Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
349 Cards in this Set
- Front
- Back
|
Pt c/ thickened GB wall (also sludge, pericholecystic fluid), RUQ pain, high WBCs, (+) HIDA
Hx severe burns, prolonged TPN, trauma, or major surgery Primary pathology = _ -> _ -> _ May also have _ 2/2 dehydration, ileus, transfusions Tx; _ |
ACALCULOUS CHOLECYSTITIS:
Burns, TPN, trauma, or major surgery -> BILE STASIS 2/2 narcotics, fasting -> distension, ischemia Also HIGH VISCOSITY 2/2 dehydration, ileus, transfusions US: thickened GB wall, sludge, pericholecystic fluid. (+) HIDA Tx: Cholecystectomy. Percutaneous drain if unstable |
|
|
_ = thickened nodule of mucosa + muscle ass'd c/ Rokitansky-Aschoff sinus
-Sx -Prognosis -Tx |
ADENOMYOSIS = thickened nodule of mucosa + muscle ass'd c/ Rokitansky-Aschoff sinus
-may cause pain -NOT premalignant, doesn't cause stones -Tx: cholecystectomy |
|
|
What tumor marker is considered most strongly associated with hepatocellular CA?
|
80% of patients with HCC has elevated AFP
|
|
|
Alpha 1 anti-trypsin deficiency: RF for what hepatobiliary cancer?
|
Alpha 1 anti-trypsin deficiency:
YES RF for hepatocellular ca |
|
|
Liver lesion treatable c/ metronidazole; no surgery needed
|
Amebic liver abscess:
-Anchovy paste appearance. Aspirate often sterile b/c protozoa only in peripheral rim -Pt c/ hx of EtOH, travel to Mexico, fecal-oral transmission. Fevers, chills, RUQ pain, jaundice, hepatomegaly. -(+) ENTAMOEBA HISTOLYTICA serology in 90% -primary infection = AMEBIC COLITIS -> reaches liver via portal vein -Tx: metronidazole. Aspiration if refractory or super-infection -Surgery only for FREE RUPTURE, antibiotic failure |
|
|
Amebic liver abscess:
Primary infection is in _ Reaches liver via _ |
Amebic liver abscess:
-Anchovy paste appearance. Aspirate often sterile b/c protozoa only in peripheral rim -Pt c/ hx of EtOH, travel to Mexico, fecal-oral transmission. Fevers, chills, RUQ pain, jaundice, hepatomegaly. -(+) ENTAMOEBA HISTOLYTICA serology in 90% -primary infection = AMEBIC COLITIS -> reaches liver via portal vein -Tx: metronidazole. Aspiration if refractory or super-infection -Surgery only for FREE RUPTURE, antibiotic failure |
|
|
Pt presents c/ fever,. RUQ pain, tenderness after travel. Found to have amebic liver abscess.
-Tx is _ |
Amebic liver abscess:
-Anchovy paste appearance. Aspirate often sterile b/c protozoa only in peripheral rim -Pt c/ hx of EtOH, travel to Mexico, fecal-oral transmission. Fevers, chills, RUQ pain, jaundice, hepatomegaly. -(+) ENTAMOEBA HISTOLYTICA serology in 90% -primary infection = AMEBIC COLITIS -> reaches liver via portal vein -Tx: metronidazole. Aspiration if refractory or super-infection -Surgery only for FREE RUPTURE, antibiotic failure |
|
|
Amebic liver abscess:
(+) serology for organism _ in _% |
Amebic liver abscess:
-Anchovy paste appearance. Aspirate often sterile b/c protozoa only in peripheral rim -Pt c/ hx of EtOH, travel to Mexico, fecal-oral transmission. Fevers, chills, RUQ pain, jaundice, hepatomegaly. -(+) ENTAMOEBA HISTOLYTICA serology in 90% -primary infection = AMEBIC COLITIS -> reaches liver via portal vein -Tx: metronidazole. Aspiration if refractory or super-infection -Surgery only for FREE RUPTURE, antibiotic failure |
|
|
Liver abscess in pt c/ hx of EtOH, travel to Mexico, fecal-oral transmission
|
Amebic liver abscess:
-Anchovy paste appearance. Aspirate often sterile b/c protozoa only in peripheral rim -Pt c/ hx of EtOH, travel to Mexico, fecal-oral transmission. Fevers, chills, RUQ pain, jaundice, hepatomegaly. -(+) ENTAMOEBA HISTOLYTICA serology in 90% -primary infection = AMEBIC COLITIS -> reaches liver via portal vein -Tx: metronidazole. Aspiration if refractory or super-infection -Surgery only for FREE RUPTURE, antibiotic failure |
|
|
Amebic liver abscess:
What do you expect to find on culture of cyst? |
Amebic liver abscess:
-Anchovy paste appearance. Aspirate often sterile b/c protozoa only in peripheral rim -Pt c/ hx of EtOH, travel to Mexico, fecal-oral transmission. Fevers, chills, RUQ pain, jaundice, hepatomegaly. -(+) ENTAMOEBA HISTOLYTICA serology in 90% -primary infection = AMEBIC COLITIS -> reaches liver via portal vein -Tx: metronidazole. Aspiration if refractory or super-infection -Surgery only for FREE RUPTURE, antibiotic failure |
|
|
Liver abscess c/ "anchovy paste" contents
|
Amebic liver abscess:
-Anchovy paste appearance. Aspirate often sterile b/c protozoa only in peripheral rim -Pt c/ hx of EtOH, travel to Mexico, fecal-oral transmission. Fevers, chills, RUQ pain, jaundice, hepatomegaly. -(+) ENTAMOEBA HISTOLYTICA serology in 90% -primary infection = AMEBIC COLITIS -> reaches liver via portal vein -Tx: metronidazole. Aspiration if refractory or super-infection -Surgery only for FREE RUPTURE, antibiotic failure |
|
|
_ = #1 cancer of biliary tract
Main RF is _ Spreads 1st to liver segments _, _ Spreads to nodes _ 90% present c/ stage _ disease _% 5-yr survival |
GALLBLADDER ADENOCA = #1 cancer of biliary tract
PORCELIN GB => 10-20% risk (do open cholecystectomy 2/2 tumor implants @ trocar sites) -Spreads to segments IV, V; cystic duct nodes (R) -Stage 1 (mucosa, usually incidental finding) => cholecystectomy -Stage 2 (muscle) => chole + 2-3 cm margins @ segments 3,4 + regional LNs inc.along portal triad (may need Whipple, lobectomy, or resection of CBD) -90% present c/ stage 4 -5% 5-yr survival |
|
|
adnocarcinma of GB:
-if grossly visible tumor, should do.. |
GALLBLADDER ADENOCA = #1 cancer of biliary tract
-PORCELIN GB => 10-20% risk (do open cholecystectomy to avoid tumor implants @ trocar sites) -Spreads to segments IV, V; cystic duct nodes (R) -90% present c/ stage 4 5% 5-yr survival -If grossly visible tumor, should do regional lymphadenectomy, wedge segment V, skeletonize portal triad |
|
|
Young F undergoes lap chole + GB adenoca found extending into muscular layer
-Next step = _ |
GALLBLADDER ADENOCA = #1 cancer of biliary tract
-PORCELIN GB => 10-20% risk (do open cholecystectomy to avoid tumor implants @ trocar sites) -Spreads to segments IV, V; cystic duct nodes (R) -90% present c/ stage 4 5% 5-yr survival - |
|
|
Why do people with cirrhosis get ascites?
|
Cirrhosis ascites:
hepatocyte destruction -> scarring -> increased hepatic pressure -> portal congestion -> LYMPHATIC OVERLOAD -> LEAKAGE OF SPLANCHNIC/ HEPATIC LYMPH into peritoneum |
|
|
After paracentesis for ascites,
replace albumin _g/ 100cc removed |
After paracentesis for ascites,
replace albumin 1g/ 100cc removed |
|
|
Ascites 2/2 cirrhosis:
best diuretic is _ |
Ascites 2/2 cirrhosis:
SPIRONOLACTONE = best diuretic counteracts hyperaldosteronism often seen c/ liver failure |
|
|
Ascites 2/2 cirrhosis:
complication of peritoneovenous shunt (Denver, LeVeen) is _ |
Ascites 2/2 cirrhosis:
complication of peritoneovenous shunt (Denver, LeVeen) = DIC |
|
|
Ascites 2/2 cirrhosis:
Antibiotic prophylaxis against SBP is _ |
Ascites 2/2 cirrhosis:
Antibiotic prophylaxis against SBP = Cipro 750mg/WEEK |
|
|
Ascites 2/2 cirrhosis:
Pts have hyperaldosteronism b/c _ |
Ascites 2/2 cirrhosis:
impaired hepatic metabolism, GFR -> hyperaldosteronism (for this reason, spironolactone is best diuretic) |
|
|
#1 cause of benign biliary stricture = _
|
Iatrogenic (lap chole) = #1 cause of benign biliary stricture
|
|
|
Biliary colic = _
Resolves in _-_ hrs |
Biliary colic = transient cystic duct obstruction 2/2 stone passage
Resolves in 4-6 hrs |
|
|
Bile: _% bile salts, _% lecithin, _% cholesterol
- Stones form if increased cholesterol or decreased salts or lecithin -GB concentrates bile active by mechanism __. -Bile pool _g, recirculated q_h, lose _g daily (_%) |
Bile: 80% bile salts, 15% lecithin, 5% cholesterol
- Stones form if increased cholesterol or decreased salts or lecithin -GB concentrates bile by active resorption of NaCl, H20 then follows. -Bile pool 5G, recirculated q4h, lose 0.5g daily (10%) |
|
|
3 things that increase bile excretion
|
Increase bile excretion:
CCK Secretin Vagal input |
|
|
3 things that decrease bile
(2 hormones, 1 neuro mechanism) |
Decrease bile excretion:
VIP (from gut + pancreas cells) Somatostatin (from antral D cells) Sympathetic stimulation |
|
|
Endocrine stimulation by _ -> constant, steady tonic contraction of GB
|
CCK -> constant, steady tonic contraction of GB
|
|
|
3 essential functions of bile
|
Essential functions of bile:
Fat-soluble vitamin absorbtion Bilirubin excretion Cholesterol excretion |
|
|
Active resorption of conjugated bile acids occurs in the _
(passive resorption of bile acids occurs 45% in sm intestine, 5% in colon) |
Active resorption of conjugated bile acids occurs in the TERMINAL ILEUM
(passive resorption of bile acids occurs 45% in sm intestine, 5% in colon) |
|
|
What makes poo brown?
|
Stercobilin = breakdown product of conjugated bili in gut
Makes poo brown |
|
|
Delta bilirubin:
defined as _ -1/2 life is _ |
Delta bilirubin:
-Bound to albumin -1/2 life = 18 days -Takes a while to clear after longstanding jaundice |
|
|
Primary bile acids = cholic acid, chenodeoxycholic acid
Secondary bile acids are formed by __: deoxycholic acid, lithocholic acid |
Primary bile acids = cholic acid, chenodeoxycholic acid
Secondary bile acids are formed by __: deoxycholic acid, lithocholic acid |
|
|
A 20-year-old woman with jaundice has a fusiform dilatation of her extrahepatic bile duct. Therapy for this condition is aimed at prevention of
|
bile duct carcinoma
|
|
|
Gallbladder: lies b/w liver segments _ and _
|
Gallbladder: b/w segments 3 and 4
|
|
|
Triangle of calot:
_ = lateral _ = medial _ = superior |
Triangle of calot:
cystic duct = lateral CBD = medial liver = superior |
|
|
Cystic artery branches off the _
|
Cystic artery branches off the R hepatic artery
|
|
|
Cystic veins drain into _ and _
|
Cystic veins drain into:
R branch of portal vein Liver |
|
|
Lymphatics are to the L or R of common bile duct?
|
Lymphatics are to the R of common bile duct
|
|
|
Parasympatetic fibers to biliary system course from L (anterior) or R (posterior) trunk of vagus?
|
Parasympatetic fibers to biliary system course from L (anterior) trunk of vagus
|
|
|
Sympathetic fibers to biliary system course from T_-T_, though _ and _ ganglia
|
Sympathetic fibers to biliary system course from T7-T10, though splanchnic and celiac ganglia
|
|
|
Sphincter of oddi:
Drug _ contracts it Drug _ relaxes it |
Sphincter of oddi:
MORPHINE contracts it GLUCAGON relaxes it |
|
|
Common bile duct:
Normal size is <_mm <_ mm after cholecystectomy |
Common bile duct:
Normal size = <8mm <10 mm after cholecystectomy |
|
|
Gallbladder wall:
Normal thickness is <_ mm |
Gallbladder wall:
Normal thickness is <4 mm |
|
|
Pancreatic duct:
Normal size is <_mm |
Pancreatic duct:
Normal size is <4 mm |
|
|
Highest concentration of CCk and secretin is in _
|
Highest concentration of CCk and secretin is in DUODENUM
|
|
|
Rokitansky-Aschoff sinuses = invagination of_
2/2_ |
Rokitansky-Aschoff sinuses = invagination of GB wall epithelium
2/2 increased gallbladder pressure |
|
|
_ = biliary ducts that go directly from liver -> GB
Involved in post-cholecystectomy complication… |
Ducts of Luschka: direct from liver -> GB
Can leak after cholecystectomy |
|
|
Bile is secreted by _ cells (80%) and _ cells (_%)
|
Bile is secreted by hepatocystes (80%) and bile cancalicualr cells (20%)
|
|
|
A 68 year old man presents with painless jaundice. He states he has been yellow for two weeks and it keeps getting worse. Workup reveals pancreatic cancer with multiple liver metastasis and high grade obstruction of the distal common bile duct. He is scheduled for a percutaneous transhepatic biliary drainage procedure. Pre-procedure laboratory studies reveal Hgb 10.6 gm/dl; platelets 80,000/mm3; INR 1.63, PT 23; PTT 44. The most likely source of the patients elevated INR is :
|
"Biliary obstruction -> lack of enteric bile salts -> decreased absorption of fat and fat solutes, inc. Vit K
|
|
|
young woman develops jaudice + ascites 2 wks postpartum.
-Consistent c/ ... |
Post-partum hepatic vein thrombosis/Budd-Chiari ;
-rare, related to hypercoag state. -Dx: mesenteric angiogram c/ venous phase contrast. MRI less sensitive |
|
|
Budd Chiari: tx is _
|
Budd Chiari: occlusion of hepatic veins, IVC
-RUQ pain, hepatosplenomegaly, ascites, hepatic failure, muscle wasting, variceal bleeding -Dx: CT angio c/ venous sphase contrast Liver bx: sinusoidal dilation, centrilobular congestion Tx: portacaval sunt (needs to connect to IVC above obstruction) |
|
|
Pt c/ portal HTN gets a bx that shows:
sinusoidal dilation, congestion, centrilobular congestion What is wrong c/ pt? |
Budd Chiari:
Portal HTN 2/2 pre-sinusoidal obstruction Bx:sinusoidal dilation, congestion, centrilobular congestion What is wrong c/ pt? |
|
|
the caudate lobe is fed by what arterial supply?
|
the caudate lobe:
- receives separate right and left portal and arterial blood flow -has its own venous drainage to the IVC, so Budd Chiari has caudate lobe hypertrophy |
|
|
4 roles of CCK in digestion...
|
CCK:
-GB contraction -pancreatic enzyme release -relaxation of sphincter of Oddi -increased intestinal motility |
|
|
what are the elements of Child-Pugh score (hint: ProBAAN)
|
Child-Pugh score: ProBAAN
Prothrombin tume Bili Albumin Ascites Neuro disorder |
|
|
what are the factors in Child's classification for liver failure?
(hint: 3 lab, 2 clinical) |
Child's classification of liver failure :
Lab: bilirubin, albumin, PT Clinical: ascites, neurologic disorder. |
|
|
most common location for cholangiocarcinoma is _
-Tx is _ |
Cholangiocarcinoma -RFs: elderly, male, C. sinensis, UC, choledochal cysts (15% risk) PSC, congen hepatic fibrosis, chronic bile duct ingecion, typhpid
-Suspect in pt c/ focal bile duct stenosis, no hx bile duct surgery or pancreatitis -60-80% of cholangiocarcinomas occur in perihilar region (around hepatic duct bifurcation). -Distal cholangiocarcinoma resection is more likely to be curative. -Pancreatoduodenectomy (Whipple procedure) c/ pylorus preservation = treatment for distal resectable cholangiocarcinomas. -CA 19-9 may be elevated in cholangiocarcinoma, similar to pancreatic cancer. -Upper 1/3 (Klatskin) #1: if resectable, lobectomy + stent contralateral bile duct -Middle 1/3 => EHBDR (extra-hep bile duct resection), hepatico-jej -Lower 1/3: Whipple |
|
|
tx for cholangiocarcinoma in middle 1/3 of duct
|
Cholangiocarcinoma -RFs: elderly, male, C. sinensis, UC, choledochal cysts (15% risk) PSC, congen hepatic fibrosis, chronic bile duct ingecion, typhpid
-Suspect in pt c/ focal bile duct stenosis, no hx bile duct surgery or pancreatitis -60-80% of cholangiocarcinomas occur in perihilar region (around hepatic duct bifurcation). -Distal cholangiocarcinoma resection is more likely to be curative. -Pancreatoduodenectomy (Whipple procedure) c/ pylorus preservation = treatment for distal resectable cholangiocarcinomas. -CA 19-9 may be elevated in cholangiocarcinoma, similar to pancreatic cancer. -Upper 1/3 (Klatskin) #1: if resectable, lobectomy + stent contralateral bile duct -Middle 1/3 => EHBDR (extra-hep bile duct resection), hepatico-jej -Lower 1/3: Whipple |
|
|
tx for cholangiocarcinoma in lower 1/3 of duct
|
Cholangiocarcinoma -RFs: elderly, male, C. sinensis, UC, choledochal cysts (15% risk) PSC, congen hepatic fibrosis, chronic bile duct ingecion, typhpid
-Suspect in pt c/ focal bile duct stenosis, no hx bile duct surgery or pancreatitis -60-80% of cholangiocarcinomas occur in perihilar region (around hepatic duct bifurcation). -Distal cholangiocarcinoma resection is more likely to be curative. -Pancreatoduodenectomy (Whipple procedure) c/ pylorus preservation = treatment for distal resectable cholangiocarcinomas. -CA 19-9 may be elevated in cholangiocarcinoma, similar to pancreatic cancer. -Upper 1/3 (Klatskin) #1: if resectable, lobectomy + stent contralateral bile duct -Middle 1/3 => EHBDR (extra-hep bile duct resection), hepatico-jej -Lower 1/3: Whipple |
|
|
A 52 yo male with history of hepatolithiasis presents with painless jaundice. ERCP and brush biopsy reveals cholangiocarcinoma.
Where do most cholangiocarcinomas occur? What location of cholangiocarcinoma is most amenable to resection and what would that surgery be? What tumor marker may be elevated? |
Cholangiocarcinoma -RFs: elderly, male, C. sinensis, UC, choledochal cysts (15% risk) PSC, congen hepatic fibrosis, chronic bile duct ingecion, typhpid
-Suspect in pt c/ focal bile duct stenosis, no hx bile duct surgery or pancreatitis -60-80% of cholangiocarcinomas occur in perihilar region (around hepatic duct bifurcation). -Distal cholangiocarcinoma resection is more likely to be curative. -Pancreatoduodenectomy (Whipple procedure) c/ pylorus preservation = treatment for distal resectable cholangiocarcinomas. -CA 19-9 may be elevated in cholangiocarcinoma, similar to pancreatic cancer. -Upper 1/3 (Klatskin) #1: if resectable, lobectomy + stent contralateral bile duct -Middle 1/3 => EHBDR (extra-hep bile duct resection), hepatico-jej -Lower 1/3: Whipple |
|
|
A 62-year-old woman had an uneventful cholecystectomy at age 30. She now has jaundice and pruritus. Endoscopic retrograde cholangiopancreatography shows a tight stricture at the junction of the right and left hepatic ducts. The most likely diagnosis is
|
Cholangiocarcinoma -RFs: elderly, male, C. sinensis, UC, choledochal cysts (15% risk) PSC, congen hepatic fibrosis, chronic bile duct ingecion, typhpid
-Suspect in pt c/ focal bile duct stenosis, no hx bile duct surgery or pancreatitis -60-80% of cholangiocarcinomas occur in perihilar region (around hepatic duct bifurcation). -Distal cholangiocarcinoma resection is more likely to be curative. -Pancreatoduodenectomy (Whipple procedure) c/ pylorus preservation = treatment for distal resectable cholangiocarcinomas. -CA 19-9 may be elevated in cholangiocarcinoma, similar to pancreatic cancer. -Upper 1/3 (Klatskin) #1: if resectable, lobectomy + stent contralateral bile duct -Middle 1/3 => EHBDR (extra-hep bile duct resection), hepatico-jej -Lower 1/3: Whipple |
|
|
Cholangiosarcoma:
2 things that correlate c/ outcome |
Cholangiosarcoma: these correlate c/ outcome
1.) TUMOR SIZE 2.) SATELLITE NODULES |
|
|
Cholangiosarcoma:
worse survival c/ intra- or extra-hepatic |
Cholangiosarcoma:
INTRA-hepatic => WORSE survival |
|
|
Clonorchiasis infection = RF for cancer _
|
Clonorchiasis infection = RF for
CHOLANGIOSARCOMA |
|
|
Ulcerative colitis = RF for cancer _
|
Cholangiocarcinoma:
-RFs elderly, male, C. sinensis, thphoid, UC, choledochal cyst, clerosing cholangitis, congen hepatic fibrosis, chronic bile duct obstruction -Sx painless jaundice -> cholangitis, anemia, pruritus -Dx ERCP then MRI. FOCAL BILE DUCT STENOSIS in pt s/ hx of biliary surgery or pancreatitis -Upper 1/3 of tract = Klathskin tumor => most common but usually unresectable. Can do lobectomy + stent contralateral duct if localized to 1 lobe -Middle 1/3 of tract => HEPATICOJEJUNOSTOMY -Lower 1/3 of tract => WHIPPLE -Unresectable => palliative stent -20% 5-yr survival |
|
|
Choledochal cyst = RF for cancer _
|
Cholangiocarcinoma:
-RFs elderly, male, C. sinensis, thphoid, UC, choledochal cyst, clerosing cholangitis, congen hepatic fibrosis, chronic bile duct obstruction -Sx painless jaundice -> cholangitis, anemia, pruritus -Dx ERCP then MRI. FOCAL BILE DUCT STENOSIS in pt s/ hx of biliary surgery or pancreatitis -Upper 1/3 of tract = Klathskin tumor => most common but usually unresectable. Can do lobectomy + stent contralateral duct if localized to 1 lobe -Middle 1/3 of tract => HEPATICOJEJUNOSTOMY -Lower 1/3 of tract => WHIPPLE -Unresectable => palliative stent -20% 5-yr survival |
|
|
RFs for Cholangiocarinoma:
elderly men, typhoid, and "6 C's" which are… |
Cholangiocarcinoma:
-RFs elderly, male, C. sinensis, thphoid, UC, choledochal cyst, clerosing cholangitis, congen hepatic fibrosis, chronic bile duct obstruction -Sx painless jaundice -> cholangitis, anemia, pruritus -Dx ERCP then MRI. FOCAL BILE DUCT STENOSIS in pt s/ hx of biliary surgery or pancreatitis -Upper 1/3 of tract = Klathskin tumor => most common but usually unresectable. Can do lobectomy + stent contralateral duct if localized to 1 lobe -Middle 1/3 of tract => HEPATICOJEJUNOSTOMY -Lower 1/3 of tract => WHIPPLE -Unresectable => palliative stent -20% 5-yr survival |
|
|
Suspect cholangiocarcinoma,
need to get 2 kinds of imaging _ |
Cholangiocarcinoma:
-RFs elderly, male, C. sinensis, thphoid, UC, choledochal cyst, clerosing cholangitis, congen hepatic fibrosis, chronic bile duct obstruction -Sx painless jaundice -> cholangitis, anemia, pruritus -Dx ERCP then MRI. FOCAL BILE DUCT STENOSIS in pt s/ hx of biliary surgery or pancreatitis -Upper 1/3 of tract = Klathskin tumor => most common but usually unresectable. Can do lobectomy + stent contralateral duct if localized to 1 lobe -Middle 1/3 of tract => HEPATICOJEJUNOSTOMY -Lower 1/3 of tract => WHIPPLE -Unresectable => palliative stent -20% 5-yr survival |
|
|
Cholangiocarcinoma: natural history of spread
|
Cholangiocarcinoma:
-RFs elderly, male, C. sinensis, thphoid, UC, choledochal cyst, clerosing cholangitis, congen hepatic fibrosis, chronic bile duct obstruction -Sx painless jaundice -> cholangitis, anemia, pruritus -Dx ERCP then MRI. FOCAL BILE DUCT STENOSIS in pt s/ hx of biliary surgery or pancreatitis -Upper 1/3 of tract = Klathskin tumor => most common but usually unresectable. Can do lobectomy + stent contralateral duct if localized to 1 lobe -Middle 1/3 of tract => HEPATICOJEJUNOSTOMY -Lower 1/3 of tract => WHIPPLE -Unresectable => palliative stent -20% 5-yr survival |
|
|
Elderly man c/ early painless jaundice, high bili, high alk phos -> +/- cholangitis, wt loss, anemia, pruritus -> focal bile duct stenosis
No hx of biliary surgery or pancreatits Suggestive of _ _% 5-yr survival |
Cholangiocarcinoma:
-RFs elderly, male, C. sinensis, thphoid, UC, choledochal cyst, clerosing cholangitis, congen hepatic fibrosis, chronic bile duct obstruction -Sx painless jaundice -> cholangitis, anemia, pruritus -Dx ERCP then MRI. FOCAL BILE DUCT STENOSIS in pt s/ hx of biliary surgery or pancreatitis -Upper 1/3 of tract = Klathskin tumor => most common but usually unresectable. Can do lobectomy + stent contralateral duct if localized to 1 lobe -Middle 1/3 of tract => HEPATICOJEJUNOSTOMY -Lower 1/3 of tract => WHIPPLE -Unresectable => palliative stent -20% 5-yr survival |
|
|
Cholangiocarcinoma type that is most common, worst prognosis
Tx |
Cholangiocarcinoma:
-RFs elderly, male, C. sinensis, thphoid, UC, choledochal cyst, clerosing cholangitis, congen hepatic fibrosis, chronic bile duct obstruction -Sx painless jaundice -> cholangitis, anemia, pruritus -Dx ERCP then MRI. FOCAL BILE DUCT STENOSIS in pt s/ hx of biliary surgery or pancreatitis -Upper 1/3 of tract = Klathskin tumor => most common but usually unresectable. Can do lobectomy + stent contralateral duct if localized to 1 lobe -Middle 1/3 of tract => HEPATICOJEJUNOSTOMY -Lower 1/3 of tract => WHIPPLE -Unresectable => palliative stent -20% 5-yr survival |
|
|
Cholangiocarcinoma in middle 1/3 of tract =>
Tx: _ |
Cholangiocarcinoma:
-RFs elderly, male, C. sinensis, thphoid, UC, choledochal cyst, clerosing cholangitis, congen hepatic fibrosis, chronic bile duct obstruction -Sx painless jaundice -> cholangitis, anemia, pruritus -Dx ERCP then MRI. FOCAL BILE DUCT STENOSIS in pt s/ hx of biliary surgery or pancreatitis -Upper 1/3 of tract = Klathskin tumor => most common but usually unresectable. Can do lobectomy + stent contralateral duct if localized to 1 lobe -Middle 1/3 of tract => HEPATICOJEJUNOSTOMY -Lower 1/3 of tract => WHIPPLE -Unresectable => palliative stent -20% 5-yr survival |
|
|
Cholangiocarcinoma in lower 1/3 of tract =>
Tx: _ |
Cholangiocarcinoma:
-RFs elderly, male, C. sinensis, thphoid, UC, choledochal cyst, clerosing cholangitis, congen hepatic fibrosis, chronic bile duct obstruction -Sx painless jaundice -> cholangitis, anemia, pruritus -Dx ERCP then MRI. FOCAL BILE DUCT STENOSIS in pt s/ hx of biliary surgery or pancreatitis -Upper 1/3 of tract = Klathskin tumor => most common but usually unresectable. Can do lobectomy + stent contralateral duct if localized to 1 lobe -Middle 1/3 of tract => HEPATICOJEJUNOSTOMY -Lower 1/3 of tract => WHIPPLE -20% 5-yr survival |
|
|
Cholangiocarcinoma that is unresectable =>
Tx: _ |
Cholangiocarcinoma that is unresectable => PALLIATIVE STENT
|
|
|
Cholangitis:
#1 cause = _ -2 most common organisms are _ |
Cholangitis:
-Gallstones = #1 cause -E. coli > Klebsiella |
|
|
Cholangitis:
#1 serious complication is _ , which is 2/2 _ |
Cholangitis:
-Renal failure = #1 serious complication, 2/2 SEPSIS |
|
|
Cholangitis:
Tx is _ |
Cholangitis:
-E coli = #1 organism Tx: resuscition, abx, ERCP + sphincterotomy + stone extraction 2nd line (e.g. ,if unable to cannulate the CBD) percutaneous transhepatic cholangiography (PTC) 3rd line (e.g. radiologist unable to place PTC tube) place T-tube in OR |
|
|
Cholangitis:
Tx if PTC tube present = _ |
Cholangitis:
Change PTC tube if already present |
|
|
Cholangitis:
2 late complications |
Cholangitis:
2 late complications = stricture, hepatic abscess |
|
|
Cholangitis 2/2 biliary obstruction:
-US findings_ |
Cholangitis 2/2 biliary obstruction:
-CBD >8mm (>10mm after cholecytectomy) |
|
|
Pt presents c/ jaundice, RUQ tenderness, fever, hypotension, mental status change
-This patient has __ -Tx is __ |
Cholangitis:
-jaundice, RUQ tenderness, fever, hypotension, mental status change -Tx: immediate IV abx, fluid resuscitation, emergent drainage of CBD |
|
|
Recurrent cholangitis 2/2 primary CBD stones is called _
2/2 _ Tx: surgical, medical |
ORIENTAL CHOLANGIOHEPATITIS = recurrent cholangitis 2/2 primary CBD stones
2/2 C. sinensis, A. lumbricoides, T trichura, E. coli Tx: HEPATICOJEJUNOSTOMY + ANTI-PARASITICS |
|
|
#1 RF for positive bile culture = _
#1 bacteria = _ |
#1 RF for positive bile culture = POST-OP STRICTURE
#1 bacteria = E. coli (often polymicrobial) |
|
|
Common bile duct injury:
Anatomic abnormality in 10% of people that increases risk If > _mm => must open + perform _ (or _) If <_% of circumference, can perform _ |
Common bile duct injury:
10% have R posterior duct (from segment 6 or 7) entering CBD separately (confused for cystic duct) <50% of circumference => primary repair > 2mm => open hepatojejunostomy (or choledochojejunostomy) |
|
|
After cholecystectomy, intra-op cholangiogram shows good CBD filling but no filling of proximal hepatic duct
-Suspect _ -Next step = _ |
After cholecystectomy, intra-op cholangiogram shows good CBD filling but no filling of proximal hepatic duct
-Suspect that hepatic duct was mistaken for cystic duct + clipped -Open to evaluate |
|
|
After cholecystectomy, intra-op cholangiogram shows good CBD filling but no filling of proximal hepatic duct
-Pt re-opened and hepatic duct found to be ligated -Next step = _ |
After cholecystectomy, intra-op cholangiogram shows good CBD filling but no filling of proximal hepatic duct
-Suspect that hepatic duct was mistaken for cystic duct + clipped -Open to evaluate -> hepaticojejunostomy (end-to-end hepatic duct anastomosis leads to stricture) |
|
|
After cholecystectomy, intra-op cholangiogram shows poor CBD filling
(there had never been any sign CBD stone) -Suspect _ -Next step = _ |
After cholecystectomy, intra-op cholangiogram shows poor CBD filling, bur there is no CBD stone
-Likely CBD ligated -Open + do choledocho-jejunostomy |
|
|
Pt has persistant N/V after cholecystectomy:
Order a _ to look for _ |
Pt has persistant N/V after cholecystectomy:
Order RUQ US to r/o bile leak, cystic duct remnant leak, injuries to hepatic or CBD, leak from duct of Luschka |
|
|
Pt has persistant N/V after cholecystectomy, US shows fluid collection
Next step is _ |
Pt has persistant N/V after cholecystectomy, US shows fluid collection=>
Percutaneous drain to determine whether it is a bile leak -If bilious, send pt for ERCP |
|
|
Pt has persistant N/V after cholecystectomy -> US shows fluid collection -> percutaneous drain shows bilious fluid
Next step is _ |
Pt has persistant N/V after cholecystectomy -> US shows fluid collection -> percutaneous drain shows bilious fluid =>
ERCP -Cystic duct remnant leak, hepatic duct injury, Duct of Luscka leak, CBD injury => sphincterotomy + temporary stent (cystic duct remnant will eventually scar down) -Hepatic duct or CBD transection => hepaticojujunosotmy or choledochojejunostomy -More serious injuries might require drain x 6-8 wks, then reoperation |
|
|
Pt has persistant N/V after cholecystectomy -> US shows fluid collection -> percutaneous drain shows bilious fluid -> ERCP shows CYSTIC DUCT REMNANT LEAK.
Tx = _ |
Pt has persistant N/V after cholecystectomy -> US shows fluid collection -> percutaneous drain shows bilious fluid -> ERCP shows cystic duct remnant leak.
Tx = SPHINCTEROTOMY + STENT |
|
|
Pt has persistant N/V after cholecystectomy -> US shows fluid collection -> percutaneous drain shows bilious fluid -> ERCP shows SMALL INJURY TO HEPATIC or CB DUCT.
Tx = _ |
Pt has persistant N/V after cholecystectomy -> US shows fluid collection -> percutaneous drain shows bilious fluid -> ERCP shows small injury to hepatic or common bile duct
Tx = SPHINCTEROTOMY + STENT |
|
|
Pt has persistant N/V after cholecystectomy -> US shows fluid collection -> percutaneous drain shows bilious fluid -> ERCP shows LEAK FROM DUCT OF LUSCKA.
Tx = _ |
Pt has persistant N/V after cholecystectomy -> US shows fluid collection -> percutaneous drain shows bilious fluid -> ERCP shows leak from Duct of Luscka
Tx = SPHINCTEROTOMY + STENT |
|
|
Pt has persistant N/V after cholecystectomy -> US shows fluid collection -> found to have COMPLETE CBD TRANSECTION.
Tx = _ |
Pt has persistant N/V after cholecystectomy -> US shows fluid collection -> found to have complete CBD transection.
Tx = CHOLEDOCHOJEJUNOSTOMY |
|
|
Pt has persistant N/V after cholecystectomy -> US shows NO fluid collection, but DILATED HEPATIC DUCTS -> probably 2/2 _.
Tx = _ |
Pt has persistant N/V after cholecystectomy -> US shows NO fluid collection, but DILATED HEPATIC DUCTS -> likely TRANSECTED CBD, needs choledochojejunostomy
|
|
|
Pt has ANASTOMOTIC LEAK after hepaticojejunostomy or transplant
Tx is _ |
Pt has ANASTOMOTIC LEAK after hepaticojejunostomy or transplant
Tx = ERCP + STENT |
|
|
Pt is septic s/p cholecystectomy -> fluid resuscitate, stabilize -> RUQ US shows fluid collection or dilated intrahepatic ducts.
2 possible culprits |
Sepsis s/p cholecystectomy, RUQ US shows fluid collection or dilated intrahepatic ducts:
COMPLETE CBD TRANSECTION, CHOLANGITIS |
|
|
Pt is septic s/p cholecystectomy -> fluid resuscitate, stabilize -> RUQ US shows fluid collection, NO dilated intrahepatic ducts => Tx is _
|
Pt is septic s/p cholecystectomy -> fluid resuscitate, stabilize -> RUQ US shows fluid collection, NO dilated intrahepatic ducts =>
do ERCP + STENT STRICTURED AREA |
|
|
#1 cause of late post-op biliary strictures
2 other causes Dx (2 options) Tx |
ISCHEMIA = #1 cause of late post-op biliary strictures
Also 2/2 chronic pancreatitis, stricture of biliary-enteric anastomosis Dx:ERCP shows stricture, US shows dilated intrahepatic ducts Tx: ERCP + SPHINCTEROTOMY +/- STENT to decompress -> PTC tube if that fails |
|
|
Bilie duct injury c/ symptoms within 7 days of surgery:
Tx is _ |
Bile duct injury within 7 days of surgery=>
HEPATICOJEJUNOSTOMY (unlikely to be sufficiently treated c/ ERCP, balloon, stent) |
|
|
Bile duct injury c/ symptoms >7days after surgery:
Tx is _ |
Bile duct injury c/ symptoms >7days after surgeryy =>
HEPATICOJEJUNOSTOMY 6-8 wks after surgery Late injuries: ERCP, sphincterotomy, stent. Get brushings to r/o malignancy |
|
|
Bile duct injury/Biliary stricture years after surgery =>
Tx is _. Make sure to r/o _ |
Bile duct injury/Biliary stricture years after surgery =>
ERCP, sphincterotomy, stent. Get brushings to r/o malignancy |
|
|
Arterial injury during cholecystectomy is usually to the _
|
R HEPATIC ARTERY = arterial injury during cholecystectomy
|
|
|
Pt s/p lap cholecystectomy found to have GB adenoca limited to mucosa (stage _)
Mgmt is _ Worry about complication of surgery _ |
Pt s/p lap cholecystectomy found to have GB adenoca limited to mucosa (stage 1)
No more surgery Worry about tumor implants @ trocar site |
|
|
Pt s/p lap cholecystectomy found to have GB adenoca into muscle (stage _)
Mgmt is _ Worry about complication of lap chole _ |
Pt s/p lap cholecystectomy found to have GB adenoca into muscle (stage 2)
Wide resection (2-3 cm margins) around liver bed @ segments IV, V (most common site of spread), regional lymphadenectomy including portal triad (most commonly spreads to cystic duct nodes on R) May need Whipple, lobectomy, or CBD resection Worry about tumor implants @ trocar site |
|
|
Pt s/p cholecystectomy <24 hrs ago, now in shock
Likely _ |
Pt s/p cholecystectomy <24 hrs ago, now in shock
Likely HEMORRHAGIC 2/2 CLIP FALLING OFF CYSTIC ARTERY |
|
|
Pt s/p cholecystectomy >24 hrs ago, now in shock
Likely _ |
Pt s/p cholecystectomy >24 hrs ago, now in shock
Likely SEPTIC 2/2 ACCIDENTAL CLIP ON CBD -> CHOLANGITIS |
|
|
2 indications for asymptomatic cholecystectomy
|
3 indications for asymptomatic cholecystectomy =
-Liver transplant -Gastric bypass |
|
|
Pt undergoing routine lap chole suddenly develops drop in end-tidal CO2, (-) breath sounds, but stable BP and HR
-Suspect _ -Tx is _ |
Disconnection from vent:
-End-tidal CO2 reflects CO2 exchange from blood to alveolus -> sudden decrease suggests disconnection from vent, air embolus |
|
|
Pt undergoing routine lap chole suddenly develops rise in end-tidal CO2, decreased BS @ bases, but stable BP and HR
-Suspect _ -Tx is _ |
Atelectasis intra-op:
-Rise in ET CO2 reflects impaired exchange @ alveolar level 2/2 lung collapse, atelectasis -> probably needs larger tidal volumes |
|
|
Cholecystitis: 3 most common organisms
|
Cholecystitis: 3 most common organisms =
E. coli Klebsiella Enterococcus |
|
|
Gallstone type that has most risk of cholecystitis?
pigmented/non-pigmented |
PIGMENTED gallstones => most risk of cholecystitis
Black: hemolysis, cirrhosis, chronic TPN, ileal resection Brown (form in CBD): Asians, 2/2 E. coli producing beta-glucuronidase -> deconjugates bili -> Ca bilirubinate |
|
|
US:
_% sensitive for gallstones 3 US findings of cholecystitis _ suggests a CBD stone/obstruction |
US:
95% sensitive for gallstones Cholecystitis; stones, BG wall >4mm thick, pericholecystic fluid CBD>8mm suggests a CBD stone/obstruction |
|
|
Bacterial infection of bile
Most common cause Other possible cause |
Bacterial infection of bile
Dissemination from PORTAL SYSTEM = most common cause Also 2/2 retrograde infection from bacteria in duodenum |
|
|
Diabetic pt c/ sudden severe ab pain, N/V, sepsis
Gas in GB wall on ab x-ray Diagnosis is _ #1 organism = _ Complication to be worried about _ Tx: _ |
EMPHYSEMATOUS GALLBLADDER DZ:
Sudden severe ab pain, N/V, sepsis RF: Diabetics 2/2 CLOSTRIDIUM PERFRINGENS Ab x-ray: gas in GB wall PERFORATION risk EMERGENT CHOLECYSTECOMY or percutaneous drain if unstable |
|
|
Charcot's triad
|
Charcot's triad =
RUQ pain Fever Jaundice |
|
|
Reynold's pentad is _, suggests _
|
Reynold's pentad suggests SEPSIS 2/2 cholangitis
RUQ pain Fever Jaundice Mental status changes Shock Chylovenous reflux @ 20 mmHg -> systemic bacteremia |
|
|
Choledochal cysts:
Gender Geography _% extrahepatic _% cancer risk (cancer _) |
Choledochal cysts:
-Females in Asia, Japan -occurs during uterine development. poss 2/2 reflux of pancreatic enzymes 2/2 bad angle of insertion 9-0% extrahepatic -15% cancer risk (cholangiocarcinoma) |
|
|
Type 1 _ = fusiform or saccular dilation of extrahepatic ducts
Tx: _ |
Type 1 CHOLEDOCHAL CYST (85%) = fusiform or saccular dilation of extrahepatic ducts
Tx: CYST EXCISION + HEPATOCOJEJUNOSTOMY or CHOLECYSTECTOMY Type 2: isolated diverticulum protruding from CBD => same surgery Type 3/choledochocele: dilatation of duodenal portion of CBD or where pancreatic duct meets => NO surgery Type 4 (10%): dilation of intra- and extra-hepatic CBD=> same surgery +/- hepatectomy Type 5/Caroli's dz: cystic dilation of intrahepatic ducts => poss hepatectomy. liver TRANSPLANT if diffuse |
|
|
Type _ choledochal cyst = partially intrahepatic
Tx: _ |
Type 1 CHOLEDOCHAL CYST (85%) = fusiform or saccular dilation of extrahepatic ducts
Tx: CYST EXCISION + HEPATOCOJEJUNOSTOMY or CHOLECYSTECTOMY Type 2: isolated diverticulum protruding from CBD => same surgery Type 3/choledochocele: dilatation of duodenal portion of CBD or where pancreatic duct meets => NO surgery Type 4 (10%): dilation of intra- and extra-hepatic CBD=> same surgery +/- hepatectomy Type 5/Caroli's dz: cystic dilation of intrahepatic ducts => poss hepatectomy. liver TRANSPLANT if diffuse |
|
|
Type _ choledochal cyst = totally intrahepatic
(AKA _) Tx: _ |
Type 1 CHOLEDOCHAL CYST (85%) = fusiform or saccular dilation of extrahepatic ducts
Tx: CYST EXCISION + HEPATOCOJEJUNOSTOMY or CHOLECYSTECTOMY Type 2: isolated diverticulum protruding from CBD => same surgery Type 3/choledochocele: dilatation of duodenal portion of CBD or where pancreatic duct meets => NO surgery Type 4 (10%): dilation of intra- and extra-hepatic CBD=> same surgery +/- hepatectomy Type 5/Caroli's dz: cystic dilation of intrahepatic ducts => poss hepatectomy. liver TRANSPLANT if diffuse |
|
|
In utero bad angle of insertion -> abnl reflux of pancreatic enzymes during development ->
Infant c/ _ Symptoms |
Type 1 CHOLEDOCHAL CYST (85%) = fusiform or saccular dilation of extrahepatic ducts
Tx: CYST EXCISION + HEPATOCOJEJUNOSTOMY or CHOLECYSTECTOMY Type 2: isolated diverticulum protruding from CBD => same surgery Type 3/choledochocele: dilatation of duodenal portion of CBD or where pancreatic duct meets => NO surgery Type 4 (10%): dilation of intra- and extra-hepatic CBD=> same surgery +/- hepatectomy Type 5/Caroli's dz: cystic dilation of intrahepatic ducts => poss hepatectomy. liver TRANSPLANT if diffuse |
|
|
Antibiotic _ can -> gallbladder sludging, cholestatic jandice
|
CEFTRIAXONE can -> gallbladder sludging, cholestatic jandice
|
|
|
_ = speckled cholesterol deposits on gallbladder wall
|
Cholesterolosis = speckled cholesterol deposits on gallbladder wall
|
|
|
Up to _% of pts c/ cirrhosis develop hernia of anterior ab wall
-4 complications Main RF for peritonitis (and therefore op indication) = _ -_% recurrence if ascites not medically controlled afterward -Can use _ pre-op to reduce production of ascites |
Up to 20% of pts c/ cirrhosis develop hernia of anterior ab wall
Complications :hemorrhage 2/2 variceal disruption, peritnitis, post-op asictes leak, heaptic decompensation Ascites leak = main RF for peritonitis (and therefore op indication) -73% recurrence if ascites not medically controlled afterward -can use TIPS pre-op to reduce ascites production |
|
|
Pt undergoing routine lap chole suddenly develops hypotension, tachycardia, drop in end-tidal CO2, but (+) breath sounds
-Suspect _ -Tx is _ |
CO2 embolus
-End-tidal CO2 reflects CO2 exchange from blood to alveolus -> sudden decrease suggests disconnection from vent, air embolus -Trendelenburg, L side down, increase minute ventilation (absorb CO2 faster), 100% O2 (O2 absorbed faster than CO2 -> O2 comes into equilibrium with CO2 within embolus, can get absorbed) -If CPR needed, should go on a long time to allow reabsorbtion of embolus |
|
|
2 coagulation factors not made in liver….
|
vWF + Factor 8 are not made in liver
(made in endothelium) |
|
|
what bile duct anatomic variant present in 10% of patients is a big contributor to CBD injuries?
|
10% of patients a RIGHT POSTERIOR duct (from segment 6 or &) than enters the CBD separately =>
confused for cystic duct during cholecystectomy -if injured and >2 mm, need to open + do hepaticojejunostomy |
|
|
42 y/o female for lap chole, found to have a segment of common bile duct in when you look as the specimen. What is the most appropriate treatment?
|
Immediate reconstruction with biliary enteric anastamosis.
-Simple CBD injury found intraop => primary repair +/- stent -Major CBD injury found intraop =>roux-en-y HEPATICO-JEJUNOSTOMY (or sometimes choledocho-jejunostomy) -CBD injury found late => place a PTC, then hepatico-jejunostomy 6 weeks later. |
|
|
most common variant of common hepatic artery (2%) = _
|
most common variant of common hepatic artery = off SMA (2%)
|
|
|
aberrant __ artery can be mistaken for cystic artery during lap chole
|
CYSTIC ARTERY.
Up to 75% of blood flow comes from portal vein, the rest from hepatic artery. Most of blood supply to metastasis comes from hepatic artery. Gastroduodenal artery is a landmark for dividing common form proper hepatic artery. Hepatic artery provides more blood to bile ducts than the portal veins. Ligation of right hepatic artery, mistake for cystic artery, is an important cause of lap chole complication. |
|
|
"
|
endoscopic stenting and percutaneous fluid drainage
|
|
|
Crohns patient presents c/ duodenal obstruction, failed medical mgmt.
-what is the treatment |
Crohn's + duodenal obstruction, failed medical mgmt =>
GASTROJEJUNOSOMY in most cases (if distal, could do side-to-side duodeno-jejunostomy) unlike rest of sm bowel, stricturoplasty very difficult unless very short segment and resection not possible short of a Whipple |
|
|
Liver abscess that has:
(+) Casoni skin test (+) indirect hemagglutination Tx is _ |
Echinococcus liver abscess (hydatid cyst):
(+) Casoni skin test (+) indirect hemagglutination -Sheep are carriers. Humans exposed by dogs. -RIGHT > left liver lobe. -CT: ectocyst (calcified) + endocyst -Do not aspirate (risk for anaphyaxis) Tx: Pre-op albendazole (+ ERCP if jaundice, LFTs, or cholangitis to r/o biliary communcation) -> surgical removal of cyst -may inject alcohol before excision. make sure entire wall is excised. |
|
|
Echinococcus liver cyst:
Do pre-op _ to check for _ if jaundice, high LFTs, or cholangitis |
Echinococcus liver abscess (hydatid cyst):
(+) Casoni skin test (+) indirect hemagglutination -Sheep are carriers. Humans exposed by dogs. -RIGHT > left liver lobe. -CT: ectocyst (calcified) + endocyst -Do not aspirate (risk for anaphyaxis) Tx: Pre-op albendazole (+ ERCP if jaundice, LFTs, or cholangitis to r/o biliary communcation) -> surgical removal of cyst -may inject alcohol before excision. make sure entire wall is excised. |
|
|
Liver abscess c/ CT showing ectocyst (calcified) and endocyst
|
Echinococcus liver abscess (hydatid cyst):
(+) Casoni skin test (+) indirect hemagglutination -Sheep are carriers. Humans exposed by dogs. -RIGHT > left liver lobe. -CT: ectocyst (calcified) + endocyst -Do not aspirate (risk for anaphyaxis) Tx: Pre-op albendazole (+ ERCP if jaundice, LFTs, or cholangitis to r/o biliary communcation) -> surgical removal of cyst -may inject alcohol before excision. make sure entire wall is excised. |
|
|
Echinococcus:
_ = animal carrier _ = animal transmission to human |
Echinococcus liver abscess (hydatid cyst):
(+) Casoni skin test (+) indirect hemagglutination -Sheep are carriers. Humans exposed by dogs. -RIGHT > left liver lobe. -CT: ectocyst (calcified) + endocyst -Do not aspirate (risk for anaphyaxis) Tx: Pre-op albendazole (+ ERCP if jaundice, LFTs, or cholangitis to r/o biliary communcation) -> surgical removal of cyst -may inject alcohol before excision. make sure entire wall is excised. |
|
|
Echinococcus liver cyst:
_ lobe = most common |
Echinococcus liver abscess (hydatid cyst):
(+) Casoni skin test (+) indirect hemagglutination -Sheep are carriers. Humans exposed by dogs. -RIGHT > left liver lobe. -CT: ectocyst (calcified) + endocyst -Do not aspirate (risk for anaphyaxis) Tx: Pre-op albendazole (+ ERCP if jaundice, LFTs, or cholangitis to r/o biliary communcation) -> surgical removal of cyst -may inject alcohol before excision. make sure entire wall is excised. |
|
|
If pt undergoing cholecystectomy has jaundice, cholangitis, pancreatitis, high bili, high AST/ALT, stone in CBD on US
|
Pre-op ERCP if: jaundice, cholangitis, gallstone pancreatitis, high bili, high AST/ALT, stone in CBD on US
<5% of pts undergoing cholecystectomy have retained CBD stone, 95% of these cleared c/ ERCP |
|
|
Air in biliary tree
Most common culprit is _ 2 other possible causes |
Air in biliary tree
Usually after ERCP + sphincterotomy Also 2/2 cholangitis, gallstone ileus (gallstone erosion into duodenum) |
|
|
Esophageal varices:
1st line tx for bleed 2 drugs |
Esophageal varices:
Sclerotherapy 90% effective @ stopping bleed = 1st line tx Octreotide, Vasopressin |
|
|
Pt c/ bleeding esophageal varix + hx CAD is on vasopressin
Need to also give_ |
Pt c/ bleeding esophageal varix + hx CAD is on vasopressin
Need to also give NTG |
|
|
Esophageal varices:
_% mortality c/ 1st bleed |
Esophageal varices: from short gastrics to azygos
30% mortality c/ 1st bleed |
|
|
Esophageal varices:
Drug _ may help prevent rebleed |
Esophageal varices: from short gastrics to azygos
PROPRANOLOL may help prevent rebleed |
|
|
Esophageal varices:
Complication of sclerotx is _ Treat c/ _ |
Esophageal varices: from short gastrics to azygos
Complication of sclerotx = stricture Treat c/ dilation |
|
|
Esophageal varices:
Tx for refractory bleeding (despite sclerotx) |
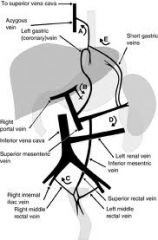
Esophageal varices: from short gastrics to azygos
Refractory bleeding (despite sclerotx) -> TIPS |
|
|
Esophageal varices:
_% mortality c/ 1st bleed _% will rebleed _% mortality c/ each subsequent episode |
Esophageal varices:
30% mortality c/ 1st bleed 50% will rebleed 50% mortality c/ each subsequent episode |
|
|
where is the falciform ligament located?
|
FALCIFORM LIGAMENT
Separates medial (1+4) + lateral (2+3) segments of L lobe Attaches liver to anterior ab wall extends to umbilicus + carries remnant of umbical vein from the underside of liver AKA LIGAMENTUM TERES |
|
|
Benign liver tumor c/ (+) uptake on sulfer colloid scan = _
|
Focal nodular hyperplasia:
NO malignant potential. Very unlikely to rupture. -Dx ab CT (or MRI) => hypervascular tumor c/ CENTRAL STELLATE SCAR that can look like cancer -Often have an overt feeding artery -KUPFFER cells => increased uptake on SULFUR COLLOID SCAN -Tx: no surgery unless symptomatic |
|
|
Focal nodular hyperplasia:
Risk of malignancy? |
Focal nodular hyperplasia:
NO malignant potential. Very unlikely to rupture. -Dx ab CT (or MRI) => hypervascular tumor c/ CENTRAL STELLATE SCAR that can look like cancer -Often have an overt feeding artery -KUPFFER cells => increased uptake on SULFUR COLLOID SCAN -Tx: no surgery unless symptomatic |
|
|
Focal nodular hyperplasia:
Tx_ |
Focal nodular hyperplasia:
NO malignant potential. Very unlikely to rupture. -Dx ab CT (or MRI) => hypervascular tumor c/ CENTRAL STELLATE SCAR that can look like cancer -Often have an overt feeding artery -KUPFFER cells => increased uptake on SULFUR COLLOID SCAN -Tx: no surgery unless symptomatic |
|
|
Benign liver tumor c/ central stellate scar that can look like cancer
|
Focal nodular hyperplasia:
NO malignant potential. Very unlikely to rupture. -Dx ab CT (or MRI) => hypervascular tumor c/ CENTRAL STELLATE SCAR that can look like cancer -Often have an overt feeding artery -KUPFFER cells => increased uptake on SULFUR COLLOID SCAN -Tx: no surgery unless symptomatic |
|
|
liver mass with increased uptake on sulfur colloid scan
-Suspect _ |
Focal nodular hyperplasia:
NO malignant potential. Very unlikely to rupture. -Dx ab CT (or MRI) => hypervascular tumor c/ CENTRAL STELLATE SCAR that can look like cancer -Often have an overt feeding artery -KUPFFER cells => increased uptake on SULFUR COLLOID SCAN -Tx: no surgery unless symptomatic |
|
|
liver mass with central stellate scar on imaging
-Suspect _ |
Focal nodular hyperplasia:
NO malignant potential. Very unlikely to rupture. -Dx ab CT (or MRI) => hypervascular tumor c/ CENTRAL STELLATE SCAR that can look like cancer -Often have an overt feeding artery -KUPFFER cells => increased uptake on SULFUR COLLOID SCAN -Tx: no surgery unless symptomatic |
|
|
A 42yo female with no history of cirrhosis presents for referral concerning a 1.5cm liver lesion. Contrast enhanced CT showed a mass with a “central scar.” Follow-up nuclear medicine scan demonstrated increased uptake. The most likely diagnosis is:
|
Hemangiomas have characteristic findings on CT that are diagnostic. Contrast enhanced CT will demonstrate peripheral nodular enhancement and progressive centripetal fill-in. Hepatocellular carcinoma (HCC) is most commonly diagnosed in the setting of cirrhosis. HCC is most easily seen during the arterial phase of contrast enhanced CT. This lesion is characterized as a hyper-vascular lesion with early filling. Simple cysts are demonstrated on CT as fluid-filled structures with thin, non-enhancing walls and absent internal septations. Liver Cell Adenomas and Focal Nodular Hyperplasia (FNH) can appear similar on CT imaging, however, the presence of Kupffer cells in FNH (which are usually absent in adenoma) allow uptake of sulfa-colloid and therefore have an enhanced appearance on Technetium scan
|
|
|
in the foramen of Winslow.
|
Foramen of Winslow = omental foramen:
-B/w lesser + greater omentum Portal triad is anterior IVC is posterior Duodenum is inferior Liver is superior |
|
|
laparoscopic cholecystectomy is contraindicated in a patient with_
|
GB adenocarcinoma:
-Rare but #1 cancer of biliary tract (4x more common than cholangiocarcinoma) -Liver = #1 site for mets -Porcelain GB => 10-20% risk of cancer. need cholecystectomy. -1st spreads to segments 4, 5,. 1st nodes = cystic duct nodes. (R) -Sx jaundice -> RUQ pain -Stage 1a (mucosa only) => cholecystectomy -Into muscle (stage 2) => wedge segments 4,5 + LN stripping along portal triad -Stage 3=> wide resection around liver bed @ segments 4, 5 c/ 2-3 cm margins. regional LNs inc. portal triad. +/- Whipple, lobectomy, or CBD resection -90% PRESENT C/ STAGE 4 -LAP CHOLE CONTRAINDICATED 2/2 risk of tumor implants @ trocar sites -5% 5-yr survival |
|
|
After laparoscopic cholecystectomy, frozen section reveals cancer that has invaded the muscular layer. What additional treatment would be appropriate
|
Wedge resection of segments 4, 5 + stripping of LNs along portal triad (not formal anatomic lobe resection)
Gallbladder cancer invaded into the muscular layer = T1b = more likely to have extended into the adjacent hepatic parenchyma. (Simple cholecystectomy appropriate for Tis and T1a lesions) Consider adjuvant chemo or XRT AFTER surgical resection. |
|
|
gallbladder anatomy:
GB concentrates bile by active resorption of __, __; __ then follows |
gallbladder anatomy:
GB concentrates bile by active resorption of Na, Cl; H20 then follows |
|
|
Gallbladder polyps:
-Worrisome if > _cm or pt >_ years old Tx: _ |
Gallbladder polyps:
-Worrisome for malignancy if > 1cm or pt >60 years old Tx: cholecystectomy |
|
|
<_% of pts undergoing cholecystectomy have retained CBD stone
_% of CBD stones are cleared c/ ERCP |
<5% of pts undergoing cholecystectomy have retained CBD stone, 95% of these cleared c/ ERCP
|
|
|
If pt being considered for cholecystectomy is very ill, may want to do _ instead
|
If pt undergoing cholecystectomy is very ill, may want to do place CHOLECYSTOSTOMY tube => do surgery when pt healthy
|
|
|
Gallstone ileus:
_ = #1 site of obstruction 2/2 fistual b/w _ Dx by _ Tx |
Gallstone ileus:
-Fistula b/w GB + 2nd portion of duodenum releases stone -> SB obstruction, most commonly in TERMINAL ILEUM -Ab x-ray: pneumobilia -Tx: ex lap + enterotomy prox to obstruction to remove stone -> cholecystectomy + fistula resection/closure if pt can tolerate (if pt too sick, leave GB and fistula) |
|
|
Pt presents c/ crampy ab pain
-Plain film shows air-fluid levels, pneumobilia, colon decompressed -No hx biliary surgery -Suspect _ -Tx is _ |
Gallstone ileus:
-Fistula b/w GB + 2nd portion of duodenum releases stone -> SB obstruction, most commonly in TERMINAL ILEUM -Ab x-ray: pneumobilia -Tx: ex lap + enterotomy prox to obstruction to remove stone -> cholecystectomy + fistula resection/closure if pt can tolerate (if pt too sick, leave GB and fistula) |
|
|
What is the recommended standard of care in the treatment of gallstone pancreatitis?
|
Gallstone Pancreatitis: 3-8% of symptomatic cholelithiasis.
-Tx: fluids, early nutritional support, +/- hemodynamic and ventilatory support. NG drainage if ileus. -ERCP and sphincterotomy may be necessary to relieve the biliary obstruction. -Intraoperative cholangiography if there is suspected or documented choledocholithiasis. -Recurrent biliary pancreatitis in 34-56% within 6 weeks. -Cholecystectomy after the resolution of acute pancreatitis but before hospital discharge |
|
|
Gallstone in fat person is likely 2/2 _
|
Gallstone in fat person is likely 2/2
overactive HMG CoA reductase (HMG CoA + HMG CoA reductase -> cholesterol Cholesterol + 7-alpha-hydroxylase -> bile acids) |
|
|
Gallstone in a thin person is likely 2/2:
over/underactive? 7-alpha-hydroxylase/HMG Co-A reductase? |
Gallstone in a thin person is likely 2/2 underactive 7-alpha-hydroxylase
(HMG CoA + HMG CoA reductase -> cholesterol Cholesterol + 7-alpha-hydroxylase -> bile acids) |
|
|
_% of gallstones are radiopaque
|
10% of gallstones are radiopaque
|
|
|
Gallstones occur in _% of population
Most asymptomatic |
Gallstones occur in 10% of population
Most asymptomatic |
|
|
Patient with a primary common bile duct stone (formed in the CBD) likely has a _-type stone
The stone type is usually 2/2 _, causing _, which creates the stone Tx = _ |
Patient with a primary common bile duct stone (formed in the CBD) likely has a BROWN stone
Infection-> deconjugation of bili E. coli most common, makes beta-glucuronidase, which deconjugates bili, forms Ca bilirubinate Most common in Asians Most need a biliary drainage procedure - sphincteroplasty |
|
|
_ type gallstones are 2/2 hemolytic disorders, cirrhosis, TPN, ileal resection
(increased bili, low liver fx, bile stasis) Form in _ Tx is _ |
BLACK stones
2/2 hemolytic disorders, cirrhosis, TPN, ileal resection (increased bili, low liver fx, bile stasis) Form in gallbladder Tx = cholecystectomy |
|
|
75% of gallstones in US are type _
Mechanism by which they form _ Due to low levels of _, _ Form in _ |
Non-pigmented stones = 75% in US
Low lecithin, bile acids -> cholesterol insolubilization (stasis, Ca nucleation by mucin glycoproteins, increased water resorption by GB) Form in gallbladder |
|
|
Pigmented stones = _% of gallstones in US
Formed by solubilization of _ c/ precipitation of _, _ Are dissolution agents a good therapy? |
Pigmented stones = 25% of gallstones in US
(majority of gallstones worldwide) Solubilization of UNconjugated bili c/ precipitation of Ca bilirubinate, insoluble salts Dissolution agents don't work (mono-octanoin) |
|
|
Most pt's c/ _-type gallstones need a bilary drainage procedure - sphincteroplasty (90% successful)
This stone type typically forms in CBD Need to check for ampullary stenosis, duodenal diverticula, abnl sphincter of Oddi |
Most pt's c/ BROWN stones need a bilary drainage procedure - sphincteroplasty (90% successful)
This stone type typically forms in CBD Need to check for ampullary stenosis, duodenal diverticula, abnl sphincter of Oddi |
|
|
Best tx for late CBD stone is _
_ procedure allows for removal of stone 3 main risks of procedure are _ |
ERCP = best tx for late CBD stone is
Sphincterotomy allows stone removal c/ graspers 3 main risks = bleeding, pancreatitis, perforation |
|
|
C. sinensis, A. lumbricoides, T trichura, E. coli cause liver dz _
|
C. sinensis, A. lumbricoides, T trichura, E. coli ->
CBD stones -> recurrent cholangitis -> oriental cholangiohepatitis |
|
|
Which GI hormone?
-GB contraction -Pancreatic enzyme release -Relaxation of sphincter of Oddi -Some increase in intestinal motility |
Cholecystokinin:
-AA's, fatty acids in SB > CCK released from I cells of duodenum, jejunum -GB contraction -Pancreatic enzyme release -Relaxation of sphincter of Oddi -Some increase in intestinal motility |
|
|
Which GI hormone?:
-Inhibits HCl and gastrin release in stomach -Increases bile flow -Increases pancreatic HCO3- release |
Secretin:
-Fat, bile, pH <4 -> released from S cells of duodenum -Inhibits HCl and gastrin release in stomach -Increases bile flow -Increases pancreatic HCO3- release -Gastrinoma => secretin injection increases gastrin release |
|
|
_ = benign neuroectoderm tumor that can occur in biliary tract
-Sx -Tx |
GRANULAR CELL MYOBLASTOMA = benign neuroectoderm tumor that can occur in biliary tract
-Sx like cholecystitis -Tx: cholecystectomy |
|
|
#1 benign hepatic tumor = _
|
#1 benign hepatic tumor = HEMANGIOMA
-Most asymptomatic. Rupture rare. F > M -Do not bx (risk of hemorrhage) -MRI (better), CT: hypervascular c/ peripheral to central enhancement. -Tx if symptomatic => surgery +/- embolization. Steroids + XRT if unresectable. -Kasabach--Merritt syndome = rare complication, more common in kids = consumptive coagulopathy, thrombocytopenia -CHF 2/2 AV shunting -Large hemangioma in child should be resected |
|
|
Benign liver tumor c/ peripheral to central enhancement on MRI, CT
|
#1 benign hepatic tumor = HEMANGIOMA
-Most asymptomatic. Rupture rare. F > M -Do not bx (risk of hemorrhage) -MRI (better - hot on T2), CT: hypervascular c/ peripheral to central enhancement. -Tx if symptomatic => surgery +/- embolization. Steroids + XRT if unresectable. -Kasabach--Merritt syndome = rare complication, more common in kids = consumptive coagulopathy, thrombocytopenia -CHF 2/2 AV shunting -Large hemangioma in child should be resected |
|
|
Hemangioma:
Tx is _ |
#1 benign hepatic tumor = HEMANGIOMA
-Most asymptomatic. Rupture rare. F > M -Do not bx (risk of hemorrhage) -MRI (better), CT: hypervascular c/ peripheral to central enhancement. -Tx if symptomatic => surgery +/- embolization. Steroids + XRT if unresectable. -Kasabach--Merritt syndome = rare complication, more common in kids = consumptive coagulopathy, thrombocytopenia -CHF 2/2 AV shunting -Large hemangioma in child should be resected |
|
|
Hemangioma:
Tx for symptomatic, unresectable cases |
#1 benign hepatic tumor = HEMANGIOMA
-Most asymptomatic. Rupture rare. F > M -Do not bx (risk of hemorrhage) -MRI (better), CT: hypervascular c/ peripheral to central enhancement. -Tx if symptomatic => surgery +/- embolization. Steroids + XRT if unresectable. -Kasabach--Merritt syndome = rare complication, more common in kids = consumptive coagulopathy, thrombocytopenia -CHF 2/2 AV shunting -Large hemangioma in child should be resected |
|
|
Hemangioma:
2 rare complications Population most commonly seen in _ |
#1 benign hepatic tumor = HEMANGIOMA
-Most asymptomatic. Rupture rare. F > M -Do not bx (risk of hemorrhage) -MRI (better), CT: hypervascular c/ peripheral to central enhancement. -Tx if symptomatic => surgery +/- embolization. Steroids + XRT if unresectable. -Kasabach--Merritt syndome = rare complication, more common in kids = consumptive coagulopathy, thrombocytopenia -CHF 2/2 AV shunting -Large hemangioma in child should be resected |
|
|
Hemangioma:
most common population |
#1 benign hepatic tumor = HEMANGIOMA
-Most asymptomatic. Rupture rare. F > M -Do not bx (risk of hemorrhage) -MRI (better), CT: hypervascular c/ peripheral to central enhancement. -Tx if symptomatic => surgery +/- embolization. Steroids + XRT if unresectable. -Kasabach--Merritt syndome = rare complication, more common in kids = consumptive coagulopathy, thrombocytopenia -CHF 2/2 AV shunting -Large hemangioma in child should be resected |
|
|
liver mass with peripheral to central enhancement on imaging
-Suspect _ |
#1 benign hepatic tumor = HEMANGIOMA
-Most asymptomatic. Rupture rare. F > M -Do not bx (risk of hemorrhage) -MRI (better), CT: hypervascular c/ peripheral to central enhancement. -Tx if symptomatic => surgery +/- embolization. Steroids + XRT if unresectable. -Kasabach--Merritt syndome = rare complication, more common in kids = consumptive coagulopathy, thrombocytopenia -CHF 2/2 AV shunting -Large hemangioma in child should be resected |
|
|
#1 liver tumor = _
|
Hemangioma is the most common benign tumor affecting the liver, followed by focal nodular hyperplasia (FNH). Hepatic hemangiomas are mesenchymal in origin and usually are solitary. They should be resected if symptomatic e.g. bleeding
|
|
|
The most common benign neoplasm of the liver is _
|
Hemangioma = #1 benign tumor of the liver.
-3:1 F:M, mean age 45. -Majority require no surgery. -Indications for resection: rupture, change in size, and development of the Kasabach-Merritt syndrome (thrombocytopenia and consumptive coagulopathy) |
|
|
Pt presents c/ UGI bleed, jaundice, RUQ pain
50% of cases are after trauma Also 2/2 4 other things Dx by _ Tx is _ |
HEMOBILIA (bile duct - hepatic arterial fistula)
UGI bleed, jaundice, RUQ pain 50% after trauma Also 2/2 infection, gallstones, aneurysm, tumors Dx: ANGIOGRAM Tx: ANGIOGRAM + EMBOLIZATION -> SURGERY = 2nd line |
|
|
Hemobilia triad is ...
|
"Haemobilia:
-2/2 fistula b/w a vessel of the splanchnic circulation and the intra- or extrahepatic biliary system. -TRIAD present in 22% of cases = GI BLEED, JAUNDICE, RUQ PAIN -next step = ARTERIOGRAM + EMBOLIZATION -Endoscopic trans-arterial embolisation (TAE) = catheterization of a hepatic artery, then embolic occlusion. Surgery is indicated when TAE has failed or sepsis present in biliary tree or drainage has failed. |
|
|
Hemochromatosis:
RF for 2 liver cancers… |
Hemochromatosis = RF for:
Hepatocellular ca Cholangiosarcoma |
|
|
Which liver lesion:
-"cold" on liver scan -Malignant potential -10% risk of rupture/bleed -Tx is _ |
Hepatic adenoma:
Pop women, steroid use, OCPs, type 1 collagen storage dz -80% symptomatic (pain, increased LFTs, palpable mass), 10-20% risk of rupture/bleed -Malignant potential -RIGHT >left lobe -Dx: hypervascular tumor on MRI, peripheral blood supply. Cold on sulfur colloid scan. -If asymptomatic, stop OCPs, monitor. Resect if no regression -If symptomatic, resect b/c of malignancy and bleeding risk. Embolize if multiple/unresectable |
|
|
Type 1 collagen storage dz = RF for benign liver tumor_
|
Hepatic adenoma:
Pop women, steroid use, OCPs, type 1 collagen storage dz -80% symptomatic (pain, increased LFTs, palpable mass), 10-20% risk of rupture/bleed -Malignant potential -RIGHT >left lobe -Dx: hypervascular tumor on MRI, peripheral blood supply. Cold on sulfur colloid scan. -If asymptomatic, stop OCPs, monitor. Resect if no regression -If symptomatic, >4 cm, unable to stop OCPs, or planning to become pregnant, resect b/c of malignancy and bleeding risk. Embolize if multiple/unresectable |
|
|
Hepatic adenoma:
_% asymptomatic |
Hepatic adenoma:
Pop women, steroid use, OCPs, type 1 collagen storage dz -80% symptomatic (pain, increased LFTs, palpable mass), 10-20% risk of rupture/bleed -Malignant potential -RIGHT >left lobe -Dx: hypervascular tumor on MRI, peripheral blood supply. Cold on sulfur colloid scan. -If asymptomatic, stop OCPs, monitor. Resect if no regression -If symptomatic, >4 cm, unable to stop OCPs, or planning to become pregnant, resect b/c of malignancy and bleeding risk. Embolize if multiple/unresectable |
|
|
Hepatic adenoma:
_-_% risk of rupture/bleed |
Hepatic adenoma:
Pop women, steroid use, OCPs, type 1 collagen storage dz -80% symptomatic (pain, increased LFTs, palpable mass), 10-20% risk of rupture/bleed -Malignant potential -RIGHT >left lobe -Dx: hypervascular tumor on MRI, peripheral blood supply. Cold on sulfur colloid scan. -If asymptomatic, stop OCPs, monitor. Resect if no regression -If symptomatic, >4 cm, unable to stop OCPs, or planning to become pregnant, resect b/c of malignancy and bleeding risk. Embolize if multiple/unresectable |
|
|
Hepatic adenoma:
Most common in _ lobe |
Hepatic adenoma:
Pop women, steroid use, OCPs, type 1 collagen storage dz -80% symptomatic (pain, increased LFTs, palpable mass), 10-20% risk of rupture/bleed -Malignant potential -RIGHT >left lobe -Dx: hypervascular tumor on MRI, peripheral blood supply. Cold on sulfur colloid scan. -If asymptomatic, stop OCPs, monitor. Resect if no regression -If symptomatic, >4 cm, unable to stop OCPs, or planning to become pregnant, resect b/c of malignancy and bleeding risk. Embolize if multiple/unresectable |
|
|
Hepatic adenoma:
Malignant potential? |
Hepatic adenoma:
Pop women, steroid use, OCPs, type 1 collagen storage dz -80% symptomatic (pain, increased LFTs, palpable mass), 10-20% risk of rupture/bleed -Malignant potential -RIGHT >left lobe -Dx: hypervascular tumor on MRI, peripheral blood supply. Cold on sulfur colloid scan. -If asymptomatic, stop OCPs, monitor. Resect if no regression -If symptomatic, >4 cm, unable to stop OCPs, or planning to become pregnant, resect b/c of malignancy and bleeding risk. Embolize if multiple/unresectable |
|
|
Hepatic adenoma:
Tx if asymptomatic |
Hepatic adenoma:
Pop women, steroid use, OCPs, type 1 collagen storage dz -80% symptomatic (pain, increased LFTs, palpable mass), 10-20% risk of rupture/bleed -Malignant potential -RIGHT >left lobe -Dx: hypervascular tumor on MRI, peripheral blood supply. Cold on sulfur colloid scan. -If asymptomatic, stop OCPs, monitor. Resect if no regression -If symptomatic, >4 cm, unable to stop OCPs, or planning to become pregnant, resect b/c of malignancy and bleeding risk. Embolize if multiple/unresectable |
|
|
Hepatic adenoma:
Tx if symptomatic (pain, elevated LFTs, palpable mass |
Hepatic adenoma:
Pop women, steroid use, OCPs, type 1 collagen storage dz -80% symptomatic (pain, increased LFTs, palpable mass), 10-20% risk of rupture/bleed -Malignant potential -RIGHT >left lobe -Dx: hypervascular tumor on MRI, peripheral blood supply. Cold on sulfur colloid scan. -If asymptomatic, stop OCPs, monitor. Resect if no regression -If symptomatic, >4 cm, unable to stop OCPs, or planning to become pregnant, resect b/c of malignancy and bleeding risk. Embolize if multiple/unresectable |
|
|
Benign liver tumor c/ (-) uptake on sulfer colloid scan = _
|
Hepatic adenoma:
Pop women, steroid use, OCPs, type 1 collagen storage dz -80% symptomatic (pain, increased LFTs, palpable mass), 10-20% risk of rupture/bleed -Malignant potential -RIGHT >left lobe -Dx: hypervascular tumor on MRI, peripheral blood supply. Cold on sulfur colloid scan. -If asymptomatic, stop OCPs, monitor. Resect if no regression -If symptomatic, resect b/c of malignancy and bleeding risk. Embolize if multiple/unresectable |
|
|
How does lactulose work?
2 mechanisms |
Lactulose:
1. cathartic that removes bacteria from gut 2. acidifies colon -> converts NH3 to ammonium -> prevents uptake |
|
|
3 drug classes that can treat hepatic encephalopathy
|
Tx of hepatic encephalopathy:
-Lactulose: reduce gut bacteria, acidify gut to convert NH3-> NH4 -Neostigmine -Dopamine R agonists: L-dopa, bromocriptine |
|
|
Hepatic encephalopathy tx:
May need to embolize (2 areas) |
Hepatic encephalopathy tx:
May need to embolize previous therapeutic shunts, other major collaterals |
|
|
liver lesion which may present c/ Kasaback-Merritt syndrome
|
Hepatic hemangioma:
-Tx: do nothing unless giant/symptomatic/consumptive -Kasaback-Merritt syndrome = hemangioma thrombocytopenia syndrome. presents c/ consumptive coagulopathy. most common in babies -Pts can also have CHF |
|
|
Hepatic sarcoma:
RFs Prognosis |
Hepatic sarcoma:
RFs: PVC, thorotrast (x-ray contrast medium), arsenic RAPIDLY FATAL |
|
|
PVC = RF for cancer _
|
PVC = RF for HEPATIC SARCOMA
(rapidly fatal) |
|
|
Thorotrast (x-ray contrast medium) = RF for cancer _
|
Thorotrast = RF for HEPATIC SARCOMA
(rapidly fatal) |
|
|
Arsenic = RF for cancer _
|
HEPATIC SARCOMA
RF's: Thorotrast (former contrast medium), arsenic, PVC (rapidly fatal) |
|
|
Post-partum liver failure c/ ascites is 2/2 _
Dx by _ |
Relative hypercoagulable state after pregnancy (higher risk if pre-exisiting hypercoalulability) ->
HEPATIC VEIN THROMBOSIS -> post-partum liver failure c/ ascites Dx: SMA arteriogram c/ venous phase contrast (more sensitive than MRI) |
|
|
3 types of viral hepatitis can cause chronic hepatitis, hepatoma
|
hepatitis B, C, D can cause chronic hepatitis, hepatoma
|
|
|
Hep A is a DNA or RNA virus?
|
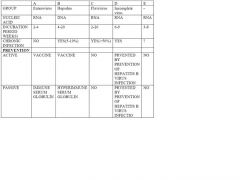
Hep A is an RNA virus
PICORNAvirus |
|
|
Hep B:
Antibody type _ dominates for 1st 6 mo |
Hep B:
IgM dominates for 1st 6 mo (check for Anti-HBc-IgM = anti-core Ab) IgG then takes over |
|
|
Hep B: IgM dominates for 1st 6 mo
Anti-_ rises 10-12 wks after infection Anti-_ rises 12-14 wks after infection Anti-_ rises 14-16 wks after infection |
Hep B: IgM dominates for 1st 6 mo
Anti-HBc rises 10-12 wks after infection Anti-HBe rises 12-14 wks after infection Anti-HBs rises 14-16 wks after infection |
|
|
HepB vaccination -> elevated Anti-_ Ab
|
HepB vaccination -> elevated anti-HBs (surface) only
|
|
|
HepC = RNA or DNA virus?
|
HepC = RNA virus
FLAVIvirus |
|
|
Hep_ -> fulminant hepatic failure in pregnancy
most often 3rd trimester DNA or RNA virus? |
HepE -> fulminant hepatic failure in pregnancy
most often 3rd trimester RNA virus = probably CALCIvirus |
|
|
What type of virus is HepD?
|
HepD = VIROID (RNA virus)
|
|
|
Only DNA viral hepatitis is …
|
HepB = only DNA viral hepatitis
HEPADNAvirus |
|
|
#1 cancer worldwide is _
|
#1 cancer worldwide = hepatocellular ca
|
|
|
#1 cause of hepatocellular ca worldwide = _
|
HepB = #1 cause of hepatocellular ca worldwide
|
|
|
Hemochromatosis: a RF for hepatocellular ca?
|
Hemochromatosis:
YES a RF for hepatocellular ca |
|
|
Aflatoxins: RF for hepatocellular ca?
|
Aflatoxins:
YES a RF for hepatocellular ca |
|
|
Steroids: a RF for hepatocellular ca?
|
Steroids:
YES a RF for hepatocellular ca |
|
|
Hepatocellular ca:
lab: _ level correlates c/ tumor size |
Hepatocellular ca:
AFP level correlates c/ tumor size (AFP >500 has very high likelihood of cancer) |
|
|
Hepatocellular ca:
_% 5-yr survival after resection |
Hepatocellular ca:
30% 5-yr survival after resection |
|
|
Hepatocellular ca:
Resection: need _cm margins Typically resectable? |
Hepatocellular ca:
1 cm margins NOT typically resectable 2/2 cirrhosis, portohepatic involvement, mets |
|
|
Hepatocellular ca:
average Met:Primary ratio is _ |
Hepatocellular ca:
average Met:Primary ratio is 1:20 |
|
|
Hepatocellular ca:
After resection, tumor recurrence is most likely in _ |
Hepatocellular ca:
After resection, tumor recurrence is most likely in LIVER |
|
|
liver lesion c/ elevated AFP and hx cirrhosis
|
hepatocellular ca:
-#1 cancer worldwide -may have high AFP -#1 cause = chronic HepB/C -Also ass'd c/ any cirrhosis: EtOH, hemochromatosis, primary biliary cirrhosis, alpha-1-antitrypsin defic, clonorchis sinensis (flukes), aflatoxin -Fibrolamellar variant => better prognosis |
|
|
Clear cell, lymphocyte infiltrative, fibrolamellar types of hepatocellar carcinoma:
Population Prognosis |
Clear cell, lymphocyte infiltrative, fibrolamellar types of hepatocellar carcinoma:
YOUNG ADULTS BEST Prognosis |
|
|
criteria for liver transplant for HCC
|
Liver tx candidate for HCC if :
-no PV or IVC involvement -tumor<5 cm -3 tumors <3 cm |
|
|
liver mass with elevated AFP
-Suspect _ |
liver mass with elevated AFP => hepatocellular ca
|
|
|
Patient c/ liver disease + pre-prenal appearance...
-Suspect _ -Tx would be _ |
Hepatorenal syndrome:
-see low urinary Na - same appearance as prerenal azotemia Tx: stop diuretics, give volume |
|
|
HIDA scan:
_ taken up by _, excreted into _ If GB not seen on HIDA => suggests _, requires tx of _ <_% of GB volume excreted over 2 hrs => suggests _ => _% benefit from cholecystectomy |
HIDA scan:
TECHNICIUM taken up by liver, excreted into GB GB not seen on HIDA => CYSTIC DUCT STONE => CHOLECYSTECTOMY <25% of GB volume excreted/2 hrs => BILIARY DYSKINESIA => 50% benefit from cholecystectomy |
|
|
Liver lesion c/ (+) Casoni skin test, (+) indirect hemaggutinin
-Tx is _ |
Hydatid cyst:
-Echinococcus -(+) casoni skin test = wheal after intradermal injection of sterilised fluid from hydatid cysts -(+) indirect hemagglutinin -CT ectocyst (calcified) and endocyst -Albendazole then resect (pericystectomy), get all of cyst wall. - do not aspirate (risk of anaphylaxis) -Preop ERCP if jaundice, increased LFTs, or cholangitis to r/o communication c/ biliary system -Can inject alcohol prior to cyst removal |
|
|
Hgb is broken down to _ -> _ -> _
|
Hgb is broken down to heme -> biliverdin -> bilirubin
|
|
|
In liver, enzyme _ conjugates bilirubin to _, which improves water solubility
|
In liver, glucuronyl transferase conjugates bilirubin + glucuronic acid -> improves water solubility
|
|
|
Bacteria in _ region of small bowel break down bilirubin to form _ -> reabsorbed in blood + secreted in urine
Urine changes to _ if excess bilirubin present |
Bacteria in terminal ileum break down bilirubin urobilinogen -> reabsorbed in blood + secreted in urine
Urine becomes dark (like cola) if excess bilirubin present |
|
|
_ = many biliary phospholipid
-solubilizes cholesterol, emulsifies fat in intestine |
lecithin = many biliary phospholipid
-solubilizes cholesterol, emulsifies fat in intestine |
|
|
Bacteria in gut dehydroxylate primary bile acids (cholic, chenodeoxycholic) to secondary bile acids _, _
|
Bacteria in gut dehydroxylate primary bile acids (cholic, chenodeoxycholic) ->
secondary bile acids: deoxycholic, lithocholic |
|
|
Bile acids are conjugated to _, _ to improve water solubility
|
Bile acids are conjugated to TAURINE, GLYCINE to improve water solubility
|
|
|
Jaundice:
tends to occur when bilirubin > _ Appears first @ _ |
Jaundice:
tends to occur when bilirubin > 2.5 Appears first under tongue |
|
|
Maximim bilirubin is _
unless pt has renal dz, hemolysis, or bile duct-hepatic vein fistula |
Maximim bilirubin is 30
unless pt has renal dz, hemolysis, or bile duct-hepatic vein fistula |
|
|
Jaundice syndrome:
abnormal uptake to bili high unconjugated bilirubinemia |
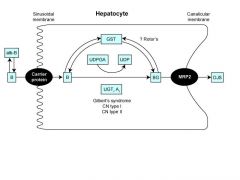
GILBERT'S disease:
abnormal uptake to bili high unconjugated bilirubinemia |
|
|
Jaundice syndrome:
inability to conjugate deficinent glucuronyl transferase high unconjugated bili life treatening |
CRIGLER-NAJJAR disease:
inability to conjugate deficinent glucuronyl transferase high unconjugated bili life treatening |
|
|
Jaundice syndrome:
immature glucouronyl transferase high unconjugated bili |
Physiologic jaundice of newborn:
immature glucouronyl transferase high unconjugated bili |
|
|
Jaundice syndrome:
deficiency in bili storage high conjugated bili |
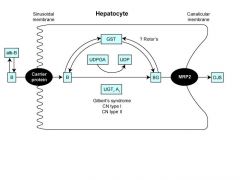
ROTOR'S syndrome:
deficiency in bili storage high conjugated bili (Gilbert's => high unconj bili) |
|
|
Jaundice syndrome:
deficiency in secretion ability high conjugated bili |
DUBIN-JOHNSON syndrome:
deficiency in secretion ability high conjugated bili |
|
|
What do Kuppfer cells do?
|
Kupffer cells = liver macrophages.
Clear portal blood. Immunosurveilance |
|
|
most common variant of L hepatic artery = off _
(travels in _) |
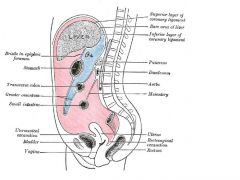
most common R hepatic artery variant = off L gastric
-travels in gastro-hepatic ligament |
|
|
What is the best way to differentiate amoebic vs. pyogenic liver abscess?
|
Serology is the gold standard to diagnosing amoebic vs. pyogenic liver abscesses. A positive fluorescent antibody test for E. histolytica is diagnostic for patient’s with suspected amebiasis.
|
|
|
Liver abscesses: #1 type (_%)
|
Liver abscesses: 80% are pyogenic
-Pyogenic cysts usually 2/2 GNRs, following intra-abdominal infection like diverticuliis, appendictis -Tx = percutaneous drainage + broad-spec abx to cover GNRs + anaerobes |
|
|
Pyogenic liver abscess:
Usually 2/2 _ (most common organism = _) Can also be 2/2 _ |
Pyogenic liver abscess: 80% of liver abscesses
RIGHT>left lobe Usually 2/2 contiguous spread from biliary tract, e.g. weeks after diverticulitis or appendicitis (E. coli = #1) Can also be 2/2 bacteremia (from diverticulitis, appendicitis) Tx: CT-guided drainage + abx. Surgical drainage if pt unstable, continued sepsis. May need surgery for biliary obstruction or multiple abscesses |
|
|
Pyogenic liver abscess:
Tx is _ |
Pyogenic liver abscess:
Tx: CT-guided drainage PLUS broad-spectrum abx (GNRs most common) Surgery if pt unstable, continued sepsis, bilary obstruction, multiple abscesses |
|
|
Pyogenic liver abscess:
more likely in _ lobe |
Pyogenic liver abscess:
more likely in R lobe |
|
|
Pyogenic liver abscess:
_ % mortality c/ sepsis |
Pyogenic liver abscess:
15% mortality c/ sepsis |
|
|
#1 common hepatic variant
|
#1 common hepatic variant = off SMA (2%)
|
|
|
#1 hepatic artery variant
|
#1 R hepatic artery variant =
off SMA (20%) coursees behind pancreas, posterp;lateral to CBD |
|
|
#1 R hepatic artery variant
|
#1 R hepatic artery variant =
off SMA in 17% -usually travels in the hepatoduodenal ligament laterally |
|
|
#1 L hepatic artery variant
|
#1 L hepatic artery variant =
off L gastric artery (10-20%) -travels in gastrohepatic ligament medially |
|
|
Liver gets symp signaling frm T_-_, parasymp signaling from _
|
Liver:
-Sympathetic from T7-10 Parasymp from R + L vagus |
|
|
_ separates medial + lateral segments of left lobe
Attaches liver to anterior ab wall extends to umbilicus + carries remnant of umbical vein |
FALCIFORM LIGAMENT
Separates medial + lateral segments of left lobe Attaches liver to anterior ab wall extends to umbilicus + carries remnant of umbical vein |
|
|
_ carries obliterated umbilical vein to undersurface of liver
|
LIGAMENTUM TERES carries obliterated umbilical vein to undersurface of liver
Extends from falciform ligament |
|
|
Portal fissure or Cantle's line:
Line from _ to _ Separates _ and _ lobes |
Portal fissure or Cantle's line:
Line from middle of gallbladder fossa to IVC Separates R and L lobes |
|
|
_ = name for peritoneum that covers the liver
|
Glisson's capsule = peritoneum that covers the liver
|
|
|
Liver segment _ = caudate lobe
|
Liver segment 1 = caudate lobe (just anterior to IVC)
|
|
|
Liver segment _ = quadrate lobe
|
Liver segment 4 = quadrate lobe
|
|
|
what is the tx for colon ca mets to liver segments 1+2?
|
Seg 1 = caudate (posterior to IVC), Seg 2 = top part of L lobe
-Tx = L hepatic lobectomy |
|
|
Left lobe of liver is segments ...
Right lobe of liver is segments ... |
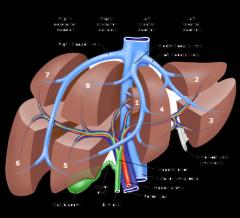
Caudate lobe = segment 1 (posterior to IVC)
Left lobe = segments 2 (left, superior) + 3 (left, inferior), 4 (anteriuor to IVC Right lobe = segments |
|
|
From the front of liver, you see 5 sections …
|
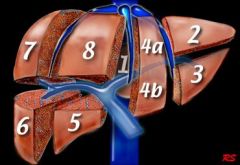
From the front of liver, you see (clockwise):
segments 2, 3, 4, 5, 8 |
|
|
Glisson's capsule does not cover _
|
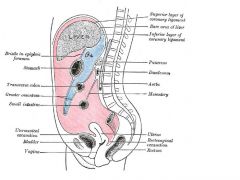
Glisson's capsule does not cover:
Bare area = area on posterior-superior surface |
|
|
_ = peritoneum on posterior surface of liver
= lateral + medial extensions of _ ligament |
Triangular ligaments = peritoneum on posterior surface of liver
= lateral + medial extensions of coronary ligament |
|
|
Portal triad enters liver segments (2)..
|
Portal triad enters liver segments 4, 5
|
|
|
Gallbladder lies under liver segments (2) …
|
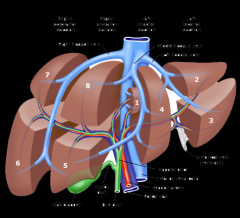
Gallbladder lies under liver segments 4, 5
|
|
|
Inferior border of liver segment _ overlies the hepatic duct confluence
|
Inferior border of liver segment 4 overlies the hepatic duct confluence
Divide connective tissue -> elevate segment 4 -> "lowers" hilar plate to expose hepatic duct confluence |
|
|
_ cells = liver macrophages
|
Kupffer cells = liver macrophages
|
|
|
Bile duct, portal vein, + hepatic artery (portal triad) meet @ the _ ligament
|
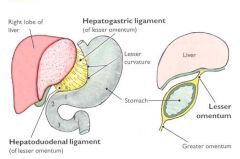
Bile duct, portal vein, + hepatic artery (portal triad) meet @ the HEPATODUODENAL ligament
|
|
|
In portal triad,
_ is posterior, _ is lateral, _is medial |
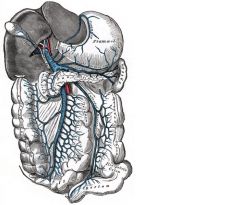
In portal triad,
portal vein is posterior, CBD is lateral, hepatic artery is medial |
|
|
Pringle maneuver = clamping of _
Will not stop bleeding from _ |
Pringle maneuver = clamping of porta hepatis
Will not stop bleeding from hepatic vein |
|
|
Foramen of Winslow:
_ is anterior _ is posterior _ is inferior _ is superior |
Foramen of Winslow:
Portal triad is anterior IVC is posterior Duodenum is inferior Liver is superior |
|
|
Portal vein arises from _ vein and _ vein
|
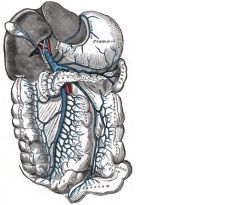
Portal vein arises from superior mesenteric vein and splenic vein (inferior mesenteric vein empties into splenic vein)
|
|
|
L hepatic drains segments (3)
|
L hepatic drains segments:
2, 3, superior 4 |
|
|
Middle hepatic vein drains segments (2)
|
Middle hepatic vein drains segments:
5, inferior 4 |
|
|
R hepatic vein drains segments (3)
|
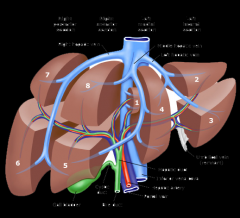
R hepatic vein drains segments:
6, 7, 8 |
|
|
In 80% of people, middle hepatic vein joins _ before draining into IVC
(other 20% go directly to IVC) |
In 80% of people, middle hepatic vein joins LEFT hepatic vein before draining into IVC
(other 20% go directly to IVC) |
|
|
Accessory R hepatic veins drain _ aspect of _ lobe directly into IVC
|
Accessory R hepatic veins drain MEDIAL aspect of R lobe directly into IVC
|
|
|
Inferior phrenic veins drain into _
|
Inferior phrenic veins drain directly into IVC
|
|
|
The _ lobe of liver gets separate R and L portal and arterial flow.
L hepatic vein drains _ aspect Middle hepatic vein drains _ aspect |
The CAUDATE (4) lobe of liver gets separate R and L portal and arterial flow.
L hepatic vein drains SUPERIOR aspect Middle hepatic vein drains INFERIOR aspect |
|
|
Enzyme _ is normally located in the canalicular membrane of liver
|
ALK PHOS is normally located in the canalicular membrane of liver
|
|
|
Usual energy source for liver is _.
|
Usual energy source for liver is keotnes.
Glucose converted to glyogen + stored Excess glucose converted to fat |
|
|
_ = only water-soluble vitamin stored in liver
|
B12 = only water-soluble vitamin stored in liver
(liver stores large amount of fat-soluble vitamins) |
|
|
2 most common post-op probs after hepatic resection are …
|
3 most common post-op probs after hepatic resection are:
Bile leak Bleeding |
|
|
What area of liver is most susceptible to ischemia?
|
Central lobular region of liver (Acinar zone 3) is most susceptible to ischemia
|
|
|
_% of normal liver can be safely resected
|
75% of normal liver can be safely resected
|
|
|
Solitary liver cysts
Most common population, location |
Solitary liver cysts
WOMEN RIGHT>left lobe -Resect if bleeding or infected (and can't be treated percutaneously) -Complications rare - most can be left alone -Walls have characteristic BLUE hue |
|
|
Solitary liver cysts
Characteristic appearance |
Solitary liver cysts
WOMEN RIGHT>left lobe -Resect if bleeding or infected (and can't be treated percutaneously) -Complications rare - most can be left alone -Walls have characteristic BLUE hue |
|
|
#1 cause of liver failure is _
|
#1 cause of liver failure = CIRRHOSIS
|
|
|
Acute fulminant hepatic failure => _% mortality
Outcome determined by course of _ |
Acute fulminant hepatic failure => 80% mortality
Couse of ENCEPHALOPATHY determines outcome |
|
|
A week after sustaining blunt abdominal trauma in an MVC, a 35 year old otherwise healthy man returns to the ER with hematemesis. Emergent EGD reveals no source of bleeding in the esophagus or stomach, but the duodenum is full of bright red blood. No ulcer is seen. What is the appropriate management of this patient?
|
Arteriography + embolization
This scenario is a classic description of a liver hematoma caused by blunt trauma which eventually bleeds into the biliary system. The patient in this scenario has an upper GI bleed due to hemobilia, not varices, gastritis, or ulcer disease. Sometimes blood is visualized as coming from the ampulla in the duodenum. There is no endoscopic therapy for this condition; the next best step in angiography with embolization to control the bleeding. |
|
|
Colon cancer mets to liver => _% 5-yr survival after resection
|
Colon cancer mets to liver => 20% 5-yr survival after resection
|
|
|
Metastatic, primary liver tumors get arterial supply via _
|
Metastatic, primary liver tumors are supplied by HEPATIC ARTERIES
|
|
|
Primary liver tumors;
hypo- or hyper-vascular? |
Primary liver tumors are HYPERvascular
(supplied by hepatic arteries) |
|
|
Metastatic liver tumors;
hypo- or hyper-vascular? |
Metastatic liver tumors are HYPOvascular
(supplied by hepatic arteries) |
|
|
Mirizzi syndrome = _
|
Mirizzi syndrome = compression of hepatic duct
-Stone in GB infundibulum -Inflammation from GB or cystic duct extending to hepatic duct -Causes stricture and hepatic duct obstruction |
|
|
what is nephrotic syndrome?
|
Nephrotic syndrome:
-renal damage -> leakage of protein, at least 3.5 g/day -Small holes in podocytes allow protein to pass through -> hypoalbuminemia, hyperlipidemia -4 main types: 1. Minimal change dz: drugs e.g. NSAIDS, malignancy esp. Hodgkin's dz 2. Focal segmental glomerulosclerosis: HTN, HIV, DM, obesity, kidney loss 3. Memranous nephropathy: HepB, Sjogren's, SLE, DM, sarcoid, syphilis, drugs, malignancy 4. Membranoproliferative |
|
|
An 80 year old woman without prior abdominal surgery presents with small bowel obstruction. A KUB shows air in the biliary tree. What is the most likely diagnosis?
|
Pneumobilia (air in biliary tree) in the context of SBO is likely 2/2 fistula between gallbladder and duodenum. Gallstone ileus is rarely diagnoses pre-operatively.
-Tx: removal of the stone via proximal enterotomy. The gallbladder and fistula should be left in tact, unless patient can tolerate this procedure. |
|
|
Porcelin GB => __-__% risk of cancer
-Tx is __ |
Porcelin GB => 30-65% risk of cancer (Fiser book says 10-20%)
-Cholecystectomy indicated |
|
|
Venous colaterals 2/2 portal HTN;
Veins of _ drain portal blood through bare areas of diaphragm -> paraumbilical vein collaterals -> umbilicus Veins of _ form in retroperitoneum, shunt portal blood from bowel, other organs -> vena cava |
Venous colaterals 2/2 portal HTN;
Veins of SAPPEY drain portal blood through bare areas of diaphragm -> paraumbilical vein collaterals -> umbilicus Veins of RETZIUS form in retroperitoneum, shunt portal blood from bowel, other organs -> vena cava |
|
|
Portal HTN 2/2 PREsinusoidal obstruction:
3 causes |
Portal HTN 2/2 presinusoidal obstruction: 2/2
1. Schistosomiasis 2. Congenital hepatic fibrosis 3. Portal vein thrombosis |
|
|
Portal HTN 2/2 POSTsinusoidal obstruction:
3 causes |
Portal HTN 2/2 POSTsinusoidal obstruction: 2/2
1. Budd-Chiari (hepatic vein occlusive dz 2. Constrictive pericarditis 3. CHF |
|
|
Normal portal vein pressure is < _ mmHg
|
Normal portal vein pressure is <12 mmHg
|
|
|
Portal HTN:
coronary veins act as collaterals b/w portal vein + systemic venous system of _ |
Portal HTN:
coronary veins act as collaterals b/w portal vein + systemic venous system of LOWER ESOPHAGUS |
|
|
Portal HTN:
the 4 major complications |
Portal HTN: 4 major complications
1. esophageal variceal hemorrhage 2. ascites 3. splenomegaly 4. hepatic encephalopathy |
|
|
Portal HTN:
4 indications for TIPS |
Portal HTN: 4 indications for TIPS
1. Protracted bleeding 2. Progression of coagulopathy 3. Visceral hypoperfusion 4. Refractory ascites (add risk of deveoping encephalopathy) |
|
|
Portal HTN:
the major risk of TIPS |
Portal HTN:
TIPS => increased risk of encephalopathy |
|
|
Portal HTN:
indication for splenorenal shunt |
Portal HTN:
Splenorenal shunt rarely used anymore CHILDS A cirrhosis who present with BLEEDING ONLY Low rate of encephalopathy Can worsen ascites |
|
|
Portal HTN:
contraindication for splenorenal shunt |
Portal HTN:
Splenorenal shunt contraindicated in REFRACTORY ASITES (can worsen ascites) |
|
|
Portal HTN:
Creation of a _ involves ligation of L adrenal vein, L gonadal vein, inferior mesenteric vein, coronary vein, pancreatic branches of splenic vein |
Portal HTN:
SPLENORENAL SHUNT: ligation of L adrenal vein, L gonadal vein, inferior mesenteric vein, coronary vein, pancreatic branches of splenic vein (Only for Childs A cirrhotics who present c/ bleeding only; low risk of encephalopathy, but increased risk of ascites) |
|
|
Portal HTN:
Tx for pt c/ Childs B/C + indication for shunt |
Portal HTN:
Childs B/C + indication for shunt => TIPS |
|
|
Portal HTN:
Tx for pt c/ Childs A + just bleeding as symptom |
Portal HTN:
Childs A + just bleeding as symptom => Splenorenal shunt |
|
|
Portal HTN:
_ predicts mortality after shunt |
Pootal HTN:
CHILDS CLASS predicts mortality after shunt |
|
|
Portal HTN in child is usually 2/2 _ (50%)
|
Portal HTN in child is usually 2/2
50% is 2/2 Extrahepatic thrombosis of portal vein |
|
|
What is the anatomy of the portal traid
(i.e. what is posterior, R/lateral, and L/medial)? |
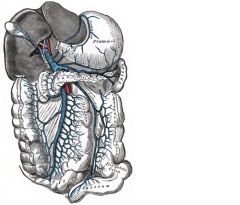
Portal triad:
-Portal vein posterior. CBD on R Hepatic artery on L |
|
|
#1 cause of massive hematemesis of children is _
|
#1 cause of massive hematemesis of children = extrahepatic thrombosis of portal vein
(portal vein thrombosis -> presinusoidal obstruction -> portal HTN) 50% of portal HTN in children |
|
|
Primary biliary cirrhosis: a RF for hepatocellular ca?
|
Primary biliary cirrhosis:
NOT a RF for hepatocellular ca |
|
|
Woman c/ fatigue, prouritus, jaundice, xanthomas
-Medium-sized hepatic ducts -Likely is _ - Lab test _ -Cancer risk -Tx |
PRIMARY BILIARY SCLEROSIS
Woman c/ fatigue, prouritus, jaundice, xanthomas -Medium-sized hepatic ducts -anti-MITOCHONDRIAL Ab's -NO cancer risk -Tx: tranplant |
|
|
Primary sclerosing cholangitis: a RF for hepatocellular ca?
|
Primary sclerosing cholangitis: YES a RF for hepatocellular ca
|
|
|
Primary sclerosing cholangitis:
RF for 2 cancers… |
Primary sclerosing cholangitis = RF for:
Hepatocellular ca Cholangiosarcoma |
|
|
RFs for _ =
men 30's-40's, retroperitoneal fibrosis, Reidel's thyroiditis, pancreatitis, UC, DM Dx by lab test _, procedure _ |
PRIMARY SCLEROSING CHOLANGITIS risk factors:
men 30's-40's, retroperitoneal fibrosis, Reidel's thyroiditis, pancreatitis, UC, DM ERCP => beaded appearance 2/2 strictures + dilations anti-MITOCHONDRIAL Ab's |
|
|
ERCP shows "beading" 2/2 strictures + dilations => likely _
|
ERCP shows "beading" 2/2 strictures + dilations => likely PRIMARY SCLEROSING CHOLANGITIS
|
|
|
Primary sclerosing cholangitis:
4 main Complications |
Primary sclerosing cholangitis ->
(scarring + patching c/ porgressive fibrosis of intra- + extrahepatic ducts) -> Portal HTN, hepatic failure, cirrhosis, cholangiocarcinoma |
|
|
Primary sclerosing cholangitis: Tx
Most need _ 2 surgeries can help 1 procedure 2 medicines |
Primary sclerosing cholangitis:
Transplant for most May benefit from PTC tube drainage, choledochojejunostomy Balloon dilation of stricture(s) Cholestyramine to decrease pruritus UDCA (urosodeoxycholic acid) to decrease bile acids, improve liver enzymes |
|
|
Pt comes in c/ signs of cholangitis, CBD obstruction
-GI can't cannulate the ampulla of vater for ERCP -Next step = _ |
Percutaneous transhepatic cholangiography (PTC) tube:
-To decompress biliary system if ERCP not possible |
|
|
Pt comes in c/ signs of cholangitis, CBD obstruction
-GI can't cannulate the ampulla of vater for ERCP, then radiologist can't place PTC tune -Next step = _ |
Pt c/ signs of cholangitis, CBD obstruction, but ERCP and PTC tube not possible ->
to OR for T-tube to decompress bilary system |
|
|
What is the most common cause of pyogenic liver abcesses?
|
Pyogenic liver abscess = 80% of liver abscesses:
-2/2 Biliary (cholangitis) > diverticulitis > appendicitis. Can arise weeks later. -RIGHT > left lobe. 15% mortality c/ sepsis -E. coli most common. Also cover for anaerobes. -Dx by aspiration -Tx: CT-guided drainage + abx. Surgery if unstable, biliary obstruction, or multiple abscesses |
|
|
what is the effect of ligating a replaced R or L hepatic artery?
|
either can be ligated without significant issue relative to hepatic ishemia
|
|
|
retained CBD stone indentified on T-tube cholangiogram 6 wks post-op is best managed by ...
|
retained CBD stone indentified on T-tube cholangiogram 6 wks post-op =>
radiology stone removal |
|
|
most common variant of R hepatic artery = off _
(travels in _) |
most common R hepatic artery variant = off SMA
-usually travels in hepato-duodenal ligament laterally -courses behind pancreas, posterior to portal vein (not anterior c/ common hepatic artery), lateral to CBD (not medial c/ common hepatic artery) |
|
|
Liver abscess that presents c/:
Maculopapular rash Increased eosinophils Sigmoid colon: granulation tissue, petichiae, ulcers Tx is 2 things… |
Schistosimiasis liver abscess:
-Presentation: Maculopapular rash, Increased eosinophils, +/- esophageal varices -Sigmoid colon c/ fine granulation tissue, petichiae, ulcers -Tx: praziquantel + control of variceal bleeding -Percutaneously drain if superinfected -Surgery only for complications, e.g. bleeding |
|
|
Fat, bile, pH <4 trigger release of __ from S cells in duodenum, which reduced HCL/gastrin release, increases bile flow, increases pancreatic HCO3- release
|
Secretin:
-Fat, bile, pH <4 -> released from S cells of duodenum -Inhibits HCl and gastrin release in stomach -Increases bile flow -Increases pancreatic HCO3- release -Gastrinoma => secretin injection increases gastrin release |
|
|
_ in liver occurs in sinusiodal membrane
|
Nutrient uptake in liver occurs in SINUSOIDAL membrane
|
|
|
_ can lead to isolated gastric varices s/ elevation of P in rest of portal system
|
Splenic vein thrombosis can ->
isolated gastric varices s/ elevation of P in rest of portal system |
|
|
Tx for splenic vein thombosis
|
Splenic vein thrombosis:
Tx: splenectomy |
|
|
Spenic vein thrombosis:
#1 cause |
Spenic vein thrombosis:
#1 cause = PANCREATITIS -Gastic varices s/ esophageal varices (very rare c/ cirrhosis) |
|
|
Spontaneous bacterial peritonitis:
PMNs > _ in fluid |
Spontaneous bacterial peritonitis:
-Fever, ab pain, PMNs >250 in fluid, (+) cx - -Usually mono-organism: E coli > pneumococcus, strep -If poly-organismal, worry suspect bowel perf -RFs; prior SBP, variceal hemorrhage, low-protein ascites, nephrotic syndrome, SLE in children -Tx: 3rd gen cephalosporin, usually responds w/in 48 hrs |
|
|
Spontaneous bacterial peritonitis:
#1 organism 2 other organisms If polymicrobial, need to r/o _ |
Spontaneous bacterial peritonitis:
-Fever, ab pain, PMNs >250 in fluid, (+) cx - -Usually mono-organism: E coli > pneumococcus, strep -If poly-organismal, worry suspect bowel perf -RFs; prior SBP, variceal hemorrhage, low-protein ascites, nephrotic syndrome, SLE in children -Tx: 3rd gen cephalosporin, usually responds w/in 48 hrs |
|
|
Spontaneous bacterial peritonitis:
Tx |
Spontaneous bacterial peritonitis:
-Fever, ab pain, PMNs >250 in fluid, (+) cx - -Usually mono-organism: E coli > pneumococcus, strep -If poly-organismal, worry suspect bowel perf -RFs; prior SBP, variceal hemorrhage, low-protein ascites, nephrotic syndrome, SLE in children -Tx: 3rd gen cephalosporin, usually responds w/in 48 hrs |
|
|
The primary cell type responsible for hepatic fibrosis is:
|
Stellate cells are responsible for fibrosis.
|
|
|
Wilson's dz: a RF for hepatocellular ca?
|
Wilson's dz:
NOT a RF for hepatocellular ca |
|
|
Crohns patient presents c/ duodenal obstruction, failed medical mgmt.
-what is the treatment |
Crohn's + duodenal obstruction, failed medical mgmt =>
GASTROJEJUNOSOMY in most cases (if distal, could do side-to-side duodeno-jejunostomy) unlike rest of sm bowel, stricturoplasty very difficult unless very short segment and resection not possible short of a Whipple |