Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
263 Cards in this Set
- Front
- Back
|
Describe the development of the vulva
|
|
|
|
What are the..... of the vulva:
a) cells (what are they rich in?) b) Blood supply c) lymphatic drainage d) innervation |
|
|
|
Describe the development of the vagina
|
|
|
|
What are the..... of the vagina:
a) cells (what are they rich in?) b) Blood supply c) lymphatic drainage |
|
|
|
Describe the development of the Cervix
What is the SCJ? |
|
|
|
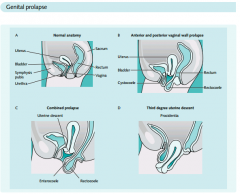
Uterine prolapse types
|
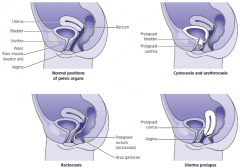
Uterine prolapse (grades i-iv)
Cystocele Rectocele Enterocele Urinary incontinence |
|
|
Cystocele
|
Postmenopausal woman
Anterior vaginal wall protrussion Urinary incontinence Diagnosis --> pelvic exam |
|
|
Rectocele
|
Postmenopausal woman
Posterior vaginal wall protrussion Digitally assisted removal of stool Diagnosis --> pelvic exam |
|
|
Medical management of pelvic relaxation
|
Used in minor relaxation
Kegel exercises --> voluntary contractions of pubococcygeus muscle Estrogen replacement --> in postmenopausal women Pessaries --> objects inserted into vagina to elevate pelvic structures |
|
|
Surgical management of pelvic relaxation
|
Used when medical management fails
Vaginal hysterectomy with anterior and posterior colporrhaphy (vaginal repair) |
|
|
Pharmacology of urinry incontincence
|
Alpha adrenergeic --> contract urethra; ephedrine, imipramine, estrogens; phenoxibenzamine is antagonist
Beta adrenergic --> relax detrusor muscle; flavoxate, progestins Cholinergic --> contract detrusor muscle; bethanecol, neostigmine; anticholinergics are oxybutynin, propantheline |
|
|
Cystometry
|
Urinary catheter empties bladder then infuses saline; measures -->
Residual volume --> normal 50ml Sensation of fullness --> normal 200-225ml Urge to void --> normal 400-500ml |
|
|
Sensory irritative incontinence
|
Involuntary detrusor contractions stimulated by irritation from infections, stones, tumor, foreign body
Presentation --> loss of urine with frequency, urgency and dysuria, suprapubic tenderness Diagnosis --> urinalysis and urine culture or cytoscopy; cystometry is usually unnecessary Management --> antibiotics for infections; cytoscopy for stones, foreing bodies and tumors |
|
|
Stress incontinence
|
From rises in intraabdominal pressure
Presentation --> involuntary loss of urine with coughing or sneezing, no urine loss at night Exam --> cystocele may be present and q-tip test is positive (rotates >30degrees) Studies --> urinalysis and culture are normal; cystometry is normal without detrusor contractions Management --> kegel or estrogen; urethropexy or tension-free vaginal tape |
|
|
Motor urge hypertonic incontinence
|
Idiopathic detrusor contractions that can't be suppressed volutarily
Presentation --> loss of urine, cannot suppress urge to void, day or night Tests --> urinalysis and culture are normal; residual volume is normal but there are involuntary detrussor contractions Management --> anticholinergics and nsaids |
|
|
Overflow hypotonic incontinence
|
Hypotonic bladder does not empty until theres excess pressure;
Etiology --> denervated bladder from diabetic neuropathy or multiple sclerosis, anticholinergics Presentation --> urine loss day and night with no detrussor contractions; decreased pudendal nerve sensation Tests --> urinalysis and culture normal or infection; markedly increased residual volume without detrussor contractions Management --> self-catheterization; cholinergics, alpha blockers |
|
|
Bypass fistula incontinence
|
Presentation --> history of radical pelvic or radiation surgery, continuous urine loss day and night
Diagnosis --> intravenous pyelogram shows dye leakage from urinary tract fistula Management --> surgical repair |
|
|
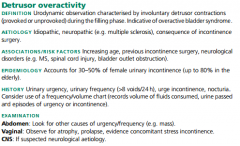
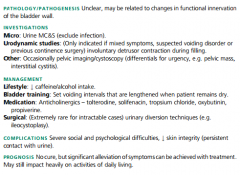
Detrusor Overactivity:
Def Aetiology Rf Epi Hx Ex |
|
|
|
Detrusor Overactivity:
Pathogenesis Ix Mx: Lifestyle, Rx and Surgery Complications Prognosis |
|
|
|
Vaginal discharge diagnostic tests
|
Speculum exam --> looking for inflammation and characteristics of discharge
Vaginal ph --> normal is <4.5; nitrazine paper turns yellow when normal or dark when high ph Koh slide --> two drops of vaginal discharge + saline + koh are analyzed on microscope |
|
|
Bacterial vaginosis
|
High ph replaces normal flora lacbacilli
Presentation and diagnosis --> fishy odor, no itching, ph>4.5, thin grayish discharge, whiff+ on koh, clue cells on wet mount Management --> metronidazole (safe in pregnancy) or clindamycin; orally or vaginally |
|
|
Trichomonas vaginitis
|
Std; protozoan resides in seminal fluid
Presentation and diagnosis -->itching, burning, pain with intercourse, green discharge, inflammation seen, erythematous cervix, ph>4.5, trichomonads and wbcs on saline Management --> oral metronidazole orally for patient and partner |
|
|
Candida yeast vaginitis
|
Presentation and diagnosis --> itching, burning, pain with intercourse, normal ph, white discharge, inflammation seen, pseudohyphae on koh
Management --> single oral dose of fluconazole or vaginal azole creams |
|
|
Physiologic discharge
|
Due to excess estrogen
Presentation and diagnosis --> watery vaginal discharge, no itching, no inflammation, normal ph, absence of pathogens on wet mount Management --> contraception with progestins |
|
|
Vaginal discharge with normal ph
|
Candida, physiologic discharge
|
|
|
Vaginal discharge with high ph
|
Bacterial vaginosis, trichomonas
|
|
|
Grayish discharge
|
Bacterial vaginosis
|
|
|
White discharge
|
Candida
|
|
|
Green discharge
|
Trichomonas
|
|
|
Watery discharge
|
Physiologic discharge
|
|
|
Differentail diagnosis of vulvar itching
|
Vulvar carcinoma
Stds Benign vulvar dystrophy Malignant cancer All lesions should have biopsy |
|
|
Vulvar dystrophy
|
Squamous hyperplasia --> whitish, firm, cartilaginous lesions with thick kertain and epithelial proliferation on microscope; management is fluorinated corticosteroid cream
Lichen sclerosis --> bluish-white papula that can coalesce into white plaques and show epithelial thinning; management is clobetasol cream |
|
|
Premalignant vulvar lesions
|
Squamous dysplasia --> white, red or pigmented multifocal lesions with epithelium atypia not reaching bm; management is surgical excision
Cis --> same presentation with more atypia but not reaching the bm; management is laser vaporization |
|
|
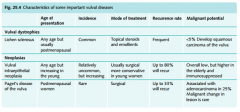
Give the...... for the 3 pre-malignant vulval diseases:
a) Age of presentation b) incidence c) Rx d) recurrence rate e) malignant potential |
|
|
|
Malignant vulvar lesions
|
Squamous cell carcinoma --> most common; associated with hpv
Melanoma --> 2nd most common; any dark or black lesion should be biopsied; prognosis related to depth of invasion Paget disease --> red vulvar lesion |
|
|
Management of malignant vulvar lesions
|
Radical vulvectomy with or without lymphadenectomy
|
|
|
Benign vulvar lesions
|
Molluscom contagiousum --> spontaneously regressing umbilicated tumors; observation, curettage, cryo
Condylomata acuminata --> hpv 6 & 11 cauliflower lesions Bartholin cyst --> aspiration yields sterile fluid |
|
|
Cervical polyps
|
Presentation --> vaginal bleeding and smooth red or purple fingerlike projections from cervical canal
Diagnosis --> biopsy shows mildly atypical cells Management --> twisting or surgical string for the polyp; electrocautery or laser for the base |
|
|
Nabothian cysts
|
Mucus-filled cyst on cervix surface
Presentation --> asymptomatic small white pimpli-likeelevation palpated or seen by colposcopy Management --> none necessary but can be removed by electrocautery or cryotherapy |
|
|
Cervicitis
|
Presentation --> mucopurulent cervical discharge without pelvic tenderness or fever
Diagnosis --> cervical culture shows chlamydia or gonorrhea Management --> oral azythromycin single dose or doxycycline 7 days |
|
|
Premalignant cervical lesions
|
Are asymptomatic and 15% can progress to cancer in 8-10 years
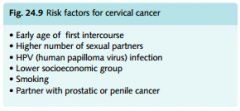
65% regress; 20% stay the same Due to hpv 16, 18, 30s Risk factors for hpv --> early age of intercourse, multiple partners, cigarette smoking, immunosuppression |
|
|
What is a pap smear
|
Exfoliative cytology
Best screening test for premalignant lesions One specimen from t-zone and one from endocervix Conventional method --> samples are smeared and fixated onto slide Liquid-based method --> samples are rinsed into a solution |
|
|
Pap smear screening
|
Start 3 years after onset of sexual intercourse or at age 21
Discontinue at age 70 after >3 consecutive negative tests If under age 30 --> screen annually with conventional or every 2 years with liquid-based If over 30 --> screen every 2-3 years if >3 negative pap smears |
|
|
Pap smear classification
|
Negative
Asc --> atypical squamous cells; undertermined significance or cannot exclude hsil Lsil --> low-grade squamous intraepithelial lesion; biopsy shows hpv, mild dysplasia or cin 1 Hsil --> high-grade squamous intraepithelial lesion; biopsy shows moderate-severe dysplasia or cin 2-3 Cancer --> biopsy will show invasive cancer |
|
|
Ascus pap smear
|
Results from inflammatory or atrophic lesions or the initial stages of hpv infection
10-15% of ascus paps can have a significant premalignant lesion Management --> repeat cytology in 3-6 months and hpv dna testing (reliable patients) or colposcopy+biopsy (unreliable patients) If high risk hpv dna test --> colposcopy+biopsy |
|
|
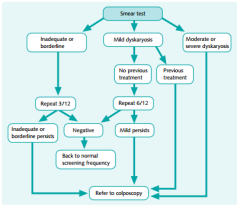
Smear test action protocol for:
a) Inadequate/borderline smear b) Mild dyskaryosis c) Mod-Severe dyskaryosis |
|
|
|
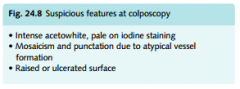
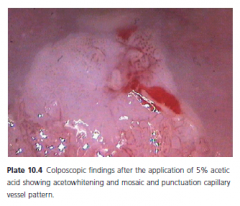
Suspicious colposcopy findings (3)
|
|
|
|
Colposcopy
|

Performed if there's high risk results from hpv dna test
Satisfactory or adequate --> entire t-zone is visualized and no lesions dissapear into endocervix Unsatisfactory or inadequate --> entire t-zone cant be visualized Colposcopy includes endocervical curettage and ectocervical biopsy |
|
|
Cone biopsy
|
Indications:
Pap smear is worst than colposcopy biopsy Abnormal endocervical curettage Lesion in endocervical canal Biopsy shows microinvasive carcinoma |
|
|
Cervical dysplasia management according to histology
|
Cin 1 --> repeat pap in 6-12 months or colposcopy+pap in 12 months or hpv dna in 12 months
Cin 1, 2, 3 --> ablation with cryotherapy, laser or electrofulguration Cin 1, 2, 3 --> excision by leep or cold-knife conization Biopsy confirmed recurrent cin 2 or 3 --> hysterectomy All ablations or excisions require repeat pap, colposcopy, hpv dna every 4-6 months for 2 years |
|
|
Rf for cervical Ca
|
|
|
|
Invasive cervical cancer presentation and diagnosis
|
Postcoital vaginal bleeding, irregular vaginal bleeding, lower extremity pain and edema
Cervical biopsy --> initial diagnostic test Metastatic workup --> do if biopsy is positive; pelvic exam, chest x-ray, iv pyelogram, cystoscopy, sigmoidoscopy Ct or mri are not used for staging |
|
|
Invasive cervical cancer management
|
Stage ia1 --> <=3mm, simple hysterectomy
Stage ia2 --> 3-5mm, modified radical hysterectomy Stage ib --> radical hysterectomy Stages ii-iv --> radio and chemo Follow-up --> pap every 3months for 2 years; then every 6 months for 3 years |
|
|
Cervical neoplasia in pregnancy
|
All abnormal pap smears should be followed by colposcopy+biopsy
No ecc is performed |
|
|
Cervical neoplasia in pregnancy management
|
Cin --> follow with pap+colposcopy evrery 3 months during pregnancy; treat postpartum
Microinvasion --> do cone biopsy; if confirmed, then treat postpartum Invasive cancer --> if diagnosis before 24 weeks then radical hysterectomy or radio; if after 24 weeks then cesarean at 32-33 weeks + definitive treatment |
|
|
Hpv vaccine
|
Quadrivalent for types 6, 11, 16, 18 (70% of cancers and 90% of warts)
Uses noninfectious particles Recommended to all women 8-26 with target age 11-12 Do not test for hpv before vaccine Continue regular paps Not recommended for pregnant, lactating or immunosuppressed |
|
|
Mullerian anomalies
|
Hypoplasia/agenesis
Unicornuate uterus Didelphys uterus Bicornuate uterus Septate uterus Arcuate uterus Des uterus |
|
|
Uterine hypoplasia/agenesis
|
May lack vagina or any part of uterus except fundus
Associated with urinary tract anomalies |
|
|
Unicornuate uterus
|
One mullerian duct does not develop or develops incompletely
The incompletely developed half uterus lacks a cavity connecting to vagina which leads to pain during menses in teenagers May have pregnancy in the bad uterus but 90% of them rupture |
|
|
Didelphys uterus
|
Double uterus from failure of mullerians to fuse
May have a single or two cervix or vaginas |
|
|
Bicornuate uterus
|
Most common
Failure of mullerians to fuse at the top results in two horns sharing a cervix or two bodies sharing a cervix |
|
|
Septate uterus
|
Mullerians fused but theres no degeneration of median septum
External shape appears normal |
|
|
Arcuate uterus
|
Small midline indentation at the fundus
Does not have negative effects on pregnancy |
|
|
Des uterus
|
Daughters of mothers exposed to des during pregnancy
May have hypoplastic uterus, t-shaped cavity and/or cervical defects |
|
|
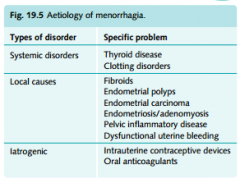
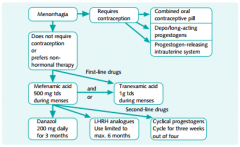
Aetiology of menorrhagia
|
|
|
|
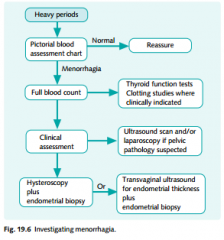
Algorythm for menorrhagia
|
|
|
|
Treatment protocol for menorrhagia
|
|
|
|
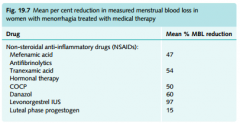
Medical Rx for menorrhagia
with Mean % MBL reduction |
|
|
|
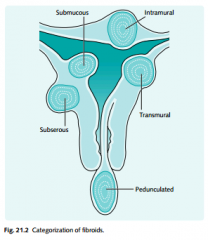
Leiomyoma presentation
|
Most common benign uterine tumor; outgrowth of the myometrium
Intramural --> most common location within the wall of the uterus Submucosal --> beneath endometrium and can distort uterine cavity; can have meno/metro or menometrorrhagia Subserosal --> beneath the serosa and can distort the external contour and pressure the bladder, rectum or ureters |
|
|
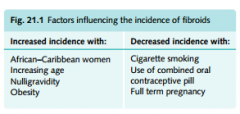
Rf for fibroids
|
|
|
|
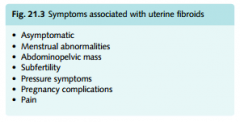
Fibroids Sc
|
|
|
|
Location of fibroids
|
|
|
|
Leiomyoma natural history
|
Slow growth --> small, grow slowly and cause no symptoms except if they are massive
Rapid growth --> estrogen receptors are increased and result in rapid growth specially during pregnancy Degeneration --> the size is more than blood supply resulting in ischemic with acute pain requiring hospitalization and narcotics Shrinkage --> when estrogen levels fall the leiomyoma shrinks |
|
|
Fibroids:
Hx Ex Pathogenesis |
|
|
|
Fibroids:
Mx: Rx and Surgery Complications Prognosis |
|
|
|
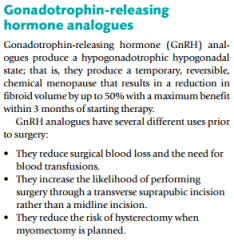
Mechanism of GnRH antagonists
|
|
|
|
Leiomyoma diagnosis
|
Pelvic exam --> enlarged asymetric, nontender uterus in absence of pregnancy
Sonography --> traditional for intramural or subserosal or with saline infusion for submucosal Hysteroscopy --> for submucosal myomas Confirmation of diagnosis is made by histologic exam of excised tissue |
|
|
Leiomyoma management
|
Observation --> most can be managed conservatively
Presurgical shrinkage --> leuprolide for 3-6 months results in 60-70% shrinkage Myomectomy --> done to conserve fertility; subsequent pregnancies should be delivered by cesarean Embolization --> catheter injects microspheres which cause ischemia and necrosis of myoma Hysterectomy --> if patient has completed childbearing |
|
|
Adenomyosis presentation
|
Ectopic endoemtrial glands in myometrium
Presents with secondary dysmenorrhea or menorrhagia, symmetrical diffuse uterine enlargement and tenderness during menses |
|
|
Adenomyosis diagnosis
|
Mostly made clinically
Ultrasound or mri shows diffusely enlarged uterus with cystic areas in myometrium Confirmation is by histology |
|
|
Ademyosis management
|
Medical --> levonorgestrel intrauterine system decreases menstrual bleeding
Hysterectomy --> definitive treatment |
|
|
Differential diagnosis for enlarged non-pregnant uterus
|
Leiomyoma --> asymmetric, firm, nontender
Adenomyosis --> symmetric, soft, tender |
|
|
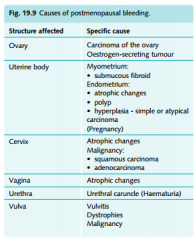
Differential diagnosis of postmenopausal bleeding
|
Endometrial carcinoma (most important), vaginal or endometrial atrophy (most common), postmenopausal hormone replacement
|
|
|
Causes of PMB
|
|
|
|
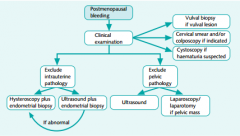
PMB Diagnostic protocol
|
|
|
|
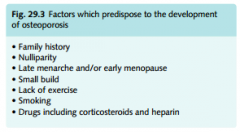
Endometrial cancer risk factors
|
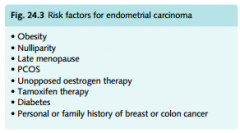
Unoppossed estrogen occurs in
Obesity Hypertension Diabetes Nulliparity Late manopause Chronic anovulation (polycystic ovarian disease) |
|
|
Endometrial cancer diagnosis
|
Endometrial sampling
D&c if cervical stenosis is present Hysteroscopy --> rules out cervical or endometrial polyps Ultrasound --> endometrial lining should measure <5mm thick in postmanopause |
|
|
Endometrial cancer management
|
If negative histology from sampling --> diagnosis is atrophy treated with estrogen/progesterone replacement
If positive histology from sampling --> adenocarcinoma is treated with total abdominal hysterectomy with bilateral salpingo-oophorectomy and pelvic/para-aortic lymphadenectomy; it may also require radio and chemo postoperative |
|
|
Endometrail hyperplasia
|
May cause bleeding; cells have no atypia; treat with progestin
|
|
|
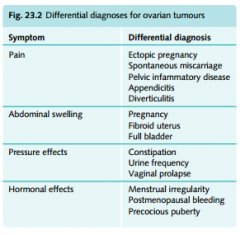
Ovarian cyst differential diagnosis
|
Pregnancy (most common)
Complex masses --> Dermoid cyst Benign cystic hematoma Endometrioma Tubo-ovarian abscess Ovarian cancer |
|
|
Ovarian cyst presentation and diagnosis
|
Pelvic mass in reproductive years
Negative betahcg (rules out pregnancy) Sonogram shows fluid-filled ovarian simple cyst |
|
|
Ovarian cyst management
|
Follow-up exam in 6-8 weeks for resolution
Alert patient of possibility of acute onset pain from torsion If >7cm or prior steroid contraception --> laparoscopy |
|
|
Ovarian hyperthecosis pathophysiology
|
Nests of active luteinized cells in ovarian stroma; peripheral estrogen is increased which leads to excess androgen production by ovaries; risk of endometrial hyperplasia and carcinoma are increased due to high estrogens
|
|
|
Ovarian thecosis presentation
|
Obesity
Less severe hirsutism than pcos Virilization (clitoral enlargement, balding, deep voice, male habitus) Amenorrhea or irregular/anovulatory cycles Can occur in postmenapause unlike pcos |
|
|
Ovarian hyperthecosis management
|
Oral contraception suppresses androgen production and free androgens
|
|
|
Luteoma of pregnancy
|
Non-neoplastic tumor-like mass that regresses spontaneously
Asymptomatic Found incidentally Hormonally active and can produce maternal and fetal hirsutism and virilization |
|
|
Theca lutein cysts
|
Benign neoplasm caused by excess fsh and beta-hcg
Associated with twins and molar pregnancies Regresses spontaneously |
|
|
Prepubertal pelvic mass presentation and work-up
|
Presents with sudden onset of acute abdominal pain in prepubertal female
Serum tumor markers for germ cell tumors: Ldh --> dysgerminoma Beta-hcg --> chroriocarcinoma Alpha-fetoprotein --> endodermal sinus tumor |
|
|
Prepubertal pelvic mass diagnosis and management
|
If simple cyst --> diagnose with laparoscopy
If complex mass --> diagnose with laparotomy If benign --> cystectomy+annual follow-up (pelvic exam+tumor markers) If malignant --> unilateral s&o, staging and chemo |
|
|
Premenopausal complex mass
|
Most common is dermoid cyst (benign cystic teratoma)
Also endometrioma, tubo-ovarian abscess, ovarian cancer B-hcg rules out pregnancy; ultrasound rules out simple mass (ovarian cyst) Manage with cystectomy or oophorectomy |
|
|
Benign cystic teratoma
|
Complex mass with calcifications on ultrasound
|
|
|
Ovarian torsion
|
Presumptive diagnosis --> abrupt unilateral pelvic pain, b-hcg-, adnexal mass on ultrasound
Management --> untwist ovary; if revitalization then cystectomy; if necrosis then oophorectomy |
|
|
Ovarian cancer presentation
|
Postmenopausal adnexal mass
|
|
|
Ovarian cancer risk factors
|
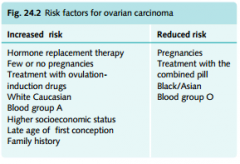
Brca1 gene
Positive family history High number of lifetime ovulations Perineal talc powder Protective factors --> oral contraceptives, chronic anovulation, brest feeding, short reproductive life |
|
|
Ovarian cancer diagnosis
|
Screening --> bimanual pelvic examination (large, solid, irregular, fixed)
Tumor markers --> cea, ca-125, ldh, afp, hcg, testosterone Abdominal pelvic ct or pelvic ultrasound Barium enema to rule out diverticulosis Iv pyelogram for urinary tract lesions |
|
|
Types of ovarian tumors
|
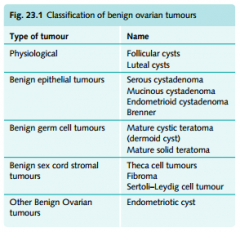
Epithelial --> older women; ovarian cancers (serous, mucinous, brenner, endometrioid, clear cell)
Germ cell --> younger women; dysgerminoma, endodermal, teratoma, choriocarcinoma Stromal --> granulosa-theca cells, sertoli-leydig cell Metastatic --> from other primary sites (endometrium, gi, breast, krukenberg) |
|
|
DDx for ovarian tumours
|
|
|
|
Serous ovarian carcinoma
|
Postmenopausal woman, pelvic mass, high cea or ca-125
|
|
|
Choriocarcinoma
|
Postmenopausal woman, pelvic mass, high hcg
|
|
|
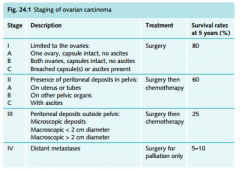
Staging ovarian Ca
|
|
|
|
Sertoli-leydig tumor
|
Postmenopausal pelvic mass, masculinization, high testosterone
|
|
|
Endometrial carcinoma metastatic to ovaries
|
Postmenopausal woman with bilateral pelvic masses
Postmenopausal bleeding Enlarged uterus |
|
|
Cea or ca-125
|
Serous ovarian cancer
|
|
|
Hcg as tumor marker
|
Choriocarcinoma (ovarian germ cell tumor)
|
|
|
Testosterone as tumor marker
|
Sertoli-leydig cell ovarian stromal tumor
|
|
|
Ldh as tumor marker
|
Dysgerminoma
|
|
|
Afp as tumor marker
|
Endodermal sinus germ cell tumor (ovary)
|
|
|
Ovarian cancer management
|
Laparotomy or laparoscopy with unilateral salpingo oophorectomy with histology during surgery
If benign --> uso is enough or tah+bso If malignant --> tah+bso, omentectomy and bowel ressection if necessary + postop chemo |
|
|
Benign gestational neoplasia types
|
Hydatiform mole
Complete --> empty egg, paternal x, 46xx, fetus absent, grape-like vesicles Incomplete --> normal egg, maternal and paternal x, 69xxy, fetus nonviable |
|
|
Malignant gestational neoplasia types
|
Nonmetastatic --> uterus only, 100%cure
Good prognosis --> metastasis to pelvis or lung, 95% cure, single agent chemo Poor prognosis --> metastasis to brain or liver, 65% cure, combo chemo |
|
|
Gestational trophoblastic neoplasia presentation
|
Bleeding prior to 16 weeks
Passage of vesicles Hypertension Proteinuria No fetal heart tones Hyperthyroidism Fundus larger than dates |
|
|
Gestational trophoblastic neoplasia diagnosis
|
Snowstorm ultrasound shows homogenous intrauterine echoes without sac or fetus
|
|
|
Gestational trophoblastic neoplasia management
|
1) baseline beta-hcg
2) chest x-ray to rule out lung metastasis 3) suction d&c 4) oral contraceptives during follow-up If benign --> weekly b-hcg until negative for 3 consecutive weeks, then monthly until negative for 12 months If b-hcg does not lower --> brain, thorax, abdominal and pelvic cts for metastasis If good prognosis metastatic --> single agent chemo + 1 year follow-up If poor prognosis metastatic --> multiple chemo + weekly b-hcg then monthly then every three months (5 years) |
|
|
Cercivitis
|
Presentation --> mucopurulent cervical discharge, without pelvic tenderness or fever
Diagnosis --> nucleic acid amplification tests of cervical discharge or urine; normal wbcs and esr Management --> single oral dose of cefixime and azithromycin |
|
|
Acute salpingo-oophoritis presentation and diagnosis
|
Bilateral lower abdominal/pelvic pain
Mucopurulent cervical discharge Cervical motion tenderness High wbcs and esr |
|
|
Acute salpingo-oophoritis management
|
Certain diagnosis and no evidence of systemic infection or absecess --> ofloxacin+metronidazole 14 days
Uncertain diagnosis, nulligravida, evidence of abscess or fever --> inpatient, iv cefoxitin or cefotetan + iv doxy |
|
|
Lower abdominal-pelvic pain differential diagnosis
|
Acute salpingo-oophoritis
Adnexal torsion Ectopic pregnancy Appendicitis Endometriosis Diverticulitis Crohn Ulcerative colitis |
|
|
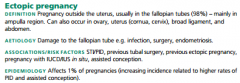
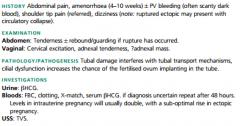
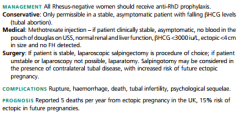
Ectopic Pregnancy
Def Aetiology Rf Epi |
|
|
|
Ectopic Pregnancy:
Hx Ex Pathogenesis Ix |
|
|
|
Tubo-ovarian abscess presentation
|
Sepsis (tachycardia, hypotension, high fever)
Severe lower abodominal-pelvic pain Peritoneal guarding and rigidity Nausea, vomit Adnexal masses may be palpated |
|
|
Ectopic Pregnancy:
Mx Complications Prognosis |
|
|
|
Tubo-ovarian abscess diagnosis
|
Positive cervical cultures for chlamydia or gonorrhea
Positive blood cultures for gram- Pus on culdocentesis High wbcs and esr Sonogram or ct show bilateral complex masses |
|
|
Differential diagnosis of sepsis+lower abdominal-pelvic pain
|
Tubo-ovarian abscess
Septic abortion Diverticular abscess Appendiceal abscess Adnexal torsion |
|
|
Tubo-ovarian abscess management
|
Iv clindamycin and gentamicin
If no change in 72 hours or abscess rupture --> laparotomy and consider tah+bso |
|
|
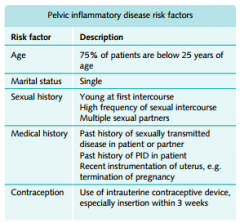
PID Rf
|
|
|
|
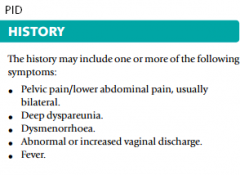
PID Hx
|
|
|
|
PID causative organisms
|

|
|
|
Chronic pid
|
Chronic bilateral abdominal/pelvic pain
No cervical discharge Cervical motion tenderness Negative cultures Normal wbcs and esr Sonography may show bilateral cystic pelvic masses Diagnosis --> laparoscopic visualization of pelvic adhesions Management --> lysis of tubal adhesions or if unremitting tah+bso |
|
|
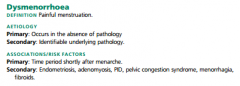
Primary dysmenorrhea vs. Secondary dysmenorrhea
|
Primary --> teenagers, absence of pelvic pathology
Secondary --> mature women, presence of pelvic pathology (endometriosis, adenomyosis) |
|
|
Primary dysmenorrhea
|
Recurrent lower abdominal pain during menstrual periods in a teenager with absence of pelvic pathology
Due to excess prostaglandin f2 Treat with nsaids (first line) or oral contraception (2nd line) |
|
|
Dysmennorrhoea:
Def Aetiology Rf |
|
|
|
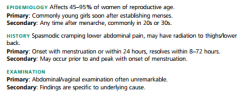
Dysmennorrhoea:
Epi Hx Ex |
|
|
|
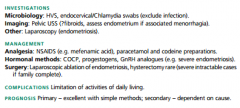
Dysmenorrhoea:
Ix Mx Complications Prognosis |
|
|
|
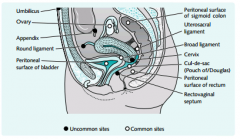
Endometriosis presentation and diagnosis
|
Pelvic-abdominal pain
Dyspareunia Painful bowel movements Infertility Exam --> cul-de-sac adhesions, uterosacral ligament nodularities, enlarged adnexa Lab --> normal wbcs and esr, ca-125 may be elevated Diagnosis --> laparoscopy |
|
|
113 Define Emdometriosis
|
|
|
|
Commonest sites for endometriosis
|
|
|
|
Clinical evaluation and classical quartet of Sx
|
|
|
|
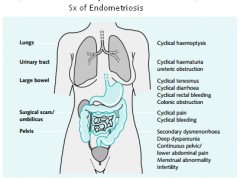
Sx of endometriosis
|
|
|
|
DDx of endometriosis
|
|
|
|
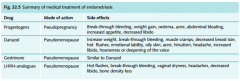
Medical Rx for endometriosis
|
|
|
|
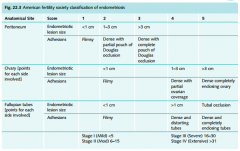
Classification of endometriosis
|
|
|
|
Endometriosis management
|
Medical --> leuprolide (doc), medroxyprogesterone, testosterone derivative
Surgical --> laparoscopic lysis of tubal adhesions, cystectomies, laser vaporization or tah+bso |
|
|
Chancroid
|
Painful ulcer with ragged edges due to haemophilus ducreyi
Confirm diagnosis with culture Treat with single dose azithromycin, single dose im ceftriaxone or erythromycin 7 days |
|
|
Lymphogranuloma venereum
|
Due to chlamydia trachomatis
Painless vesiculopustular vaginal eruption that spontaneously heals Can have perirectal adenopathy, absecesses and fistulas within weeks Diagnosis --> postitive culture from pus aspirated from lymph node Management --> doxycylcline or erythromycin for 3 weeks |
|
|
Granuloma inguinale
|
Due to calymmatobacterium granulomatis
Painless ulcer with granulation tissue and no lymphadenopathy Diagnosis --> microscopicexam shows donovan bodies Management --> doxycycline or tmp-smx 3 weeks |
|
|
Condyloma acuminatum
|
Hpv 6, 11
Generally asymptomatic but clinical lesions in 30% Pedunculated, soft papule turns into cauliflower lesion Management --> small lesions are treated topically with podophyllin, trichloroacetic acid; larger lesions with cryo, laser or surgical excision |
|
|
Mucopurulent discharge
|
Chlamydia trachomatis (cervical), gonorrhea (cervical and vulvovaginal)
|
|
|
Stds with ulcers
|
Chancroid (painful, ragged)
Granuloma inguinale Genital herpes (painful, smooth) Lymphogranuloma venerreum Syphilis |
|
|
Stds without ulcers
|
Chlamydia
Hpv Gonorrhea Hbv Hiv |
|
|
Ragged soft edge inflamed painful vaginal ulcer
|
Chancroid
|
|
|
Groove sign
|
Lymphogranuloma venereum
|
|
|
Beefy red painless vaginal ulcer
|
Granuloma inguinale
|
|
|
Rolled, hard edges, painless vaginal ulcer
|
Syphilis
|
|
|
Smooth edge inflamed painful vaginal ulcer
|
Herpes
|
|
|
Gonorrhea
|
Vulvovaginal and cervical mucopurulent discharge
If cervicitis or pid --> pelvic pain, cervical motion tenderness, etc… If disseminated --> petechial skin lesions, septic arthritis Management --> single dose cefixime + single dose azithromycin |
|
|
Oestrogen-mediated effects of oral contraception
|
Fluid retention
Accelerated cholelithiasis Increased hepatic proteins Healthy lipid profile changes |
|
|
Progestin-mediated effects of oral contraception
|
Mood changes and depression
Androgenic --> weight gain, acne Unhealthy lipid profile changes |
|
|
Absolute contraindications of oral contraception
|
Pregnancy
Acute liver disease History of vascular disease (dvt, cva, sle) Hormonally-dependant breast cancer Smoker >35y/o Uncontrolled hypertension Migraines with aura Diabetes Known thrombophilia |
|
|
Relative contraindications of oral contraceptives
|
Migraines
Depression Diabetes Chronic hypertension Hyperlipidemia |
|
|
Premanarchal vaginal bleeding differential diagnosis
|
Foreign body (mcc)
Ingestion of estrogens Cancer of vagina or cervix Pituitary or adrenal tumor Ovarian tumor Sexual abuse Idiopathic precocious puberty |
|
|
Premenarchal vaginal bleeding diagnosis
|
Pelvic exam under sedation for foreign bodies, sexual abuse or tumors
Ct or mri of pituitary, abdomen and pelvis for tumors |
|
|
Abnormal vaginal bleeding diagnosis and management
|
1) rule out pregnancy or complications of pregnancy --> incomplete abortion, threatened abortion, ectopic pregnancy, mole
Diagnosis --> b-hcg + sonogram 2) rule out anatomic lesions --> vaginal lacerations, cervical polyps, cervicitis, leiomyomas, uterine hyperplasia, adenomyosis Diagnosis --> pelvic exam, saline sonogram, endometrial sampling, hysteroscopy 3) rule out dysfunctional uterine bleeding --> anovulation (hypothyroidism, hyperprolactinemia) Diagnosis --> history of irregular unpredictable menstrual bleeding without cramps; clear thin watery cervical mucus; no midcycle temperature rise; endometrial biopsy shows proliferative endometrium |
|
|
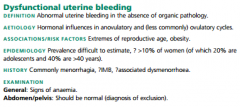
DUB:
Def Aetiology Rf Epi Hx Ex |
|
|
|
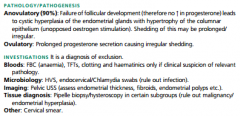
DUB:
Pathogenesis Ix |
|
|
|
DUB:
Mx Complications Prognosis |
|
|
|
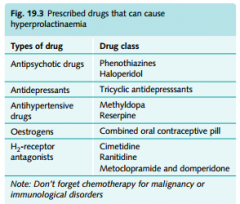
What drugs can cause hyperprolactinaemia?
|
|
|
|
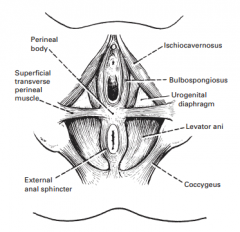
What muscles form the pelvic floor? (8)
|
|
|
|
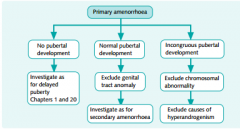
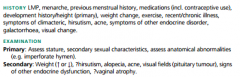
Primary amenorrhea definition and diagnosis
|
Absence of menses at age 14 without 2dary sexual characteristics or
Absence of menses at age 16 with secondary sexual characteristics |
|
|
Algorythm for Primary Amenorrhoea
|
|
|
|
Primary amenorrhea, breasts+, uterus-
|
Mullerian agenesis --> 46xx, create a vagina
Androgen insensitivity --> 46xy but looks female, absent pubic hair, high testosterone; give estrogen, create vagina and remove testes |
|
|
Primary amenorrhea, breasts-, uterus+
|
Gonadal dysgenesis --> turner, high fsh, no follicles, streak ovaries
Hp axis failure --> low fsh, normal ovaries, diagnose with brain scan Kallman --> +anosmia |
|
|
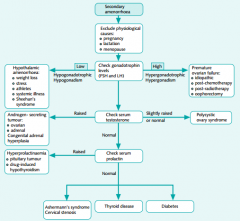
Algorythm for Secondary Amenorrhoea
|
|
|
|
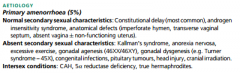
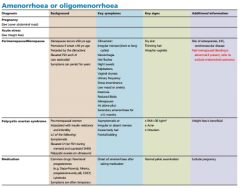
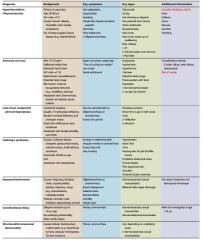
Give top 5 causes of amenorrhoea/oligiomenorrhoea with Sx and signs
|
|
|
|
Give the other causes of amenorrhoea/oligiomenorrhoea with Sx and signs (7)
|
|
|
|
Secondary amenorrhea diagnosis
|
Absence of menses for 3 months if previously regular
Absence of menses for 6 months if previously irregular |
|
|
First step in evaluation of secondary amenorrhea
|
B-hcg to rule out pregnancy
|
|
|
Etiology of secondary amenorrhea
|
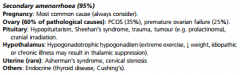
Anovulation --> pcos, hypothyroidism, pituitary adenoma, hyperprolactinemia, antipsychotics, antidepressants
Hypoestrogenic --> absence of functional ovarian folliclles, hp insufficiency Outflow tract obstruction |
|
|
Secondary amenorrhea work-up
|
1) b-hcg; if negative -->
2) tsh (primary hypothyroidism causes high trh and hyperprolactinemia); if negative --> 3) prolactin (antipsychotics or pituitary tumor); do mri tu rule out adenoma; if negative --> 4) progesterone challenge test; if positive then anovulation; if negative then inadequate estrogen --> 5) estrogen-progesterone challenge test; If positive --> inadequeate estrogen; if high fsh then ovarian failure; if low fsh then hp insufficiency If negative --> outflow tract obstruction or endometrial scarring; order hysterosalpingogram |
|
|
Secondary Amenorrhoea Complications
|

|
|
|
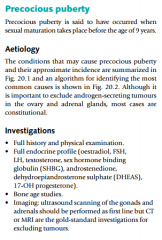
Definition, Aetiology & Ix for precocious puberty
|
|
|
|
Idiopathic/constitutional precocious puberty
|
Too much gonadotropins
All puberty changes are seen 6y/o girl Normal mri Treat with leuprolide to avoid premature closure of epiphysis |
|
|
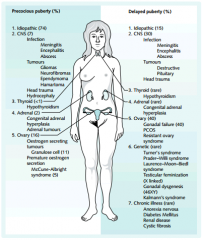
Causes of:
a. Precocious Puberty (5 classes 18 causes) b. Delayed Puberty (7 classes 24 causes) |
|
|
|
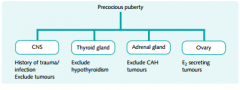
Diagnostic protocol for precocious puberty
|
|
|
|
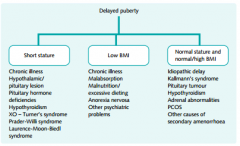
Diagnostic protocol for Delayed Puberty
|
|
|
|
Mccune-albright syndrome
|
Autonomous aromatase activation with excess estrogen
Complete precocious puberty 6 y/o Cafã© au lait spots Multiple cystic bone lesions Management --> aromatase enzyme inhibitor |
|
|
Granulosa cell tumor
|
Precocious complete puberty
6 y/o girl Pelvic mass Management --> surgery |
|
|
Premenstrual syndrome (pms) diagnosis
|
Based on diary of symptoms throughout 3 menstrual cycles; must meet all criteria -->
Recurrent in at least 3 consecutive cycles Absent in preovulatory phase Present in the 2 postovulatory weeks Intereferes with normal functioning Resolves with onset of menses |
|
|
Premenstrual syndrome management
|
Yaz (drospirenone/estradiol)(low-dose combo ocp, 4-day hormone free)
Drospirinon (drsp)(spironolactone analogue with antimineralocortocoid effects) Ssris (for emotional symptoms) Alprazolam (for emotional symptoms) Gnrh agonists |
|
|
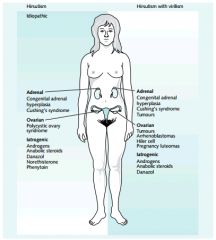
Hirsutism due to adrenal tumor
|
Rapid onset virilization
Abdominal/flank mass on ct or mri Markedly elevated dheas Remove surgically |
|
|
Hirsutism definition
|
Excessive male-pattern hair growth with or without virilization (clitorimegaly, baldness, deep voice, increased muscle)
|
|
|
Differential diagnosis for:
a) hirsutism b) hirsuitism with virilisation |
|
|
|
Differential diagnosis of hirsutism
|
21-hydroxylase deficiency
Stromal ovarian tumor Pcos Idiopathic (mcc) Adrenal tumor |
|
|
Hirsutism work-up
|
Sudden onset --> testosterone and dheas levels, pelvic exam, abdominal ct or mri, pelvic ultrasound
Gradual onset --> serum 17oh progesterone levels, testosterone, pelvic ultrasound (pcos) |
|
|
Hirsutism due to sertoli-leydig tumor
|
Rapid onset virilization
Adnexal pelvic mass on exam and ultrasound Markedly elevated testosterone Remove surgically |
|
|
Hirsutism due to congenital adrenal hyperplasia
|
21-hydroxylase deficiency
Gradual onset hirsutism without virilization Normal exam Markedly increased 17oh progesterone Treat with corticosteroid replacement |
|
|
Idiopathic hirsutism
|
Due to 5-alpha reductase overactivity
Gradual onset hirsutism Normal dheas, 17-oh progesterone and testosterone Treat with spironolactone or eflornithine |
|
|
Polycystic ovarian syndrome presentation
|
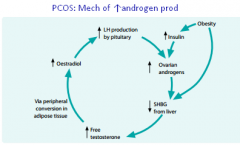
Irregular menstrual bleeding (from anovulation/unopposed estrogen; gonadotropins arent pulsatile)
Hirsutism (increased lh stimulates androgens which also decrease shbg) Obesity Infertility Ovarian enlargement with multiple cysts |
|
|
Polycystic ovarian syndrome diagnosis
|
2/3 oligo/ammenorrhoea, polycystic ovaries and biochem/clinical signs of hyperandrogenism.
Suspected with --> irregular menstrual bleeding, obesity, hirsutism, infertility Confirmed with --> lh/fsh ratio 3:1 (normal is 1.5:1) |
|
|
Mechanism for androgen production in PCOS
|
|
|
|
Polycystic ovarian syndrome management
|
Ocps (normalize bleeding and suppress lh)
Spironolactone (suppresses 5-alpha reductase) If pregnancy is desired --> clomiphene |
|
|
Semen analysis for infertility
|
Normal values:
Volume >2ml Ph 7.2-7.8 Sperm density >20million/ml Motility >50% Morphology >50% normal If sperm density is low --> intrauterine insemination If severely abnormal --> intracytoplasmic sperm injection or in-vitro fertilization |
|
|
Causes of infertility
|
Primary hypothyroidism
Hyperprolactinemia Pcos Pituitary adenoma Antipsychotics Ph insufficiency Ovarian insufficiency Semen abnormalities Pid |
|
|
Infertility work-up
|
1) initial step is semen analysis
2) rule out anovulation with history, progesterone levels, endometrial biopsy and temperature chart 3) if semen is normal and anovulation is ruled out --> hysterosalpingogram If positive --> attempt laparoscopic correction or in-vitro fertilization If negative --> unexplained infertility; spontaneous pregnancy occurs in 60% at 3 years or treat with clomiphene+intrauterine insemination |
|
|
Premature ovarian failure
|
Hot flashes and sweats
>30 y/o High fsh |
|
|
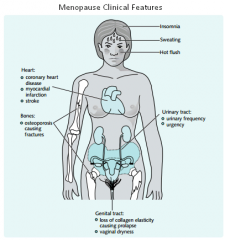
Menopause presentation and diagnosis
|
Presentation --> amenorrhea, hot flashes, cardiovascular disease, osteoporosis
Diagnosis --> 3 months of amenorrhea with elevation of gonadotropins |
|
|
Sx of Menopause
|
|
|
|
Immediate Sx of Menopause
|
|
|
|
Osteoporosis presentation and diagnosis
|
Vertebral crush fractures, hip and wrist fractures
Diagnosis --> dual-energy x-ray absoprtiometry (dexa scan) |
|
|
Osteoporosis Rf
|
|
|
|
Osteoporosis management
|
Lifestyle changes --> ca+ and vitamin d, weight-bearing exercise, stop cigarettes and alcohol
Medications --> biphosphonates and/or serms (raloxifene) |
|
|
Risks of hormone replacement therapy
|
Estrogen+progestin --> breast cancer, heart disease, stroke
Estrogen alone --> risk of stroke; no change in risk of breast cancer or heart disease Both groups --> dvt |
|
|
Benefits of hormone replacement therapy
|
Improves -->
Vaginal dryness Hot flashes Vasomotor symptoms Osteoporois |
|
|
Indications of hormone replacement therapy
|
Only indication is vasomotor symptoms
If only need to treat osteoporosis consider serms |
|
|
CI of HRT
|
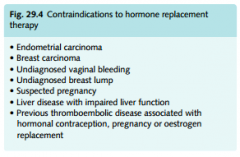
uncontrolled HTN
|
|
|
Cystic breast mass diagnosis and management
|
Diagnosis --> cyst aspiration and fine-needle aspiration with pathology exam
Management --> preaspiration mammography then aspiration; if benign, no further work-up |
|
|
Fibrocystic breast change presentation
|
Bilateral breast enlargement which fluctuates with menstrual periods (cyclic mentrual mastalgia)
May have palpable painful nodules |
|
|
Fibrocystic breast change diagnosis and management
|
Aspiration and complete drainage
Mass dissapears and fluid is clear --> discard fluid; reexamine in 4-6 weeks Mass dissapears and fluid is bloody --> send for cytologic exam; reexamine in 4-6 weeks Mass persists after aspiration --> wait 2 weeks after aspiration then mammography + excisional biopsy |
|
|
Fibroadenoma presentation
|
Most common in adolescents and young women
Discrete, smoothly contoured, rubbery, nontender, movable mass |
|
|
Fibroadenoma diagnosis and management
|
Diagnose with ultrasound or fine needle aspiration showing a solid mass that does not collapse after aspiration
Treat conservatively or elective excisional biopsy |
|
|
Mammographic calcifications
|
Nonpalpable; most are benign but 15-20% are early cancer; requires steoretactic needle localization and biopsy under mammographic guidance; treatment depends on histology
|
|
|
Indications of excisional biopsy of the breast
|
Cellular bloody cyst on fluid aspiration
Failure of a suspicious mass to dissapear completely upon aspiration Bloody nipple discharge with or without palpable mass Skin edema and erythema and needle biopsy cannot be performed |
|
|
Bloody nipple discharge
|
Requires excisional needle biopsy
Usually results from intraductal papilloma Management based on histology |
|
|
Breast cancer management
|
Determine prognostic factors
Stages i and ii do breast-conserving therapy with wide excision + axillary node dissection or sentinel node biopsy + radiotherapy |
|
|
Breast cancer prognostic factors
|
Lymph node status --> most important; inversely proportional to survival
Tumor size --> correlates with lymph node involvment but 15% of small tumors have positive node involvement Receptor status --> estrogen and progesterone receptor status is needed before surgical therapy; it's prognostic and predictive factor Dna ploidy --> determines diploid or aneuploidy (worse); it's unclear wether this is an independent risk factor |
|
|
Infiltrating ductal carcinoma
|
80% of breast cancers
Starts as atypical ductal hyperplasia --> ductal carcinoma in situ --> invasive Mas is stony hard and increases in size |
|
|
Infiltrating lobular carcinoma
|
10% of breast cancers
Better prognosis than infiltrating ductal carcinoma |
|
|
Inflammatory breast cancer
|
Uncommon
Rapid growth with early metastasis Skin is erythematous, swollen, warm, edematous and orange |
|
|
Paget disease
|
Uncommon
Lesion is pruritic, red and scaly, located in nipple and areola Nipple may become inverted Discharge may occur |
|
|
Breast cancer risk factors
|
Brca 1 or 2 gene mutation (rr 15)
Ductal or lobular carcinoma in situ (rr 15) Atypical hyperplasia (rr 4) Breast irradiation age < 20 (rr 3) Positive family history (rr 3) |
|
|
Sentinel node biopsy
|
First lymph node to which cancer cells are likely to spread from primary tumor
Dye is injected into tumor which flows into the sentinel node Biopsy is performed to determine stage and if removal of nodes is necessary |
|
|
Adjuvant treatment for node positive breast cancer
|
Premenopausal, er or pr positive --> chemo +- ovarian ablation +- tamoxifen
Premnopausal, er and pr negative --> chemo Postmenopausal, er or pr positive --> tamoxifen + chemo Postmnopausal, er and pr negative --> chemo Elderly --> tamoxifen or chemo |
|
|
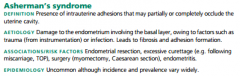
Ashermans Syndrome
Def Aetiology Rf |
|
|
|
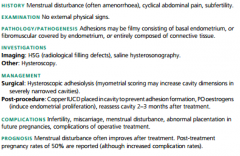
Ashermans Syndrome
Hx, Ex Path Ix Mx |
|
|
|
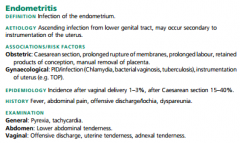
Endometritis:
Def Aetiology Rf Epi Hx Ex |
|
|
|
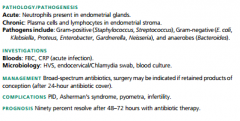
Endometritis:
Pathogenesis Ix Mx Complications Prognosis |
|
|
|
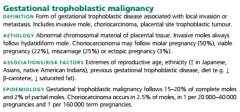
Gestational Trophoblastic Malignancy:
Def Aetiology Rf Epi |
|
|
|
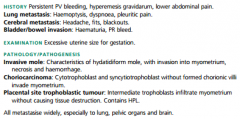
Gestational Trophoblastic Malignancy:
Hx Ex Pathogenesis |
|
|
|
Wha embryonical structure forms:
What embryology forms: a. testes b. Seminiferous tubules c. rete testis d. appendix of epi, duct deff, sem ves e. appendix of testes f. urethra, prostatic utricle, prostate g. penis h. ventral penis i. scrotum |
248 Wha embryonical structure forms:
What embryology forms: a. Gonad b. Gonad cortex c. Gonad medulla d. Mesonephric (Wolffian) duct e. Paramesonephric duct f. urogenital sinus g. phallus h. urogenital folds i. labioscrotal swellings |
|
|
Gestational Trophoblastic Malignancy:
Ix Mx: Lifestyle, Rx and Surgery Complications Prognosis |
|
|
|
What embryology forms:
a. Ovaries b. Fallopian Tubes c. Uterus d. Cervix e. Upper vagina f. Lower vagina g. Minora h. Majora i. Clit j. Hymen K. Round/ov lig.s |
a. primordial follicle(gonad), surrounding mesoderm
b. paramesonephric ducts c. fused paramesonephric ducts d. mullerian tubercle e. f. g. Urogenital folds h. labioscrotal swellings i. phallus j. sinus tubercule k. gubernaculum |
|
|
225 Cyclical Vs Continuous
|
Switch to Continuous if:
>1 year since last period >2 years if premature menopause have been taking cyclical HRT for >1yr |
|
|
Give classification of Rx:
Premique, Prempak-C conjugated oestrogens only Premarin |
Conjugated oestrogens with progesterone
|
|
|
Give type of Rx:
Angeliq, Climagest, Climesse, Clinorette, Cyclo-Progynova, Elleste Duet, Evorel, Femapak, Femoston, FemSeven Conti, FemSeven Sequi, Indivina, Kliofem, Kliovance, Novofem, Nuvelle, Tridestra, Trisequens |
Oestradiol with progesterone
|
|
|
Give type of Rx:
Estradiol implants, Bedol, Climaval, Elleste-Solo, Elleste Solo MX, Estraderm MX, Estraderm TTS, Estradot, Evorel, Fematrix, FemSeven, Oestrogel, Progynova, Progynova TS, Sandrena, Zumenon |
Oestradiol only (only in Women with hystorectomy)
|
|
|
Give type of Rx:
tibolone, Livial, raloxifene |
SERM
|
|
|
Abdo pain
|
OVARIAN TORSION
Sudden onset unilat, constant. Requires opiate analgesia. ↔ WCC, OVARIAN INFARCTION Raised CRP, ↔ WCC. TUBO-OV ABCESS Fever ↑WCC |
|
|
210 PCOS Long term implications
|
Infertility
Endometrial Hyperplasia (caused by severe amen/oligo) Endometrial Ca (due to unopposed E2) Hirsuitism Obesity Sleep Apnoea DM Acne No evidence of ↑Breast or Ov Ca |
|
|
Rx in heavy mennorhagia, faint
Hb 5.2g/dl WCC 8.9g/dl Hct 0.41% MCV 80fl |
Large Bore Venous Access
Fluid Resus CX 4 units blood Lay flat Evelvate legs 1l Saline 0.9% STAT High flow 02 Ig ↑BP or ↓HR consider blood transfusion |
|
|
Ovarian cyst Mx
|
Postmenopausal <5cm = conservative
|
|
|
Treatment of menorrhagia
1st 2nd 3rd line |
|
|
|
Treatment of DUB
|
|
|
|
DUB Diff Diagnosis & Rx
|
|
|
|
PMS Rx guidelines
|

|