![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
39 Cards in this Set
- Front
- Back
|
Amniotic Fluid Embolism - Features |
- Sudden,profound and unexpected maternal collapse associated with:
o Hypotension o Hypoxemia o DIC |
|
|
Amniotic Fluid Embolism - Mortality |
- 10%fetal deaths Australia
- Fetalmortality is around 70% - Mostoccur during labour – some after and some from caesarian section |
|
|
Amniotic Fluid Embolsim - No proven risk factors - possible assossiations |
o Late maternal age
o Termination of pregnancy o Caesareansection o Polyhydramnios o Multiparity o Meconiumstained liquor o Intrauterinedeath o Strong/frequenttetanic contraction o History of allergy or atopy o Uterine rupture o Amnionitis |
|
|
Amniotic Fluid Embolism - Pathophysiology - Entry and Phase 1 |
Can enter through placental implantation but most commonly through the endoservic PHASE 1 - An anaphylactoid biochemical mediator response causing peripartum hypoxia, hemodynamic collapse and coagulopathy. Lasts about 30 minutes |
|
|
Amniotic Fluid Embolism - Phase 2 |
PHASE 2 - occurs in patients that survive phase 1 – L ventricular failure, DIC and pulmonary edema |
|
|
Amniotic Fluid Embolism - Causes of Cardiac dysfunction |
o Cardiac dysfunction is due to ischemia and the presence of endothelin (potent vasoconstrictor), histamine, PGs, Serotonins, Thromboxanes and leukotreins from the fluid
o Vasospasm and shunting causes ARDS o Fluidalso contains coagulation factors and sloughed fetal skin which cause DIC without significant blood loss |
|
|
Amniotic Fluid Embolism - Presentation |
Breathlessness, cyanosis, hypotension, dysrhythmia, DIC, seizures, profound fetal distress
|
|
|
Amniotic Fluid Embolism - Mx |
o O2 –CPAP or PEEP
o Fluidsand vasopressors o Coagulants o Fastdeliver of baby |
|
|
Shoulder Dystocia - Principle |
Disproportion between bisarcomial diameter of the fetus and anteroposterior diameter of pelvic inlet - confirmed if no delivery 60 seconds after head presents with normal downward traction Around 1% of all vaginal births C-section usually planned if >5kg or in instance of gestational diabetes |
|
|
Shoulder Dystocia - Risk Factors (Weak) |
o Previous shoulder dystocia
o Advanced maternal age o Malebaby o Macrosomia o Maternal diabetes o Maternal obesity o Prolonged1st and 2nd stages of labor |
|
|
Turtles Sign |
In Shoulder Dystocia where the chin retracts into perineum |
|
|
Aim of Emergency Manouvers in Shoulder Dystocia |
o Increase functional size of bony pelvis
o Decrease bisacromial diameter of the fetus o Change relationship of bony pelvis with bisacromial size of fetus by rotation |
|
|
McRoberts Manouvre Goal |
o Increases width of birth canal by reducing lumbosacral lordosis
o Avoid fundal pressure |
|
|
Managing Chord in Shoulder Dystocia |
- Avoid cutting chord early if possible – increases risk cerebral palsy and asphyxia -
- Delay chord clamping if it has had sustained traction on it – increased transfer of blood to placenta may have occurred - If chord must be immediately divided – try milking chord quickly |
|
|
Documentation Elements in Shoulder Dystocia |
o Time of head birth
o Maneuvers performed and timing o Direction baby is facing and which shoulder is impacted o Time of delivery o Staff in attendance o Condition of baby |
|
|
Shoulder Dystocia - Complications for Mother |
o 3rd,4th dergree tears
o PPH o Uterinerupture o Futureissues o Physcological obstetric effects |
|
|
Shoulder Dystocia - Complications for Baby |
§ Brachial plexus injury
§ Fractured hummers/clavicle § Hypoxia (pH drops .04 per minute) § Death |
|
|
Umbilical Cord Prolapse |
· Chord below or beside presenting part
· Life threatening: o Chord compressed – vessels within cord spasm o O2 can be prevented from reaching the fetus o Mx is complicated due to ongoing contractions - more compressive force |
|
|
Cord Prolapse Mx |
o Immediate transport o May only survive 10 min – no O2 o 15L/minO2 o Positioning 'knee-to-chest' of mother to reduce cord pressure o Ifcord not pulsating or fetal distress present – push presenting part off chord o Cover cord with sterile moist towel/dressing – avoid handling |
|
|
Nuchal Cord |
· Up to 25% birth
· Can be looped up to 4 times · If cord is needed to be cut – time criticaldelivery |
|
|
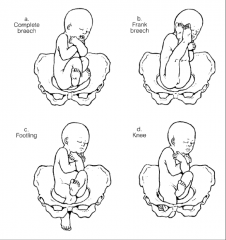
Breech Birth Types |
|
|
|
Breech - Risk Factors |
Most significant are preterm labour and gravida o Previousbreech o Low-lyingplacenta/praevia o Pelvicmasses o Bicornuateuterus o Polyhraminios o Oligohydraminios o Fetalabnormalities o Twinsor higher multiples o Grandmultiparty |
|
|
Breech - Mx |
o Loveset’s
o Marceau-Smellie-Viet o Burns–Marshall method § Not recommended |
|
|
Hematomas - Delivery |
Vulvul - usually varicose veins Vaginal - potential space for 2 liters of blood Broad Ligament - level of shock is out of proportion with the amount of blood seen |
|
|
Uterine Rupture |
A tear in uterus usually associated with: § Previous caesarian section§ Other uterine surgery § Grand multiparity |
|
|
Uterine Rupture - Management |
· O2
· Appropriate positioning · Fluid · Pain relief · Notification receiving hospitaland urgent transport |
|
|
Uterine Rupture - Classifications |
ACUTE - less than 24 hours post delivery SUBACUTE - from 24 hours to 4 weeks CHRONIC - 4 weeks onwards INCOMPLETE - fundus reaches servic COMPLETE - fundus passes through cervix PROLAPSE - uterus visible from vulva |
|
|
Uterine Inversion (Prolapse) |
o Spontaneouslyor following excessive traction being applied to the umbilical cord
o Severeabdo/pelvic pain due to excessive traction on the broad ligament and ovarianligaments o Hemorrhage if placenta is partially separated o Manifestations of shock are more common with complete uterine inversion |
|
|
Uterine Inversion - Mx |
§ Cover uterus with sterile dry drape –minimize infection
§ Help women achieve a position of reasonablecomfort § Administer pain relief as appropriate § Treat for hypervolemia § Transport to definitive care § Notify |
|
|
Secondary PPH |
§ 24hrs to 6 wks
§ 1% of postpartum women High association with maternal morbidity –85% require admission |
|
|
Secondary PPH - Risk Factors |
· Primary PPH
· Manual removal of placenta |
|
|
Secondary PPH - Aetiology |
· Unknown in one third of cases
o Subinvolution of the uterus – does not return to normal size o Retainedproducts o Endometriosis |
|
|
Secondary PPH - Characteristics |
· Ongoing vaginal bleeding
· Pallor from recent blood loss · Change in lochia – regression to bright redand increasing amounts – if infection, smell may be offensive · Uterus may be larger than expected –failure to contract · Pyrexia · Tachycardia – indicates infection orhypervolemia |
|
|
VTE - Risk Factors |
o >35
o Obesity o Parity>4 o FamilyHx o Grossvaricose veins o Majorconcurrent illness o Prolongedbed rest >4 days o Longhaul travel o C-section o Prolongedlabor |
|
|
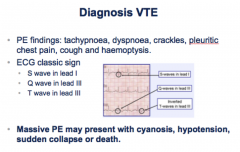
VTE Diagnosis |
|
|
|
VTE - Mx |
o Transportcritical o O2Analgesia o IVresus. As required o Positioning to prevent mobilisation of clot
|
|
|
Cord Prolapse - Risk Factors |
- Abnormla fetal presentation - Multiparity - Low birth weight - Prematurity - Polyhydramnios |
|
|
Shoulder Dystocia - 3 P's to Avoid |
- Pushin - Pullin - Pivoting |
|
|
Shoulder Dystocia - Prepare for (Mother and Baby) |
MOTHER: - PPH - Perineal trauma - Psychological trauma BABY: - Birth trauma - Hypoxia |