![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
68 Cards in this Set
- Front
- Back
|
What are the bony parts of the nasal septum? The cartilaginous parts? |
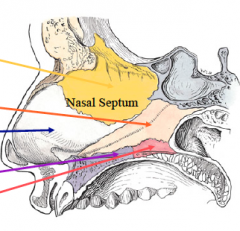
Bony: vomer, perpendicular plate of the ethmoid, maxillary crest, palatine bone Cartilaginous: quadrangular cartilage |
|
|
On the lateral nasal wall, what drains through each meatus (inferior, middle and superior)? |
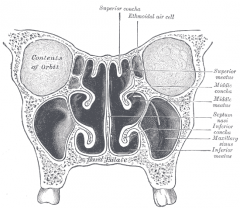
Inferior: nasolacrimal duct
Middle: maxillary, anterior ethmoid, frontal sinuses
Superior: posterior ethmoid sinus |
|
|
What branch of the ECA supplies the external nose?
What the two branches of the above artery, and what subdivisions of the nose do they supply? |
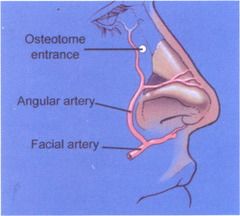
ECA -> Facial artery, splits into: 1. Superior Labial Artery: columella, lateral nasal wall (gives off an alar branch) 2. Angular Artery: nasal side wall, tip, dorsum |
|
|
What branch of the ECA supplies the nasal cavity? What are the three divisions of this branch, and what are their subdivisions? |
![ECA -> Internal Maxillary Artery, divides into:
1. Sphenopalatine Artery:
-Lateral nasal artery [lateral nasal wall]
-Posterior septal artery [posterior septum]
2. Descending Palatine Artery
-Greater palatine artery (see below)
-Lesser pal...](https://images.cram.com/images/upload-flashcards/69/67/79/9696779_m.png)
ECA -> Internal Maxillary Artery, divides into:
1. Sphenopalatine Artery: -Lateral nasal artery [lateral nasal wall] -Posterior septal artery [posterior septum]
2. Descending Palatine Artery -Greater palatine artery (see below) -Lesser palatine artery [lower portion of nasal cavity/soft palate]
3. Greater Palatine Artery - a continuation of the descending palatine artery [hard palate, nasal septum] - arteries meet in midline, run through incisive foramen back into nose
|
|
|
What branches of the ICA supplies the nasal cavity? What are the two branches of this artery and their targets? |
![ICA -> ophthalmic artery, subdivisions:
1. Anterior Ethmoid Artery [lateral, anterior 1/3 of nasal cavty]
2. Posterior Ethmoid Artery [superior turbinate, posterior septum]](https://images.cram.com/images/upload-flashcards/69/69/26/9696926_m.jpg)
ICA -> ophthalmic artery, subdivisions:
1. Anterior Ethmoid Artery [lateral, anterior 1/3 of nasal cavty]
2. Posterior Ethmoid Artery [superior turbinate, posterior septum] |
|
|
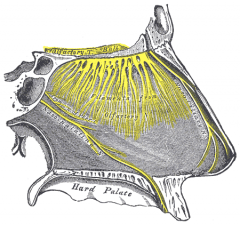
What is Kiesselbach's plexus/Little's area and where is it located? What arteries anastomose here? |
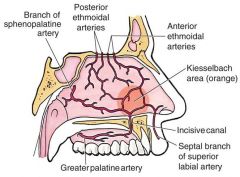
Located at anteroinferior nasal septum - confluence of: i. SPA ii. Anterior ethmoid artery iii. Greater palatine artery iv. Superior labial artery (septal branches) |
|
|
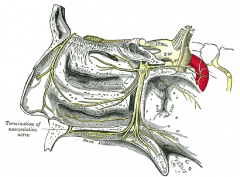
What is Woodruff's plexus (naso-nasopharyngeal plexus)/where is it located? What arteries anastomose here? |
![Located posteroinferior to the medial turbinate [lateral nasal wall].
Anastomosis of:
i. Posterior ethmoid
ii. Posterior nasal
iii. SPA
iv. Ascending pharyngeal](https://images.cram.com/images/upload-flashcards/73/58/39/9735839_m.jpg)
Located posteroinferior to the medial turbinate [lateral nasal wall]. Anastomosis of: i. Posterior ethmoid ii. Posterior nasal iii. SPA iv. Ascending pharyngeal |
|
|
What feature of the veins that drain the nose/paranasal sinuses makes transmission of pathogens easier? |
Veins are valveless |
|
|
Nasociliary nerve - what is it's source? Where does it arise? What parts of the nose do they innervate? |
From V1 in cavernous sinus. Branches: i. Infratrochlear n: skin over medial canthus ii. Anterior ethmoid n: -Anterior tips of middle/inferior turbs + septum, region anterior to superior turbinate -Skin over dorsum of tip of nose
|
|
|
Where does V2 exit the middle cranial fossa? To what ganglion does it run? |
Exits at the foramen rotundum, runs to the pterygopalatine ganglion |
|
|
What are the somatic divisions of the pterygopalatine ganglion? What do they supply? |
i. Lateral posterior superior nasal branch: Posterior superior/middle turbs, posterior ethmoids
ii. Medial posterior superior nasal branch: Posterior septum, roof of nasal cavity
iii. Nasopalatine n.: Anterior hard palate
iv. Greater palatine n.: Mucuous membrane below inferior turb, and middle/inferior meatus |
|
|
What is the source of the infraorbital n.? What structures does it supply? |
Infraorbital n. from V2; suplies anterior inferior meatus, nasal cavity floor, nasal vestibule |
|
|
What types of autonomic nerves arise from the pterygopalatine ganglion? Which ones are preganglionic/postganglionic? Name the nerves and their targets. |
Types of autonomic fibers: i. Sympathetic (postganglionic) -From T1-T3 spinal nerves; from superior cervical ganglion - travel w/ ICA, join GSPN to form Vidian n. ("nerve of the pterygoid canal"); vasoconstriction in nose
ii. Parasympathetic (preganglionic and postganglionic) - from CN VII -Preganglionic: From superior salivatory nucleus (medulla), to geniculate ganglion with greater superior petrosal n. -> vidian n. then to pterygopalatine ganglion
-Postganglionic: vasodilation and mucous secretion in nose |
|
|
What are the borders of the internal nasal valve? |
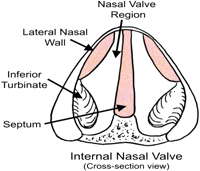
Lower edge of upper lateral cartilage Nasal septum Anterior edge of inferior turbinate |
|
|
What is the normal angle between the upper lateral cartilage and the nasal septum? |
10-15 degrees |
|
|
A newborn female presents with respiratory distress, cyanosis relieved by crying ("paradoxical cyanosis") and inability to pass a NG tube - what is the most likely diagnosis? What is the (general) incidence of this condition? What are the two types? Are males or females more likely to present with it? How do you treat it? |

Bilateral choanal atresia ~1:5000-1:8000 live births Can be bony or membranous-bony Female:male ratio 2:1 *Note that unilateral choanal atresia > bilateral
Treat immediately - i) place oral airway (stabilize airway) ii) McGovern nipple (cut off end of nipple, place intraorally, secure with ties) iii) endotracheal intubation |
|
|
How and when does unilateral choanal atresia usually present? How do you establish definitive diagnosis? |

Unilateral choanal atresia: -5-24 months with unilateral obstruction, nasal discharge |
|
|
What are some congenital disorders associated with choanal atresia? Name four. |
1. Treacher Collins (mandibulofacial dysostosis) 2. Crouzon disease 3. Apert syndrome 4. CHARGE (coloboma, heart disease, atresia choanae, retardation [mental], genital hypoplasia, ear anomalies) |
|

4YO child with nasal mass - does not appear to be tender, is noncompressible, firm and does not transilluminate. Histologically, mass contains keratin debris -Identify mass -What is its origin, of what is it comprised? What are some complications of this lesion? -Next diagnostic step? -Next |
Dermoid cyst - teratoma with keratin, hair, sweat/sebaceous glands (can present as mass, pit, fistulous tract - on nasal dorsum, )
Due to dural projection into prenasal space that adheres to epidermis and does not regress (traps epidermal components)
Image with CT/MRI (determine lesion size)
Treat with surgical excision (do not I&D - must remove entire mass and tract en bloc with bone/cartilage) |
|

2YO male with firm, bluish mass over nasal dorsum. Mass does not pulsate or increase in size with compression of the ipsilateral jugular vein. It is firm, noncompressible and does not transillumnate. Doppler flow studies of the mass show low arterial flow velocity during the end-diastolic phase. Identify mass. What percentage are external? what percentage are intranasal? Combined? Imaging? Treatment? |
Nasal glioma 60% external, 30% intranasal (unilateral), 10% both Get radiology Treat with complete surgical excision |
|

2YO with a bluish-red mass. Mass is pulsatile, expands with crying/straining. On palpation it's soft, compressible and transilluminates. When you compress the internal jugular veins, the mass expands. Identify. What contents could be in this mass? How do you classify these types of massesTreatment/complications? |
Encephalocele - CNS herniation through skull base defect Can be meninges only (meningocele) or meninges + glial tissue (meningoencephalocele) Classify by location -Occipital (75%) -Sincipital (25%)
Beware CSF leak, meningitis and herniation - resect mass, repair defect |
|
|
In a sincipital encephalocele ("fronto ethmoidal encephalocele"), where is the defect in the skull base? Where are you most likely to find a mass? Name 3 subtypes of the sincipital encephalocele |
Defect is in the foramen cecum of the frontal bone - most likely to find a mass externally over the glabella (superior to the nasion), nose or forehead Subtypse: -Nasofrontal -Nasoethmoidal -Naso-orbital |
|
|
What is the Furstenberg test? What congenital nasal masses can this help you identify? |
Compression of the ipsilateral internal jugular vein leads to expansion of the mass - can help to identify encephaloceles |
|
|
In a basal encephalocele, where is the defect? Where are you most likely to find a mass? What are the 4subtypes? |
Defect between the cribriform plate and the anterior clinoid process. Most likely to find an internal mass intranasally/in the nasopharynx Subtypes: 1. Transethmoidal 2. Transphenoidal 3. Spheno-ethmoidal 4. Spheno-maxillary |
|

Newborn with nasal mass. Mass was noted on ultrasound examination antenatally; on physical exam mass is firm, does not transilluminate. X-ray films show calcifications within the mass.
Identify. What germ layers are present within the mass? What is the most common anatomical site? The 2nd most common? What further imaging should be obtained? |
Neonatal teratoma - contains all 3 germ layers (ectoderm, endoderm, mesoderm). Most common site = cervical (neck), 2nd most common = nasopharyngeal
|
|
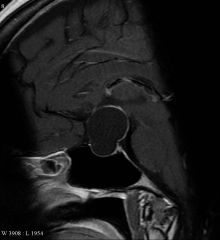
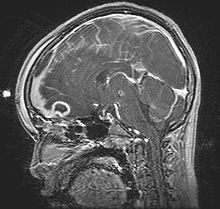
50YO male with bitemporal hemianopsia, MRI shows the above lesion. Identify. When does it usually present? Gender ratio? What is a tumor of this location called? |
Rathke's Pouch cyst - remnants of the pouch can persist to form a cyst/tumor Most common at 50-60YO; F>M Sx: compression of pituitary gland/optic chiasm Tumor of Rathke's Pouch = craniopharyngeoma |
|

23YO male with cervical pain, aural fullness, postnasal drip. Examination shows a smooth submucosal midline mass in the nasopharynx. Identify. Signs/symptoms? What is its origin? Treatment? |
Thornwaldt's Cyst - benign midline mucosal nasopharyngeal cyst; from notochord remnant
S/Sx: Cervical pain, aural fullness, serous otitis media, potnasal drip
Tx: None if asymptomatic, else marsupialization
|
|
|
20YO male c/o rhinorrhea, watery eyes. States he cannot taste food and his "eyes itch". Symptoms occur most strongly around his fiancee's cat. On physical exam he has dark circles under the eyes and a transverse "crease" across his nose.
Identify this condition. What type of hypersensitivity? Describe some s/sx, possible triggers |
Allergic Rhinitis - Type I Hypersensitivity S/Sx: rhinorrhea, nasal/ocular/palatal pruritus, PND, anosmia/hyposmia Triggers: -Perennial: dust mites, insects (roaches), dogs/cats -Seasonal: grass, trees, pollen ragweed |
|
|
When does the early response of allergic rhinitis begin? The late response? What happens during each phase (and what are some important inflammatory mediators)? |
Early phase: 5-15 min post exposure -IgE binds to mast cells; degranulation: histamine, tryptase, heparin release cause pruritus, congestion, rhinorrea, sneezing -Degranulation also causes release of PGD2, leukotrienes (C4, D4, E4), platelet activating factor
Late phase: 2-4H post exposure -Cytokins recruit eosinophils, neutrophils, basophils; cause chronic inflammation |
|
|
40YO female with nasal congestion, PND, congestion that is consistent and not described by any triggers. Denies eye itching or nasal itching. |
Nonallergic Rhinitis ("Vasomotor rhinitis") |
|
|
What are the eight subtypes of vasomotor (nonallergenic) rhinitis? |
1. Infectious - most commonly viral [rhinovirus, RSV, adeno, influenza/parainfluenza, enterovirus] 2. Vasomotor - parasympathetic>sympathetic 3. Hormonal 4. Occupational 5. Drug induced - beware NSAIDs, OCPs, ACEIs, B-blockers 6. Rhinitis medicamentosa 7. Gustatory rhinitis 8. NARES |
|
|
Describe NARES (nonallergic rhinitis of eosinophilia syndrome) - what are s/sx, how is it diagnosed? |
Rhinitis with congestion, rhinorrhea, sneezing, pruritus and hyposmia
Diagnosed by 10-20% eosinophilia on nasal smears |
|
|
What are four (major) drug classes associated with drug induced rhinitis? |
1. OCPs 2. B-blockers 3. ACEIs 4. NSAIDs |
|

12YO female with chronic nasal obstruction and anosmia. On physical exam her nose has a foul smell with yellow crusting, and she has a 6mm septal perforation. She also has a right middle ear effusion.
Identify this condition. Pathophys? Name some possible etiologies. |
Atrophic Rhinitis (Rhinitis Sicca/Ozena) Degeneration of the nasal mucosa with loss of mucociliary function (replacement with stratified squamous epithelium); decreasing blood supply causes atrophy of turbinates, bones, seromucinus glands.
Possbile etiologies: 1. Infection: Klebsiella ozaenae, proteus, diptheroids, E.coli 2. Nutritional deficiencies: Iron, vit A/D 3. Hereditary 4. Autoimmune |
|
|
45YO female with years of unexplained rhinosinusitis, rhinorrhea, severe nasal crusting and intermittent epistaxis. PMHx also significant for conjunctivitis, CKD stage III, and arthritis with chronic pain/swelling of her joints. A prior CXR shows bilateral fluffy infiltrates in the lower lobes.
Identify this disease. What three markers could you test for to determine the diagnosis? How do you treat nasal symptoms? |
Granulomatosis with polyangiitis -Triad (vasculitis, glomerulonephritis, necrotizing granulomas of the restpiratory tract) -Test C-ANCA, anti-myeloperoxidase (MPO), anti-proteinase 3 (PR3)
-Treatment: Topical abx, saline irrigation, nasal moisturizers |
|

47YOF Honduran with history of purulent rhinorrhea and dysphonia with sclerosis/fibrosis of the nose on examination.
Identify. In what regions is this disease endemic? What are the three stages of disease and their respective s/sx? What are two important histological findings? Treatment? |
Rhinoscleroma Granulomatous disease due to Klebsiella rhinoscleromatis. Most common in tropical regions (SE Asia, Africa, Central America)
Phases: 1. Catarrhal/atrophic: nasal crusting, purulent rhinorrhea 2. Granulomatous/hypertrophic: upper respiratory granulomas (painless) 3. Sclerotic: Sclerosis/narrowing
Histologically: 1. Mikulicz cells: Large macrophage, clear cytoplasm containing bacilli 2. Russell bodies: inside plasma cells
Tx: Bx, debridement, long term abx |
|
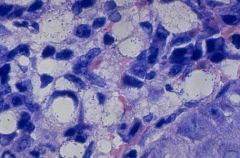
What type of cells are these? What disease are they associated with? |
Miculicz cells - large macrophage w/ clear cytoplasm containing bacilli. Associated with Rhinoscleroma |
|

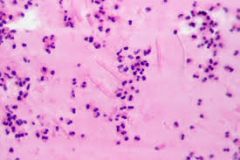
What are these large pink inclusions? What cells are they inside? With what disease are they associated? |
Russell bodies inside plasma cells - associated with Rhinoscleroma |
|

62YO Pakistani male with recurrent nasal obstruction and epistaxis. Exam shows the above friable red nasal polyps that bleed easily when palpated.
Identify. What would you see on histopathology of the lesion? What organism is associated with this condition? Treatment |
Rhinosporidiosis Granulomatous; caused by Rhinosporidium seeberi
See pseudoepitheliomatous hyperplasia on histopath with R. seeberi present
Treat with surgical excision |
|
|
Name three intrinsic coagulopathies that may predispose a patient to epistaxis |
1. Granulomatosis with Poly-Angiits 2. Hemophilia 3. HHT/Osler-Weber-Rendu |
|
|
What medical intervention should be prescribed for patients with nasal packing for epistaxis? Why? |
Place patients on prophylactic antibiotics (Augmentin, cephalosporin, topical mupirocin) for prophylaxis against toxic shock syndrome. |
|
|
Where would one find the SPA on an endoscopic approach for ligation? |
Roughly 7-8mm anterior to the posterior edge of the middle turbinate |
|
|
What is the definition of rhinosinusitis? What are the diagnostic criteria? |
Inflammation of the nose and paranasal sinuses Criteria (>2 symptoms): i. Nasal blockage/obstruction, or anterior/posterior nasal drip (must have this criteria) ii. +/- Facial pain or pressure iii. +/- Anosmia or hyposmia |
|
|
How do you classify rhinosinusitis? Describe the criteria for acute vs. subacute vs. chronic RS.
What are two subdivisions of CRS?
What is recurrent ARS? |
Stratify by duration of time = <4wks, 4-12 wks, >12 wks (acute/subacute/chronic)
CRS divisions = polypoid/nonpolypoid (although there's also eosinophilic vs. noneosinophilic)
Recurrent ARS: >= 4 episodes/year, each lasting 7-10 days with complete resolution between episodes
|
|
|
Within ARS, what are the three classifications (by etiology)? What are some signs/sx for each? |
ARS Subtypes: 1. Acute Viral: "The common cold" - rhinovirus, influenza; lasts >14d with nasal obstruction, facial pain/pressure, post/ant nasal drip, hyposmia/anosmia
2. Acute Non-Viral: An acute increase in symptoms after 5d or persistent symptoms after 10d; sudden onset of the above sx
3. Acute Bacterial: purulent sinus drainage, sinus pain/pressure, nasal obstruction |
|
|
What are three "cardinal signs" of acute baterial rhinosinusitis? Secondary signs? What main pathogens are involved? |
"Cardinal Signs": i. purulent nasal discharge ii. facial pain/pressure iii. nasal obstruction
Anosmia, fever, cough, HA, aural fullnesss
Bugs: H. flu, Strep pneumo, Moraxella catarrhalis |
|
|
What are some factors that could predispose a patient to ARS? |
1. Anatomical abberations: think about things that can obstruct sinus openings: septal deviaton/spur, turbinate hypertrophy, concha bullosa of middle turbinate, uncinate pneumatization, Haller cells
2. Acute viral respiratory infection: alters mucociliary clearance of sinuses -> decreased outflow
3. Blockage via neoplasm, trauma, nasal packing |
|
|
What are the four "cardinal symptoms" of chronic rhinosinusitis? How many must you have for a diagosis? What other signs must be present for a diagnosis? |
Diagnosis of CRS: >2 of 4 "cardinal symptoms" i. Purulent nasal drainage (ant/post) ii. Nasal obstruction iii. Facial pain/pressure iv. Hyposmia/anosmia
Must also have 1 of the following: v. Mucosal inflammation - purulent mucus/edema in middle meatus/ethmoids vi. Polyps in middle meatus/nasal cavity vii. Radiologic evidence of mucosal inflammation |
|
|
What are the three subtypes of CRS? What are the frequencies of each type? What inflammatory cells and inflammatory mediators are involved in each type? |
1. CRS with polyps (CRSwNP) - 20-33% -Neutrophilic inflammation
2. CRS w/o polyps (CRSsNP) - 60-65% -Eosinophilic inflammation -Eotaxin, IL-5 involved
3. CRS with fungal allergy ("allergic fungal rhinosinusitis") 8-12%
|
|
|
What eponymous pentad criteria are used to diagnose Allergic Fungal Rhinosinusitis? |
Bent and Kuhn criteria: 1. Eosinophilic Mucin (Charcot-Leyden crystals) 2. Noninvasive fungal hyphae 3. Nasal polyposis 4. Radiological findings -CT: hyperintense center, hypointense rim -CT: "speckles" of attenuation d/t ferromagnetic fungal parts -MRI: peripheral hyperintensity/central hypointensity (both T1/T2), "central void (T2) 5. Type I hypersensitivity (skin testing/serology) |
|
A patient complains of face pain, hypesthesia and purulent nasal discharge for four months. On biopsy of his mucus, you find the above finding. What type of crystals are these, and what type of CRS do they typify? |
Charcot-Leyden crystals; indicate an eosinophilic mucus seen in allergic fungal rhinosinusitis |
|
|
What species of fungus are most associated with allergic fungal CRS? |
"Black Yeasts/demitacious fungi: Alternaria Bipolaris Curvularia Cladosporium Deschlera |
|
|
What is the triad of Kartagener syndrome? How does it result in CRS? |
Kartagener's Triad: 1. CRS 2. Situs inversus 3. Bronchiectasis
Loss of ciliary function stops the mucociliary clearance of sinuses |
|
|
What percentage of CRS patients also have asthma? |
50% |
|
|
What is Samter's triad? |
1. Aspirin insensitivity 2. Nasal polyposis 3. Asthma
Mediated by leukotrienes (pro-inflammatory modifiers) |
|
|
Fungal Ball: What sinus is most affected? What fungus are you most likely to see? Is this more common in an immunocompetent or immunocompromised patient? On a physical exam, what are your findings? How do you treat a fungal ball? |
Affects a single sinus (mc= maxillary sinus) in immunocompetent patients; most likely to see Aspergillus fumigatus
On physical exam, patient will have pain over the affected sinus with a noninvasive "fungal ball" (hyphae + secondary debris). Treatment is surgical removal |
|
|
Acute Invasiva/Fulminant Fungal Rhinosinusitis: What type of patients most affected? S/Sx? What complication do you worry about? |
Most common in diabetics, immunocompromised (HIV, transplant, chemo) patients - see painless ulcers, necrotic eschar/drainage, periorbital swelling and ophthalmoplegia
Beware tissue necrosis, bony destruction, and angioinvasion (with thrombosis) |
|
|
Acute Fulminant Fungal Rhinosinusitis: What two histological classes of fungi are most likely? What medical/surgical treatment do you give? |
Histological classes: 1. Nonseptate, 90deg branching, necrotic background, "serpiginous" (wavy borders): rhizopus, rhizomucor, absida, mucor, zygomycosis [mc in diabetics/DKA]
2. Septate, 45deg branching, vermiform (tubular/cylindrical), "tissue background": Aspergillus
Treat with aggressive debridement, antifungals (itraconazole/posiconazole/amphotericin), correct immunosuppressive states |
|
|
Chronic Invasive Fungal Rhinosinusitis: How long does invasive fungal rhinosinusitis have to be invasive to be classified as "chronic"? Immunocompetent vs. immunocompromised patients? |
>4w duration in immunocompetent patients |
|
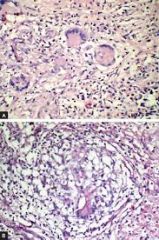
36YO immunocompetent female with 6w of chronic facial pain, purulent nasal discharge and hyposmia. On histology of a mucus sample, the above is seen. What findings do you see on the slide? Identify this subtype of CRS; what fungus is most common? Describe treatment. |
Multinucleated giant-cell granulomas with fungal elements; Chronic Granulomatous Fungal Rhinosinusitis -Most common fungus = Aspergillus flavus -Treatment = surgery, systemic antifungals |
|
|
Describe some of the ophthalmologic complications of rhinosinusitis. What eponymous classification system is used? |
Chandler's Classification: 1. Preseptal cellulitis 2. Orbital cellulitis 3. Subperiosteal abscess 4. Orbital abscess 5. Cavernous sinus thrombosis |
|
|
How do you differentiat pre-septal cellulitis from orbital cellulitis? |
Pre-septal: edema, EOM okay, no visual impairment Orbital cellulitis: chemosis, EOM impairment, proptosis, visual impairment possible |
|
|
How would you differentiate a sub-periosteal abscess from an orbital abscess?
What two syndromes are associated with an orbital abscess/what cranial nerves are affected for each> |
Subperiosteal Abscess: pus between bone, periorbita (periosteum) - see chemosis, EOM impairment, worsening visual impairment, exophthalamos (pus pushes globe forward)
Orbital Abscess: pus within the orbit; complete ophthalmoplegia, visual impairment Syndromes: i. Superior Orbital Fissure Syndrome: CN III, IV, V-1, VI ii. Orbital Apex Syndrome: CN II, III, IV, V-1, VI
ii. Orbital apex syndrome |
|
|
What symptoms describe cavernous sinus thrombosis? What cranial nerves are involved? |
Abrupt onset of periorbital edema, headache, proptosis, photophobia.
Involvement of CN II, IV, V-1, V-2, VI (VI most common). May see contralateral cavernous sinus involvement in 24-48H. |
|
|
What is a Potts' Puffy Tumor? What is the main complication associated with progression of the disease? |
Subperiosteal abscess (associated with osteomyelitis) - frontal bone osteomyelitis, can progress to erosion of the anterior bony table |
|
|
8YO boy with 16 days of high fever, purulent right nasal discharge and swelling over the right eye. Identify this disease - how is it classified. What pathogens are most common? Name a few predisposing factors that would give you chronic episodes of this condition. |
Acute Pediatric Rhinosinusitis - beware cold-like symptoms that do not improve after 10d; most likely viral in nature; beware secondary bacterial sinusitis (H. flu - nontypable, S. pneumo, M. catarrhalis)
1. ARS: URI sx >7-10d, daytime cough & rhinorrhea (most common sx), irritability, HA otitis media (50-60%), purulent rhinorrhea, periorbital edema, fever >39C
2. Subacute: 30-90d of sx
3. CRS: Low-grade persistence of s/sx for >90d without improvement. Beware predisposing factors: -Allergic rhinitis, GERD -Kartagener syndrome, immunodeficiencies -Day care attendance, 2nd hand smoke -Otitis media, tonsillitis
|
|
|
Antibiotic therapy for rhinosinusitis? 1st line drugs/duration? What if patient is penicillin allergic? When to switch to 2nd line?
What other therapies are used? |
First line: Augmentin/amoxicillin x 7-14d -If penicillin allergic - TMP/SMX, doxycycline, macrolides
Second line: After 72H without improvement of sx; try high dose Augmentin, quinolones (levo/moxi)
Other therapies: -Nasal decongestants -Nasal corticosteroids -Oral H1/H2 blockers (with allergic rhinitis) |
|
|
Medical treatment of CRS with polyps vs. CRS without polyps? What initial dose of PO steroids do you use/how do you taper it? |
1. CRS +Polyps: >12w abx (remember - more neutrophilic infiltrate), topical nasal corticosteroids, nasal irrigation
2. CRS -Polyps: The above triad of drugs, but add >12w PO systemic corticosteroids (1mg/kg initial dose, then taper over 10d) |