![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
94 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Advantages |
The most definitive way of achieving complete control of an airway |
1 |
|
|
Disadvantages |
- Takes time - Takes practice - Can be difficult to achieve |
3 |
|
|
Indications |
Basic airways failed Long term ventilation required Airway burns/anaphylaxis Suction of bronchial tree Inhalation risk CPR - asynchronous Also Intermittent positive pressure ventilation (IPPV) and loss of airway reflexes |
BLASIC + 2 |
|
|
Contraindications |
Airway maintained by basic techniques Patient maintains own airway Epiglottitis Unable to intubate within 15 secs |
4 |
|
|
Complications |
- Receding lower jaw, obtuse angle @mandible - Short muscular neck - Full set of teeth - Prominent upper incisors - Long narrow mouth with high arched palate - Carious/insecure teeth - C-spine abnormality - Late pregnancy |
8 Vampire gnomey boy |
|
|
Is this airway gonna be a ball ache? |
Looks bad? probably is! Evalute. 3-3-2 score Mallampati score Obesity Neck mobility |
citrus fruit |
|
|
3-3-2 score |
Use patients own fingers 3 - between upper and lower incisors 3 - between mentum and hyoid bone (chin-neck junction) 2 - between hyoid bone and thyroid notch |

|
|
|
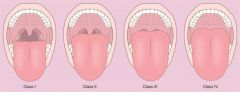
Mallampati score |
- The degree to which the mouth opens revealing the posterior oropharynx with tongue extended. - Grade I = easy - Grade IV = hard |
|
|
|
When is the mallampati for? |
Upright seated patient who is able to fully open their mouth. LIMITED VALUE IN UNRESPONSIVE PATIENTS WHO CANNOT FOLLOW COMMANDS |
|
|
|
Obstruction |
- Anything that might interfere with visualisation or ET tube placement. - Foreign bodies - Obesity - Haematoma - Masses - Muffled voice (hot potato) - Difficulty swallowing - Stridor |
|
|
|
Neck mobility |
Difficulties achieving sniffing the morning air position. - Neck trauma - Elderly patients (osteoporosis, arthritis) |
|
|
|
Hazards |
Total airway blockage Oesophageal intubation Patient resists; reflex activity present Induced bradycardia Clenched teeth due to cerebral irritation Airway burns Facial trauma Regurgitation and swallowing Intubation of right main bronchus Cervical spine injury Attachments too heavy |
TOPIC AFRICA |
|
|
Total airway blockage |
- Use initial basic techniques, back slaps etc. Forceps (guided by laryngoscope) - Attempt intubation - Consider needle crichothyroidotomy |
|
|
|
Oesophageal intubation |
- Deflate cuff - Remove tube - Re-oxygenate patient - Re-attempt intubation |
|
|
|
Patient resists |
- Abandon attempt - Use basic airway techniques |
|
|
|
How do you pre-oxygenate a patient? |
- Hyperventilate with 5 breaths of bag valve mask, 1/3 of the bag, 1 second a go. - Suction - Remove airway adjunct. |
|
|
|
Induced bradycardia |
- Careful laryngoscopy to avoid problem. - Atropine (600micrograms initial dose - every 3-5mins up to 3 milligrams max dose) |
|
|
|
Clenched teeth |
- Cerebral irritation, tetanus - Abandon irritation - Basic airways - Oxygenation to relieve cerebral irritation |
|
|
|
Airway burns |
- Early intubation - Uncut tube - Use bougie for all pre-hospital intubations - Consider smaller tube - Consider needle crichothyroidotomy |
|
|
|
Facial trauma |
- Careful suctioning - Careful laryngoscopy |
|
|
|
What to do when Regurgitation and swallowing |
- Suction using wide bore catheter (measure from the corner of mouth to tragus of ear) - Discard and replace tube if becomes blocked during intubation - Revert to basic techniques if unsuccessful. |
|
|
|
Intubation of right main bronchus |
- Deflate cuff - Withdraw to correct position - Re-inflate cuff - Re-check positioning with stethescope |
|
|
|
Cervical spine injury |
- Apply in-line immobilisation immediately - Intubation attempted only if attempts to maintain airway failing - Minimal neck movement |
|
|
|
Attachments too heavy |
- Displacement of tube due to equipment or rough handling - Check tube position - Re-intubate if tube dislodged - Stabilise head and neck (consider collar) |
|
|
|
What position should patient's head be for intubation? |
Sniffing the morning air |
|
|
|
What position should patient's head be for use of supraglottic airway (i-gel)? |
Neutral |
|
|
|
What equipment checks need to be performed? |
- Is all equipment there? - Does the cuff on the tube inflate? - Bulb working on laryngoscope? - 2 of everything |
|
|
|
Why would you insert an ET tube and an OPA? |
When a Thomas Mount with bite block is not available....OPA acts as a bite block. |
|
|
|
At what point do you extubate? |
Suction prior to? Point of maximal inspiration. Vocal cords are widest apart, then withdraw as they exhale. Patient on their side. |
|
|
|
Stages of intubation |
1.Position the patient 2. Blade insertion 3. Visualisation of glottic open 4. Tube insertion 5. Ventilation 6. Confirmation of tube placement |
|
|
|
Average size ET tube for male |
8 |
|
|
|
Average size ET tube for female |
7 |
|
|
|
i-gel features |
- Gastric channel - Forms an anatomical seal with the pharyngeal, laryngeal and perilaryngeal structures - Epiglottic rest prevents epiglottis from down folding - Integral bite block |
|
|
|
Upper airway |
All anatomical airway structures above the level of the vocal cords. |
|
|
|
Vallecula |
An anatomical space or pocket located between the base of the tongue and the epiglottis |
|
|
|
How to position the patient? |
Sniffing the morning air position |
|
|
|
Sellick manoevre |
The application of posterior pressure to the cricoid cartilage to minimise the risk of regurgitation during positive pressure ventilation |
|
|
|
BURP manoeuvre |
Backwards, upwards, right pressure manoevre used to improve the view of vocal cords during intubation |
|
|
|
What marks where the upper airway ends and the lower airway begins? |
Larynx |
|
|
|
How many cartilages in the larynx |
9 |
|
|
|
How many of the cartilages in the larynx are paired? |
6/9 |
|
|
|
How many of the cartilages in the larynx are unpaired? |
3 |
|
|
|
Which cartilages are paired? |
- arytenoid - corniculate - cuneiform |
|
|
|
Which cartilages are unpaired? |
- Thyroid - Cricoid - Epiglottis |
|
|
|
Facts about the thyroid cartilage? |
- Hyaline - Largest cartilage - Adams apple |
|
|
|
Facts about the cricoid cartilage? |
- Most inferior - Forms the base of larynx - First ring of the trachea, only one the is circumferential |
|
|
|
Facts about epiglottis? |
- Elastic - Attached to the thyroid cartilage and projects superiorly as a free flap towards the tongue. |
|
|
|
Facts about arytenoid cartilage? |
- Articulate with the posterior superior border of the cricoid cartilage. - Posterior attachment for the vocal cords. |
|
|
|
Facts about corniculate cartilages |
- Attached to the superior tips of the arytenoid cartilages. |
|
|
|
Facts about cuneiform cartilages |
- Contained in a mucous membrane anterior to the corniculate cartilages. |
Think snotty Daniel |
|
|
Glottis |
Vocal folds and opening between them. |
|
|
|
How to insert the blade? |
- Insert blade into right side of mouth - Use the flange of the blade to sweep the tongue gently to the left side of the mouth while moving the blade into the midline - Slowly advance the blade |
|
|
|
How to visualise the glottic opening |
–Vocal cords are white fibrous bands thatlie vertically within the glotticopening –If you are having difficulty seeing theopening, consider cricoid pressure |
|
|
|
How to insert the tube |
–Insert the tube from the right corner ofthe patient’s mouth through the vocal cords - insert the tube until the proximal end ofthe cuff is 1 to 2 cm past the vocal cords - Blade is not designed as a guide for thetube |
|
|
|
How to ventilate the patient? |
- Remove the blade. Remove the boujie - Inflate cuff with 5-10ml air - Attach bag valve mask and ventilate - Monitor chest for full respiratory cycle |
|
|
|
How to confirm tube placement? |
- Ascultation at apex and base of each lung and over the epigastric region - Capnography - If breath sounds heard only on right side then tube advanced into right bronchus |
|
|
|
Vestibular folds |
- False vocal cords - Superior pair of ligaments that extend from anterior surface of the arytenoid cartilages to the posterior surface of the thyroid cartilage. - Covered by mucus membrane |
|
|
|
Vocal folds |
- True vocal cords - Inferior pair of ligaments that extend from the anterior surgace of the arytenoid cartilages to the posterior surface of the thyroid cartilage - Covered by mucus membrane |
|
|
|
Pyriform fossae |
Two pockets of tissue on the lateral borders of the larynx. Airway devices are occasionally inadvertently inserted into these pockets. |
|
|
|
Epiglottic vallecula |
Groove between the base of the tongue and the epiglottis |
|
|
|
Landmarks |
Lips-teeth-tongue-hard palate-soft palate-palentine tonsil-uvula-pharynx-epiglottis-epiglottic vallecula. |
|
|
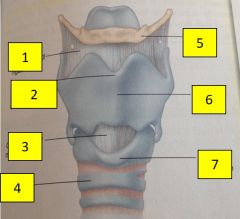
1 |
Thyrohyoid ligament |
|
|
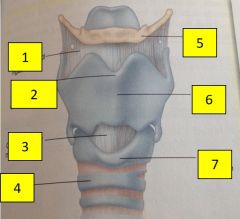
2 |
Laryngeal prominence (Adams apple) |
|
|
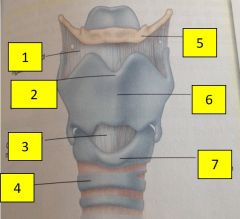
3 |
Cricothyroid membrane |
|
|
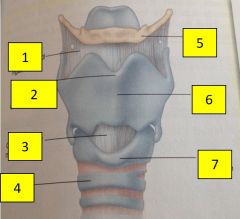
4 |
Trachea |
|
|
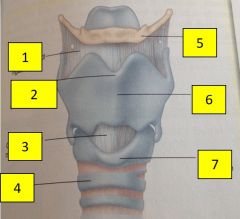
5 |
Hyoid bone |
|
|
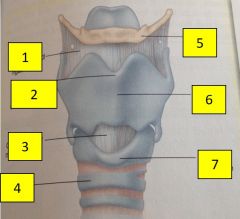
6 |
Thyroid cartilage |
|
|
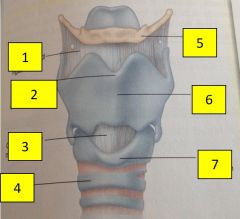
7 |
Cricoid cartilage |
|
|
|
igel orange |
size 5 90+kg |
|
|
|
igel green |
size 4 50-90kg |
|
|
|
igel yellow |
size 3 30-60kg |
|
|
2 |
epiglottis |
|
|
3 |
vestibular folds |
|
|
4 |
glottis |
|
|
5 |
vocal folds |
|
|
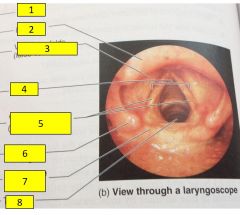
6 |
Cuneiform cartilages |
|
|
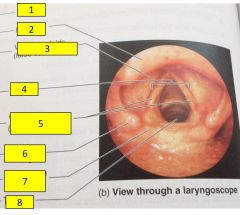
7 |
Corniculate cartilages |
|
|
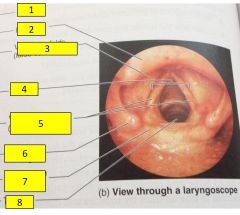
8 |
Trachea |
|
|
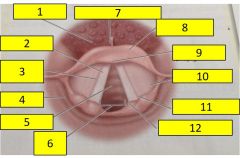
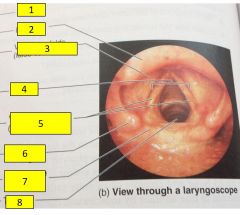
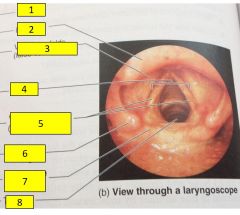
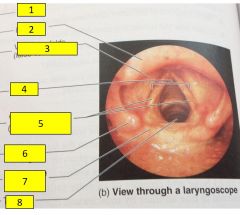
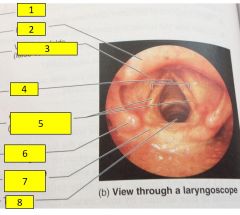
1 |
Base of tongue |
|
|
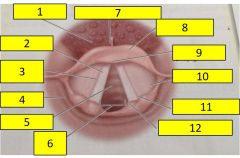
2 |
Vocal cord |
|
|
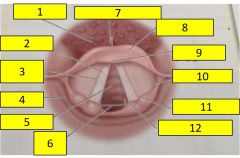
3 |
Vestibular fold |
|
|
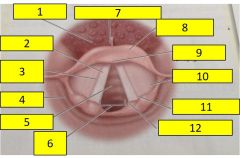
4 |
Pyriform fossae |
|
|
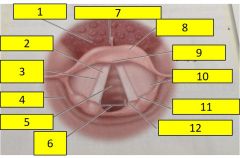
5 |
Trachea |
|
|
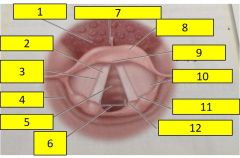
6 |
Glottic opening |
|
|
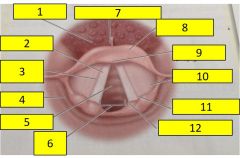
7 |
epiglottic valleculae |
|
|
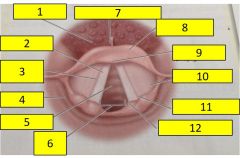
8 |
Epiglottis |
|
|
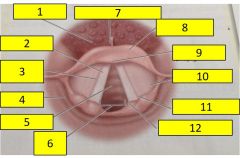
9 |
Tubercle of epiglottis |
|
|
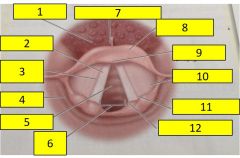
10 |
Aryepiglottic fold |
|
|
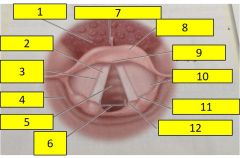
11 |
Cuneiform cartilage |
|
|
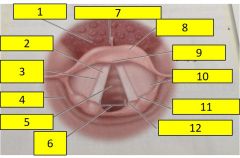
12 |
Corniculate cartilage |
|
|
|
How do you check tube placement? |
- "I visualised the tube passing the cords" - Rise and fall of chest - Auscultate - ETCO2 - Capnography - Oesophageal detector - Not cyanosed/improved perfusion |
|
|
|
What do you titrate oxygen to if patient starts breathing on own again? |
94-98% |
|
|
|
Why do you tritrate to 94-98% only not 100%? |
To avoid vasoconstriction as a result of myogenic response. |
|
|
|
Wave form capnography |
4-6 kPa
35-40 mmhg |
|