![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
13 Cards in this Set
- Front
- Back
|
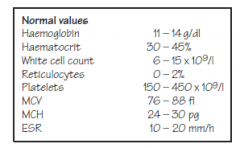
Haematology
|
|
|
|
Normal Arterial Blood Gas |
pH >> 7.35 – 7.42
PCO2>>> 4.0 – 5.5 kPa
PO2 >>>11 – 14 kPa (children) 8 – 10 (neonatal period) HCO3 17 – 27 mmol/l |
|
|
Determining the type of blood gas abnormality
|
pH PCO2 PO2 HCO3
Metabolic acidosis Low N/low* N Low Respiratory acidosis Low High N/low N/high* Metabolic alkalosis High N/high* N High Respiratory alkalosis High Low N/high N/low* |
|
|
Electrolytes and clinical chemistry
|
Normal ranges
Sodium 135 – 145 mmol/l Potassium 3.5 – 5.0 mmol/l Chloride 96 – 110 mmol/l Bicarbonate 17 – 27 mmol/l
Creatinine 20 – 80mmol/l Urea 2.5 – 6.5 mmol/l Glucose 3.0 – 6.0 mmol/l Alkalinephosphatase 150 – 1000 (infants) 250 – 800 (child) |
|
|
patterns of serum electrolyte abnormality
• Pyloric stenosis • Diabetic ketoacidosis • Gastroenteritis:
|
• Pyloric stenosis: metabolic alkalosis,
low chloride & potassium >>> (due to repeated vomiting andloss of stomach acid) low sodium concentration • Diabetic ketoacidosis: metabolic acidosis very low bicarbonate, high potassium, high urea &creatinine veryhigh glucose • Gastroenteritis: high Urea sodium may be eitherhigh or low depending on the sodium content of thediarrhoea, and on the type of rehydration fluid that hasbeen administered |
|
|
Causes of abnormal sodium balance
|
Hypernatraemia (Na+ >145 mmo/l)
• Dehydration- fluid deprivation or diarrhoea • Excessive sodium intake-inappropriate formula feed preparation-deliberate salt poisoning (very rare) Hyponatraemia (Na <135 mmol/l) • Sodium loss- 1. diarrhoea (especially if replacementfluids hypotonic) 2. renal loss (renal failure) 3. cystic fibrosis (loss in sweat) • Water excess 1. excessive intravenous fluidadministration 2. SIADH (inappropriate antidiuretichormone secretion |
|
|
interpret chest radiographs.
|
1• Identify the patient name, date and orientation (left and right).
2• Assessment of Quality PIER: Position: is this a supine AP file? PA? Lateral?Inspiration: count the posterior ribs. 10 to 11 ribs with a good inspiratory effect Exposure: well-exposed films have good lung detail and an outline of the spinal column Rotation: the space between the medial clavicle and the margin of the adjacent vertebrae should be roughly equal on each other; look for indwelling lines or foreign objects 3. Bones and soft tissue Examine the Bony structures, looking for fractures, asymmetry andabnormalities (e.g. hemivertebrae). Rib fractures are best seen byplacing the X-ray on its side. 4• Look at the Cardiac outline. At its widest it should be less than half the width of the ribcage (cardiothoracic ratio <0.5). 5• Check both Diaphragms The rightdiaphragm is higher than the left because of the liver. Check there is noair beneath the diaphragm (indicates intestinal perforation). 6. Effusions Check costo-phrenic angles are clear. Look for sharpness (blunted angles may indicate small effusions). Check a lateral film for small posterior effusions. 7. Fields and Fissures Check lung fields for infiltrates (interstitial vs. alveolar), masses, consolidation, air bronchograms, pneumothoraces, and vascular markings. Vessels should taper and should be almost invisible at the lung periphery.Evaluate the major and minor fissures for thickening or fluid. 8.Great vessels Check aortic size and shape and the outlines of pulmonary vessels. The aortic knobshould be clearly seen. 9• Hila and mediastinum Evaluate the hila for lymphadenopathy, calcifications, and masses. Look at the Mediastinum—note that in infants the thymus gland cangive a ‘sail’-like shadow just above the heart. |
|
|

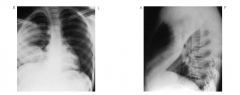
CXR of right middle and upper lobe pneumonia
Lateral X-ray showing right upper and middle lobe pneumonia |
|
|
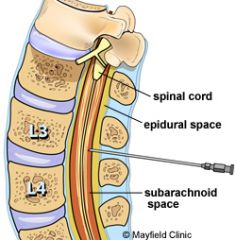
Lumbar puncture diagram
|
|
|
|
Lumbar puncture procedure
|
the patient in the lateral recumbent or prone positions or sitting upright. The lateral recumbent or prone positions are preferred >> they allow more accurate measurement of the opening pressure.
choice of needle >>> lumbar puncture headache >>>20 or 22 gauge spinal needle While patient is standing- The highest points of the iliac crests should be identified visually and confirmed by palpation; a direct line joining these is a guide to the fourth lumbar vertebral body. The spinal needle can be safely inserted into the subarachnoid space at the L3/4 or L4/5interspace, since this is well below the termination of the spinal cord. Once CSF appears and begins to flow through the needle, the patient should be instructed to slowly straighten or extend the legs to allow free flow of CSF within the subarachnoid space. up to 40 ml can be safely removed COMPLICATIONS PostLPheadache●Infection●Bleeding●Cerebral herniation●Minor neurologic symptoms such as radicular pain or numbness●Late onset of epidermoid tumors of the thecal sac●Back pain |
|
|
Urinalysis
|
Fresh urine should be collected into a sterile container from a midstreamsample if possible.
1• Observe the urine—is it cloudy (suggests infection) or clear? 2• What is the colour—pink or red suggests haematuria from the lowerurinary tract? Brown ‘cola’ coloured urine suggests renal haematuria. 3• Smell the urine for ketones and for the fishy smell of infection.Unusual smelling urine may suggest an inborn error of metabolism.• Dipstick test the urine using commercial dipsticks. This may revealprotein (suggests infection, renal damage or nephrotic syndrome),glucose (present in diabetes), ketones (in diabetic ketoacidocis, DKA)or nitrites (suggestive of infection). These sticks are very sensitive tothe presence of blood, and may detect haematuria even if the urine looksclear. 4• Finally, examine the urine under the microscope for white cells, redcells, casts and the presence of organisms. If suspicious of infectionsend a sample for culture. A pure growth of >105 colony-forming unitsof a single organism and >50 white cells/mm3 confirms infection |
|
|
Urine dIpstick finding 1 Specific gravity (low) Specific gravity (high) pH (low) pH (high) Blood present Can represent rbcs hbg myoglobin |
Nonpathologic pathologic Specific gravity (low) polydipsa DI renal tubular dyfunction Specific gravity (high) dehydration volume depletionpH (low) high protein diet acidosis pH (high) low protein diet : recent meal RTA uti (proteus)Blood present Can represent rbcs hbg myoglobin menses trauma catherization excercize Glomerular d/o tubular d/o uti stones hyper Ca , urinary tract trauma tumour rhabdo hemolysis |
|
|
Urinalysis 2 Protein present Glucose present Ketones Bilirubin present Urobilinogen Nitrite LE from (PMNs) |
Non pathologic pathologic Protein present orthostatic proteinuria fever exercise glomermular d/o tubular d/o uti Glucose present renal glycosuria ( SGLT2 defect DM fanconi anemia Ketones restricted carbohydrate in take DM starvation etohBilirubin present hepatitis, bilary obstruction Urobilinogen low amts systemic antibitic rx Hepatitis intravascular hemolysis Nitrite uti enterobacteriae only LE from (PMNs) fever Uti glomeruloneohritis pelvic inflam sterile pyuria |