Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
29 Cards in this Set
- Front
- Back
|
difference between the Hx / prgression in chron's and UC
|
CHRON's - yrs, recurrent flare ups/ remissions
UC- gradual onset |
|
|
site/ loc/ distribution where chron's and UC affect GI tract
|
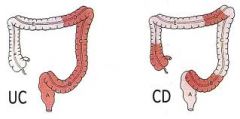
CHRON's- anywhere incl mouth, common terminal ileum. Starts proximally. "skip" lesions
UC- starts distal, continuous |
|
|
Histological difference Chron's & UC
|
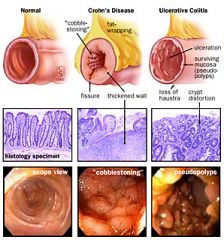
CHRON's: non-caseating granulomas (macrophages & Tcells), TRANSMURAL, deep fissuring ulcers
UC: plasma cells infiltrates, MUCOSAL & submucosal, mucosal ulcers |
|
|
common extra-intestinal manifestations of IBD
more common in which type |
EYES: uveitis
MOUTH: oral ulcers (chron's) clubbing anaemia SKIN: pyoderma gangrenosum JOINTS: arthritis Extra-GI more common in UC |
|
|
genes/ FH have more of an influence in which type, esp with HLA-DR1
|
Chron's HLA-DR1
(UC- HLA-DR2) |
|
|
what environmental factors are associated with CHron's
|
SMOKING
infectious agents vasculitis high sugar low fibre both: ?steril enviro NB: smoking not assoc with UC!!! |
|
|
many candidate genes assoc with IBD have a role in what
|
IMMUNE SYSTEM
|
|
|
what role do the Paneth cells in the small int normally have in mucosal immunity
- where are they located |
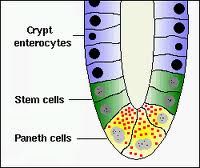
base of crypts
secrete ANTIMICROBIAL PEPTIDES --> defensive |
|
|
what 4 immune cell components are defective in CHRON's mucosal immunity
& how |
GOBLET cells= ↓mucin
EPITHELIAL cells: ↓TLR sensitivity & ↓clearance bact ('autophagy') PANETH= ↓antimicrobial peptides ↑CYTOKINES = ↑Tcell activation & INFLAM cell influx |
|
|
symptoms of CHRON's
|
diarrhoea + BLOOD
↓weight abdo pain +/- RIF mass (Extra-GI) PERIANAL abscess, fissure, tags, structures activE: fever, malaise, anorexia |
|
|
symptoms of UC
|
gradual onset diarrhoea + BLOOD
MUCUS CRAMPing abdo discomfort tenesmus, urgency EXTRA-GI active: fever, ↑HR, malaise, anorexia, ↓weight |
|
|
when does Chron's and UC present?
which sex? |
CHRON's- can go undiagnosed for years, <40, M♂
UC- YOUNG 15-30, peaks in 30's |
|
|
complications of Chron's
|
toxic megacolon (rare)
both IBD's: anaemia, anal disease, perforation, bleeding, nocturnal defaecation SBS - iatrogenic FISTULAS Ca amyloids ABSCESS |
|
|
complications of UC
|
both IBD's: anaemia, anal disease, perforation, bleeding, nocturnal defaecation
TOXIC MEGACOLON fistulas (rare) CA EXTRA-GI: eyes, mouth, skin, joints |
|
|
differentiate Chron's and UC on colonoscopy
|
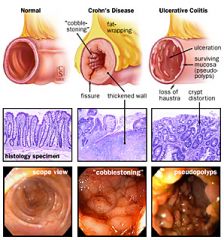
CHRON's: "skip" lesions, deep fissuring ulcers, "cobblestone", strictures
UC: continuous, severe mucosal ulceration, pseudopolyps, MUCUS |
|
|
2 drugs used in both IBD's (anti-inflams)
how do they work |
STEROIDS- immune supression & anti-inflam
ANTI-TNFa- inhibits main inflam agent |
|
|
example of a 5-ASA 1st line drug used in IBD
- administration - effect |
SULPHASALAZINE- topical/oral
affects composition & function of gut bacteria - reduces ca risk - anti-inflam |
|
|
disease course difference in Chron's and UC
|
Chron's: flare ups/ remissions, years
US: chronic LOW-grade activity, single attack = FULIMANT colitis (?toxic megacolon) |
|
|
colorectal cancer risk is higher for which IBD
|
UC
|
|
|
other types of colitis
|
UC & chron's colitis
collagenous lymphocytic radiation abx/ drug-induced ischaemia infective necrotizing enterocolitis |
|
|
Ix's for IBD
specifics for Chron's and UC respoectively |
CRP
albumin platelets B12 (Chron's) Endo-/colono-scopy + BIOPSY CHRON's: Ba follow through, MRI, White-cell scan (activity loc) UC: AXR |
|
|
side effects of anti-inflam corticosteroids used in IBD
|
x. dependency
x. osteoporosis x. skin thinning, acne x. metabolic: weight gain, DM, HTN x. growth failure |
|
|
an immunosuppressive agent used in IBD (both) for those with steroid side-effects
SE's |
AZATHIOPRINE (steroid-sparing agent)
x. pancreatitis x. hepatitis x. small risk ca |
|
|
eg of an anti-TNF drug used in both IBD's, how it works & SE's
|
INFLIXIMAB
- promotes apoptosis activated T cells x. infection x. ca x. infusion reactions |
|
|
what 4 reasons will emergency surgery be carried out in IBD
|
fail respond to medical therapy
small bowel obstruction abscess fistula |
|
|
for which IBD is surgery curative and non-curative
|
CURATIVE- UC
non-curative: chron's ...repeated = short-bowel syndrome |
|
|
what 2 scenarios is elective surgery an option for IBD
|
fail to respond to medical therapy
DYSPLASIA of colonic mucosa |
|
|
curative surgery for UC may leave the patient with what
|
an ileostomy
|
|
|
what's the Rx for IBD
|
prednisolone
5-ASA azathioprine/ methotrexate Abx- Crohn's Probiotics SURGERY |