![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
58 Cards in this Set
- Front
- Back
|
What is a group of chronic inflammatory conditions of the colon and small intestine? |
IBD |
|
|
What is characterized by a tendency for chronic or relapsing immune activation and inflammation within the GI tract (also as a dysregulation of the immune respond to GI luminal bacteria)? What are the two major forms? |
Idiopathic inflammatory bowel disease
Crohn disease and ulcerative colitis |
|
|
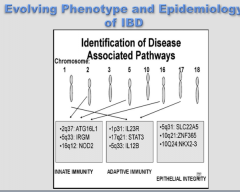
Name three gene mutations associated with each component of IBD: Innate immunity, adaptive immunity, and epithelial immunity |
|
|
|
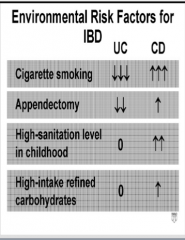
Describe whether each has an increased incidence, decreased incidence, or no effect on UC and CD:
Cigarette smoking, appendectomy, high-sanitation level in childhood, high-intake refined carbohydrates. |
|
|
|
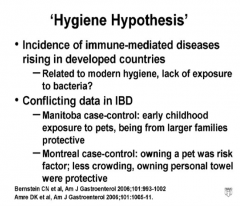
What is the hygiene hypothesis? What is the conflicting data on IBD between the Manitoba case-control and the Montreal case-control? |
|
|
|
Draw the pathogenesis of inflammatory bowel disease. Use bacterial components, macrophage, dendritic cell, neutrophils, CD4 T cell, and the associated cytokines release by each. |

|
|
|
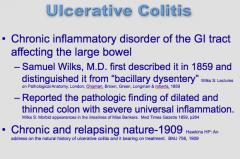
What is a chronic inflammatory disorder of the GI tract affecting the large bowel? |
|
|
|
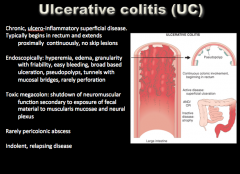
Where does ulcerative colitis usually begin? Where does it extend? Any skip lesions?
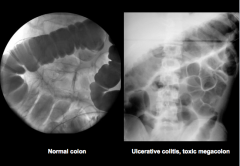
Endoscopically: hyperemia, ____ , granularity with friability, easy bleeding, broad based ulceration, _____, tunnels with mucosal bridges, rarely perforation Toxic megacolon: shutdown of _____ function secondary to exposure of fecal material to _____ and neural plexus Rarely pericolonic abscess Indolent, relapsing disease |
|
|

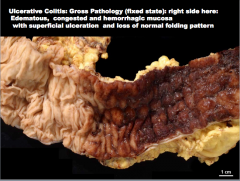
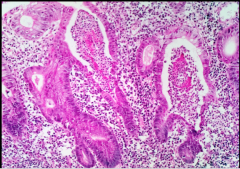
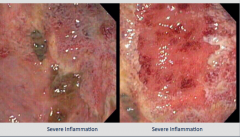
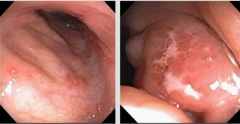
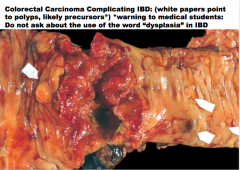
What is shown here? Describe it. |
|
|
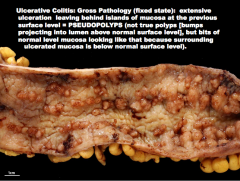
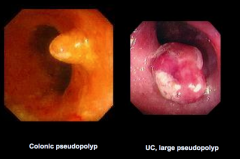
![What is the condition?
Describe: extensive
_____ leaving behind islands of mucosa at the previous
surface level = ______ (not true polyps [bumps
projecting into lumen above normal surface level], but bits of normal level mucosa looking like th...](https://images.cram.com/images/upload-flashcards/81/69/94/7816994_m.png)
What is the condition? Describe: extensive |
|
|
|
What is a characteristic feature of ulcerative colitis (where layer is the disease limited to)? |
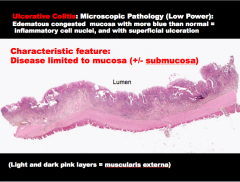
Muscularis and serosa are NOT affected. |
|
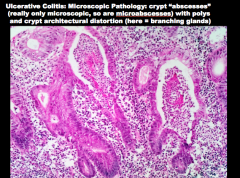
What is this characteristic finding in ulcerative colitis? What are they filled with? |
|
|
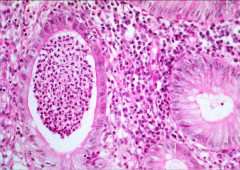
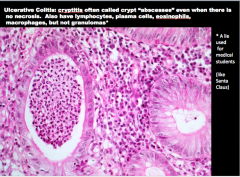
What is this condition called that is associated with UC? |
|
|
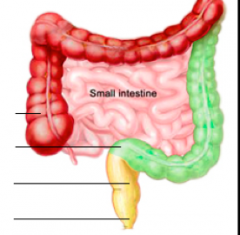
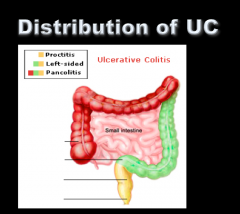
Identify Proctitis, left-sided, and pancolitis. |
|
|
|
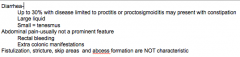
UC: Up to 30% with disease limited to proctitis or proctosigmoiditis present with what?
Is abdominal pain usually a prominent feature? Are fistulization, stricture, skip areas, and abscess formation characteristic? |
|
|
What percent of patients have rectal sparing? What is this called? If the rectum is normal, what is the disease? Does Crohn's disease typically have skip areas? |

|
|
What is the condition? |
Ulcerative proctitis |
|
What is the condition? |
Proctosigmoiditis |
|
What is the condition? |
Left-sided colitis |
|
What is the condition? |
Pancolitis |
|
What is the condition? |
Fulminant colitis |
|
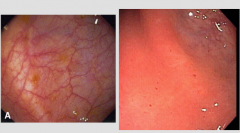
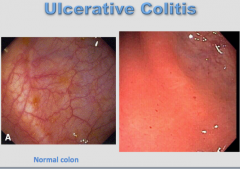
Which is normal? Which is abnormal? What is the condition? |
|
|
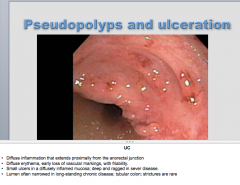
Again, what is the condition? |
UC |
|
Condition? |
UC |
|

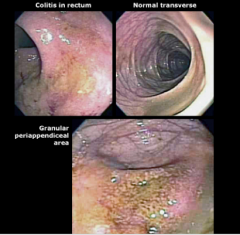
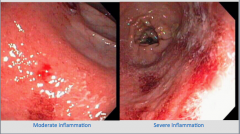
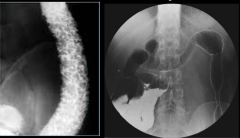
What is shown in each image? |
|
|
Which is normal? Which is UC (toxic megacolon)? |
|
|
|
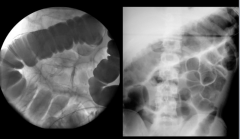
What study can you use to observe fine mucosal detail in UC? |
|
|
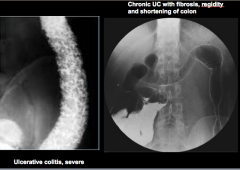
Identity severe UC and chronic UC with fibrosis (rigidity and shortening of colon). |
|
|
|
What study is most sensitive for evaluation of free air (which condition would this be useful for)? Does it demonstrate mucosal detail well? |
|
|
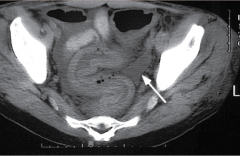
What is shown here? |
Thickened mucosa with edema and pericolonic fluid |
|
What is the condition? |
Crohn's disease |
|
|
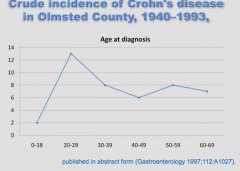
At what age does Crohn's disease peak in incidence (diagnosis)? |
|
|
|
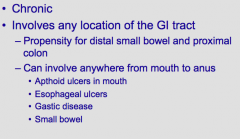
Crohn's Colitis:
1. _____ (symmetrical or asymmetrical) disease where there is involvement |
Asymmetrical disease where there is involvement |
|
|
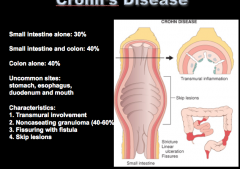
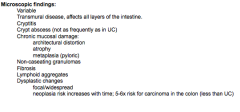
Crohn's Disease: What percent involves small intestine alone, small intestine and colon alone, colon alone? What are four uncommon sites?
What layers of the wall are involved? Do you often see non-caseating granulomas? Fissuring with fistula? What types of lesions? |
|
|
|
What is the incidence of Crohn's disease? At what ages does it peak (bimodal)? What race?
What are three recurrent symptoms? What will you see in 50% of cases (mild)? |
|
|
|
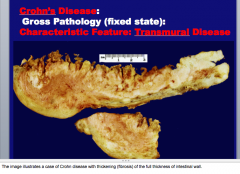
What is characteristic of Crohn's disease (in terms of wall involvement)? |
|
|
|
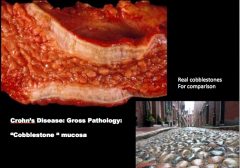
What is the descriptive term for the mucosa in Crohn's disease? |
|
|
|
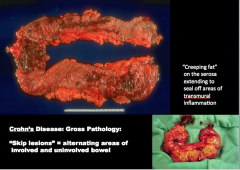
What are "skip lesions" in Crohn's disease?
What are areas on the serosa extending to seal off areas of transmural inflammation? |
|
|
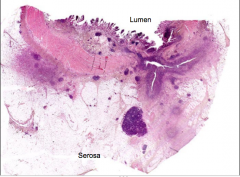
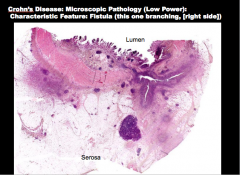
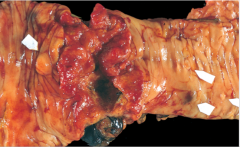
What is the disease? What is characteristic of the disease that is shown here (branching on the right side)? |
|
|
What is the disease? |
Crohn's disease |
|
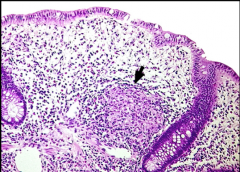
What is the arrow pointing to? What disease is this characteristic of? In what layer is this typically present? What other cells do you see? |
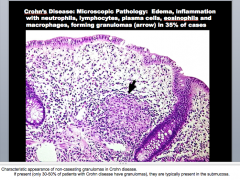
|
|
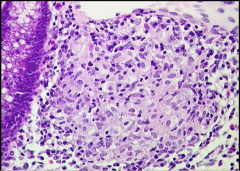
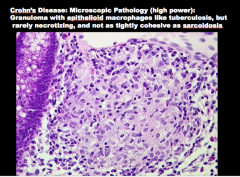
What is shown and what is the condition? What cell type is present (like in TB)? Is it usually necrotizing? |
|
|
|
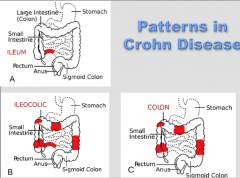
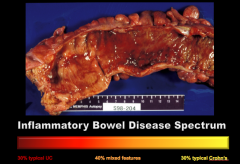
What are the three patterns of Crohn disease? |
|
|
What do you see in this endoscopy? What could this? |
Ulcerations => Crohn's disease |
|

What two things do you see here? What condition could this be? |
|
|
? |
|
|
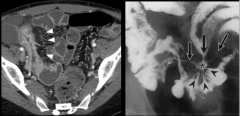
What do the white arrows and black arrows show? What disease? |
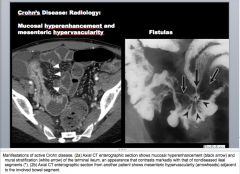
White arrow = mural stratification (mesenteric hypervascularity?) of the terminal ileum
Black arrow = mucosal hyperenhancement |
|

|

|
|

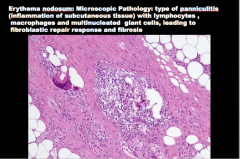
What is this tender subcutaneous nodule with an erythematous or dusky appearance that tends to parallel the activity of IBD (may also see it in Crohn's)? |
Erythema nodosum |
|
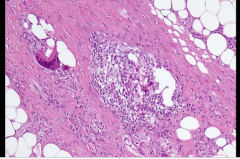
Fibrosis What is this?
Description: Swollen venules
What cells are involved? |
|
|

Appears first as a papule or nodule usually on the anterior aspect of the shin. May occur anywhere. Progresses to an ulcer with undermined borders. Not usually painful
What is this? |
Pyoderma gangrenosum (mild) |
|

What is this? |
Pyoderma gangrenosum (severe) |
|
|
What is episcleritis? What percent of Crohn's disease? It is an emergency? |
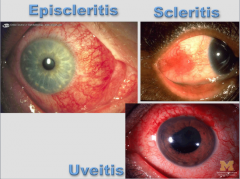
Infection of the sclera and conjunctiva => parallels activity of UC and Crohn's (6% of Crohn's). Involves deeper structures of eye => requires urgent care. |
|
What are all these? |
Extra-intestinal manifestations of Crohn's |
|
What is the current theory of IBD? What three things does the pathogenesis involve? |
Chronic relapsing, and remitting inflammatory disorder(s) of unknown etiologies: |
|

|

|
|
St. Mark’s London followed 600 patients with extensive UC for 5932 patient years |
|
|
What are all of these patients with IBD at risk for?
Do patients with Crohn's disease respond to TNF antagonists? |
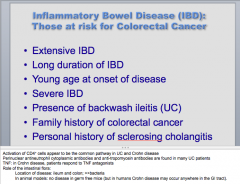
Colorectal cancer, yes |