital and perianal warts in pts 12 year and over; BUT it is also used off-label for plantar warts, flat warts, periungual warts, and mollucsum contagiosum
|
|
|
Q125. What is used prophylactically after total knee or hip replacements to prevent DVT's?
|
A125. LMW-heparin (Enoxaparin 30 mg subQ q 12h) and adjusted dose Warfarin; *these can be augmented by intermittent pneumatic compression
|
|
|
Q126. What is Black Cohosh?
|
A126. Herbal preparation widely used in the treatment of Menopausal symptoms and menstrual dysfunction
|
|
|
Q127. What medication class is the most appropriate for treating patients with Post-traumatic stress disorder?
|
A127. SSRI's due to low side-effect profile; Sertraline, Escitalopram, Paroxetine
|
|
|
Q128. What drug class is contraindicated in the treatment of patients with cocaine-arrhythmias? Why?
|
A128. Beta-blockers (Metoprolol); b/c they have been shown to exacerbate coronary vasospasm
|
|
|
Q129. A 3 yo female is brought to your office for evaluation of mild intoeing. The child's patellae face forward, and her feet point slightly inward. What is the most appropriate thing to do? What is the cause of this?
|
A129. Reassurance; Internal Tibial Torsion is believed to be caused by sleeping in the prone position, and sitting on the feet. In 90% of cases, the condition gradually resolves without intervention by the age of 8.
|
|
|
Q130. When is it recommended to screen women for Gestational Diabetes?
|
A130. 24-28 WGA; *pt is given 50-g oral glucose load followed by glucose determination 1 hour later
|
|
|
Q131. What co-morbidity is Sleep Apnea associated with? By improving sleep apnea this condition may also be improved.
|
A131. Hypertension
|
|
|
Q132. What medication can provide rapid relief of the symptoms of a patient in severe panic disorder?
|
A132. Alprazolam (Xanax) - works in hours
|
|
|
Q133. After how many weeks is a pregnancy termed "post-date or post-term"? What is the signifigance?
|
A133. 42 weeks; b/c perinatal mortality doubles at 42 WGA
|
|
|
Q134. A 36 yo member of the National Guard who has just returned from Iraq consults you b/c of several "boils" on the back of his neck that have failed to heal over the last 6 months, despite 2 week-long courses of cephalexin. you observe 3 1-to-2-cm raised minimally tender lesions with central ulceration and crust formation. He denies any fever or systemic symptoms. What is the most likely cause?
|
A134. Leishmaniasis
|
|
|
Q135. What is the earliest presenting symptoms in most older patients with open-angle glaucoma?
|
A135. Tunnel vision = gradual loss of peripheral vision
|
|
|
Q136. DOC's for Premenstrual Dysphoric Disorder
|
A136. SSRI's; Fluoxetine, Sertraline
|
|
|
Q137. Why should patients with CHF avoid taking NSAID's?
|
A137. b/c they cause Sodium and water retention, as well as increase systemic vascular resistance which may lead to cardiac decompensation
|
|
|
Q138. A pregnant patient is positive for Hepatitis B surface antigen. What is the most appropriate therapy for the infant?
|
A138. Hepatitis B immune globulin (HBIG) and Hepatitis B vaccine at birth; Testing for seroconversion is recommended at 9-12 months of age
|
|
|
Q139. What is the amount of RhoGam administered to an Rh negative mother if she has an ectopic pregnancy/spontaneous/therapeutic abortion at less than 12 WGA? > 12 WGA?
|
A139. < 12 WGA = 50 g RhoGAM; > 12 WGA = 300 g
|
|
|
Q140. What is the leading cause of death among women?
|
A140. Cardiovascular disease
|
|
|
Q141. Describe "postpartum blues"
|
A141. affect up to 85% of women and typically resolve by the 10th day postpartum
|
|
|
Q142. Describe Postpartum Depression
|
A142. may not occur until 6 months following delivery (as opposed to postpartum blues, which resolves by 10 days postpartum); Can be treated with SSRI's
|
|
|
Q143. Describe GER in infants; is it normal?; is it harmful?
|
A143. It is common & self-limited and represents a physiologic process of "spitting up"; Occurs in the absence of poor weight gain, irritability, cough, pain, or anemia...majority are thriving; Usually resolves by 1 year of age
|
|
|
Q144. What is the most frequent etiologic agent of occult bacteremia in children?
|
A144. S. pneumo
|
|
|
Q145. What is the cause of Kaposi's Sarcoma?
|
A145. HHV-8
|
|
|
Q146. How long is the Nuvaring kept in place before removing it?
|
A146. 3 weeks and then removed for 1 wk so that withdrawal bleeding occurs; new ring is then inserted; If for some reason the ring is out of the vagina for more than 3 hours, back-up contraception should be used until the device has been in place for 7 days
|
|
|
Q147. What is the prophylactic treatment for an outbreak of Menigococcal disease in a day care center?
|
A147. Rifampin
|
|
|
Q148. What is the most common cause of chronic, unilateral nasal obstruction in adults?
|
A148. Nasal septal deviation
|
|
|
Q149. What is the most common cause of nasal obstruction in all age groups?
|
A149. Common cold; usually bilateral and intermittent
|
|
|
Q150. What is the most common tumor or growth to cause nasal obstruction?
|
A150. Adenoidal hypertrophy followed by nasal polyps
|
|
|
Q151. List the 4 diagnostic criteria for Delerium
|
A151. 1. disturbances of consciousness with reduced ability to focus, sustain, or shift awareness; 2. A change in cognition (memory, disorientation, language disturbance) or development of a perceptual disturbance that is not better accounted for by a preexisting, established, or evolving dementia; 3. Development over a short period of time with a tendency to fluctuate during the course of a day; 4. Evidence from the history, PE, or lab findings that indicated the disturbance is caused by direct physiologic consequences of a general medical condition
|
|
|
Q152. What treatment is recommended for intravaginal genital warts in pregnant women?
|
A152. Cryotherapy with liquid nitrogen
|
|
|
Q153. A 25-year-old white truck driver complains of 1 day of throbbing rectal pain. Your examination shows a large, thrombosed external hemorrhoid. What is your treatment?
|
A153. Elliptical excision of the thrombosed hemorrhoid
|
|
|
Q154. How long should a pharmacologic treatment of depression last?
|
A154. minimum of 6 months
|
|
|
Q155. What is the best definition of Specificity?
|
A155. true-negative rate, or how well the test correctly identifies patients without disease
|
|
|
Q156. What is the best definition of Sensitivity?
|
A156. True-positive rate, or how well the test correctly identifies patients with disease
|
|
|
Q157. What is most bleeding in Meckel's diverticulum secondary to?
|
A157. heterotrophic gastric mucosa causing acid-induced ileal ulceration
|
|
|
Q158. What is the most common cause of proteinuria in children? Describe...
|
A158. Orthostatic Proteinuria
|
|
|
Q159. What is the most appropriate treatment for asymptomatic chlamydial infection during the 2nd trimester of pregnancy?
|
A159. Azithromycin
|
|
|
Q160. What is the general notion regarding the use of automated external defibrillators by lay persons in out-of-hospital settings?
|
A160. It has been shown to contribute to significant gains in full neurologic and functional recovery
|
|
|
Q161. What is the most accurate parameter during the 2nd trimester to assess Gestational Age? During the 1st trimester?
|
A161. Biparietal diameter; Crown-rump length
|
|
|
Q162. What is the leading cause of congenital hearing loss?
|
A162. CMV
|
|
|
Q163. Define the 2nd stage of labor
|
A163. Period from complete cervical dilation to complete delivery of the baby
|
|
|
Q164. Define the 3rd stage of labor
|
A164. delivery of the baby and ends with delivery of the placenta
|
|
|
Q165. When are secondary causes of N/V during pregnancy usually suspected?
|
A165. after 9 WGA
|
|
|
Q166. What can be given safely during pregnancy for N/V?
|
A166. Metoclopramide is not associated with an increased risk of adverse effects on the fetus
|
|
|
Q167. A 12-year old wrestler comes to your office c/o of recurrent painful rash on his arm. There appear to be several dry vesicles. What is the most likely diagnosis?
|
A167. Herpes gladiatorum caused by herpes simplex
|
|
|
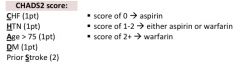
Q168. In a patient with Atrial Fibrillation, what confers the greatest risk of stroke?
|
A168. Previous history of a stroke or TIA; other factors are: CHF, Hypertension, Age greater than 75, DM; CHADS is the mnemonic
|
|
|
Q169. In a patient with HIV infection, the threshold for initiating treatment for TB after PPD screening is an induration greater than or equal to:
|
A169. 5 mm
|
|
|
Q170. What symptoms are most suggestive of CHF in a 6-mo old white male presenting with tachypnea?
|
A170. Diaphoresis with feeding
|
|
|
Q171. What pain reliever should be avoided when managing chronic pain in the elderly? Why?
|
A171. Propoxyphene; Its efficacy is similar to that of aspirin or acetaminophen alone, but drug accumulation, neurotoxicity effects, and ataxia or dizziness may add unnecessary morbidity in older patients. Acetaminophen, hydrocodone, oxycodone, and hydromorphone are options for treating chronic pain in elderly
|
|
|
Q172. 20 year old female runner has a 1 week history of constant groin pain. There is limited hip motion on flexion and internal rotation of the right hip. Radiographs of the hip and pelvis are normal. What is the most likely diagnosis?
|
A172. Stress fracture of the right femoral neck
|
|
|
Q173. A runner has stinging pain over the lateral femoral epicondyle. What is the most likely diagnosis?
|
A173. Iliotibial band syndrome
|
|
|
Q174. A distance runner presents with pain in the anterior pelvic area and tenderness over the symphisis pubis. Diagnosis?
|
A174. Osteitis pubis
|
|
|
Q175. Uterine rupture is a potential complication of attempted VBAC. The most reliable indication that uterine rupture may have occurred is what?
|
A175. Fetal Bradycardia
|
|
|
Q176. A 14 year old AA female presents for a routine evaluation. On exam, you note a rubbery, well-defined, nontender breast mass approximately 2 cm in diameter. The patient denies any history of breast tenderness, nipple discharge, or skin changes. Diagnosis?
|
A176. Fibroadenoma; slow growing, nontender, rubbery, well-defined mass, most commonly in the upper, outer quadrant
|
|
|
Q177. Breast disease found in older adolescents and is characterized by bilateral nodularity and cyclic tenderness
|
A177. Fibrocystic disease
|
|
|
Q178. Spongy, tender breast mass with symptoms exacerbated by menses
|
A178. Benign breast cyst; frequently multiple and spontaneous regression occurs in 50% of patients
|
|
|
Q179. Firm, rubbery breast mass that may enlarge rapidly and is associated with skin necrosis.
|
A179. Cystosarcoma phyllodes
|
|
|
Q180. When is the probability of pregnancy after unprotected intercourse the highest?
|
A180. 1 day before ovulation
|
|
|
Q181. Patients with Wolff-Parkinson-White syndrome who have episodic symptomatic supraventricular tachycardia or Atrial fibrillation benefit most from what treatment?
|
A181. Radiofrequency catheter ablation of bypass tracts
|
|
|
Q182. A moderately obese 50 year old AA female presents with colicky right upper quadrant pain that radiates to her right shoulder. What is the most likely diagnosis? What is the best study to confirm the cause?
|
A182. Cholelithiasis; Abdominal sono
|
|
|
Q183. A 62 yo female with numbness in the LE and macrocytosis has a normal serum folate level and serum B12 level of 200 pg/mL (N 150-800). What lab finding would confirm diagnosis of B12 deficiency?
|
A183. elevated Methylmalonic Acid
|
|
|
Q184. What is a reduced haptoglobin level useful to confirm?
|
A184. Hemolytic anemia
|
|
|
Q185. What 2 things can lead to an elevated free erythrocyte protoporphyrin level?
|
A185. Lead poisoning and Iron deficiency
|
|
|
Q186. In what disease is an elevated ACE found?
|
A186. Sarcoidosis
|
|
|
Q187. What 2 drug classes have been found to decrease mortality after MI?
|
A187. Beta-blockers; ACE inhibitors
|
|
|
Q188. How often should young adults (until age of 40) have a routine physical exam?
|
A188. every 3-5 years
|
|
|
Q189. At what age are mammograms recommended?
|
A189. after age 40
|
|
|
Q190. A 23 yo hispanic female at 18 wks gestation presents with a 4 wk history of a new facial rash. She noticed worsening with sun exposure. On exam, you note symmetric, hyperpigmented patches on her cheeks and upper lip. Diagnosis?
|
A190. Melasma (Chloasma)
|
|
|
Q191. A rare polymorphous skin eruption of unknown origin occurring in late pregnancy that is more common on the extremities than on the trunk. It may recur during each subsequent pregnancy.
|
A191. Herpes gestationis
|
|
|
Q192. Treatment of asymptomatic chlamydial infections in women reduces their risk of developing these 4 things
|
A192. 1. PID; 2. Tubal infertility; 3. Ectopic pregnancy; 4. Chronic pelvic pain
|
|
|
Q193. What is the DOC for chlamydial infections in women?
|
A193. Azithromycin
|
|
|
Q194. Sexual contacts of a woman with chlamydial infection during what preceding number of days should be treated empirically or test for infection and treated if positive?; How long should a patient avoid intercourse after initiation of treatment?
|
A194. 60 days; 7 days
|
|
|
Q195. Cellulitis in patients after breast lumpectomy is thought to be related to lymphedema. What 2 things predispose to these infections?; What is the most common organism associated with this infection?
|
A195. Axillary dissection & Radiation; Non-group A hemolytic strep
|
|
|
Q196. What 3 drugs are used to treat Acute uncomplicated cystitis?
|
A196. Bactrim; Fluoroquinolone; Nitrofurantoin
|
|
|
Q197. Describe the McRoberts maneuver for managing shoulder dystocia
|
A197. Maximal flexion and abduction of the maternal hips
|
|
|
Q198. What would be the most appropriate empiric therapy for nursing home-acquired pneumonia in a patient with no other underlying disease?
|
A198. Levaquin
|
|
|
Q199. What criteria define Severe Preeclampsia?
|
A199. BP 160/110 on two occasions > 6 hrs apart; Proteinuria > 5 g / 24h; Thrombocytopenia with platelet count < 100,000; Liver enzyme abnormalities; Epigastric or RUQ pain; Alteration of mental status
|
|
|
Q200. What criteria define MILD Preeclampsia?
|
A200. BP > 140/90 on two occasions > 6 h apart; Proteinuria >300 mg / 24 h
|
|
|
Q201. What is the best initial screening test for Hereditary Hemochromatosis?; What are the symptoms of this disease?
|
A201. Serum Transferrin Saturation; Bronze skin pigmentation, glucose intolerance, hypogonadism, arthropathy of the MCP joints, heart failure, or cirrhosis
|
|
|
Q202. When is the median age of closure for the anterior fontanelle in newborns?
|
A202. 13.8 months of age
|
|
|
Q203. Describe the mechanism of Vasovagal syncope
|
A203. Period of high sympathetic tone (often induced by pain or fear), followed by sudden sympathetic withdrawal, which then triggers a paradoxical vasodilation and hypotension
|
|
|
Q204. What test is useful in diagnosing Vasovagal Syncope?
|
A204. Tilt testing, which causes pooling in the legs; Demonstrates Hypotension and Bradycardia
|
|
|
Q205. What is the antibiotic of choice for a dog bite?
|
A205. Amoxicillin/Clavulanate
|
|
|
Q206. When evaluating a patient with a solitary thyroid nodule, what are red flags indicating possible thyroid cancer? (8)
|
A206. 1. Male gender; 2. < 20 years or > 60 years; 3. rapid growth of nodule; 4. Symptoms of local invasion such as dysphagia, neck pain, & hoarseness; 5. History of head or neck radiation; 6. FH of thyroid CA; 7. hard, fixed nodule > 4 cm; 8. Cervical lymphadenopathy
|
|
|
Q207. In a euthyroid patient with a palbable nodule, what is the first test that should be ordered?
|
A207. Fine-needle aspiration
|
|
|
Q208. Studies have shown that Epidural analgesia during labor increase the incidence of these things
|
A208. 1. increase length of both First and Second stage of labor; 2. increase rate of instrument-assisted delivery; 3. Fourth degree laceration; 4. likelihood of maternal fever
|
|
|
Q209. A positive flexion abduction external rotation (FABER) test that elicits posterior pain indicates involvement of which joint?; Anterior pain?
|
A209. Sacroiliac; Hip involvement
|
|
|
Q210. What is the most effective long-term management of the majority of patients with Bipolar disorder?
|
A210. Lithium
|
|
|
Q211. What is the most appropriate therapy for a patient with DVT? What should the INR be maintained at?
|
A211. Initial SQ LMW-heparin (Enoxaparin) followed by PO Warfarin for 3-6 months; INR: 2-3
|
|
|
Q212. What should the INR be maintained at for patients with mechanical heart valves?
|
A212. 2.5-3.5
|
|
|
Q213. Gamekeeper's thumb is associated with a sprain of what?; How does it occur?
|
A213. Ulnar Collateral Ligament; Hyperextension and Hyperabduction of the thumb, usually as a result of a fall; *also called Skier's thumb
|
|
|
Q214. This is seen in a patient with a history of hypertriglyceridemia and severe abdominal pain with vomiting over the last 6 hours. WBC of 20,000; Glucose 295; AST 333; LDH 375; Most likely diagnosis?; What is the name of the sign shown in the picture? What does it indicate?
|
A214. Acute Pancreatitis; Grey Turner's sign indicates hemorrhage and a mortality rate approaching 50%
|
|
|
Q215. What effects does Estrogen have on the laboratory results of HDL and LDL?
|
A215. HDL -> increased; LDL -> decreased
|
|
|
Q216. Antidote to Atropine poisoning
|
A216. Physostigmine
|
|
|
Q217. Antidote for Cyanide poisonig
|
A217. Amyl nitrate
|
|
|
Q218. Antidote for Magnesium poisoning
|
A218. Calcium carbonate
|
|
|
Q219. Antidote for Ethylene glycol poisoning
|
A219. Ethanol and Pyridoxine
|
|
|
Q220. Antidote to Organic phosphates
|
A220. Atropine
|
|
|
Q221. What can be taken 45 minutes prior to Niacin administration to decrease flushing?
|
A221. Aspirin
|
|
|
Q222. What joint is usually affected in gout? What is this called?; What are the crystals in Gout?
|
A222. Metatarsophalangeal Joint; Podagra; Monosodium urate crystals
|
|
|
Q223. Antibiotic recommended in the treatment of a Brown Recluse spider bite?
|
A223. Dapsone
|
|
|
Q224. What can be done to distinguish Atrial Flutter from Sinus Tachycardia
|
A224. Carotid Massage; Atrial Flutter = regular, rapid cardiac rhythm characterized by an ectopic focus that gives rise to atrial rates from 280-350 per minute. Usually impulses are only transmitted to ventricles every 2nd, 3rd, or 4th impulse
|
|
|
Q225. DOC for Trigeminal Neuralgia?
|
A225. Carbamazepine (others are Phenytoin and Baclofin)
|
|
|
Q226. What ADR's have Methicillin and Nafcillin been associated with?
|
A226. Interstitial Nephritis with Renal Tubular Acidosis
|
|
|
Q227. What is the most common inherited bleeding disorder?; How can it be diagnosed?; Treatment for bleeding episodes?
|
A227. von Willebrand's disease (autosomal dominant); normal PT, prolonged PTT resulting from Factor 8 deficiency (vWF carries Factor 8); Ristocetin cofactor assay measures ability of vWF to agglutinate platelets in vitro in the presence of ristocetin; Cryoprecipitate or Factor 8 concentrate; or DDAVP (vasopressin) causes release of vWF from endothelial cells
|
|
|
Q228. This murmur is associated with severe chronic aortic regurgitation and may be middiastolic or presystolic. It occurs when there is backflow of blood from the aorta into the LV and flow into the LV from the LA. The regurgitant stream often prevents the full opening of the mitral valve, thus obstructing flow into the ventricle.
|
A228. Austin Flint murmur
|
|
|
Q229. This murmur affects children and is described as a humming or musical-sounding systolic murmur that is loudest at the left sternal border. It is a benign murmur. The murmur is usually heard in children 3-7 years of age and disappears before the onset of puberty
|
A229. Still's murmur
|
|
|
Q230. What ECG findings may be found in a patient with a Pulmonary Embolism? (3)
|
A230. Right Axis Deviation; S1-Q3-T3 pattern; Right Bundle Branch Block
|
|
|
Q231. When are children allowed to go back to school or daycare after having Strep Throat?
|
A231. After having taken the antibiotic for 24 hours and temperature has returned to normal
|
|
|
Q232. A 17 year old girl presents to your office. She had a URI 1 wk before the visit. She now complains of severe vertigo. Diagnosis?
|
A232. Vestibular Neuronitis = Acute Labrinthitis
|
|
|
Q233. Where is the most common location for the development of Morton's Neuroma?
|
A233. interdigital nerves b/w the 3rd and 4th metatarsal heads
|
|
|
Q234. What characterizes PVC's (premature ventricular contractions)? What can make them disappear?
|
A234. wide QRS complexes without a preceding P wave; Exercise
|
|
|
Q235. Severe complication of Warfarin that is unrelated to bleeding?
|
A235. Skin necrosis
|
|
|
Q236. Alternate name for Shin Splints?
|
A236. Medial Tibial Stress Syndrome; Physical examination reveals tenderness along several centimeters at the posteromedial border of the tibia, whereas a more focal anterior tibial tenderness suggests a stress fracture
|
|
|
Q237. Treatment of choice for Pyoderma Gangrenosum?
|
A237. Steroid therapy; Pyoderma gangrenosum also may develop in surgical scars, fistulas, and ostomy sites. However, pyoderma gangrenosum is an immune-mediated, inflammatory condition commonly associated with inflammatory bowel disease and immunodeficient states. These ulcers are painful with well-demarcated, undermined edges. They have a purulent, dusky purple base, surrounding erythema, and satellite pustules
|
|
|
Q238. Best treatment for chronic allergic rhinitis?
|
A238. Intranasal steroids
|
|
|
Q239. A 72 y/o smoker with a positive history of severe DJD, diabetes, and CVD presents c/o bilateral leg pain that occurs after walking 200 yards. He reports that rest improves his Sx's. Diagnosis and testing
|
A239. Claudication + Ankle/Brachial indices
|
|
|
Q240. 36 y/o runner presents with pain associated with the anterior heel. The pt reports his Sx's are worse on awakening and improve as the day progresses. Diagnosis?
|
A240. Plantar Fascitis
|
|
|
Q241. 52 y/o man is seen for fevers & wt loss. CXR shows mediastinal lymphadenopathy. Labs show hypercalcemia, elevated Alk Phos, and elevated ACE. Diagnosis?
|
A241. Sarcoidosis
|
|
|
Q242. What EKG finding is associated with Hypothermia?
|
A242. J (Osborne) wave = positive deflection after the QRS complex
|
|
|
Q243. A BUN:Cr ratio greater than 20 indicates?
|
A243. Prerenal causes; hypovolemia; cardiogenic shock; sepsis; anaphylaxis; drugs; renal artery stenosis; FeNa < 1% because kidneys are trying to conserve Na
|
|
|
Q244. What test is used in the initial evaluation of persistent hemoptysis
|
A244. CXR then if mass is noted then do flexible bronchoscopy; Hemoptysis = bright red blood and alkaline from the lungs
|
|
|
Q245. Progressive motor neuron disease that affects the corticospinal tracts &/or anterior horn cells &/or bulbar motor nuclei = ?
|
A245. ALS
|
|
|
Q246. 32-year-old man presents with recurrent oral and genital ulcers. He also has had arthalgias. Recently he was administered a tetanus vaccination and developed a sterile abscess at the site of the injection. Most likely diagnosis?
|
A246. Behcet's Syndrome; Behçet's disease is a multisystem inflammatory condition, probably of autoimmune origin, that is triggered by infectious antigens or other antigens in genetically predisposed persons. Recurrent, painful ulcerations of the oral and genital mucosa are the most common symptoms. Therapeutic agents, such as topical or intralesional corticosteroids, generally are used only for palliative therapy. Sucralfate, which is commonly used in the treatment of peptic ulcers, can also heal ulcers of the gastrointestinal tract. However, its effectiveness in healing oral and genital ulcerations is unknown. Behçet disease (BD), also known as Behçet syndrome, is a chronic form of vasculitis (inflammation of the blood vessels) involving four primary symptoms: oral and genital ulcers, ocular inflammation, and arthritis.
|
|
|
Q247. A boy who plays Little League baseball presents with swelling over the lateral elbow and pain with valgus and varus stress while flexing and extending the elbow. The patient reports locking of the elbow. Radiographs show the presence of loose bodies. Diagnosis?
|
A247. Osteochondritis dissecans; In osteochondritis dissecans, a loose piece of bone and cartilage separates from the end of the bone because of a loss of blood supply. The loose piece may stay in place or fall into the joint space, making the joint unstable. This causes pain and feelings that the joint is "catching" or "giving way."; These loose pieces are sometimes called "joint mice."; Osteochondritis dissecans usually affects the knees and elbows.
|
|
|
Q248. Describe Ludwig's Angina; What is a serious complication?
|
A248. Infection invloving the sublingual and submaxillary space usually due to poor dental hygiene, tooth extraction, or trauma; Tongue displacement upwards compromising the airway
|
|
|
Q249. A 28 year old homosexual man presents to your office c/o of nonproductive cough, SOB, fever, chills. CXR shows bilateral interstitial infiltrates. Diagnosis? Treatment?
|
A249. Pneumocystis; IV Bactrim
|
|
|
Q250. What is the treatment for a patient suspected of Wernicke- Korsakoff Syndrome?
|
A250. Thiamine followed by IV Dextrose
|
|
|
Q251. What is the name of the test that confirms Benign Positional Vertigo?
|
A251. Dix-Hallpike maneuver = turn patient's head to the side while having them go from a sitting to lying position with head positioned below the level of the bed; BPV = severe episodes of vertigo that usually last less than 1 minute and are precipitated by certain head movements. Nystagmus is usually associated. Pathophysiology: caused by free-floating particulate matter in the semi-circular canals, usually the posterior canal (the most dependent structure of the labyrinth). movement of this debris causes endolymph movement/pressure and cupular deflection; this causes an imbalance in the signals from the labyrinths resulting in vertigo; the particles are calcium carbonate crystals and are referred to as “ otoliths”
|
|
|
Q252. If an elderly man is diagnosed with Myasthenia Gravis what else should you suspect?
|
A252. Thymoma
|
|
|
Q253. A 60-year-old woman presents with complaints of diffuse proximal muscle pain, low-grade fevers, and generalized fatigue. Labs show elevated ESR and mild anemia. Diagnosis? Rx?
|
A253. Polymyalgia Rheumatica; inflammatory disease with pain and stiffness associated with proximal muscles; more common in women; symmetrical pain and morning stiffness in neck, shoulders, and hips; fever, generalized fatigue, anorexia, & wt. loss; elevated ESR and anemia of chronic disease; Rx = oral corticosteroids (prednisone)
|
|
|
Q254. A 16 yo girl presents c/o throat pain, difficulty swallowing, and trismus (spasm of jaw muscles). PE shows redness and enlargement of the left tonsillar pillar. The patient holds her head to the left side and has muffled speech. Diagnosis?
|
A254. Peritonsillar abscess
|
|
|
Q255. A 65 year old man c/o gynecomastia and galactorrhe with erectile dysfunction. Most likely diagnosis? Rx?
|
A255. Prolactinoma; Dopamine agonist; Cabergoline, Bromocriptine, Pergolide
|
|
|
Q256. MCC of chronic cough?
|
A256. Postnasal drip
|
|
|
Q257. A 62 yo woman presents c/o joint pain, polyuria, polydipsia, and generalized fatigue. The woman reports a history of recurrent kidney stones and depression. Radiographs show osteopenia and subperiosteal resorption on the phalanges. What blood test may help determine the cause of her symptoms?
|
A257. Parathyroid hormone level for Primary Hyperparathyroidism
|
|
|
Q258. What is the treatment for someone under the age of 35 who has a + PPD test but no evidence of disease (including a - CXR)?
|
A258. INH for 6 months
|
|
|
Q259. What is the name of a test that can be performed to diagnose Raynaud's phenomenon?
|
A259. Allen's Test = occlude the radial and ulnar arteries while the patient makes a fist, the hand is the opened and one side of the wrist is released. Blood flow to the hand should be detected by color, which is restored to the hand. If the hand remains pale and cyanotic with either of the 2 sides, Raynaud's phenomenon should be suspected
|
|
|
Q260. Recurrent vertigo, tinnitus, and hearing loss are all hallmark findings of what? What is the treatment?
|
A260. Meniere's Disease = endolymphatic hydrops (increased fluid pressure within the inner ear); Salt restriction + HCTZ
|
|
|
Q261. DOC for Cryptococcal meningeal infection?
|
A261. Amphotericin B & Flucytosine
|
|
|
Q262. A 28 year old man presents to your office c/o pain in the perirectal area for the last week. Exam shows an area of tenderness, redness, and induration (hardened) lateral to the anus. The area is warm and fluctuant. Most likely diagnosis? Treatment?
|
A262. Pilonidal cyst; Surgical incision and drainage
|
|
|
Q263. A 78 year old retired carpenter presents c/o gradually increasing right-sided shoulder pain. Pt is unable to sleep on his right side and has difficulty raising right arm. PE shows ROM is significantly restricted. X-rays show osteopenia of humeral head. Most likely diagnosis?
|
A263. Adhesive capsulitis
|
|
|
Q264. What supplement has been associated with an increased risk of lung cancer in smokers?
|
A264. Beta-carotene
|
|
|
Q265. What 3 groups of people should be treated for Asymptomatic Bacteriuria?
|
A265. 1. pregnant women; 2. pts with renal transplants; 3. pts who are about to undergo GU tract procedures
|
|
|
Q266. A 2 cm nodule is found on the left lobe of the thyroid in a healthy 40 year old woman. What is the most appropriate management at this time?
|
A266. Fine-needle aspiration
|
|
|
Q267. A 38 year old describes severe rectal pain associated with pallor, diaphoresis, and tachycardia that lasts for only a few minutes. The pain occurs mostly at night and are described as spasms. Diagnosis?
|
A267. Proctalgia fugax is a unique anal pain. ★ - Patients with proctalgia fugax experience severe episodes of spasm-like pain that often occur at night. ★ - Proctalgia fugax may only occur once a year or may be experienced in waves of three or four times per week. ★ - Each episode lasts only minutes, but the pain is excruciating and may be accompanied by sweating, pallor and tachycardia. ★ - Patients experience urgency to defecate, yet pass no stool. ★ - No specific etiology has been found, but proctalgia fugax may be associated with spastic contractions of the rectum or the muscular pelvic floor in irritable bowel syndrome. ★ - Reassurance that the condition is benign may be helpful, but little can be done to treat proctalgia fugax. ★ - Medications are not helpful since the episode is likely to be over before the drugs become active. ★ - Sitting in a tub of hot water or, alternatively, applying ice may provide symptomatic relief. ★ - A low dose of diazepam (Valium) at bedtime may be beneficial in cases of frequent and disabling proctalgia fugax
|
|
|
Q268. A 21 yo returns from a camping trip early c/o dull numbness affecting his upper left extremity He recalls a sharp pinprick sensation before the development of symptoms. The pt now describes a cramping pain & muscle rigidity of the back and chest area. A red, indurated area is found on the distal left arm. The pt has profuse sweating, nausea, vomiting, and SOB. Diagnosis?
|
A268. Black Widow spider envenomation
|
|
|
Q268. A 21 yo returns from a camping trip early c/o dull numbness affecting his upper left extremity He recalls a sharp pinprick sensation before the development of symptoms. The pt now describes a cramping pain & muscle rigidity of the back and chest area. A red, indurated area is found on the distal left arm. The pt has profuse sweating, nausea, vomiting, and SOB. Diagnosis?
|
A268. Black Widow spider envenomation
|
|
|
Q269. A 75 year old man presents to your office c/o flashes of light and blurred vision. He reports no pain. In-office exam reveals no findings other than decreased visual acuity. Most likely diagnosis?
|
A269. Retinal detachment; painless; dark floaters; flashes of light; blurred vision; REFER TO OPHTHALMOLOGIST
|
|
|
Q270. Subnormal visual acuity in one or both eyes despite correction of refractive error = ?
|
A270. Amblyopia; lazy eye; results when a child suppresses the vision in one eye to avoid diplopia; most common cause is strabismus (misalignment of the eyes)
|
|
|
Q271. 12 year old boy presents c/o gradual, increasing hip pain that radiates to the thigh and knee. PE shows an obese boy with pain associated with hip abduction and adduction. Radiographs show evidence of acetabular dysplasia. Diagnosis?
|
A271. Slipped Capital Femoral Epiphyses; femoral head slips posteriorly and inferiorly exposing the anterior and superior aspects of the metaphysis of the femoral neck
|
|
|
Q272. Idiopathic aseptic necrosis of the femoral head is also known as?
|
A272. Legg-Calve-Perthes disease
|
|
|
Q273. The most common cause of a limp in a 5 year old boy is?
|
A273. Transient Synovitis of the hip; Transient synovitis is the most common cause of hip pain in children. Many children will have a history of recent minor trauma, although this is obviously nonspecific in this age group. Transient synovitis typically affects young children who present with a limp of acute onset. On examination, the child will often refuse to use the affected leg and will have pain with any motion. Most children rapidly improve over two to three days, and more serious conditions such as a septic arthritis or juvenile rheumatoid arthritis should be considered if this rapid improvement is not seen.
|
|
|
Q274. What is the most common bacterial pathogen associated with lung infections in adolescents? Rx?
|
A274. Mycoplasma pneumonia -> malaise, sore throat, coryza, myalgias, and increasing productive cough of mucopurulent or blood-streaked sputum; Erythromycin
|
|
|
Q275. What 3 criteria can define boys as having "delayed sexual maturation"?
|
A275. 1. no testicular development by age 13.5 years; 2. no pubic hair by age 15 years; 3. more than 5 years between initial and completed growth of the genitalia
|
|
|
Q276. Describe Posterior Urethral Valves
|
A276. Valves are secondary to abnormal folds in the prostatic urethra that enlarge with voiding and cause obstruction of the urethral lumen; Symptoms include decreased urinary stream, overflow incontinence, and UTI's with dysuria.
|
|
|
Q277. What is the most common curvature in scoliosis?
|
A277. to the right in the thoracic spine, causing the right shoulder to be higher than the left
|
|
|
Q278. The most common cause of septic joint in an immigrant 3- year-old boy with no prior immunizations would be?
|
A278. H. influenza
|
|
|
Q279. A newborn is cyanotic shortly after birth and CXR shows the characteristic "egg on a string". Diagnosis?
|
A279. Tranposition of Great Vessels
|
|
|
Q280. A 3-month-old girl is brought in b/c she has been having excessive non-purulent tearing from the left eye for the past 4 weeks. Diagnois and treatment?
|
A280. Dacryostenosis; Massage the duct twice daily as it usually resolves by 6 months of age
|
|
|
Q281. Transient Cortical Blindness:; Cause?; How long before resolves?; CT and EEG findings?
|
A281. Cause: mild head trauma; Resolves within 24 hours; CT: unremarkable; EEG: initially shows slowing but resolves as blindness dissipates
|
|
|
Q282. A painless, cystic structure in the scrotum that transilluminates but is not associated with the presence of sperm is most likely?
|
A282. Hydrocele; (vs. a Varicocele, which is an enlargement of the pampiniform plexus due to incompetent valves of the veins)
|
|
|
Q283. Explain Tick Paralysis
|
A283. Dermacentor and Amblyomma have been linked to tick paralysis that causes muscle weakness, anorexia, lack of coordination, lethargy, nystagmus, and an ascending flaccid paralysis; Caused by inoculation of a neurotoxin found in the tick's salivary gland; Antibiotics are not indicated, but symptomatic treatment is
|
|
|
Q284. Syringomyelia may expand during adolescent years. Typically, what is the first neurologic deficit seen?
|
A284. Pain and temperature sensation
|
|
|
Q285. Are high or low frequency sounds affected first in Presbycusis?
|
A285. High frequency sounds; Pt. usually c/o trouble hearing normal conversations in crowds
|
|
|
Q286. Describe each of the 4 stages of pressure ulcers
|
A286. 1. localized area of nonblanchable, red skin; 2. break in the skin with surrounding redness and induration; 3. full-thickness ulcer that extends to the subcutaneous layer but not thru the underlying fascia; 4. ulcer penetrates the deep fascia exposing bone or underlying muscle
|
|
|
Q287. A 79 year-old woman with a history of atherosclerosis and HTN is seen in the ER. The pt reports she suddenly lost her vision in her left eye on awakening this morning. She reports no pain associated with the eye and has no other symptoms. Funcuscopic examination shows disk swelling, extensive retinal hemorrhages, and cotton-wool spots. The most likely diagnosis is?
|
A287. Central Retinal Vein Occlusion
|
|
|
Q288. What is the triad characteristic of Normal Pressure Hydrocephalus?
|
A288. 1. Dementia; 2. Gait ataxia = stuttering gait in which the initiation of gait is hesitant but gives way to walking; 3. Urinary incontinence Due to inadequate absorption of CSF
|
|
|
Q289. How to treat rhinitis medicamentosa
|
A289. stop offending agent and start inhaled/oral corticosteroids to wean off of steroids
|
|
|
Q290. who gets anterior epistaxis? how is it treated?
|
A290. young people with chronic nosebleeds, treat by cauterizing with silver nitrate
|
|
|
Q291. who gets posterior epistaxis? how to treat
|
A291. elderly, hypertensives. Pt. needs referral to ENT
|
|
|
Q292. Of the following, which is a risk factor in developing Otitis Media:; Tonsillar hypertrophy; Adenoidal hypertrophy
|
A292. Adenoidal hypertrophy
|
|
|
Q293. What percent chance of developing otitis media is associated with:; RSV?; Adenovirus/Influenza
|
A293. RSV - 33%; Adeno/Inf. - 28%
|
|
|
Q294. What precent of otitis media bugs are PCN/Amox resistant?
|
A294. 20-30%
|
|
|
Q295. How long can a middle ear effusion take to resolve following otitis media?
|
A295. up to 16 weeks
|
|
|
Q296. What other anomaly is found in half of people with coarctation?
|
A296. Bicuspid aortic valve
|
|
|
Q297. What are the top 3 valvular abnormalities caused by Rheumatic Fever?
|
A297. 1. MR; 2. AS; 3. AS+MS
|
|
|
Q298. What is the most common problem that Mitral Stenosis causes?
|
A298. Systemic embolus due to left atrial enlargement.
|
|
|
Q299. What is the mortality rate associated with a first heart attack?
|
A299. 0.25
|
|
|
Q300. Patients with unstable angina have a __% chance of MI in 2 years.
|
A300. 0.12
|
|
|
Q301. What drugs are good to treat prinzmetal's angina? what is a poor choice to treat it?
|
A301. Calcium channel blocker and ACE inhibitor. Beta blockers are a poor choice because they may aggravate small vessel spasm
|
|
|
Q302. What is a good test to differentiate Paroxysmal Atrial Tachycardia with block from AVNRT?
|
A302. Vagal maneuvers (carotid sinus massage/valsalva) cause an AV node block. Since supraventricular tachycardias occur independent of the AV node, there will be no response. So, PAT with block will not be slowed while AVNRT could be converted with a vagal maneuver.
|
|
|
Q303. PAT can be due to toxicity from what drug?
|
A303. Digoxin
|
|
|
Q304. 55 year old woman who is unable to lie flat because of SOB. No edema. 50% EF. what drug treatment is best?
|
A304. This woman has LV CHF with Diastolic dysfracturen (EF>40%). This is best treated with a Calcium channel blocker because of their anti-ischemic actions, preload reduction, BP control, LVH regression potential, and HR control which allows increased coronary filling during prolonged diastolic relaxation.
|
|
|
Q305. What is systolic dysfunction defined as (2 things) and what drug is best used to treat it?
|
A305. EF < 40%, dilated heart. Digoxin + a thiazide is best to treat a symptomatic (orthopnea, neck veins, edema) person with CHF. ACE inhibitors work well also
|
|
|
Q306. Name 3 drug classes used to slow down A-fib with RVR
|
A306. Digoxin, Beta Blocker, Calcium channel blocker
|
|
|
Q307. When should patients be anticoagulated before A-fib conversion?
|
A307. when they have had A-fib for > 2 days
|
|
|
Q308. Is LVH a characteristic of diastolic or systolic dysfunction?
|
A308. Diastolic
|
|
|
Q309. Why are calcium channel blockers and beta blockers relatively contraindicated in systolic dysfunction?
|
A309. they have negative inotropism
|
|
|
Q310. What are some characteristics of systolic dysfunction
|
A310. 1. Reduced EF; 2. Increased end diastolic pressure; 3. Increased resistance to flow
|
|
|
Q311. Name one other cause of a systemic embolism besides Afib.
|
A311. MI
|
|
|
Q312. Would you suspect embolism or thrombosis in a patient with Afib, MS, LAE, Claudication
|
A312. Embolism in AF, MS, LAE; Thrombosis in Claudication
|
|
|
Q313. What is the earliest sign and most sensitive indicator of chronic occlusive disease?
|
A313. ABI < .9
|
|
|
Q314. What causes a descending (2) vs. ascending (2) AAA?
|
A314. Descending - atherosclerosis, trauma (rarely); Ascending - cystic medial necrosis, syphilis
|
|
|
Q315. How does the caliber, length and flow rate of vessels affect 5 year patency rates of balloon angioplasties?
|
A315. High flow rate, larger caliber, and occluded segment < 3cm are associated with higher patency rates
|
|
|
Q316. How much does treatment of DVT with anticoagulants decrease the risk of PE?
|
A316. by 50%
|
|
|
Q317. How do you treat a superficial thrombophlebitis with no extension to deep venous systems?
|
A317. Heat + NSAIDS (excision not indicated)
|
|
|
Q318. What sign is most consistent with a hemorrhagic stroke?
|
A318. severe headache
|
|
|
Q319. What complication has the greatest morbidity in patients with subarachnoid hemorrhage? how can it be treated?
|
A319. Vasospasm - treat with a calcium channel blocker
|
|
|
Q320. What is reflex sympathetic dystrophy?
|
A320. syndrome of burning pains, tenderness, vasomotor skin changes, hyperesthesia, and edema usually to a hand or foot following trauma, peripheral nerve injury, or stroke
|
|
|
Q321. What is a major side effect of Ticlopidine when used in a patient with a recent ischemic stroke?
|
A321. Neutropenia
|
|
|
Q322. What is the stroke risk in a male with 70% carotid stenosis? How much does a carotid endarterectomy decrease the risk?
|
A322. 2% per year. Endarterectomy will reduce risk by 53%
|
|
|
Q323. How does a chronic subdural hematoma usually present?
|
A323. headache or confusion, patients don't usually present with neuro defecits
|
|
|
Q324. What is the post traumatic hematoma that can appear anytime within 24 hours of the trauma?
|
A324. epidural
|
|
|
Q325. A musical murmur in childhood that usually disappears by puberty
|
A325. Still's murmur
|
|
|
Q326. Most common congenital heart defect
|
A326. VSD
|
|
|
Q327. What two populations are normal pulmonary flow murmurs heard in?
|
A327. 3rd trimester and adolescents
|
|
|
Q328. What is a jugular venous hum?
|
A328. A buzz like noise heard throughout the cardiac cycle in some kids. It is produced by cerebral blood flow hitting the right angle at the innominate vein. There is no clinical siginificance
|
|
|
Q329. Harsh murmur at the 2nd left intercostal space that radiates to the back
|
A329. PS
|
|
|
Q330. How can the severity of PS be evaluated on physical exam?
|
A330. degree of RVH
|
|
|
Q331. What physical exam finding best correlates with the severity of AS?
|
A331. Palpable thrill in the suprasternal notch
|
|
|
Q332. How is a PDA treated in newborns?
|
A332. A PDA should be given 48 hours of observation to close on its own, after that indomethacin can be used. If indomethacin is not successful, surgical ligation can be used
|
|
|
Q333. How should a carotid bruit in a child be treated?
|
A333. No treatment, they aren't a big deal
|
|
|
Q334. When is a PVC concerning in children?
|
A334. when they occur in couplets or triplets, they are more likely to go into vtach
|
|
|
Q335. What are the two heart defects that cause cyanosis in infancy and when are they usually cyanotic?
|
A335. Transposition - becomes cyanotic withn the first few days of life after the ductus arteriosus closes; Tetralogy - more likely to be cyanotic within the first few weeks of life
|
|
|
Q336. What is the largest risk factor for HTN?
|
A336. DMII
|
|
|
Q337. What percent of newly diagnosied HTN is secondary?
|
A337. 5-10%
|
|
|
Q338. Primary aldosteronism is due to an adenoma ____% of the time (rather than idiopathic hyperplasia)
|
A338. 70-90%
|
|
|
Q339. When and how much does CrCl begin to decrease in life?
|
A339. CrCl falls by 1ml/min/1.73m2/year beginning at age 30-35
|
|
|
Q340. What is an acceptable range of microalbuminuria:; in HTN?; in DM?
|
A340. HTN - 200-500 mg/24hrs; DMII - 30-300 mg/24hrs
|
|
|
Q341. What is the rate of renal decline once PCKD begins to affect renal function
|
A341. CrCl declines by half every 36 months
|
|
|
Q342. What is the blood pressure target for:; Non African americans/non diabetics?; African americans/diabetics?
|
A342. non AA/non DM - < 130/80; AA/DM - < 125/75
|
|
|
Q343. What meds does HTN in the elderly typically respond to and which don't they respond to?
|
A343. Typically, HTN in the elderly is less sensitive to beta blockers and more sensitive to diuretics.
|
|
|
Q344. New onset diastolic HTN in the elderly suggests what?
|
A344. It suggests changing physiology such as reovascular processes (renal artery obs. chronic GN, or nephrosclerosis) and high renin states.
|
|
|
Q345. How does HTN and treatment differ between high renin, low renin, and normal renin?
|
A345. High renin (10% of HTN)- These patients will respond better to beta blockers and ACE inhibitors; Low renin (30-40% of HTN)- lower than normal renin activity for a given salt intake leads to "salt sensitive" HTN. These patients can best be treated with thiazied diuretics. Normal renin - (55% of HTN) These patients respond to both families of drugs, and often better when diuretics are combined.
|
|
|
Q346. How can hyperinsulinemia increase vascular tone (4)?
|
A346. 1) Promotes Na+ retention; 2) Promotes hypertrophy or hyperplasia of vascular smooth muscle; 3) modifying ion transport leading to an increase in intracellular Ca++; 4) Sympathetic activation
|
|
|
Q347. What are the side effects of HCTZ (4) and at what dose do they usually occur?
|
A347. > 25 mg/day; 1) hyperlipidemia; 2) hyperuricemia; 3) hypokalemia; 4) carbohydrate intolerance
|
|
|
Q348. How does the efficacy of HCTZ change with age/race?
|
A348. HCTZ is effective in the majority of african americans / elderly populations. HCTZ is effective in only 30-40% of caucasians
|
|
|
Q349. List the four leading causes of ESRD.
|
A349. Diabetic nephropathy; Hypertensive nephropathy; Chronic GN; PCKD
|
|
|
Q350. What percent of pts. is a thiazide used as a first line drug effective?
|
A350. 30-40%
|
|
|
Q351. Differentiate between broca's and wernicke's aphasia and the location of the lesion in each.
|
A351. Broca's - lesion in the lower posterior frontal lobe and presents with good comprehension but non-fluent effortful speech often associated with Right hemiparesis. Wernicke's aphasia - Posterior/Superior frontal lobe. Presents with poor comprehension, abundant, fluid, well articulated speech that makes no sense.
|
|
|
Q352. How does a sensory defect affect Alzheimer's disease
|
A352. Alzheimer's disease is exacerbated in the presence of another sensory defect.
|
|
|
Q353. How does Parkinson's disease usually begin?
|
A353. unilateral tremor
|
|
|
Q354. What are some autonomic dysfunctions associated with Parkinson's?
|
A354. Orthostatic hypotension, constipation, and impotence.
|
|
|
Q355. Tacrine - use? major side effect?
|
A355. Tacrine is a cholinesterase inhibitor used to treat Alzheimer's and its major side effect is elevation of serum transaminases.
|
|
|
Q356. Benztropine. Mech? use?
|
A356. anticholinergic used to reduce the tremor in PD
|
|
|
Q357. What are two drugs that reduce the rigidity associated with Parkinson's Disease?
|
A357. Levodopa and Amantidine
|
|
|
Q358. What are two drugs that can treat absence seizures? when do absence seizurs usually stop occurring?
|
A358. Valproic acid and ethosuximide. Absence seizures usually resolve around adolescence.
|
|
|
Q359. What are two firstline treatments for generalized or focal seizures?
|
A359. Phenytoin and phenobarbitol
|
|
|
Q360. What are 3 pulmonary bugs that can complicate a viral infection?
|
A360. Strep pneumo, H flu, Staph aureus
|
|
|
Q361. What virus is most likely to cause pneumonia?
|
A361. Influenza
|
|
|
Q362. What is the criteria for a fluid to be considered an exudate?
|
A362. Pleural fluid : serum protein > .5; Pleural fluid : serum LDH >.6
|
|
|
Q363. What does retrosternal airspace suggest in CXR?
|
A363. COPD
|
|
|
Q364. What drug is the first line agent to treat COPD?
|
A364. Ipratropium bromide is preferred over corticosteroids, beta agonists, and theophylline because of a better side effect profile.
|
|
|
Q365. Most bronchiolitis cases are caused by ___?
|
A365. RSV
|
|
|
Q366. What viral infection can lead to asthma later in life if a child is infected multiple times?
|
A366. RSV
|
|
|
Q367. What 2 bugs are responsible for the majority of respiratory infections from birth to 3 months?
|
A367. Chlamydia trachomatis and GBS
|
|
|
Q368. What 2 bugs are suspected in lobar pneumonia in a 4 year old? Which one causes a monoarticular arthritis?
|
A368. H flu and S. pneumo. H flu causes the arthritis. (treat with ceftriaxone)
|
|
|
Q369. What is the best empiric treatment of URI in a 3 month - 5 year old
|
A369. Erythromycin because of its effectiveness against S. pneumo, Chlamydia pneumoniae, and Mycoplasma
|
|
|
Q370. What causes croup, what is the peak age range, and what is the hospitalization rate for kids?
|
A370. Parainfluenza; 3 months - 6 years; <10% hospitalization rates
|
|
|
Q371. Muffled speech, drooling, stridor, and agitation with the child's head held in a sniffing position.
|
A371. Epiglottitis
|
|
|
Q372. Epiglottitis:; Diagnostic Xray sign?; Treatment?
|
A372. Thumb sign on lateral neck CXR; Treat with ceftriaxone or ampicillin
|
|
|
Q373. What are the indications for adding a daily anti-inflammatory to an asthmatic
|
A373. Use of beta agonist >3x/week; 20% variance in twice daily peak flows; < 80% of predicted peak flow; < 80% of patient's peak flow history
|
|
|
Q374. Differentiate the etiologies of the following causes of dysphagia:; difficulty swallowing solids and liquids; rapidly progressing dysphagia with weight loss; slowly progressing dysphagia over months to years; Intermittent acute sx or spasmodic obstruction; odynophagia of recent onset
|
A374. -esophageal motor disorder; esophageal cancer; benign stricture; esophageal ring; ulcerative esophagitis
|
|
|
Q375. What is the best treatment for GERD?
|
A375. PPI's (esp. omeprazole) are the most potent and reliably successful therapy in treating GERD
|
|
|
Q376. What are some risk factors for esophageal carcinoma?; (race, sex, other Ca, health conditions, social history)
|
A376. Nasopharyngeal Ca; Long standing achalasia; Tylosis (hyperkeratosis); Male; Alcohol use; Blacks
|
|
|
Q377. What percent of chest pain is caused by GI?
|
A377. 40%
|
|
|
Q378. What NSAID has the most ulcerogenic properties?
|
A378. ASA
|
|
|
Q379. What is the average 5 year recurrence rate of Crohn's after surgical treatment?
|
A379. 75%
|
|
|
Q380. What percent of patients with diverticulosis will develop diverticulitis?
|
A380. 20%
|
|
|
Q381. What are three diseases known to be associated with UC?
|
A381. Pyoderma gangrenosum,; Cholangitis,; arthropathies
|
|
|
Q382. What bug is responsible:; 1. incubation 6-48 hours, 33% of all bacterially caused food poisoning; 2. incubation 3-6 hours, vomiting/diarrhea, sx last 24-48 hours. ham, pork, canned beef, cream filled pastry; 3. incubation 8-24 hours, lasts < 24 hours. beef, turkey, chicken; 4. watery diarrhea, seafood; 5. Incubation 9-18 hours, Diarrhea or Vomiting, lasts 3 days
|
A382. 1. Salmonella; 2. Staph aureus; 3. C. pergringens; 4. Vibrio parahaemolyticus; 5. B. cereus
|
|
|
Q383. does the obturator sign suggest appendicitis or hernia
|
A383. appendicitis
|
|
|
Q384. What is the most common cause of bowel obstruction in the first two years of life and what are some presenting signs (5)?
|
A384. Intussusception which presents as colicky abd pain, currant jelly stools, reflex vomiting, leukocytosis, and a palpable mass
|
|
|
Q385. What does a first degree relative of CCA or adenomatous polyp do to your chance of getting colon cancer
|
A385. It raises it from 2.5% to 7-7.5%
|
|
|
Q386. An elevated GGT in the presence of normal AlkPhos is _____ until proven otherwise
|
A386. Alcohol
|
|
|
Q387. What is the most specific diagnostic criterion for PBC?
|
A387. AMA
|
|
|
Q388. _____ is associated with 60% of patients who have PSC
|
A388. IBD
|
|
|
Q389. recent history of jaundice and fever, no h/o alcohol use, homosexuality, or IVDA. Negative GB ultrasound, negative hepatitis screen,; elevated ALT, AST, Alk Phos, and Tbili and conjugated bili; AMA; Resolution with ABX; How is the dx confirmed?
|
A389. Primary Sclerosing Cholangitis - confirmed by ERCP
|
|
|
Q390. What are the three diseases included under Autoimmune liver disease?
|
A390. Autoimmune hepatitis - involves the parenchyma rather than the collecting system. 75% of cases. Treatment with steroids is effective; PSC, PBC are the other two
|
|
|
Q391. Ascites with a serum albumin:peritoneal fluid albumin ratio of 1:1 suggests what etiology?
|
A391. Cirrhosis
|
|
|
Q392. What should you suspect in a cirrhotic patient with fever and abdominal pain? What two tests should be ordered?
|
A392. Spontaneous Bacterial Peritonitis. Order a diagnostic peritoneal tap and CBC
|
|
|
Q393. Which hepatitis is most dangerous in pregnancy?
|
A393. Hep E
|
|
|
Q394. How do you treat acute bacterial prostatitis
|
A394. 2 week course of Fluroquinolones
|
|
|
Q395. What bacteria produces struvite stones?
|
A395. The urea splitting organisms which is usually proteus, but can also be ureaplasma
|
|
|
Q396. How does a patient with hemorrhagic cystitis present?
|
A396. Dysuria, frequency, urgency prior to or with the hematuria
|
|
|
Q397. When is the only time when males are more likely to get UTIs than females?
|
A397. during the first year of life, uncircumsized males are more likely to get UTIs
|
|
|
Q398. What study would be most likely to demonstrate VUR in a child?
|
A398. Radionuclide cystogram
|
|
|
Q399. What is the most common urinart tract abnormality in kids?
|
A399. VUR
|
|
|
Q400. How is a 3 year old with newly diagnosed VUR treated?
|
A400. With prophylactic ABX because most cases will resolve within a year
|
|
|
Q401. What is the most common presenting sign of pyelo?
|
A401. Fever
|
|
|
Q402. What type of amenorrhea will respond to a methylprogesterone challenge?
|
A402. Anovulatory cycle - this condition involves appropriate estrogen priming of the endometrium, but no egg release and thus no progesterone phase and no menstruation
|
|
|
Q403. Define Asherman's syndrome
|
A403. an obstruction to uterine outflow usually due to fibrous tissue development in response to infectionn, endometrial instrumentation, or therapeutic abotion
|
|
|
Q404. What is the underlying problem when a patient fails to respond to a progesin challenge, but does respond to a reproduction of the estrogen/progestin cycle.
|
A404. This would rule out uterine obstruction and would likely be an absence of estrogen stimulation of the uterus
|
|
|
Q405. Will PCOS patients bleed in response to progesterone withdrawal? What are PCOS patients at risk for?
|
A405. PCOS patients have amenorrhea secondary to anovulatory cycles, so they will respond to progesterone withdrawl. Their unopposed estrogen stimulation poses a risk for endometrial hyperplasia
|
|
|
Q406. What are women with hypothalamic amenorrhea at increased risk for?
|
A406. Osteoporosis
|
|
|
Q407. What level of FSH confirms the dx of ovarian failure (usually due to menopause)? What step is taken at this point?
|
A407. >20 IU, begin HRT
|
|
|
Q408. What is the change found most often after surgical rather than natural menopause?
|
A408. Loss of libido is more in a surgical hysterectomy
|
|
|
Q409. What is the most significant predicted benefit of HRT?
|
A409. 50% reduction in CAD
|
|
|
Q410. When is ERT contraindicated?
|
A410. When the uterus is present
|
|
|
Q411. What should be done if a patient is still experiencing uterine bleeding after 6 months of HRT?
|
A411. Endometrial Bx since postmenapausal bleeding is the hallmark for endometrial carcinoma
|
|
|
Q412. What percent of patients with unilateral bloody nipple discharge will end up having cancer?
|
A412. 33%
|
|
|
Q413. What age range does the largest percentage of breast cancer occur?; List the percentages that occur in each age group.
|
A413. >65 years old (>50%); 50-65 (25%); <50 (25%)
|
|
|
Q414. What is the most common cause of complaint of breast pain?
|
A414. Costochondritis
|
|
|
Q415. What is the size limit for lumpectomy + radiation?
|
A415. 5 cm
|
|
|
Q416. Orchitis due to mumps spreads to the testes by what route?
|
A416. Hematogenous spread is the usual route by which viruses spread to produce orchitis
|
|
|
Q417. What testicular abnormality is often associated with infertility?
|
A417. Varicocele - a varicosity of veins in the pampiniform plexus
|
|
|
Q418. What condition is a contraindication to the use of a vacuum device to achieve an erection?
|
A418. Sickle Cell
|
|
|
Q419. What is an important side effect of papavrine?
|
A419. Priapism
|
|
|
Q420. What are the top two cancer deaths in men?
|
A420. Lung and Prostate
|
|
|
Q421. When should annual PSA/DRE begin in asymptomatic AA men?
|
A421. 40
|
|
|
Q422. What type of cancer is most common associated with cryptochordism? Does surgically descending the testical decrease cancer risk?
|
A422. Seminoma - descending does not reduce risk of cancer, but it allows for earlier detection
|
|
|
Q423. What test is the best to confirm testicular torsion?
|
A423. Testicular scintillation scan
|
|
|
Q424. What are two sexual changes that are not considered normal in elderly men
|
A424. Testicular atrophy and decrease in libido
|
|
|
Q425. What cervical nerve roots are most affected by cervical disc herniation and spondylosis?
|
A425. C6, C7
|
|
|
Q426. What physical exam finding would lead most strongly to the diagnosis of cervical radiculopathy?
|
A426. Atrophy of hand/arm muscles
|
|
|
Q427. What is the preferred imaging modality to evaluate cervical radiculopathy?
|
A427. C-spine xrays (not MRI)
|
|
|
Q428. Pain experienced upon active abduction at the shoulder is indicative of what?
|
A428. Rotator cuff tendonitis
|
|
|
Q429. What fracture is seen in anterior dislocations of the humerus?
|
A429. posterolateral humeral head fracture
|
|
|
Q430. A positive Finklestein's test is indicitive of what?
|
A430. De Queverian's tenosynovitis
|
|
|
Q431. What is the general rule to determine if a humerus fracture requires ORIF?
|
A431. >45 degrees of displacement or a fracture through pathologic bone
|
|
|
Q432. A football player who develops hip pain after being tackled and has pain with rotation and lateral bending of the trunk would most likely have an injury to what part of the hip?
|
A432. Iliac Crest (hip pointer)
|
|
|
Q433. Differentiate between Osgood Schlatter and Patellofemoral Instability
|
A433. Osgood Schlatter - pain at the tibial tubercle; Patellofemoral - Pain in activities where the knee is flexed. No jointline or patella tenderness
|
|
|
Q434. What additional injury is likely to be found with an acl tear?
|
A434. MCL tear
|
|
|
Q435. How does tibial stress syndrome usually present? What is a risk factor?
|
A435. Posteromedial tibial pain lasting 1-2 hours after resuming a running program. A risk factor is a flat foot. If the pain does not improve after 1-2 hours, evaluation for a stress fracture is required
|
|
|
Q436. The most commonly sprained ligament in the ankle
|
A436. Anterior talofibular ligament
|
|
|
Q437. How does treatment of a sprain with an avulsion fracture differ from treatment of a sprain
|
A437. They are treated the same
|
|
|
Q438. What movement is painful in a patient with a fracture of the posterior process of the talus?
|
A438. Plantar flexion
|
|
|
Q439. What location (1st - 5th) of a metatarsal stress fracture requires more aggressive management?
|
A439. The 5th metatarsal, it is more likely to become a complete fracture with non union
|
|
|
Q440. What are the top 3 most common underlying factors in recurrent otitis media?
|
A440. Atopic Constitution; Adenoid hypertrophy; Congenital palatal deformity
|
|
|
Q441. How does passive motion affect OA?
|
A441. It exacerbates it.
|
|
|
Q442. What are some signs of ehlers Danlos syndrome?
|
A442. Hyperextensibility of joints, soft stretchy skin, open gaping wounds, easy bruisability. Patients can also develop arthralgias from overuse aggrivated by loose joint capsules.
|
|
|
Q443. RA postinactivity swelling lasts a minimum of ____ minutes
|
A443. 30
|
|
|
Q444. How long does RA remain monoarticular?
|
A444. up to 5 years
|
|
|
Q445. What is the first line agent for OA?
|
A445. Acetaminophen
|
|
|
Q446. What are 3 typical xray findings in OA?
|
A446. Joint space narrowing; Bone Spurs; Subchondral new bone formation
|
|
|
Q447. Subperiosteal bone resorption is indicative of what? Where is this best visualized?
|
A447. HyperPTH - best seen in radiographs of the fingers where, on the radial side of the phalanyx, the cortex has undergone resorption
|
|
|
Q448. Calcification of hyaline and fibrous cartilage is indicative of what?
|
A448. Pseudogout
|
|
|
Q449. What 3 things can precipitate Gout (2 drugs, 1 IV agent)
|
A449. Aspirin,; Thiazides,; IV dye
|
|
|
Q450. Between Gout and Psuedogout, which is limited to the weight bearing joints? Which is more likely to be polyarticular?
|
A450. Gout is limited to weight bearing joints; Pseudogout can be polyarticular
|
|
|
Q451. Why is aspirin not a good choice for patients with an acute gout attack?
|
A451. ASA in low doses decreases renal uric acid excretion. All other NSAIDs are excellent first line agents
|
|
|
Q452. Why is Colchicine not a good choice for Acute gout attack?
|
A452. because it may cause diarrhea, nausea, and emesis before an effective dose can be achieved
|
|
|
Q453. Developmental dysplasia of the hip has a family history in ___% of cases. What screening tool should be used in these kids?
|
A453. 20% have a fhistory, use ultrasonographic screening
|
|
|
Q454. What is the age cutoff of nonsurgical treatment of developmental dislocation of the hip?
|
A454. 6 months
|
|
|
Q455. With respect to delayed development of the hip, what percentage of the time is:; Left hip alone affected?; Both hips affected?; Right hip alone affected?; Is it more common in females or males?
|
A455. Left hip - 60%; Both hips - 20%; Right hip 20%; Females are more common
|
|
|
Q456. Legg-Calves-Perthes disease is characterized by what?
|
A456. Avascular necrosis of the femoral head
|
|
|
Q457. What is the most significant risk factor in postchlamydial infectious arthriris?
|
A457. H/O multiple sex partners
|
|
|
Q458. What injury would you suspect from a patient who is repeatedly kneeling throughout the day?
|
A458. Prepatellar bursitis
|
|
|
Q459. At what age range could you expect Osgood Schlatter disease to remit?
|
A459. When the tubercle fuses between 9 and 15 years old
|
|
|
Q460. In patients with hip pain, what tests are necessary to rule out Legg-Calves-Perthes disease or a slipped femoral capital epiphysis?
|
A460. serial X-rays
|
|
|
Q461. What patter of ANA is most specific for SLE?
|
A461. Rim or peripheral pattern
|
|
|
Q462. What Ab is most commonly associated with neonatal lupus?
|
A462. Anti SS-A (anti ro)
|
|
|
Q463. What antibodies correlate most specifically with Limited Systemic Sclerosis?
|
A463. Anticentromere
|
|
|
Q464. What cancers are most commonly associated with dermatomyositis?
|
A464. Lung (most common), Stomach, Breast, ovary
|
|
|
Q465. Decribe the classic presentation of dermatomyositis.
|
A465. Proximal muscle weakness, violaceous plaques on the dorsal aspect of interphalangeal joints, edema and violaceous coloring of upper eyelids.
|
|
|
Q466. What are some blood tests that are elevated in polymyositis, how is a definitive dx established?
|
A466. Elevated LDH, CPK, SGOT. An open muscle bx is req'd for dx.
|
|
|
Q467. What antibody tests are most specific for Sjrogrens syndrome?
|
A467. Anti SS-A and SS-B (ro and la)
|
|
|
Q468. What are two findings (one clinical and one serologic) needed to dx mixed CTD?
|
A468. Clinical evidence of more than 2 CTDs and elevation of anti- RNP
|
|
|
Q469. How is Henoch-Schonlein purpura started?
|
A469. Viral respiratory infection
|
|
|
Q470. Claudication, Angina, cold extremities in a young adult woman
|
A470. Takayasu's arteritis
|
|
|
Q471. PMR:; How long does it last?; How is it treated?; What age range?
|
A471. Lasts 6-9 months and is treated by moderate amounts of glucocorticoids; Over 50 years old
|
|
|
Q472. What percent of Behcet's patients have ocular manifestations?
|
A472. 90%
|
|
|
Q473. Wegners:; What gender is it most common?; What age range?; Triad of sx?
|
A473. Males; Middle age; Triad includes clinical disease in:; upper resp (nose bleeds, sinusitis); lower resp (hemoptysis); kidney
|
|
|
Q474. Define Grade I, II, and III concussions and when the patient can return to activity
|
A474. Grade I - Confusion, no amnesia. Return to normal activity in 20 min if sx are absent; Grade II - Confusion with Amnesia. Return to play in 1 week if sx absent; Grade III - LOC. Take to hospital, may return to conditioning after 1 asymptomatic week, return to play 1 month after 2 asymptomatic weeks
|
|
|
Q475. what is the official definition of AIDS?
|
A475. CD4>200
|
|
|
Q476. When are HIV patients more likely to get thrush?
|
A476. 200-500, also more likely to get diarrhea and weight loss
|
|
|
Q477. When are HIV patients more likely to get sebhorrea and folliculitis?
|
A477. 500-1000
|
|
|
Q478. What is the only fluid excreted by the body that contains a significant amount of HIV virus?
|
A478. Vaginal secretions
|
|
|
Q479. What health maintenance is necessary in HIV pts with:; CD4 < 500?; CD4 < 200?; CD4 50-75?
|
A479. <500: Check CD4/Viral load every 3 months; <200: PCP prophylaxis; 50-75: Mycobacterium avium prophylaxis
|
|
|
Q480. What AIDS patient population is more likely to develop Kaposi's sarcoma? What is the effect of treatment?
|
A480. Homosexual men are most likely and treatment only helps cosmetically by diminishing the size of the lesions.
|
|
|
Q481. What HIV drug can cause pancreatitis?
|
A481. Didanosine
|
|
|
Q482. How does treatment of TB change with HIV infected patietns
|
A482. INH treatment time doubles from 6 months to 1 year
|
|
|
Q483. What are the likely organisms responsible for the following symptoms in an HIV patient:; 1) 2 day h/o Occipital HA, fever, malaise in pt. with AIDS; 2) Space occupying lesion with focal neuro defecits; 3) retinitis, visual disturbance; 4) TB like pulmonary sx
|
A483. 1) Cryptococcus; 2) Toxo; 3) CMV; 4) Mycobacterium
|
|
|
Q484. What 3 opportunistic infections are seen in CD4<200?
|
A484. PCP, Kaposi, CMV retinitis
|
|
|
Q485. What test allows legoinnaire's disease to be distinguished from other pneumonitidies?
|
A485. elevated CK
|
|
|
Q486. What is the indicated treatment for Legionnaire's disease?
|
A486. Erythromycin with Rifampin. Other macrolides or sulfamethoxazole can also be used.
|
|
|
Q487. What is the minimum exposure time to a tick in order to be exposed to lyme disease?
|
A487. 24 hours
|
|
|
Q488. Describe stage 1, 2 and 3 of lyme disease. When does each stage begin?
|
A488. Stage 1 - erythema chronicum migrans (lasts 7 days); Stage 2 - dermal, CNS, MS systemic symptoms, begins 30 days after exposure; Stage 3 - First degree AV block among some stage 2 symptoms
|
|
|
Q489. What is the largest risk factor for TB?
|
A489. IVDA
|
|
|
Q490. What are the incubation periods of the following:; RMSF?; Lyme disease?
|
A490. RMSF - 4 days; Lyme - 7 days
|
|
|
Q491. What is the estimated prevalence (in millions) of DM in the US? What percent is undiagnosed?
|
A491. 10-20 million, 50% are undiagnosed
|
|
|
Q492. What HLA types are associated with DM I?
|
A492. DR3, DR4
|
|
|
Q493. How many calories per gram are carbohydrates, protein, and fat? What percent of each is recommended in a diet?
|
A493. 55% Carbs: 4 cal/gram; 15% Protein: 4 cal/gram; <33% Fat: 8 cal/gram
|
|
|
Q494. How many units per kg are usually req'd in a diabetic?
|
A494. .5-1 U/kg
|
|
|
Q495. What is the recommended protein intake for diabetics to prevent renal failure? (in g/kg/day)
|
A495. .75 g/kg/day
|
|
|
Q496. What is the most sensitive diagnostic indicator of diabetic peripheral neuropathy? (found on PE)
|
A496. Loss of ankle jerk
|
|
|
Q497. What type of DM is Gestational diabetes most similar to? What causes it? When is an appropriate time to test women for it?
|
A497. most like type II, placental lactogen causes it and is at its highest during the beginning of the 3rd trimester of pregnancy, so testing should be done between 24-28 weeks.
|
|
|
Q498. What is the treatment for gestational diabetes?
|
A498. Insulin therapy
|
|
|
Q499. What is the general rule for approximating Creatinine clearance in people? (without using a formula)
|
A499. For young adults, the CrCl is usually around 100, and subtract 1 ml/hr for every year over 20.
|
|
|
Q500. What clinical scenario is direct measurement of free T3 (as opposed to calculation) most appropriate?
|
A500. T3 toxicosis - because T4 is normal in this situation
|
|
|
Q501. What is the cause of the widened palpebral fissures in thyrotoxicosis?
|
A501. elevated catecholamine state
|
|
|
Q502. How can you differentiate endogenous thryotoxicosis from exogenous thyrotoxicosis?; Name 1 way on PE and one lab value
|
A502. Endogenous thyrotoxicosis will have a palpable thyroid and will have a decreased I123 uptake.
|
|
|
Q503. What drug is best suited to give rapid relief of thryotoxicosis?
|
A503. Non selective beta blocker
|
|
|
Q504. What is the first lab abnormality to appear in hypothyroidism
|
A504. increasing TSH
|
|
|
Q505. What is the most common type of hypothyroidism in the US?
|
A505. Post ablative hypothyroidism due to surgery or radioiodine therapy
|
|
|
Q506. How long does treatment of hypothyroidism with levothyroxine take to achieve full effect?
|
A506. 1 month
|
|
|
Q507. What type of thyroid cancer results from childhood irradiation to the neck?
|
A507. Papillary
|
|
|
Q508. How much stronger is Dexamethasone than Prednisone?
|
A508. 10x
|
|
|
Q509. How will Primary vs Secondary adrenal insufficiency differ in response to ACTH?
|
A509. Primary - No change, since defect is in the adrenals; Secondary - Adrenals will be stimulated since defect is lack of ACTH secretion
|
|
|
Q510. What is a positive dexamethosone suppression test?
|
A510. >50% suppression of 17-hydroxycorticosteroid in the overnight suppression test
|
|
|
Q511. What is suspected when there is no response to low dose dexa suppression test but a response to high dose
|
A511. Cushing's disease - Pituitary tumor secreting ACTH
|
|
|
Q512. What effect does primary aldosteronism have on renin?
|
A512. low renin due to the effect of hypervolemia and sodium retention
|
|
|
Q513. What is the best way to test for pheo?
|
A513. 24 hour urine catecholamine and metanephrine levels. VMA is not nearly as sensitive
|
|
|
Q514. What is the most common type of CAH?
|
A514. 21 alpha hydroxylase deficiency
|
|
|
Q515. After infancy, children grow about ___ inches per year.
|
A515. 2" per year, but it occurs in spurts
|
|
|
Q516. What would elevated FSH indicate in the setting of delayed or failed puberty?
|
A516. a primary failure or primary gonadal failure as the cause.
|
|
|
Q517. What age ranges does puberty occur in boys and girls?
|
A517. Girls: 8-13; Boys: 8-14
|
|
|
Q518. What are the Tanner stages for Boys?
|
A518. I: no pubic hair, preadolescent genitalia; II: scant, slightly pigmented pubic hair, scrotum enlarged; III: small amt. of darker, coarser, curling pubic hair, longer penis, larger testes; IV: adult type pubic hair but less quantity, glans widened, testes approaching adult size, scrotum pigmented; V: pubic hair spread to thighs, adult genitalia
|
|
|
Q519. What are the tanner stages for girls?
|
A519. I: no pubic hair, preadolescent breasts (elevation of papilla only); II: Sparse, long straight, slightly pigmented hair on labia, visible or palpable breast buds, increased areolar diameter. III: small amt of darker, coarser, curlier hair spreading over mons pubis,enlargement of breast and areola with no separation of coutours; IV: Adult type, coarse, curly, pubic hair covering less area than adult, breast and papilla no separated by coutour; V: pubic hair forming inverted triangle, adult contoured breast with projection of the papilla only, areola more pigmented
|
|
|
Q520. What is the definition of delayed puberty?
|
A520. The continued absence of secondary sex characteristics by age 14 for boys and 12 for girls. Treatment is necessary to develop secondary sex characteristics and prevent short stature
|
|
|
Q521. What hormone would you use to treat central precocious puberty in a male?
|
A521. GnRH
|
|
|
Q522. At what age does Atopic dermatitis appear on cheeks?
|
A522. Infants
|
|
|
Q523. At what age does Atopic Dermatitis usually remit?
|
A523. Usually by age 20
|
|
|
Q524. What drug is a good choice for long time (30 hours) control of asthma symptoms?
|
A524. Salmeterol (B2 agonist)
|
|
|
Q525. What is the peak age range for seasonal allergies?
|
A525. 15-25
|
|
|
Q526. What is the measure of ability to diagnose presence of disease
|
A526. Sensitivity
|
|
|
Q527. What is the measure of the ability to be truly negative in the absence of disease?
|
A527. specificity
|
|
|
Q528. What is the max diastolic BP in hypertensive patients going to surgery?
|
A528. 110mmHg
|
|
|
Q529. What is the minimum time after a heart attack that a patient must wait for elective surgery?
|
A529. 3 months
|
|
|
Q530. What values of the following labs indicate severe malnourishment?; Albumin?; Transferrin?; Pre Albumin?; Lymphocytes?
|
A530. Albumin < 2.0; Transferrin < 100; Pre Albumin < 7; Lymphocytes < 1000
|
|
|
Q531. What delay is required for elective surgery following stabilization of CHF?
|
A531. 1 week
|
|
|
Q532. What age should you begin to order:; BUN/Cr?; Lytes/CXR?; Urinalysis/Albumin?; EKG?
|
A532. BUN/CR - >50; Lytes/CXR - >60; Urinalysis/Alb - >65; EKG - Women >50 Men >35
|
|
|
Q533. What screen is used for appropriate lung function to go to surgery?
|
A533. FEV1 > 2L
|
|
|
Q534. What is the one class of hypertensive meds that hypertensive patients must stop prior to surgery?
|
A534. Diuretics - to prevent hypokalemia
|
|
|
Q535. How long should the following blood thinners be stopped prior to surgery, and when can the patient begin to take them again after surgery?; Aspirin; Ticlopidine; Warfarin
|
A535. Aspirin - Stop 1 week prior; Restart 48 hours post; Ticlopidine - Stop 2 weeks pre; Restart 48 hours post; Warfarin - Stop 3-5 days pre; Restart 3-5 days post
|
|
|
Q536. What is an ideal TC:HDL ratio for a man?
|
A536. 4.5:1
|
|
|
Q537. How many calories per day does a very low calorie diet contain and who should go on it?
|
A537. 800 kcal per day for 12-16 weeks. Pts who are >30% overweight
|
|
|
Q538. What are the two effects of a fibrate on cholesterol?
|
A538. Decrease TG; Raise HDL
|
|
|
Q539. What type of cancer is reduced the soonest after smoking cessation?
|
A539. Bladder
|
|
|
Q540. After beginning a moderate exercise program, how long will it take to see a decrease in the resting pulse? How about an increase in endurance?
|
A540. 4-6 weeks for both
|
|
|
Q541. How long following an MI should exercise rehab begin?
|
A541. 2-4 weeks
|
|
|
Q542. What does silver nitrate prevent upon delivery?
|
A542. neonatal gonorrhea (chlamydia must be treated with erythromycin PO)
|
|
|
Q543. What type of Abs are provided in breast milk?
|
A543. IgA
|
|
|
Q544. what is an expected volume of food to feed a newborn and how many times per day?
|
A544. 1/2-1oz every 2 1/2-4 hours totaling 7 times per day.
|
|
|
Q545. What should be started by age 2 months in an infant with sickle cell disease?
|
A545. PCN because by age 2, they are functionally asplenis and at great risk for encapsulated organisms.
|
|
|
Q546. Differentiate between pathologic and physiologic jaundice in newborns
|
A546. Physiologic - unconjugated, peaks on 3rd or 4th day and declines by 1 week. Pathologic - appears within first 24 hours (or upon birth), conjugated, will last 7-10 days
|
|
|
Q547. What 4 inborn errors of metabolism must be screened for at birth?
|
A547. PKU, Galactosemia, biotinidase deficiency, hypothyroid
|
|
|
Q548. What age is associated with the highest death rate from drowning?
|
A548. 1-3 years old
|
|
|
Q549. What is increased hand to mouth activity suggest in kids?
|
A549. Lead poisoning
|
|
|
Q550. what type of anemia is seen in lead tox?
|
A550. microcytic, hypochromic anemia with basophilic stippling with a normal TIBC (which is what differentiates it from iron deficiency)
|
|
|
Q551. What age is MMR first given?
|
A551. 15 months
|
|
|
Q552. What are the top two leading causes of death in children?
|
A552. 1) MVA; 2) Fires and Burns
|
|
|
Q553. When should the first dose and booster of DTaP be given
|
A553. 1st - before 6 months; 2nd - 4-6 years old
|
|
|
Q554. When should the first dose of MMR and the booster be given?
|
A554. 1st dose - 12-15 months; booster - 4-6 years old
|
|
|
Q555. what is the attempted suicide rate among male adolescents?
|
A555. 10-15%
|
|
|
Q556. Of teenagers who smoke two cigarettes completely, what percent will eventually become regular smokers?
|
A556. 85%
|
|
|
Q557. When should Pap smears begin?
|
A557. after age 18
|
|
|
Q558. What is the recommended level of calcium intake for adolescents? adults?
|
A558. adolescents - 1200-1500mg/day; adults - 1500mg/day
|
|
|
Q559. What is the leading cause of cancer deaths in the 25-44 year old age group?
|
A559. Breast cancer
|
|
|
Q560. What percentage of premature deaths result from "unhealthy habits"?
|
A560. 50%
|
|
|
Q561. How often should a monogamous middle aged woman with 3 previous consecutive negative pap smears be getting a pap?
|
A561. every 3 years
|
|
|
Q562. How often should women in the 40-49 year age group get a screening mammography?
|
A562. every year
|
|
|
Q563. How does a family history of CCA change the screening guidelines?
|
A563. Changes the beginning of colonoscopy, FOBT, DRE from age 50 to age 40
|
|
|
Q564. When should DRE be initiated?
|
A564. age 40
|
|
|
Q565. What percent of 65 year olds have chronic dementia? 80 year olds?
|
A565. 65 years old - 5%; 80 years old - 20%
|
|
|
Q566. List some examples of basic ADLs
|
A566. eating, voiding, dressing, bathing
|
|
|
Q567. List some examples of instrumental ADLs
|
A567. shopping, telephone, preparing meals, housekeeping, doing laundry
|
|
|
Q568. What is the most serious common medical condition encountered in travel?
|
A568. Viral Hepatitis
|
|
|
Q569. What is the best choice of antibiotic for malaria prophylaxis in an area where there is chloroquine resistance?
|
A569. Mefloquine
|
|
|
Q570. What vaccination is recommended before travel to all developing countries?
|
A570. Influenza
|
|
|
Q571. When is the best time for a pregnant woman to travel?
|
A571. Second Trimester
|
|
|
Q572. What is the altitude where mountain sickness occurs in 25% of people? 50% of people
|
A572. 6500 feet and 10000 feet
|
|
|
Q573. What are the rules with Post MI and travel
|
A573. Not within 4 weeks of MI
|
|
|
Q574. For the following drugs, state how they work to prevent HACE/HAPE:; Dexamethosone; Acetazolamide; Nifedipine; Prochlorperazine
|
A574. Dexa - reduces cerebral edema; Acetazolamide - Increases ventilation thought induction of metabolic acidosis; Nifedipine - reduces pulmonary arterial pressure; Prochlorperazine - increases ventilatory drive
|
|
|
Q575. In an alcoholic with depression, which condition should be treated first?
|
A575. Alcoholism, then depression if it still exists 1 month after abstinence
|
|
|
Q576. What age range is depression the most common?
|
A576. 25-34
|
|
|
Q577. what percent of new mothers does post partum depression effect?
|
A577. 10%
|
|
|
Q578. What antidepressant would you give to someone who is also complaining of trouble sleeping?
|
A578. Amitriptyline
|
|
|
Q579. What are 4 common side effects of SSRIs?
|
A579. N/D, tremor, agitation
|
|
|
Q580. What antidepressant may cause dry mouth and sleepiness? how about nervousness and insomnia?
|
A580. Paroxetine; Fluoxetine
|
|
|
Q581. TCAs block the reuptake of what two neurotransmitters?
|
A581. Serotonin and Epinephrine
|
|
|
Q582. What is the most common method of suicide in teenagers?
|
A582. TCAs
|
|
|
Q583. What is the best choice to treat mixed anxiety and depression?
|
A583. TCAs
|
|
|
Q584. Which Benzo has the shortest half life?
|
A584. Alprazolam
|
|
|
Q585. What is the first line drug in panic attacks? What about if panic attacks are disabling?
|
A585. SSRIs are first line but use benzos if the attacks are disabling
|
|
|
Q586. What is first line for OCD?
|
A586. SSRIs
|
|
|
Q587. What drugs are first line for Generalized Anxiety Disorder?
|
A587. Azopirones (Buspirone)
|
|
|
Q588. What are the 3 criteria for somatization disorder?
|
A588. 1) multiple systems involved; 2) onset early in life; 3) abscence of abnormalities in tests
|
|
|
Q589. Describe a hypochondriac
|
A589. These patients fixate on a single disease and one persistent symptom at a time.
|
|
|
Q590. Which system does conversion disorder typically involve?
|
A590. Nervous System (sensory/motor)
|
|
|
Q591. Distinguish between Factitious disorder and Malingering
|
A591. Malingering - secondary gain (narcotics); Factitious disorder - patient has a less rational goal, patients often undergo many painful procedeures and only recieves the gain of "attention getting"
|
|
|
Q592. Describe somatic depressive equivalent
|
A592. Patients who have potentially serious symptoms (CP) and appear to be indifferent to the potentially serious symptoms.
|
|
|
Q593. Distinguish between hypochondriasis and somatic anxiety equivalent
|
A593. Hypochondriasis patients tend to focus on symptoms and are difficult to dissuade from their feared dx. The somatic anxiety patients focus on the disease, but are easily reassured with explanation
|
|
|
Q594. What disorder is implicated in a patient with symptoms that might have some serious implications, but the patient's body and facial language indicates a lack of concern
|
A594. Conversion disorder
|
|
|
Q595. sx of otitis externa; most common orgs
|
A595. pain on palpation of tragus or traction of the pinna; itchiness, prurulent d/c; pseudomonas, staph
|
|
|
Q596. tx of otitis externa
|
A596. acidic drops (less favorable environment for pseudo to thrive); ABx + steroids
|
|
|
Q597. tx for complete occlusion by cerumen
|
A597. H2O2; cerumenolytics; water irrigation (done after cerumenolytics); NEVER use curette to remove unless occlusion is incomplete
|
|
|
Q598. risk of topical nasal decongestant use
|
A598. rebound swelling after vasoconstrictuion wears off
|
|
|
Q599. what does weber test mean if it lateralizes to unaffected side?; if it lateralizes to affected side?
|
A599. sensorineural loss; conduction
|
|
|
Q600. tx of recurrent otitis media infection
|
A600. if <4 yo tympanostomy tubes; if >4 yo, adenoidectomy
|
|
|
Q601. when can kids return to school after starting ABx for strep throat
|
A601. after 24 hrs of tx
|
|
|
Q602. where is coccidiomycosis found
|
A602. 4 Corners
|
|
|
Q603. resp complication of chickenpox; tx?
|
A603. pneumonia, esp in pregnancy; IV acyclovir
|
|
|
Q604. pts who are susceptable to pseudomonas pneumonia
|
A604. pts with bronchiectasis; on steroids; pts recently taken broad spectrum ABx
|
|
|
Q605. pts susceptable to aspergillus pneumo
|
A605. those with prolonged neutropenia, immunosuppressed
|
|
|
Q606. most common causes for CAP
|
A606. S. pneumo; H, flu; M. pneumo
|
|
|
Q607. risk factors for legionella pneumo
|
A607. smokers; renal failure; CA; DM; COPD; immunosuppression
|
|
|
Q608. micro classification of legionella
|
A608. GNR
|
|
|
Q609. when does breast milk jaundice occur?; what is it and what is elevated?
|
A609. btwn 4-14 days; etiology is unknown, but something in breast milk inhibits bilirubin metabolism; unconjugated bili is elevated
|
|
|
Q610. what is breast feeding jaundice?; when does it occur
|
A610. jaundice caused by decreased volume of feeding; occurs on day 3 of life
|
|
|
Q611. tx fo breast milk jaundice
|
A611. continue breast feeding as long as possiblead increase frequency of feeds, this helps with conjugating the bili; phototherapy can be added; stopping breast feeding is a last resort
|
|
|
Q612. in what time frame would you expect to see pathologic jaundice
|
A612. within 24 hrs post-partum
|
|
|
Q613. tx for ABO incompatibility jaundice
|
A613. phototx then exchagne transfusion if absolutely necessary
|
|
|
Q614. progression of kernicterus
|
A614. increased bili is toxic to basal ganglia cells and brainstem nuclei --> hypotonicity and lethary, then CP, MR, and hypertonicity
|
|
|
Q615. who's got what blood type in ABO incompatibility of the infant and newborn
|
A615. mom has O and fetus has A, B, or AB
|
|
|
Q616. how frequently does jaundice of newborn develop
|
A616. 60%
|
|
|
Q617. when is phototherapy contraindicated in jaundice of the newborn
|
A617. when there is increased conjugated bilirubin; it can lead to bronze baby syndrome (permanent discoloration)
|
|
|
Q618. criteria for infantile colic
|
A618. unexplained fussiness x 3h/d, 3d/w, for longer than 3 wks, in an infant younger than 3 mo
|
|
|
Q619. physical findings in a colicky infant
|
A619. tense abdomen, clenched fists, flexed legs into abdomen, and flushing
|
|
|
Q620. which medication --> Reye's syndrome
|
A620. ASA
|
|
|
Q621. minimum weight gain during neonatal period
|
A621. >20 g/day
|
|
|
Q622. biological agents found in colostrum
|
A622. macrophages, complemetn, lysozymes, lactoferrin, AB vs bact/viruses
|
|
|
Q623. which class of AB is present in breast milk
|
A623. IgA
|
|
|
Q624. treatment of mastitis; which bacteria is usually implicated
|
A624. warm compresses and ABx (methicillin or cloxacillin); S. aureus; no need to stop breast feeding
|
|
|
Q625. what vitamin is human milk deficient in
|
A625. d
|
|
|
Q626. when is solid food added to diet
|
A626. 6 mo
|
|
|
Q627. major complications of formula feeding
|
A627. constipation; overfeeding
|
|
|
Q628. how to deal with constipation associated with formula feeds
|
A628. add increased fluid or corn syrup; if giving soy formula, switch to cow's
|
|
|
Q629. what is implicated in spitting up; how to reduce sx
|
A629. incompetent GE sphincter; sit infant up and increase burping frequency
|
|
|
Q630. noonan's syndrome
|
A630. a rare genetic disease, similar to turner's syndrome, with webbed neck and short stature, but no facial abnormalities
|
|
|
Q631. what are the recommendations for CIN II/III tx
|
A631. pap smear w or without colposcopy q6 mo until 3 negative results are obtained, then resume normal screening recommended by age.
|
|
|
Q632. how often should pap smears be performed in women <65 yo
|
A632. annually until there are 3 consecutive - smears in the setting of 1 monogamous partner
|
|
|
Q633. what immunizations should pts with cirrhosis receive?
|
A633. HAV, HBV, pneumococcal, flu
|
|
|
Q634. meaning of dexa scans
|
A634. if t score <-1.5 + risk factor or <-2.0 with no risk factors should receive preventive meds (bisphosphonates or SERMS)
|
|
|
Q635. which cholesterol meds will raise HDL?
|
A635. fibrates and niacin
|
|
|
Q636. screening protocol for AAA
|
A636. in 65-70 yo men who smoke or have h/o smoking should receive a 1-time abdominal US; if aorta >5.5 cm, then repair
|
|
|
Q637. who receives pneumococcal vaccine
|
A637. adults >65 yo or adults with chronic cv, lung, liver, kiney, metabolic disease or immunosuppression
|
|
|
Q638. screening procedure for ovarian ca
|
A638. women with isolated family h/o ovarian ca should get transvaginal u/s and CA 125 screening. If strong family history, check brca 1/2 twice a year and CA 125 and transvaginal u/s
|
|
|
Q639. who should receive routine chlamydia screening
|
A639. all women <24 yo, if sexually active
|
|
|
Q640. contraindication for varicella vaccine
|
A640. immunosuppression... it's a live attenuated vaccine
|
|
|
Q641. recommended screening for bladder ca
|
A641. there is none, no good tests exist
|
|
|
Q642. what is the mortality rate for HAV
|
A642. 3%
|
|
|
Q643. what is the #1 cause of conjunctivitis in children
|
A643. adenovirus
|
|
|
Q644. organism that causes the croup
|
A644. parainfluenza
|
|
|
Q645. tx for cluster ha
|
A645. triptans, 100% O2 (don't use ergotamine... takes too long to work)
|
|
|
Q646. prevention of menstrual ha
|
A646. low dose estrogen supplements, NSAIDS, ergot, tripans (do not use sSris)
|
|
|
Q647. tx for analgesic rebound ha
|
A647. tcas
|
|
|
Q648. tx for absence seizure
|
A648. ethosuxamide; valproic acid; clonazepam
|
|
|
Q649. most common causes for new onset seizure in >40 yo
|
A649. tumors > stroke > trauma
|
|
|
Q650. most common causes for status epilepticus
|
A650. decreased compliance with meds, EtOH withdrawal, intracranial infection, neoplasm, metabolic d/o
|
|
|
Q651. risk factors for febrile seizures in children
|
A651. + family history, previous febrile convulsions
|
|
|
Q652. sequelae of febrile seizures
|
A652. 98% of kids with febrile seizure don't develop addl seizures in 5 yrs, but it can progress if there are developmental delays, CP, abnormal neuro development, + fam h/o epilepsy
|
|
|
Q653. tx of febrile seizures
|
A653. diazepam q8 h
|
|
|
Q654. definition of fuo
|
A654. fever >38 x 3 wks, without an underlying dx
|
|
|
Q655. orgs that most commonly --> bacteremia in kids
|
A655. s. pneumo > hib > n. meningitis
|
|
|
Q656. what ABx should be given if to prevent spread of meningitis
|
A656. none!
|
|
|
Q657. prodrome of acute meningitis in kids; what can indicate septicemia
|
A657. resp illness, st (precedes fever), ha, stiff neck, vomiting; rash
|
|
|
Q658. why should juices not be given for rehdration following diarrhea
|
A658. increased OSM from juices --> hypernatremia and exacerbated stool loss
|
|
|
Q659. #1 cause of bacterial gastroenteritis; presentation
|
A659. campylobacter; fever, malaise, n/v/d, ab pain, bloody bm
|
|
|
Q660. which ABx is most commonly associated with diarrhea
|
A660. ampicillin
|
|
|
Q661. which childhood illnesses might present first with diarrhea
|
A661. acute appendicitis; OM; UTI; PNA
|
|
|
Q662. describe clinical manifestations associated with slipped capital femoral epiphysis
|
A662. seen in overweight sedentary teenage boys, pain is in groin or medial side of knee; there is limited internal rotation of hip
|
|
|
Q663. tx of slipped capital femoral epiphysis
|
A663. it is an emergency and must be stabilized; AVN can result
|
|
|
Q664. what is a complication of capital femoral epiphysis
|
A664. AVN!!!!
|
|
|
Q665. clinical features of legg-calve-perthes
|
A665. idiopathic avn in kids; pain in hip/knee, limp with decreased ROM
|
|
|
Q666. tx for legg-calve-perthes
|
A666. braces or casting for 2 yr s; or surgery --> normal fracture in 4-6 mo
|
|
|
Q667. sequelae of legg-calve-perthes
|
A667. 50% need hip replacement after adulthood
|
|
|
Q668. osgood schlatter: clinical features
|
A668. tenderness over tibial tuberosity; traction apophysitis in tibial tuberosity
|
|
|
Q669. tx of osgood schlatter:
|
A669. NO steroids; tx w rest
|
|
|
Q670. sequelae of osgood-schlatter
|
A670. avulsion fracture if patellar tendon can pull off tibial tubercle
|
|
|
Q671. presentation of patellofemoral syndrome
|
A671. anterior knee pain, exp when walking up stairs, or running; crepitus and tender undersurface of medial patella
|
|
|
Q672. tx of patellofemoral syndrome
|
A672. vastus medialis exercises to help keep patellar tendon aligned
|
|
|
Q673. when should children have established bladder control
|
A673. 5 yo
|
|
|
Q674. tx of enuresis; pharm?
|
A674. behavior modifications; adh just treats sx, but doesn't tx underlying cause
|
|
|
Q675. presentation of whooping cough in adult
|
A675. can be a post-infection cough lasting 4-6 w post infection; post-tussive emesis is common
|
|
|
Q676. is methalcholine challenge test effective in exercise induced asthma
|
A676. no
|
|
|
Q677. clinical features of vocal cord dysfracturen
|
A677. presents as difficult to treat asthma with normal spirometry (doesn't respond to any of the asthma drug tx)
|
|
|
Q678. how does depression affect sleep
|
A678. causes you to go into early REM, makes you easy to awaken... therefore poor quality sleep
|
|
|
Q679. signs of interstitial lung disease
|
A679. crackles, clubbing and cxr changes
|
|
|
Q680. pathophys of rotator cuff impingement
|
A680. supraspinatus tendon impinges on undersurface of coracoacromial arch
|
|
|
Q681. tx of rotator cuff injury
|
A681. strengthening end ROM exercises, if not successful, steroid injections; if all else fails after 3-6 mo, arthroscopc subacromial decompression
|
|
|
Q682. tx of lateral epicondylitis
|
A682. rest, nsaids, possibly steroid injections; surgical debridement is a last resort
|
|
|
Q683. sx of dequervian's tenosynovitis
|
A683. stenosing tenosynovitis of 1st dorsal compartment of wrist; caused by repetitive grasping/use of thumb; tenderness to palpation of radial styloid
|
|
|
Q684. tx of de quervian's tenosynovitis
|
A684. thumb splint and immobilitization for 3 w
|
|
|
Q685. "grades" of sprains
|
A685. I: tear of a few ligament fibers. joint is tender and painful, no joint laxity; II: mod # of torn fibers; mod swelling/pain; little to no instability of joint; III: complete laxity of joint, no endpoint when joint is stressed. prominent swelling
|
|
|
Q686. what is the most common ligament injured in ankle sprains? how do they occur?
|
A686. talofibular joint; inversion type injuries occur most commonly; max tenderness occurs at lateral malleolus
|
|
|
Q687. tx of ankle sprain
|
A687. early wb --> hastened return of activity
|
|
|
Q688. effusion seen with ACL tear? why?
|
A688. ACL is very vascular --> effusion seen immediately
|
|
|
Q689. mechanism of whiplash
|
A689. lower c-spine extends; upper c-spine flexes
|
|
|
Q690. best tx of whiplash
|
A690. early exercise
|
|
|
Q691. definition of concussion
|
A691. clinical syndrome characterized by immediate and transient post-traumatic impairment of consciousness, vision changes, and equilib changes due to brainstem involvement
|
|
|
Q692. levels of concussions
|
A692. grade I: no LOC, amnesia <30 mins; grade II: LOC <5 min and/or amnesia >30 mins but <24 h; grade III: LOC > 5min, amnesia >24 h
|
|
|
Q693. second impact syndrome
|
A693. 2nd hit after not recovering from first concussion; autoregulation of brain is lost and there is reactive swelling and edema; >50% mortality; LIMIT ACTIVITIES OF ALL ATHLETES W SX AFTER HEAD INJURY!!!
|
|
|
Q694. who should be screened for osteoporosis?
|
A694. all women >65 yo; if risk factors, >60 women
|
|
|
Q695. how long do RA sx have to be present for dx
|
A695. 6 wks
|
|
|
Q696. who would get parvovirus? complication?
|
A696. adults working with kids; > arthritis
|
|
|
Q697. sx of dermatomyositis
|
A697. PMR + rash
|
|
|
Q698. is there weakness in fibromyalgia
|
A698. no, just muscle pain
|
|
|
Q699. sx of aortic stenosis
|
A699. angina, syncope, doe
|
|
|
Q700. what test should be avoided in as?; how is dx made?
|
A700. exercise tolerence tests; echo
|
|
|
Q701. pathophys of baker cyst; when are they seen?
|
A701. increased fluid production from synovium; fluid accumulates in popliteal bursa; seen in OA, RA, cartilage tears
|
|
|
Q702. another name for obesity hypoventilation syndrome; what is associated w it?
|
A702. pickwickian syndrome; obesity, thick neck, hypersomnolence, polycythemia (2/2 alveolar hypovent)
|
|
|
Q703. benefits of lidocaine; adverse effects of lidocaine
|
A703. decreased PVC frequency, decreased risk of v-fib,; asystole- therefore, only use if absolutely needed
|
|
|
Q704. steps to study the esophagus
|
A704. contrast study; esophagoscopy (to exclude mechanical causes of dysphagia); manometry to confirm dx
|
|
|
Q705. what is the only pharm intervention proven to prolong life in hypoxemic pts?; non-pharm?
|
A705. supplemental o2; quitting smoking, and lung volume reduction
|
|
|
Q706. which drugs prolong sx in copd
|
A706. BB,; ipratropium,; theophylline
|
|
|
Q707. what is the paO2 that supplemental O2 is helpful for?
|
A707. 55-60 in setting of cor pulmonale
|
|
|
Q708. what do early am ha signify in copd?
|
A708. nocturnal co2 retention (O2 won't help)
|
|
|
Q709. tx of HTN in pregnancy
|
A709. hydralazine; methyldopa
|
|
|
Q710. what happens to LDL levels following ischemic event
|
A710. LDL decreases 24-48 hrs following ischemic event and takes weeks to return to baseline; in pts with known ca, they should go on statins
|
|
|
Q711. what cholesterol meds are contraindicated in pts with high TGs
|
A711. bile acid sequesterants
|
|
|
Q712. which cholesterol med raises LDLl
|
A712. fibrates
|
|
|
Q713. which cholesterol drug worsens insulin r
|
A713. niacin
|
|
|
Q714. what heart sound is heard with WPW
|
A714. paradoxically split s2
|
|
|
Q715. which drugs slow conduction at the av node?
|
A715. atenolol; diliazem
|
|
|
Q716. what can result if BB and CCB are combined
|
A716. av block
|
|
|
Q717. which is worse: Mobitz I or Mobitz II? why?
|
A717. Mobitz II, usually associated with BBB
|
|
|
Q718. GI sx of DM; tx?
|
A718. post-prandial bloating, early satiety, constipation, diarrhea; metoclopramide
|
|
|
Q719. where are blebs normally found in lungs? what are they?; complication?
|
A719. apex (ruptured alveoli); apical fibrosis
|
|
|
Q720. indication for HIDA scan?
|
A720. dx acute cholecystitis
|
|
|
Q721. what is the risk of transmitting HBV from mother to fetus?; tx of fetus?
|
A721. if HBeAg +, then 90% risk of vertical transmission; HB Ig, follow with HB vaccine (Ig is insufficient alone)
|
|
|
Q722. sx of vitreous hemorrhage; cause?
|
A722. sudden loss of vision and onset of floaters, fundus is hard to visualize; usually DM
|
|
|
Q723. what effects does acute pancreatitis have on the lung?
|
A723. pleural effusion or ARDS (15%)
|
|
|
Q724. prophylaxis of breast ca
|
A724. 49% decrease in dx if tamoxifen is given
|
|
|
Q725. tx for claudication
|
A725. CCB
|
|
|
Q726. test for lactose intolerance
|
A726. lactose H-breath test, increase in H2 levels after lactose; + clinitest for reducing substrates; increased osmotic gap, acidic stool
|
|
|
Q727. what is transferring sat?
|
A727. Serum Fe/TIBC
|
|
|
Q728. relationship between athlete's foot and cellulitis?
|
A728. athlete's foot --> leg cellulitis (latter caused by staph or strep)
|
|
|
Q729. chalazion; complications?
|
A729. nodular rubbery lesion, granulomatous; from obstructed; tear gland; can turn into squamous cell carcinoma, must bx
|
|
|
Q730. saddle anesthesia
|
A730. cauda equina syndrome
|
|
|
Q731. tx for v-tach without cardiac compromise
|
A731. amiodarone
|
|
|
Q732. complications from hemochromatosis
|
A732. hypogonadism; arthropathy; pancreatic endocrine dysfracturen; dilated cmp; conduction abnormalities
|
|
|
Q733. how does pulmonary fibrosis affect; lung volume; dlco; FEV/FVC
|
A733. decrease; decrease; normal
|
|
|
Q734. S3; S4
|
A734. floppy ventricle, so systolic dysfunction; stiffened ventricle, so diastolic dysfunction
|
|
|
Q735. when should digoxin be used in CHF?
|
A735. in a-fib w rapid vent rate or with decreased ef
|
|
|
Q736. what is the first line HTN med for ppl without other complications
|
A736. thiazides
|
|
|
Q737. what HTN med should be used in pts with recurrent strokes
|
A737. ace i + thiazide combo
|
|
|
Q738. what HTN med should be used to decrease strokes in dm
|
A738. CCB
|
|
|
Q739. what HTN med should be used in the elderly
|
A739. diuretics
|
|
|
Q740. what is the most effective long-term med for chronic bronchitis
|
A740. ipratropium bromide (anti-cholinergic)
|
|
|
Q741. blue bloater; pink puffer
|
A741. bronchitis; emphysema
|
|
|
Q742. tx of prinzmetal's angina
|
A742. CCB and nitrates
|
|
|
Q743. tx for chlamydia
|
A743. azithromycin or doxycycline
|
|
|
Q744. tx for bacterial vaginosis
|
A744. metronidazole,; clindamycin
|
|
|
Q745. tx for pubic lice
|
A745. permethrin
|
|
|
Q746. tx for hsv
|
A746. -cyclovir
|
|
|
Q747. tx for yeast infection
|
A747. fluconazole/terconazole
|
|
|
Q748. tx for gc
|
A748. ceftriaxone or quinolones
|
|
|
Q749. tx for trichomonas
|
A749. metronidazole
|
|
|
Q750. tx for chancroid
|
A750. ceftriaxone,; azithromycin,; erythromycin
|
|
|
Q751. tx for syphilis
|
A751. penicillin G
|
|
|
Q752. tx of condyloma acumulatum
|
A752. podofilox,; imiquinod,; podophillin,; benzoin
|
|
|
Q753. when should a pt with gc/chlamydia be retested following tx
|
A753. never, unless there is reason to believe the tx didn't work
|
|
|
Q754. what, if given to a pt with mono --> rash
|
A754. PCN
|
|
|
Q755. describe streptococcal rash
|
A755. feels like sandpaper
|
|
|
Q756. when should tonsillectomy be considered
|
A756. if 3x documented strep throat within 3 mo
|
|
|
Q757. complications of strep throat
|
A757. post-strep GN; rheumatic heart disease; peritonsillar abscess
|
|
|
Q758. what bacteria can cause pharyngitis
|
A758. strep; diptheria; gonorrhea
|
|
|
Q759. most common pathogen for otitis externa
|
A759. staph
|
|
|
Q760. watchful waiting in AOM?
|
A760. if over the age of 6 mo, wait to see if it gets better in 2-3 days; otherwise, if 100% sure treat AOM
|
|
|
Q761. otitis media with effusion
|
A761. this is not AOM, this is just fluid behind tm
|
|
|
Q762. classic finding of als on muscle bx; clinical sx
|
A762. denervation and renervation; flaccid paralysis, foot drop, hand clumsiness, muscle wasting and fasciculations
|
|
|
Q763. pathology of guillan-barre
|
A763. ascending paralysis ==> demylenation of peripheral nerves
|
|
|
Q764. list the different types of incontinence
|
A764. stress incontinence; urge incontinence; overflow incontinence; functional incontinence; reflex incontinence
|
|
|
Q765. features of stress incontinence
|
A765. voiding of urine during laughing, sneezing, etc; caused by the urethra that gets pushed below the bladder so that when there is increased intraabdominal pressure, only the bladder gets squeezes, leading to leakage of urine
|
|
|
Q766. features of overflow incontinence
|
A766. incomplete voiding of bladder upon urination --> nocturia and frequent loss of small amounts of urine
|
|
|
Q767. features of urge incontinence
|
A767. involuntary detrusor contractions --> sudden urge to urinate, but can't make it to bathroom; loss of large volumes of urine
|
|
|
Q768. features of reflex incontinence
|
A768. usually associated w spinal cord injury... can't sense that you need to urinate
|
|
|
Q769. features of functional incontinence
|
A769. secondary to a disease
|
|
|
Q770. differential dx of lower back pain
|
A770. musculoligamentous back pain; herniated disc; degenerative disc disease; ankylosing spondylitis; spinal stenosis; malignancy; compression fracture; infection; cauda equina syndrome
|
|
|
111find me
|
uggg
|