Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
26 Cards in this Set
- Front
- Back
|
OBJECTIVES:
! To learn to identify the clinical signs of respiratory distress in the newborn. ! To understand the pathophysiology of respiratory illnesses in the newborn. ! To learn the clinical presentations and management of the common pulmonary causes of neonatal respiratory distress ! To understand the various airway and lung anomalies which may cause respiratory distress in the newborn ! Investigation and management of common respiratory anomalies ! To develop an understanding of non-pulmonary causes of respiratory distress in the newborn. |
Just objectives
|
|
|
What are the 4 Primary Clinical Signs/ Presentation of Resp Distress in the New Born?
|
1. Cyanosis
2. Grunting 3. Retraction 4. Tachypnea |
|
|
What tool is used to assess Neonatal Respiratory Distress? What variables are measured?
|
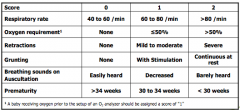
Respiratory Distress Score - ACoRN
Variables: Resp Rate, O2 requirement, Retractions, Grunting, Breathing sounds on Auscultation, Prematurity |
|
|
What 4 questions can help narrow down the diagnosis of Resp distress?
|
(Age, Severity, Timing, Radio)
1. What gestation is the baby (guessing this means age/how early baby was born) 2. How significant is the resp disorder? 3. When did the distress start? 4. What does the CXray show? |
|
|
What are some Pulmonary Causes of Respiratory problems in the new born: Common (3), Less Common (3), Rare (3)
|
Common:
1.Idiopathic RDS (aka Hyaline Membrane Disease) 2.Transient Tachypnea of the New Born (TTN) 3.Aspiration Syndromes Less Common: 1.Pneumonia 2.Pneuomothorax 3.Pulmonary Hemorrhage Rare: 1.Airway Obstruction 2.Abnormal Lung Devo 3.Diaphragmatic Hernia |
|
|
How can Pathophysiology of Lung Development go wrong in A: Normal Lung Devo; B:Abnormal Lung Devo?
|
A: Normal Lung Devo
- Infection - Interference with normal adaptation to extra-uterine life - Interference with air-blood interface B: Abnormal Lung Development - Timing of Delivery - Developmental/Congenital Abnormalities - All can lead to lung AbNorms - form and/or function relationship |
|
|
Pulmonary Embryology (woot!) What are the 5 phases of Lung Development and their Asc. gestational age of development?
|
1.Embryonic Phase - 4th week gestation (6th week preggers)
2.Pseudoglandular Phase - 7-16 weeks (9th-18th) 3.Canalicular Phase - 16-25 weeks (18-27) 4.Terminal Sac Phase - 25-40 weeks (27-42) 5.Alveolar Stage - late fetal-8years old (Langman's =10) |
|
|
The lungs are formed from an ________ of the ________ part of the ______-______ beginning in the ____ week of gestation.
|
The lungs are formed from an -(out-pouching)- of the -(ventral)- part of the -(fore-gut)- beginning in the (4th) week of gestation.
|
|
|
How does Alveolar and Capillary development relate?
|
they are linked
|
|
|
In weeks 7-16 gestation-the ____ phase- what has been completed? What is forming and being deposited? Is Respiration Possible at this time?
|
- Pseudoglandular Phase
- Bronchial Branching is done - Pre-Acinar blood vessels are forming and Connective tissue is deposited after 10 weeks gest. - No Respiration is not possible at this time - lack of Type 2 cell development |
|
|
During what phase and weeks is Respiration possible? Why?
|
-Canalicular Phase - 16-25 weeks
- 22 weeks (earliest) Respiration is "possible" - most places its 23 or later WHY?: - Walls of Air spaces start to thin - Vascularity increases -Terminal Bronchioles have 2+ Respiratory Bronchioles with terminal sacs Present - Most Importantly - Type-2 Cells emerge even though No Alveoli are present yet - requires Resp Bronchioles only |
|
|
What 3 key processes occur in the Terminal Sac Phase?What weeks is this occurring?
|
- Gradual Flattening of the air space
- Type 2 Pneumocyte (aka Type 2 alveolar Epithelial cells) differentiation /surfactant production starts - Capillaries bulge into terminal sacs |
|
|
The Alveolar Stage occurs from ___ to ___ of age. What two processes occur in this time?
|
- late fetal - 8 years
1. terminal Sac Epithelium thins further 2. Surfactant Production matures |
|
|
***What is the most common cause of respiratory distress in term or near term babies? In what population is it more common and why does it occur?
|
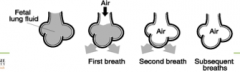
- Transient Tachypnea of the New Born
- it occurs more in ***C-section*** delivered babies - Caused by delay in the the clearance of Residuale lung fluid after birth |
|
|
When do babies present most with TTN? How many require oxygen? When does it resolve?
|
- First few hours of life with mild to moderate Respiratory distress
- with O2 requirement in <40% (I'm pretty sure that's what was meant?) - Resolves once residual lung fluid is reabsorbed - from minutes to hours after birth but... ***can last up to 72 hours*** |
|
|
Name a type of Aspiration Syndrome Discussed in Lecture
|
Meconium Aspiration Syndrome
|
|
|
Answer: This is a disease of post-term, term, and occasionally near-term babies. (Jeopardy style)
When is it: worse, more common, acquired? What does it result in? What's the presentation? |
Question: What is Meconium Aspiration Syndrome
- Worse if the meconium is thick or particulate - More common if the baby is depressed at birth - Acquired Perinatally Results in: - Combination of large and small airway obstruction -Pneumonitis -Surfactant inactivation -Ventilation: perfusion Mismatch - How does this mismatch alter O2 saturation levels? -Presents Immediately after birth with any degree of O2 requirement/severity of respiratory distress -***may be accompanied by persistent pulmonary HTN of the new born*** - Severe MAS is life threatening and requires prompt specialized care |
|
|
Pneumonia in the new born is usually due to infection and ______ rather than lobar in appearance
|
Diffuse
|
|
|
When is Pneumonia in the New Born more likely to occur?
|
In the presence of Risk factors for sepsis: ie. prolonged rupture of membranes, maternal colonization with GBS, or chorioamnonitis)
|
|
|
When/How will pneumonia present in the new born?
|
- Maybe in the first few weeks depending on source of infection
- At any level of Resp Illness - Babies may/may not be systemically ill at onset, but clinical course may be fulminant - |
|
|
When should a Respiratory disease in the new born be treated with IV Antibiotics?
|
With the inability to rule out Pneumonia via clinical OR radiographic appearance
|
|
|
Who is Respiratory Distress Syndrome mostly a disease of? How does it relate to age?
|

- Primarily a disease of Preterm Babies
- Incidence increases with decreasing Gestational Age |
|
|
Describe the Pathophysiology of Respiratory Distress Syndrome (5 points)
|
1. Lack of Surfactant
2. Decreased Alveoli # 3. Increased Resistance 4. Thick Alveolar Walls 5. Results in Progressive collapse of the terminal bronchioles/alveoli |
|
|
Name two abnormalities that can cause Hypoxemia and Hypercarbia in a New Born
|

Acute: - Inadequate Surfactant
Chronic: - Structurally Immature Lung |
|
|
How do babies present with RDS?
|
- Any degree of Resp Distress and O2 requirements
- *** Presents at <3 hours of age AND persists beyond 6 hours of age and during first few days*** |
|
|
How might TTN and RDS be differentiated On Exam?
|
- Edema and decreased urine out put are much more common in RDS than TTN
|