Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
125 Cards in this Set
- Front
- Back
|
Anatomical considerations for Pediatric patients receiving anesthesia
|
-Bone density is less
-Mandibular foramen located more inferiorily |
|
|
Behavior management for pediatric patients
|
-BE HONEST!!
-Use of topical anesthetic -Distraction -Counter irritation -Assistant to hold hands and stabilize -cradle the head when posible -use mouth prop when it is essential to have mouth open or with patients you do not know -young children have a limited ability to inform about anesthesia DONT STOP |
|
|
What should you do while giving anesthesia to children??
|
DONT STOP
|
|
|
Children often become upset over the feeling of numbness....
|
-let them see themselves. they may feel distorted
-tell the child when the feeling of numbness (big, tingly, sparkly etc) will go away. Use terms the child will understand |
|
|
technique tips
|
-slow deposition of solution (not too slow)
-use 27 gauge needle -maxillary short (1") -mandibular long (1 5/8") usuallly inferior alveolar block & long buccal injection - may use mouth prop ('tooth pillow") -reflect lip and pull tissue tight -finger rests -DONT STOP |
|
|
complications of local anesthesia
|
-biting of lip, cheek, tongue or excessive rubbing
-Hematoma -Over dose |
|
|
Dosage of Local anesthetic
|
2 year old = 20 lb = 1 carpule 40 mg
4.5 year old = 40 lb = 2 carpule 80 mg 8 year old= 60lb = 3 carpule 120 mg |
|
|
duration of anesthesia
|
-consider shorter duration of anesthesia
-3% mepivacain 20-40 min pulpal anesthesia and 1-3 hr soft tissue anesthesia -2% lidocaine 1:100,000 epi 1-2.5 hr pulpal anesthesia and 2-5 hr soft tissue anesthesia -3% mepivacaine = 20 min Maxillary and 40 min mandibular |
|
|
Short acting local anesthetic
|
-consider 3% mepivacaine (carbocaine) when the procedure is
-very short -expected to have little post op pain -done for patients who are at high risk to bite their lips or tongue |
|
|
Articaine (Septocaine)
|
-4% articaine
-1:100,000 epinephrine -be careful about dose-higher concentration of drug -not approved for use in children under 4 years |
|
|
Local Anesthesia complications: LOCAL
|
-needle breakage
-pain on injection -persistent anesthesia or parasthesia -trismus -hematoma -edema -sloughing of tissues -soft tissue injuries -facial nerve paralysis -postanesthesia intraoral lesions |
|
|
Local Anesthesia Complications: SYSTEMIC
|
-overdose
-allergy |
|
|
Needle Breakage
|
-extremely rare with disposable needles
-causes: smaller needles, bent needles, manufacture's defect -problem: scar tissue, migration (generally posteriorily), infection -prevention: longer, larger needles, don't insert to hub, don't redirect while needle is deep (more than 1cm into tissues) |
|
|
Needle breakage management
|
-instruct the patient not to move
-keep the mouth open (bite block) -if you can see it, grab it (hemostat) -if you can't see it, refer to OMS immediately, inform patient, document incident, keep needle stump -litigation? call your lawyer |
|
|
Causes of Pain on injection
|
Causes:
-careless technique, callous attitude -dull needles -rapid injection -needles become barbed after contacting bone |
|
|
Problems with pain on injection
|
-pain--> anxiety---> medical emergency
-pain --> sudden movement--> needle breakage |
|
|
Prevention of Pain on injection
|
-proper techniques
-sharp needles -topical anesthetic -sterile local anesthetic solution -inject slowly -anesthetic solution too hot or too cold (room temperature is good) |
|
|
Burning on injection Causes
|
-solution pH (5,3)
-rapid injection -contamination (sterilizing solutions) -carpule warmed to body temp is "too hot" |
|
|
Problem burning on injection
|
-related to pH: transient
-related to others: possible tissue damage |
|
|
Prevention and Management of Burnign on injection
|
Prevention:
-slow injection (ideally 1cc/min) -don't store carpules in alcohol or other sterilizing agent Management: -follow up -manage specific problem |
|
|
Persistent Anesthesia or Parasthesia Causes
|
-contaminated anesthetic solution
-needle trauma to nerve ('electric shock") -hematoma --> pressure |
|
|
Persistent Anesthesia or Parasthesia Problems
|
-self-inflicted injury (biting, heat)
-taste -hyperesthesia (normal stimuli cause an excessive sensation) or dyesthesia (normal stimuli cause pain) |
|
|
Persistent Anesthesia or Parasthesia Prevention
|
-adherence to injection protocol
-proper care and handling or carpules |
|
|
Persistent Anesthesia or Parasthesia Management
|
-Reassure; follow up; document in chart
-refer to OMS if still present after 2 months |
|
|
Trismus
|
-restricted jaw movement
Causes -trauma to muscles or blood vessels: hemorrhage, multiple injections, large volume of anesthetic, infection -contaminated anesthetic solution -local anesthestics are slightly myotoxic |
|
|
Trismus problem
|
-usually minor
-chronic hypomobility |
|
|
Prevention of Trismus
|
-sharp, sterile, disposable needle
-proper handling of anesthetic carpule -aseptic technique -practice atraumatic insertion and injection -avoid repeated injections; use regional blocks -use minimum volumes |
|
|
Trismus Management
|
-usually occurs 1-6 days after injections
-record incident and treatment in dental chart -use heat therapy, warm saline rinses, NSAIDs, muscle relaxants (e.g. Valium) -physical therapy (gum chewing) -if trismus/pain continues > 2 days --> add antibiotics -if problem worsens or if not improving after 7 days refer to OMS |
|
|
Causes of Hematoma
|
-effusion of blood into extravascular space
-usually related to arterial injury -related to density of tissues surrounding vessel -PSA (most common site for hematoma, bruise visible on skin) -IAN bruise visible only intraorally |
|
|
Hematoma Problem
|
-trismus and pain
-swelling and discoloration usully subside in 2-3 weeks: inconvenience to patient, source of embarassment to HCP -possible source of infection |
|
|
Hematoma Prevention
|
-knowledge of normal anatomy in injection site
-modify injection technique as dictated by patient's anatomy -use short needle for PSA -minimize number of needle penetrations into tissue -don't use a needle as a probe in tissues |
|
|
Hematoma Management
|
-immediate- apply direct pressure for 5 minutes
-IAN-medial ramus -Infraorbital- directly over foramen -Mental- directly over foramen -PSA: Ice/Pressure on face, digital pressure in mucobuccal fold as far posterior as patient will tolerate |
|
|
Hematoma Subsequent
|
-document in patient's record
-advise patient about possible trismus, discomfort, and dicoloration (bruise) -ice for first 2 hours -heat after first 24 hours -OTC meds -Tincture of time |
|
|
Infection
|
-extremely rare
Causes: -contaminated needle or solution -improper technique -injecting into an area of infection |
|
|
Problem with infection
|
-trismus
-fascial space infection |
|
|
Infection Prevention
|
-use disposable needles
-avoid contamination of needle through contact with nosterile surfaces -avoid multiple injections with the same needle -proper care/handling of carpule -store aseptically in originally ocntainer -cleanse diaphragm with a sterile disposable alcohol wipe -properly prepare tissues prior to penetration: dry, topical anesthetic |
|
|
Edema
|
-swelling of tissues
Causes -trauma during injection -infection -allergy: angioedema from topical anesthetic; vasodilation secondary to histamine release -hemorrhage -injection of irritating solution (alcohol or cold sterilizing fluid) |
|
|
Edema Problem
|
-usually not significant
-occasionally pain and dysfunction in region -angioneurotic edema can compromise airway |
|
|
Edema Prevention
|
-proper care and handling of local anesthetic armamentarium
-atraumatic injection technique -good medical evaluation of patient before treatment |
|
|
Edema Management
|
-if from trauma or irritating solutions: usually no formal therapy maybe Rx analgesics
-If from hematoma : see hematoma If from infection: see infection |
|
|
Edema Management if from allergic reaction
|
in buccal tissues:
-no airway involvement -antihistamines -consult with allergist in tongue, FOM, or pharynx -life threatening -BLS, EMS (911) -epinephrine (.3mg q 5 min), antihistamine, corticosteroid -cricothyrotomy |
|
|
Sloughing of the tissues Causes
|
epithelial desquamation
-prolonged application of topical anesthetic -heightened sensitivity of tissues to local anesthetic sterile abscess -prolonged ischemia -almost always in the tissues of the hard palate |
|
|
Sloughing of the tissues problem
|
-pain (like an ulcer)
-infection (rare) |
|
|
Sloughing of the tissues prevention
|
-topical anesthetics 1-2 minutes
-avoid concentrated vasoconstrictors -avoid reinjection of palatal tissues |
|
|
Sloughing of tissues Management
|
-inform/reassure patient
-document in chart -analgesics |
|
|
Soft tissue injury Cause
|
-child or mentally handicapped adult
-self-inflicted trauma to tongue, lips, or cheeks while tissues are numb |
|
|
Soft tissue injury Prevention
|
-local anesthetic of appropriate duration
-warn the patient and guardian (self adherent warning sticker) -cotton roll between lip and teeth -advise patient to avoid chewing foods until numbness wears off |
|
|
Soft tissue injury management
|
-analgesics for pain
-antibiotics if infection results (rare) -warm NS rinses -lubricant to cover lip lesion |
|
|
Facial Nerve Paralysis Causes
|
-infraorbital block or maxillary canine infiltration
-anesthetic into deep lobe of parotid gland: -too far posterior during IAN block or too deep during akinosi block |
|
|
Facial nerve paralysis Problems
|
-transitory: several hours
-unilateral paralysis of involved muscles -loss of protective lid reflex --> corneal irritation |
|
|
Facial nerve paralysis prevention
|
-adhere to injection protocols
-IAN -contact with bone -akinosi <25mm |
|
|
Facial Nerve Paralysis Management
|
-reassure patient
-eye patch or manually close eye -avoid contact lenses -document in chart |
|
|
Postanesthetic Intraoral Lesions
|
-intense pain and ulcerations at injection site approximately 2 days after intraoral anesthetic injection
-cause: activation of latent form of disease process -recurent apthous stomatitis (probably autoimmune) -herpes simplex virus |
|
|
Postanesthetic Intraoral Lesions Problem
|
-pain in ulcerated areas
-secondary infection (rare) |
|
|
Postanesthetic intraoral lesions prevention
|
-no way to prevent
-can use acyclovir in prodromal phase to minimize the acute phase of the disease process |
|
|
Postanesthetic Intraoral Lesions Management
|
Symptomatic
-reassure patient -analgesics if required -topical anesthetic preparations (viscous lidocaine, 1-2-3 mouth rinse (lidocaine, benedryl, MOM), orabase ointment, zilactin -ulcers usually last 7-10 dyas -document in chart |
|
|
Anatomy of an Aspirating Syringe
|
-Thumb ring
-Finger grip -Spring -Guide bearing -Piston with Harpoon (harpoon most likely to break) -Barrel -Adapter |
|
|
Types of Needle
|
- 25 gauge (Red)
-27 gauge (Yellow) -30 gauge (Blue) |
|
|
Needle Lengths
|
-Short 20mm
-Long 32mm |
|
|
Needle Parts
|
-syringe adaptor
-Hub -shaft -bevel (should be towards nerve you are trying to anesthetize) -cartridge penetration end |
|
|
How to assemble a syringe
|
-place needle on syringe
-pull back on thumb ring to insert carpule into syringe -slowly slide carpule forward to penetrate diaphragm -Use needle puncture guard -engage harpoon into stopper -verify flow of local anesthetic |
|
|
Atraumatic Injection Technique Part 1-7
|
1-use a sterilized sharp needle
2-check the flow of local anesthetic solution 3-solution at room temp 4-Position of the patient-supine if tolerated 5-Dry the tissue 6-Apply topical antiseptic (optional) 7-Apply topical anesthetic |
|
|
Atraumatic Injection Technique Part 8-14
|
8-Communicate with the patient-explain superficial numbness, minimize discomfort
9-establish a firm hand rest 10-make the tissue taut 11-keep the syringe out of patient's sight 12-insert the needle into the mucosa-bevel towards bone 13-watch and communicate with patient-never say it wont hurt 14-inject several drops (optional) |
|
|
Atraumatic injection Technique part 15-21
|
-Slowly advance needle towards target
-aspirate slowly deposit the local anesthetic solution -communicate with the patient-explain why you are injecting slowly -slowly withdraw the syringe and cap the needle using safe technique -observe the patient after the injection -record the injection in the pt's chart |
|
|
Nerves that can be blocked in maxilla
|
-Posterior Superior Alveolar (PSA)
-Infraorbital -Maxillary (2nd division block) -Greater palatine -nasopalatine |
|
|
Nerve Block Advantages
|
-fewer injections (pain) when anesthetizing several sites
-Less total volume of anesthetic soln and less chance of overdose -Lasts longer and more profound |
|
|
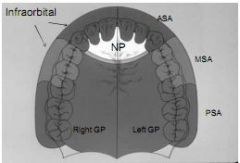
Distribution of Nerve blocks in Maxilla
|
|
|
|
Nerve Block disadvantages
|
-lasts longer
-Greater chance of complication(hematoma, intravascular injection, slightly lower success rate, trismus, anesthesia more wide |
|
|
Structures exiting a foramen
|
-nerves
-arteries -veins |
|
|
Reasons for the bevel toward the bone
|
-bevel away from bone is more likely to penetrate periosteum and cause pain and bruising
-bevel towards bone prevents this |
|
|
Infiltration
|
-depositing fluid that will diffuse through the periosteal and into the nerve near the end of the root
-canine root is longer and less likely to be anesthetized -Muscle attachments can effect distribution of anesthesia can anesthetize molars with a half a carpule |
|
|
Posterior Superior Alveolar Nerve Block (PSA)
|
-anesthetizes maxillary 3rd, 2nd and 1st molars (MB root of 1st molar not anesthetized=28%) and buccal periodontium and facial bone
-Indications: treating >1maxillary molar, infection site, infiltration not effective -Contraindication: risk of hemorrhage too great -angled across 2nd molar crown |
|
|
PSA Advantages
|
-atraumatic
-95% success rate -less injections when treating multiple teeth -less total volume |
|
|
PSA disadvantages
|
-hematoma
-no bony landmarks -2nd injection usually required for 1st molar |
|
|
Infraorbital Nerve Block
|
-Anesthetizes ASA nerve and MSA nerve
-ASA nerve: pulps of incisors and canine -MSA nerve:72% pulp of premolars, MB root of 1st -Infraorbital Nerve (inferior palpebral, lateral nasal superior labial) -Facial bone and periodontium of effected teeth |
|
|
Infraorbital Indication and Contraindications
|
-Indications: multiple teeth, infection, infiltrations not effective
-Contraindications: 1 or 2 teeth, bleeding disorders, anticoagulants |
|
|
Infraorbital nerve block advantages and disadvantages
|
-Advantages: simple, minimal volume of solution, minimal punctures
-Disadvantages: lack of confidence in operator-fear of injury to eye, landmarks usually difficult to palpate |
|
|
Infraorbital nerve block landmarks
|
-lower rim of the orbital
-center of the eye |
|
|
Greater Palatine Nerve Block
|
-Anesthetizes posterior portion of hard palate and its overlying soft tissues, anteriorly as far as the 1st premolar and medially to the midline
-indications: pain control during restorative, periodontal, or oral surgical procedures -contraindications inflammation in site, smaller area of therapy (1 or 2 teeth) |
|
|
Advantages and Disadvantages of Greater Palatine Nerve Block
|
-Advantages: minimizes needle penetrations and volume of solution
-Disadvantages: no hemostasis except at site of injection, potentially traumatic/painful -Alternatives: infiltration, V2 block |
|
|
Target of Greater Palatine Nerve Block
|
-Anterior 1/2 2nd : 0%
-Posterior 1/2 2nd: 40% -Anterior 1/2 3rd: 50% -Posterior 1/2 3rd: 10% |
|
|
Nasopalatine Nerve Block
|
-Anesthetizes nasopalatine nerves bilaterally anterior portion of hard palate (soft and hard tissues) from mesial of right 1st premolar to the mesial of the left 1st premolar
-Indications: restorative, periodontal, or oral surgery procedures on multiple teeth -Contraindications: inflammation or infection in area, smaller area of therapy |
|
|
Nasopalatine Nerve Block Advantages and Disadvantages
|
-Advantages: Fewer needle penetrations, less volume of soln
-Disadvantages: hemostasis only in area of injection, potentially the most painful intraoral injection -Alternatives: local infiltrations, maxillary nerve (V2) block |
|
|
Maxillary Nerve (V2) Block
|
-Anesthetizes: pulpal anesthesia in hemimaxilla, soft tissue and bone and hemimaxilla, skin of lower eyelid, side of nose, cheek, upper lip
-Indications: extensive restorative, periodontal or oral surgery procedures, inflammation or infection precluding other blocks, diagnosis or treatment of neuralias or tics of V2 nerve |
|
|
Maxillary Nerve (V2) Block Contraindications
|
-inexperienced operator
-pediatric patient -uncooperative patient -inflammation or infection at injection site -when hemorrhage is risky -bony obstructions in canal (5-15%) |
|
|
Maxillary Nerve (V2) Block Advantages and disadvantages
|
-Advantages: high success rate-95%
-minimizes needle penetrations (1 vs 4) and volume of anesthetic (1 vs 2 carpules) -usually atraumatic -Disadvantage: risk of hematoma, lack of hemostasis at surgery site, discomfort, arbitrary landmarks -Alternatives - other blocks, infiltrations |
|
|
V2 block methods
|
-Greater palatine canal approach to V2 block
-high tuberosity approach to V2 |
|
|
Inferior Alveolar nerve block general
|
-aka mandibular nerve block
-most commonly used -highest rate of failure (15-20%) -Try and avoid bilateral mandibular blocks (uncomfortable to pt) -most difficult to master |
|
|
Inferior Alveolar Nerve block
|
-nerves anesthetized: inferior alveolar, mental, incisive, lingual (usually)
-indications: procedures on multiple teeth in one quadrant, buccal and lingual soft tissue required -contraindications: infection or acute inflammation, tongue or lip biters (children, mentally handicapped) -Advantages: one injection provides a wide area of anesthesia |
|
|
Inferior alveolar nerve block Disadvantages
|
-sometimes not necessary for localized areas/procedures
-high block failure rate -intra-oral landmarks not consistent -high rate of positive aspiration (10-15%) -lingual and lip anesthesia (biters/hot beverages) |
|
|
Inferior Alveolar Nerve Block Insertion and Target
|
-insertion: mucosa on medial aspect of mandibular ramus
-target: inferior alveolar nerve before it enters the foramen |
|
|
Inferior Alveolar Nerve Block Landmarks
|
-coronoid notch (greatest concavity on the anterior border of the ramus)
-pterygomandibular raphe -occlusal plane of mandibular posterior teeth (6-10 mm above occlusal plane ) |
|
|
Inferior Alveolar Nerve Block Failures
|
-deposition of anesthetic below mandibular foramen
-deposition of anesthetic too far anteriorly -accessory innervation of mandibular teeth (mylohyoid nerve posteriorly and mylohyoid/overlapping fibers of contralateral IAN) -bifid inferior alveolar nerve (lower indicidence) |
|
|
Inferior Alveolar Complications
|
-hematoma (hold pressure)
-trismus -facial paralysis (anesthetic in parotid) |
|
|
Inferior Alveolar Technique
|
-place index finger or thumb on the coronoid notch, pull tissue tight
-6-10mm above the occlusal plane of the mandible & middle of thumb determines height of injection -the anteroposterior point of the injection is 3/4 the distance of the pterygomandibular raphe -align the barrel of the syringe across the contralateral premolars -come across contralateral premolars & anterior to the soft tissues -if you touch bone, redirect around to ipsilateral canine & advance slightly into base of V formed by the pterygomandibular raphe & ramus of mandible -penetration depth is 20-25mm, 2/3 to 3/4 length of long needle |
|
|
Adjunctive Mylohyoid Block
|
-retract tongue to midline, then inject at the apical area of second molar on the lingual surface of the mandible
|
|
|
Adjunctive Contralateral Inferior Alveolar
|
-supraperiosteal injection technique across the midline of the anterior mandibular teeth (buccal surface)
|
|
|
Adjunctive Lingual Nerve Block
|
-deposit .1 to .2ml of anesthetic when withdrawing needle from inferior alveolar block
|
|
|
Inferior Alveolar Signs and Symptoms
|
-tingling or numbness of lip and chin to midline
-tingling or numbness of the inpsilateral anterior two thirds of the tongue -anesthesia of teeth and gingiva ipsilaterally (except buccal nerve distribution) |
|
|
Buccal Nerve Block Complications and Technique
|
-AKA long buccal nerve block
-anesthetizes soft tissues and periosteum buccal to the mandibular molars -indications: buccal soft tissu anesthesia for procedures on the mandibular molars -Contraindications: infection/inflammation in the area -Complications: rare (hematoma) -Technique: penetrate mucosa about 2mm contact bone, aspirate and inject |
|
|
Buccal Nerve Block Advantages/Disadvantages
|
-advantages: easy, high, success rate
-disadvantages: potentially painful if periosteum is torn -insertion: mucosa distal and buccal to the most posterior mandibular molar -target: buccal nerve as it passes over the anterior border of the ramus -landmarks: mandibular molars and mucobuccal fold -failures: rare |
|
|
Gow-Gates Block
|
-Aka mandibular block
-blocks entire distribution of V3 -Anesthesia of inferior alveolar, lingual, mental, incisive, mylohyoid, buccal and auriculotemporal nerves -Difficult learning curve -more successful than inferior alveolar block |
|
|
Gow-Gates Indications/ Contraindications
|
-Indications: procedures on multiple teeth, soft tissue anesthesia , failed inferior alveolar block
-Contraindications: infection/inflammation, lip/tongue biters, pts who are unable to open mouth wide |
|
|
Gow-Gates Block Advantages/disadvantages
|
-Advantages: only one injection
-high success rate (95%) -minimal complications -successful anesthesia of bifid -inferior alveolar nerves, -Disadvantages: tongue/lip anesthesia,-longer time to onset of anesthesia, higher learning curve |
|
|
Gow Gates Block Insertion/Target
|
-insertion: mucosa on the mesial of ramus in line of tragus and commissure distal to the maxillary second molar
-Target (lateral surface of condylar neck, below insertion of lateral pterygoid -landmarks: tragus and commissure, just below mesiopalatal cusp of the maxillary second molar |
|
|
Gow Gates Complications
|
-hematoma (rare)
-trismus (rare) -paralysis of cranial nerve III, IV, VI (eye paralysis diplopia) |
|
|
Gow-Gates Technique
|
-have pt open wide, point of insertion below mesiopalatal cusp of maxillary second molar aiming to tragus of ear (considerably higher than occlusal plane)
-advance needle 20-25mm until bone is contracted aspirate and injection -have pt stay open 1-2min after injection |
|
|
Akinosi Block
|
-aka closed mouth block
-useful when dental therapy required in pts with limited mouth opening (trismus) |
|
|
Akinosi Block Indications/contraindications
|
Indications: limited mouth opening,inability to visualize landmarks for conventional block
Contraindications: infection or acute inflammation, lip/tongue biters, inability to gain access to the lingual aspect of ramus |
|
|
Akinosi Block disadvantages and insertion
|
-disadvantages: difficult to visualize path of needle and depth of insertion , no bone contact
-Insertion: soft tissue overlying medial border of ramus adjacent to maxillary tuberosity at the mucogingival junction height |
|
|
Akinosi Target/Landmarks
|
-soft tissue of the medial ramus (below Gow-Gatesand above inferior alveolar block)
-Landmarks: mucoginigval junction of maxillary (second/third molar), maxillary tuberosity/coronoid notch |
|
|
Akinosi Block Failures/complications
|
-must stay in line with flare of the mandible or injection will be too lateral, needle insertion too low, under/overinsertion of the needle
-Complications: hematoma/trismus, facial nerve paralysis (overinsertion into parotid gland) |
|
|
Akinosi Block Technique
|
-bevel of needle away from bone
-advance needle 25mm -aspirate -inject |
|
|
Mental/Incisive Block
|
-the mental nerve leaves the mental foramen and provides sensory innervation to the lip and chin area
- incisive nerve continues forward to provide sensory innervation to anterior mandibular teeth -both have limited usefullness on a routine basis for dental therapy |
|
|
Mental block indications/contraindications
|
-Indications: buccal soft tissue anesthesia for procedures anterior to the mental foramen (biopsy)
-Contraindications: inflammation and infection in the areas |
|
|
Mental Nerve Advantages/Disadvantages/Failures
|
-Advantages: high success rate, easy/atraumatic
-Disadvantages: hematoma (5%) -Failures: rare, miss the foramen |
|
|
Mental Block Insertion/Target/Landmarks
|
-Insertion: mucobuccal fold anterior to foramen
-Target: mental nerve as it exits the mental foramen -landmarks: mandibular premolars, mucobuccal fold |
|
|
Mental block Complications
|
-complications: hematoma
-Technique: locate foramen with finger in mucobuccal fold, insert needle anterior to foramen (5mm), aspirate and inject |
|
|
Incisive Nerve Block Indications/contraindications
|
-dental procedures which require pulpal anesthesia of the mandibular anterior teeth, used instead of bilateral inferior alveolar blocks for treatment limited to the anterior mandible
-Contraindications: inflammation or infection |
|
|
Incisive Nerve Block Advantages/Disadvantages
|
-advantages: pulpal anesthesia of the anterior mandibular teeth without lingual anesthesia (uncomfortable), high success rate
-Disadvantages: no lingual anesthesia, cross innervation from contralateral inferior alveolar nerve may require additional supraperiosteal injections for pulpal anesthesia |
|
|
Incisive Nerve Insertion/Target/landmarks
|
-insertion:mucobuccal fold anterior to mucobuccal fold
-target: mental foramen (incisive nerve lies in this) -Landmarks: mandibular premolars, mucobuccal fold |
|
|
Incisive Nerve Failure/Complications
|
-failure: inadequate volume of anesthetic, inadequate pressure after injection
-Complications: rare, hematoma |
|
|
Incisive Nerve Technique
|
-same as for mental block
-hold pressure for two minutes after injection to force anesthetic into the foramen and reach the incisive nerve |
|
|
Mandibular Infiltration
|
-useful for supplemental anesthesia of anterior mandibular teeth when getting crossover fibers from contralateral inferior alveolar nerve
-thin cortical plate allows for supraperiosteal injection technique to be successful for mandibular incisors only in most pts -technique exactly the same as for maxillary teeth with deposition of anesthetic at root apex to block dental plexus |
|
|
Injection Pearls
|
-always recap needle after injection
-be confident -understand the anatomy -always use a finger rest for stabilization -if pt complains of an electric shock after the needle is positioned, re-position the needle as you are likely in the nerve itself |