![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
403 Cards in this Set
- Front
- Back
|
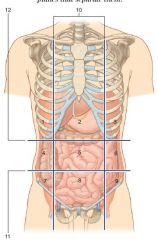
what's the purpose of abdominal regions |
to describe the site of abnormalities i.e masses |
|
|
1. Right hypochondrium
2. Epigastric 3. Left hypochondrium 4. Right lumbar 5. Umbilical region 6. Left lumbar 7. Right iliac/inguinal 8. Pubic region9. Left iliac/inguinal 10. Midclavicular planes 11. Intertubercular plane 12. Subcostal plane |
|
|
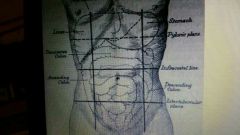
2 horizonal lines that make up quadrants |
1. subcostal plane 2. Transpyloric plane |
|
|
2 Vertical lines and their positions |
L&R mid-clavicular passing through ipsilateral mid-inguinal point |
|
|
Location of transpyloric plane
|
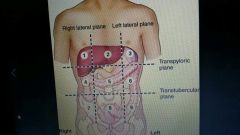
- between sternal notch and upper border of pubic symphysis
-L1 |
|
|
transtubecular plane location
|
-through iliac tubercles (lie on iliac crest forming its lateral part) at L3
|
|
|
Organs in Right upper quandrant
|
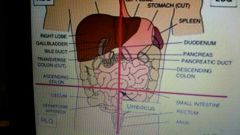
Liver
Gall bladder R kidney and adrenal gland Colon Duodenum with head of pancreas Small intestine Bile duct L GB KA C DP SI |
|
|
LUQ organs
|
Stomach
Spleen Pancreas Kidney + Adrenal gland Colon (splenic flexure ) JeJunum |
|
|
LRQ organs
|
-colon ascending
-caecum -appendix (mc burney's point) -Ileum |
|
|
Left Lumbar Quadrant Organs
|
-Colon- descending
-Sigmoid -SI |
|
|
Is the liver palpable |
yes, just below costal margin |
|
|
Is the spleen palpable |
no- only when enlarged or in slender patients |
|
|
IS the GI tract palpable
|
not normally but some of the colon can be palpitated if pathological
E.g sigmoid Colon in chronic constipation |
|
|
in what case are retroperitoneal organs such as kidney, spleen palpable |
when enlarged |
|
|
RHR organs
|
Liver and Gall bladder
Kidney+ adrenal gland Colon- hepatic flexure (ascending) |
|
|
Epigastric region
|
liver transverse C abdominal aorta and IVC Pylorus and Duodenum: first part |
|
|
LHR
|
stomach
spleen K+A Colon |
|
|
RLR |
Kidney Colon small intestines |
|
|
Umbilical region
|
T colon pancreas and Duodenum Ab aorta, vena caca Small Intestine Iliac vessels |
|
|
LLR
|
Kidney
D colon pancreas Jejunum |
|
|
RIR
|
caecum
appendix Ileum |
|
|
Hypo R
|
distendible organs of pelvis
SI Iliac vessels Spermatic cords |
|
|
LIR |
sigmoid colon SI |
|
|
Position of the Liver
|
-mostly R hypochondrium and epigastric
-upper border is at 5th rib |
|
|
Gall bladder location |
-tip of 9th costal cartilage on the right - where lateral border of rectus abdominis crosses costal margin on transpyloric plane |
|
|
Rectus Abdominis: attachments, function, lateral border
|
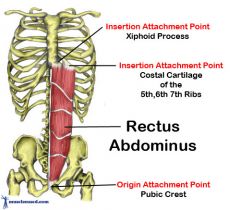
-A: inferior edges of 5-7th costal cartilages, xiphoid process, pubic symphysis, pubic crest
-F:flexes trunk, compresses abdominal viscera, controls tilt of pelvis Lateral border: Linea semilunaris |
|
|
Stomach Location |
-pylorus (consistenly placed part) at transpyloric plane -pylorus descends on supine position -Fundus lies at 5th rib of midclavicular line |
|
|
the transpyloric plane marks the position of what organs? |
-gall bladder -renal hila -spleen Hilum -origin of SMA |
|
|
Duodenum and pancreas location |
head: just below and right of pyloric position Duodenum: curves from pylorus rightwards, downwards and leftwards to reach transpyloric plane |
|
|
Appendix Location |
Mcburney's point 2/3 between umbilicus and ASIS |
|
|
The mesentry location |
-root attached to posterior abdominal wall -extends from 4th part of duodenum to Mcburney's point |
|
|
Colon regions
|
Ascending: Mcburney's point to transpyloric plane
Transverse: hangs at umbilicus and rises to the left lumbar regions Sigmoid: crosses to centre of hypogastric |
|
|
Spleen Location |
-between 9th and 10th ribs -between erector sipnae muscle and midaxillary line |
|
|
Kidneys location |
Hila: transpyloric plane Posteriorly: covered by 11th & 12th Ribs positions change by 5 cm when supine |
|
|
Abdominal aorta palpitation |
can be felt by pulsing forcefully by the lumbar vertebrae bodies to the left of midline
|
|
|
Desceding colon palpitation |
can be felt in L lumbar region due to solidity of its contents |
|
|
Liver palpitations |
-palpable in infants |
|
|
Spleen palpitation
|
-palpable in infants as a mass descending from left hypochondrium
- cannot be felt in adults unless 3x its size |
|
|
GI tract palpitations |
- normally impalpable -in chronic constipation S colon filled with faeces and can be felt in left iliac fossa -caecum and S colon if inflamed can be palpated in left iliac fossa |
|
|
uterus and ovaries palpitations |
- common site for cancer, fribrois etc... -masses can be felt in iliac fossae or hypochondrium -uterus palpitated in 12th week of pregnancy |
|
|
Urinary bladder palpitations |
-can be palpitated in abdominal region in infants in hypochondrium when full (300-500ml) -in Adults palpitable when full above pubic symphysis |
|
|
Why is suprapubic puncture of the distended bladder possible without damage to peritoneal cavity?
|
Bladder is retroperitoneal
|
|
|
If muscles are retracted nerves are also retracted why is that clinically useful ?
|
.
|
|
|
Where does the neurovascular plane of anterior abdominal wall lie ? |
between intermediate and deepest muscle. between Internal oblique and transversus abdominis |
|
|
how is the rectus sheath formed |
from aponeuroses of the 3 muscle layers |
|
|
where is the inguinal ligament located |
from ASIS to pubic tubercle |
|
|
what forms the lower border on the layers of the abdominal muscles
|
Inguinal ligament
|
|
|
Whats an aponeurosis |
tendinous sheath which connects/anchors muscles |
|
|
Functions of Anterior abdominal wall muscles
|
- compress and support abdominal organs
-flex and rotate trunk -expiration -stabilises and controls tilt of pelvis |
|
|
NErve supply to skin and muscles of AAW |
- T7-T11 spinal nerves - T12 subcostal nerve - First lumbar nerves, Iliohypogastric and ilioingunal - |
|
|
Which dermatome lies at the level of: i) the xiphisternum? ii) the umbilicus? iii) the pubic tubercle? |
i) T7 II) T10 iii) L1 |
|
|
What name is given to the fascia in the perineum continous with the scarpa's fascia ? |
Colles Fascia |
|
|
what is the name given to boundaries formed by ataching to colles fascia |
Superficial perineal pouch |
|
|
In which direction do external oblique fibres run ? |
downwards medially |
|
|
Which muscle's inferior border is thickened to form inguinal ligament |
External oblique |
|
|
where is the inguinal canal located ?
|
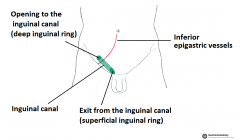
superior to pubic tubercle
|
|
|
superficial inguinal ring LOCATION |
-MARKS END OF INGUINAL CANAL AND LIES SUPERIOR TO PUBIC TUBERCLE -TRIANGLE SHAPED OPENING FORMED BY INVAGINATION OF EXTERNAL OBLIQUE |
|
|
WHAT STRUCTURES PASS THROUGH INGUINAL RINGS ?
|
SPERMATIC CORD OR ROUND LIGAMAMENT IN FEMALES
as well as blood vessels, lymphatic vessels, and the ilioinguinal nerve (which enters the canal from the side, rather than passing through the deep ring). |
|
|
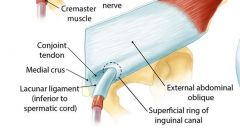
How is the aponeurosis of external oblique arranged at THE POINT THEY FORM THE SUPERFICIAL INGUINAL RING ? Which component of thespermatic cord is formed from this aponeurosis?
|
- EXTERNAL OBLIQUE FORMS ANTERIOR WALL IF THE RING -IT DIVIDES TO FORM MEDIAL AND LATERAL CRURA FORMING SUPERFFICIAL iNGUINAL RING -external oblique gives rise to external spermatic fascia |
|
|
fibres of internal oblique. In which direction do they run? |
upwards |
|
|
How do the fibres of internal oblique relate to the inguinal ligament? |
It originates from the lateral 2/3 of the inguinal ligament |
|
|
In which direction do the fibres of transversus abdominis run? |
transversally |
|
|
How do the fibres of transversus abdominis relate to the inguinal ligament? |
it originates from the 1/3 of the inguinal ligament |
|
|
What and where is the conjoint tendon? |
-combined insertion of transversus abdominis and internal oblique -It is at the pectineal lines and pubic crest |
|
|
What and where is the transversalis fascia? |
the internal surface of the transversus abdominis -It is continuous with the general fascia of the abdomen to the extent that it is regarded by some as a part of the extraperitoneal connective tissue. |
|
|
what is the Linea alba |
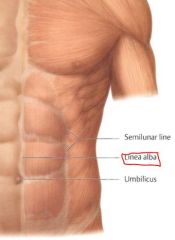
white line formed by the joining of aponeurises |
|
|
What is the linea smilunaris |
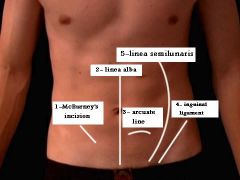
marks lateral border of rectus abdominis |
|
|
Arcuate line |
line between aponeurosis posterior wall and transversalis fascia of rectus sheath |
|
|
Which vessels run in the rectus sheath, deep to rectus abdominis muscle? |
superior and inferior epigastric arteries and veins |
|
|
Ingunal canal
|
-lies above medial half of inguinal ligament
-extends from deep inguinal ring to superficial inguinal rings -has spematic cord and round ligament in female - It is the route by which the testis descends into the scrotum inthe male foetus -forms weak point especially in males |
|
|
Testis and development |
-Testes push way into anterior abdominal wall -as this happens testes and ductus vas defs acquire coverings of abdominal wall |
|
|
From what is the tunica vaginalis derived? How? |
-from peritoneum when testes descend to scrotum |
|
|
What is the cremasteric reflex? |
contraction of the cremastor muscle by lighty stoking the medial aspect of the thigh |
|
|
what structures run in spermatic cord
|
testicular artery, ductus dus deferens, cremasteric artery, genital pempiniform venous, venous plexus, sympathetic nerve fibres, genitofemoral nerve, lymphatic vessels, vestige of process vaginalis.
|
|
|
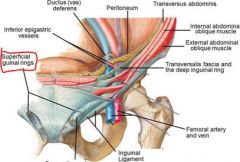
where is the deep inguinal ring located ? |
superior to inguinal ligament + lateral to inferior epigastric artery |
|
|
Boundaries of canal? |
-The anterior wall is formed by the aponeurosis of the external oblique, and reinforced by the internal oblique muscle laterally.
-The posterior wall is formed by the transversalis fascia. -The roof is formed by the transversalis fascia, internal oblique and transversus abdominis. -The floor is formed by the inguinal ligament and thickened medially by the lacunar ligament |
|
|
What is the approximate length of the inguinal canal?
|
4 cm |
|
|
What are the boundaries of the superficial inguinal ring? |
pubic crest and tubercle |
|
|
Which nerve enters the inguinal canal through the deep ring? What does it supply?
|
Genitofemoral nerve
-crematoric muscle -skin of scrotum -mons pubis -upper anterior thigh |
|
|
How does the ilioinguinal nerve enter the inguinal canal? What does it supply? |
- enters obliquely - supplies upper medial thigh, roof of penis, anterior surface of scrotum, mons pubis, labium majus. |
|
|
What is a hernia |
protrusion of parietal peritoneum and viscera through a normal or abdominal opening from cavity in which they belong |
|
|
difference between Direct and Indirect |
Direct: weakness of anterior abdominal wall muscles. lateral to edge of conjoint tendon in the inguinal triangle and rarely descends into scrotum. lies medial to inferior epigastric artery and protruds forward to superficial inguinal ring, rarely through. acquired and develops after birth Indirect: patency of processus vaginalis. passes through deep inguinal ring, inguinal canal, and superficial inguinal ring and descends to scrotum. lies lateral to inferior epigastric vessels. it is congenital |
|
|
what is a reducible hernia |
it can be returned back to its normal place in peritoneal cavity |
|
|
a cruciate incision: |
A vertical incision just to the right of the midline, from the costal margin to the pubis. • A horizontal incision through the umbilicus, running laterally on each side for about 10cm |
|
|
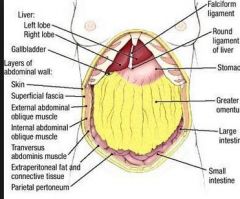
Parietal peritoneum
|
-lines abdominal wall cavities
-clothes anterioir and posterior abdominal walls |
|
|
What is the nerve supply of the parietal peritoneum? |
-thoracolumbar nerves T7-11 -Subcostal nerve (T12) -iliohypogastric and inguinal nerves (L1) |
|
|
The visceral peritoneum
|
-continuous with the parietal peritoneum
-leaves posterior abdominal wall to invest in viscera -passes in front of organs in some cases e.g duodenum - in some cases t forms a mesentry (2 layers) -The upperparts of the pelvic organs (rectum, uterus, bladder) project into the abdominal cavity and aretherefore covered by visceral peritoneum which hangs down in depressions or pouchesbetween them. |
|
|
What characteristic does suspension by a mesentery confer on the suspended organ? |
- Neurovascular and lymphatic communication -organ mobility |
|
|
When in situ, which of the following organs lie retro-peritoneally on the posterior abdominalwall?
|
duodenum, pancreas, rectum (middle third, ascending and desceding colon |
|
|
falciform ligament which runs from the anterior wall ofthe abdominal cavity to the liver. Its free border contains the ligamentum teres.Of what is the ligamentum teres a remnant?
|
Umbilical vein |
|
|
Where is the ligamentum teres |
in the free border of the falciform ligament |
|
|
What is an adhesion? |
Abdominal adhesions are bands of scar tissue that form between abdominal tissues and organs, causing them to stick together.
|
|
|
What is attached to the posterior surface of the greater omentum |
transverse colon |
|
|
what structure divides abdominal cavity into dividing the abdominal cavity into a supracolic compartment and aninfracolic compartment |
mesocolon AKA mesocolic shelf |
|
|
where is the hepatic flexure located |
on the right handside under the liver |
|
|
splenic fexure |
on left handside under spleen |
|
|
what lies between liver and diaphragm
|
the subphrenic space |
|
|
The subprenic space is divided into 2 parts by what ligament |
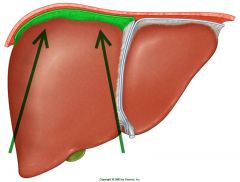
falciform ligament |
|
|
What ligament stops your hand running all the way through the subphrenic space |
coronary ligament |
|
|
what structure bounds the bare area of the liver |
coronary ligament |
|
|
where is the sub hepatic channel
|
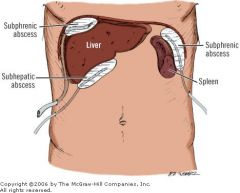
-under the liver
-its inferior limit is the transverse mesocolon |
|
|
what is on the right of the subhepatic channel by the right kidney |
hepato-renal pouch (ofRutherford Morison). |
|
|
what structure is continuous with the paracolic gutter |
hepato-renal pouch (ofRutherford Morison). |
|
|
The hepato-renal pouch is of surgical importance. Why?
|
INtraperitoneal fluid can collect here
-common site for subphrenic abscess. -infects can spread from gall bladder and other neighbouring organs |
|
|
Lesser omentum |
-suspends lesser curvature of the stomach and first part pf duodenum |
|
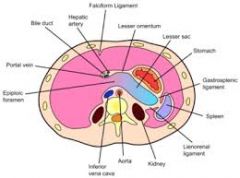
Free margin of lesser omentum |
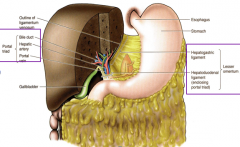
lies immediately anterior to epiploic foramen ( space under lesser omentum ) -free border of lesser omentuis is AKA duodenohepatic ligament forming anterior boundary of epiploic foramen The lesser omentum consists of two layers of peritoneum. Between these two layers, at the free border, pass the portal vein, the hepatic artery, the hepatic, cystic, and common bile ducts, and the nerves and lymphatics. |
|
|
What is the embryological origin of the lesser omentum? |
VEntral mesentry |
|
|
lesser sac
|
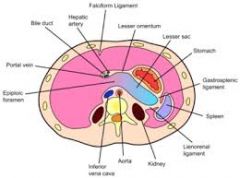
- lies posterior to the stomach and lesser omentum
-connects with the greater sac via epiploic foramen - space enclosed between the anterior and posterior layers of the greater omentumis part of the lesser sac. |
|
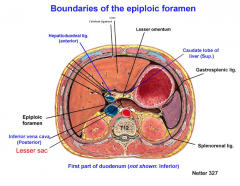
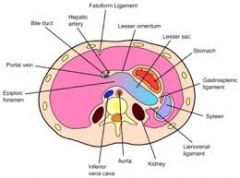
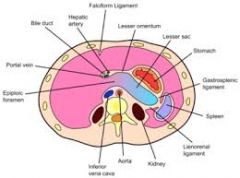
what makes up the anteriorn posterior, superior and inferior margins of epiplpoic foramen
|
--anterior margin: hepatoduodenal ligament/ free border of lesser omentum ( with portal triad)
-posterior margin: IVC, diaphragm -superior margin: covering of caudate lobe -inferior margin: peritoneum covering of duodenum (first part) |
|
|
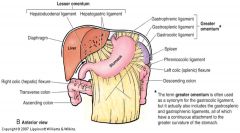
How many layers of peritoneum make up the greater omentum:a) as it runs between the greater curvature of the stomach and the transverse colon? |
4 layers |
|
|
How many layers of peritoneum make up the greater omentum: b) inferior to the transverse colon? |
2 |
|
whats the gastrocolic ligament |
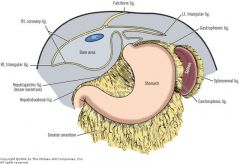
The part of the greater omentum between the greatercurvature and the transverse colon |
|
|
ligament between greater omentum and spleen |
gastrosplenic ligament |
|
|
in what ligamnet does the terminal part of the splenic artery run into |
lienorenal ligament |
|
|
where is the lineorenal ligament located
|
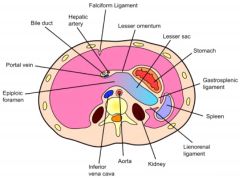
From the pleen, this same fold continues to the posterior abdominal wall where it attaches in theregion of the left kidney, forming the lienorenal ligament.
|
|
|
The infracolic compartment
|
- is of greater sac -lies below transverse mesocolon -contains main mass of intestinal coils -contains iliolumbar fossa |
|
|
which is higher hepatic flexure or splenic flexure |
splenic flexure, hepatic is lower due to bulk of liver |
|
|
the phrenico-colic ligament.
|
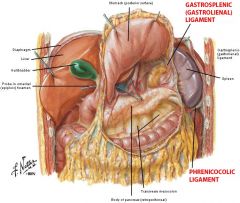
the small transverse fold of peritoneum between the splenicflexure and the diaphragm |
|
|
wheres the beginning of the ascending colon
|
iliac fossa
|
|
|
why are the communications of the paracolic gutters important |
- there is no communication between left paracolic gutter and the left subphrenic space because of the phrenicocolic ligament -on the right there is a communicatin which is clinically significant because the connection aids spread infection |
|
|
does the duodenum have a mesentry ? |
nope |
|
|
what mesentry suspends the SI |
the mesentry proper |
|
|
where does the attachment of the mesentry of the small intestine begin? |
s at the duodenojejunal flexure and slopes downwardsand to the right sacroiliac joint |
|
|
where is the root of the mesentry proper |
The line of attachment of the mesentery to the posteriorabdominal wall |
|
|
Which side of the infracolic compartment communicates with the pelvis?
|
left infracolic compartment
|
|
|
where does the SI terminate |
right iliac fossa |
|
|
what does the mesoappendix contain |
-appendicular artery + vein,iliocoic vein, lymph nodes and nerves |
|
|
sigmoid colon in the pelvis is suspended by what |
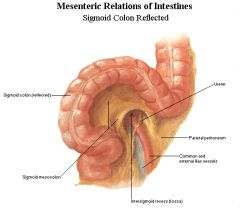
It is suspended by the sigmoidmesocolon, which attaches it to the pelvic wall in an inverted “V” arrangement over thedivision of the left common iliac artery. |
|
|
Sensation from viscera can be crudely divided into “normal” (usually associated withmotility and/or distension) and “abnormal” (i.e. painful). “Normal” sensory information from an organ is generally transmitted through visceralsensory fibres that accompany the parasympathetic motor fibres supplying that organ.What is the parasympathetic motor supply to:(i) the fore- and midgut?(ii) the hindgut?(iii) the bladder?
|
i ) the fore- and midgut? : T9-10 and 11 (thoracic splanchnic nerves)
(ii) the hindgut? L1+L2 (lumbar nerves) (iii) the bladder? S2-S4 (sacral plexus |
|
|
sympathetic supply to bladder |
T11 to L2 |
|
|
“Painful” sensory information from an organ (usually as a result of abnormaldistension of the organ) is generally transmitted through visceral sensory fibres thataccompany the sympathetic motor fibres supplying that organ. What is the sympathetic motor supply to the abdominal and pelvic viscera? |
T5-L3 |
|
|
through what visceral sensory fibres is “Painful” sensory information from an organ (usually as a result of abnormaldistension of the organ) is generally transmitted |
through visceral sensory fibres thataccompany the sympathetic motor fibres supplying that organ. |
|
|
wher eare painful sensations from viscera vaguely localised despite location of viscus |
Painful sensations from the viscera are vaguely localised to the median plane, no matterwhat the location of the viscus. |
|
|
Why does pain from parietal layers localise well ? |
because parietal layers are innervated by sensorybranches of somatic nerves. Therefore, if the pathology comes to include the parietalmembranous layer, the pain now localises well, because it signals through thesomatic systems. |
|
|
Which somatic nerves supply the parietal peritoneum? |
Spinal : thoracolumbar : t7-11 subcotal nerves: T12 iliohypogastric +ilioinguinal L1 |
|
|
1. when only the vermiform appendix and visceralperitoneum are inflamed where is the pain felt ? 2.as soon as parietalperitoneum in the right iliac fossa is involved, the pain localises to what ? |
1. pain is felt in the central abdomen
2. to the fossa |
|
|
in appendicitis does one feel pain in appendix |
no |
|
|
whats the gastrocolic ligament |
ligament ie. that part of the greater omentum running to thetransverse colon. |
|
|
Define the boundaries of the lesser sac.
|
anterior wall -peritoneum of lesser omentum -posterior surface of stomach -anterior two layers of greater omentum posterior wall -peritoneum that covers the diaphragm, pancreas, left kidney and adrenal gland, and duodenum -posterior two layers of the greater omentum |
|
|
Is the cardiac orifice an "anatomical" sphincter? |
no, serves as physiological sphincter relaxing muscles as food enters stomach |
|
|
is pylorus an "anatomical" sphincter? |
yes has circular muscle layers controls discharge of food into duodenum |
|
|
At what vertebral level does the pylorus normally lie? This is the level of the “transpyloricplane”. |
L1 |
|
|
branches of which nerve sink in muscular wall of stomach |
vagus |
|
|
How does the left vagus come to lie anteriorly on the stomach and the right vagusposteriorly?
|
l. vagus from L vagal trunk enters abdomen on anterior surface of oesophagus. it divides into branches whiich supply anterior part of stomach R. Vagus forms posterior v. trunk which divides from posterior oesophagus to supply posterior stomach |
|
|
Anterior relations of stomach
|
Ant abdominal wall
l. costal margin L pleura and L lung lobe of liver |
|
|
posterior relations of stomach |
lesser sac, diaphragm, spleen, adrenal gpand, upper part of kidney, splenic arterty, pancreas, transverse colon |
|
|
What is a hiatus hernia? |
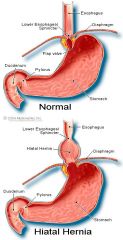
protrusion of upper par of stomach into thorax through a tear/weakness in oesophageal hiatus |
|
|
How does a hiatus hernia differ from a congenital diaphragmatic hernia?
|
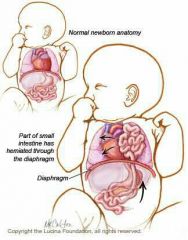
diaphragmatic hernia is congenital usually in new borns involves the small intestine
Hiatus hernia is acquired (sliding hernia- stomach slides through oesophageal sphincter) |
|
|
what does the coeliac trunk supply |
Supplies foregut, liver pancreas, and spleen |
|
|
Branches of coeliac trunk |
Left Hand Side (LHS) Left gastric artery] Hepatic artery Splenic arter |
|
|
what does the SMA supply |
midgut |
|
|
what does IMA supply |
hindgut |
|
|
at what level vertebra is the coeliac trunk given off |
T2 |
|
|
Left gastric artery course |
-enters at lesser omentum -runs along lesser curvature of stomach |
|
|
components of midgut |
lower duodenum, jejunum, ileum, caecum, appendix, 2/3 of transverse colon |
|
|
The superior mesenteric artery supplies the midgut, list the components of the midgut |
- duodenum (3&4) - jejunum - ileum - cecum - appendix - ascending colon - transverse colon (1st half) |
|
|
list below five points that will enable a surgeon todetermine the level of a loop of small intestine during an operation.
|
-jejunum has greater diameter
-jejunum has thicker walls -jejunum has larger more numerous circular folds and villi -Jejunum is longer and is a deeper red/pink -Jejunum has less fat in mesentry |
|
|
What is Meckel’s diverticulum? |
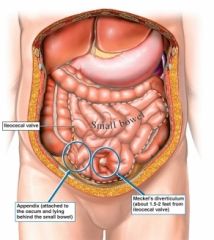
is a slight bulge in the small intestine present at birth and a vestigial remnant of the omphalomesenteric duct (also called the vitelline duct or yolk stalk) |
|
|
Where are diverticuli common |
sigmoid colon |
|
|
What is diverticulosis? |
–Multiplefalse diverticula formed from evaginations of colonic mucosa- common in sigmoid collon |
|
|
What is diverticulitis? |
–Inflamed/infectedand/or ruptured diverticula can erode arteries and cause hamorrhage and can lead to faecal matter in peritoneum causing peritonitis |
|
how far can can the retrocaecal fossa be extended |
liver |
|
|
where is the vermiform appendix attached |
posteromedial wall of caecum below ileocaecal junction. |
|
|
why is it dangerous to use laxative in suspected appendicitis |
vigorous contraction of the gut wall often ruptures theinflamed appendix, precipitating peritonitis). |
|
|
point of maximum tenderness during appendicitis |

mc burneys point. This lies at the junction of the lateral one-third with the medial twothirdsof a line joining the anterior superior iliac spine to the umbilicus. |
|
|
in what % of adults is the appendix retrocaecal |
65 |
|
|
where does the appendix lie in 25% of people |
hangs over pelvic brim |
|
|
The colon is most easily freed from itslateral side. Why? |
because it possesses a short mesentry allowing it to move |
|
|
the ascending colon rums from------ to ------ |
It runs from the right iliac fossa to the hepatic flexure underthe right lobe of the liver |
|
|
At what vertebral level is the superior mesenteric arterygiven off? |
L1 (*inferior= L3) |
|
|
Where does the superiorpancreatico-duodenal artery come from?
|
gastro-duodenal artery |
|
|
From which side of the superior mesenteric artery do the following vessels arise?
• jejunal; • ileal; • ileocolic; • right colic; • middle colic |
• jejunal; left • ileal; left • ileocolic; right • right colic; right • middle colic. right |
|
|
List the components of the hindgut. |
- the distal third of the transverse colon and the splenic flexure, -the descending colon, -sigmoid colon and rectum. |
|
|
Which vessels contribute to the formation of the marginal artery? What does it supply?
|
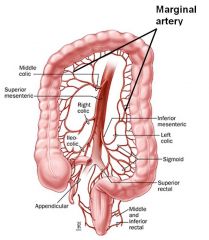
IMA ,Middle colic, left colic, sigmoid arteries and superior sigmoid. they sypply transverse colon |
|
|
Attempt to explain why this gradual obstruction of the IMA doesn’t impair gutfunction.
|
because blood can still get to the gut from other arteries such as the colic artery and marginal arteries arising from SMA -Aneurysm repair often involves ligation or obstruction of the inferior mesenteric artery, againusually without impairing gut function. |
|
|
the colon |
has haustra, taeniae coli, |
|
|
at what vertebra leve l does sigmoid colon continue as rectum |
S3 |
|
|
at what junction are the taenia coli and appendices epiploicae are no longer present on the surface of the largeintestine. |
From the rectosigmoid junction
|
|
|
What is a sigmoid volvulus? Why is it a serious condition? |

This occurs in cases of long-standing chronic constipation where patients develop a large, elongated, relatively atonic colon. a large sigmoid loop full of faeces and distended with gas twists on its mesenteric pedicle to create a closed-loop obstruction. If uncorrected, venous infarction leads to perforation and faecal peritonitis, and ischaemia |
|
|
describe course of rectum |
runs from the rectosigmoid junction to the ano-rectal junction which lies at thelevel of the pelvic floor
|
|
|
How do the peritoneal attachments of the rectum differ from those of the sigmoid colon?
|
upper= peritoneal
Mid: sub peritoneal lower: retroperitoneal |
|
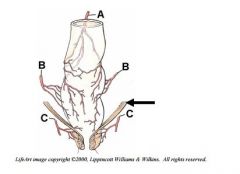
Label vessels A, B and C on the following diagram of the rectal arteries. Where does eachof these vessels originate |
a- superior rectal a. is from IMA b- middle rectal arteries from internal iliac c. inferior rectal arteries from internal pudendal |
|
|
What is the definition of a portal vein? Are there any other examples elsewhere in the body? |
-blood flow that bypasses the heart -splenic portal vein, left gastric, superior rectal |
|
|
midgut drainage |
Each branch of the superior mesentericartery is accompanied by a vein. All these veins ultimately flow into the superiormesenteric vein, a large trunk which lies to the right of the artery. Superior mesenteric veinunites with the splenic vein posterior to the neck of the pancreas to form the portal vein. Note that it is named portal vein above and superior mesenteric vein below the level of entryof the splenic vein, but the two represent a single continuous trunk. Remember that theportal vein runs in the free edge of the lesser omentum. |
|
|
where does the protal vein run |
in free edge of lesser omentum |
|
|
what drains the hindgut |
IMV |
|
|
IMV drainage |
receives tributaries identicalto the branches of the inferior mesenteric artery. The inferior mesenteric vein runssuperiorly, well to the left of the corresponding artery, and usually joins the splenic veinbehind the body of the pancreas, just before the union of the splenic vein with superiormesenteric vein.
|
|
|
What is the purpose of the portal circulation?
|
to supply the liver with metabolic substrates which it detoxifies before reaching systemic circulation |
|
|
where do oesophageal veins drain |
azygous vein |
|
|
Portosystemicanastomoses |
A.Betweenportal left gastric vein and systemic submucosal oesophageal veins B.Between portal superior rectalvein and systemic inferior and middle rectal veins C.Betweenportal paraumbilical veins and systemic epigastricveins D.Between twigs of portal visceralveins in bare areas of secondarily retroperitoneal organs and systemicretroperitoneal veins draining posterior abdominal wall or diaphragm |
|
|
Portosystemic anastomoses, What is their clinical significance? |
they can become congested and cause portal hypertension A.Inportal hypertension (from alcoholic liver disease) flow reverses causingenlargement of submucosal oesophageal systemic veins whichcan rupture causing lifethreatening haemorrhage B.Normal appearance is varicose. Ifrectal mucosa prolapses, haemorrhoids result C.Theseanastomoses are responsible for caput medusae sign in alcoholic liver diseaserelated to portal hypertension D.If tumour or liver disease causesobstruction to flow in valveless portal vein and branches, blood can reach IVC via twigs of visceralveins at bare areas of secondarily retroperitoneal organs (including at liver)m |
|
|
Lymph drainage of the gastrointestinal tract
|
From virtually the whole length of the gastrointestinal tract, the lymph vessels pass backalong the course of the arteries to lymph nodes that lie in front of the aorta at the origins ofthe coeliac, superior and inferior mesenteric arteries. These are called the coeliac, superiorand inferior mesenteric groups of lymph nodes.
|
|
|
what are preaortic nodes, where do they drain? |
The coeliac, superior mesenteric and inferior mesenteric lymph nodes are also termed preaorticnodes. They drain into each other from below upwards, the coeliac group itselfdraining into the cisterna chyli. |
|
|
Which lymphatic channel originates from the cisterna chyli? Where does this channel runand where does it empty its contents?
|
thoracic duct at L2 l. of head, neck, chest, upper limb and chest wall l. internal jugular and subclavian |
|
|
What are Peyer's patches?
|

aggregatedlymphoid nodules, they form an important part of the immune system by monitoring intestinal bacteria populations and preventing the growth of pathogenic bacteria in the intestines
|
|
|
Nerve supply of the gastrointestinal tract
|
-All parts of the gut and its derivatives are innervated by parasympathetic and sympatheticnerves.
-These fibres modify the activity of the intrinsic nerve plexuses of the gut |
|
|
In which layers of the gut wall are the intrinsic (myenteric) nerve plexuses located?
|
between circular and longitudinal layers |
|
|
Most of the autonomic fibres to the gut travel via.......although the parasympathetic fibres to the hindgut (which originate fromsacral segments of the spinal cord) travel via t............ |
1. the coeliac plexus, which is located aroundthe coeliac trunk
2.he inferior hypogastric (pelvic) plexus |
|
|
The coeliac plexus receives its parasympathetic input from the two vagus nerves. What is their function?
|
The function of the vagus nerve is to stimulate smooth muscle contraction and glandular secretions in these organs. For example, in the stomach, the vagus nerve increases the rate of gastric emptying, and stimulates acid production. so increases peristalsis
|
|
|
Where do splanchnic arise? How do they reach the abdomen?
|
-arise from sympathetic trunk
-pierces through diaphragm and descends on vertebral colum - R trunk lies posterior to inferior vena cava and L beside aorta -each give off 5 lumbar ganglia -give rise to lumbar splanchnic nerves which join celiac, intermesenteric, and superior hypogastric plexuses. Both sympathetic trunks continue into the pelvis anterior to the sacrum. pelvic splanchnic nerves (s2-4_ |
|
|
Where would a patient feel pain referred from • foregut? • midgut? • hindgut? |
1. foregut: lower thorax + epigastric pain 2.midgut:umbilical region 3. hindgut: L+R lumbar regions , lateral and anterior thighs |
|
|
Pain from the gall bladder is sometimes referred to the shoulder. Attempt to explain this.
|
due to irritation of diaphragm |
|
|
What structure is found in the free edge of the falciform ligament? |
ligamentum teres |
|
|
Locate the porta hepatis and name the structures going through it. |
-liver hium -portal triad: proper hepatic artery, common bile duct and hepatic portal vein |
|
|
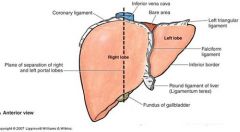
Name two other factors that will contribute to the support of the liver. |
falciform and coronary ligaments |
|
|
which lobe of the liver is larger |
right |
|
|
What is the function of the gall bladder? |
store and concentrate bile produced by the liver by absorbing salts and water |
|
|
what manufactures bile |
liver cells |
|
|
where is bile collected |
It is collected into microscopic canaliculi |
|
|
where do microscopic canaliculi drain |
left and right hepatic ducts |
|
|
what forms the common hepatic duct |
l + R hepatic ducts |
|
|
whats formed once the common hepatic duct joins the cystic duct |
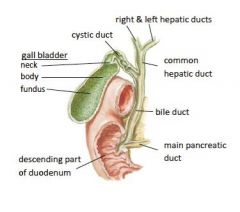
common bile duct |
|
|
At this stage, remind yourself of the structures that run in the freeedge of the lesser omentum. What is their relationship one to another? |
portal triad runs in the free edge of lesser omentum and joins the liver |
|
|
Where does the common bile duct run after it leaves the edge of the lesser omentum? |
passes posterior to 1st part of duodenum and head of pancreas to hepatopancreatic ampulla of vater |
|
|
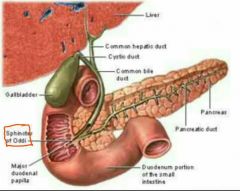
What is the hepatopancreatic ampulla (of Vater) and where is the sphincter of Oddi? |
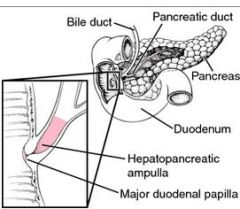
It is formed by the union of the pancreatic duct and the common bile duct. The ampulla is specifically located at the major duodenal papilla. The sphincter of Oddi is asphincter muscle, a circular band of muscle at the bottom of the biliary treewhich controls the flow of pancreatic juices and bile into the second part of the duodenum. |
|
|
If a gallstone became lodged at the sphincter of Oddi, which other organ would be affected?
|
the pancreas |
|
|
If a gallstone became lodged at the sphincter of Oddi, which other organ would be affected?
|
the pancreas
|
|
|
Why do patients with biliary obstruction appear yellow? Such patients also have pale faecesand dark urine. Why?
|
bile enters systemic circulation
pale faeces are due to lack to bile in GIT dark urine is due to bile in the kidneys filtered in renal system |
|
|
describe parts of duodenum |
•1st or superior part – L1–Onlypart that has peritonealised part•2nd or descending part –L2/3–Plicae circularesbegin–Receives common bile duct andmain pancreatic duct at hepatopancreatic ampulla (of Vater)•3rd or horizontal part – crosses L3 at midline–SMAcrosses anterior and IVC and aorta posteriorly•4th or ascending part –up to L2–Suspensory muscle (ligament of Treitz)attaches it to posterior body wall (from left crus to duodenum)•Supports duodenojejunaljunction at duodenojejunalflexure•
|
|
|
Which vessels provide the blood supply to the duodenum? From which vessels do theyoriginate? Why does the arterial supply to the duodenum have this dual origin? |
gastroduodenal artery from superior and inferior pancreaticoduodenal artery. -dual supply because arterial originates from 2 arteries which are SMA and caeliac trunk |
|
|
where does duodenum terminate |
at the duodeno-jejunal flexure. |
|
|
what mesentrey is attched to anterior surface of pancreas |
transverse mesocolon |
|
|
what is the uncinate process |
The uncinate process is the formed prolongation of the angle of junction of the lower and left lateral borders in thehead of the pancreas.
|
|
|
Which vein is formed behind the neck of the pancreas?
|
Portal Vein |
|
|
In what ligament does the tail of the pancreas pass to reach the spleen |
lienorenal ligament |
|
|
whats the exocrine component of the pancreas responsible for ?
|
secretion of digestive enzymes into pancreatic duct
-pancreatic ducts joins common bile duct at the hepatopancreatic ampulla (of Vater) -ampula opens into duodenum at the major duodenal papilla |
|
|
whats the endocrine component of the pancreas responisble for |
hormone secretion |
|
|
where does the accessory pancreatic duct drain and what does it drain |
The accessory pancreatic duct (drainingthe uncinate process) also opens in the duodenum, about 2cm proximal to the majorduodenal papilla |
|
|
The major duodenal papilla marks the boundary between which two subdivisions of the gut |
foregut and midgut |
|
|
What is the blood supply of the pancreas? |
-large splenic artery- branch of caeliac trunk -branches from gastroduodenal artery + SMA |
|
|
relations of pancreas. |
Head: extends to SMA and attaches to transverse and descending colon Neck: Ant. art adjacent to pylorus, where hepatic portal vein forms Body: ant. part lies on floor of omental bursa (lesser sac) Tail:ant to left kidney passes through splenorenal ligament |
|
|
What effects might you expect from a carcinoma of the head of the pancreas?
|
extrahepatic obstruction of biiliary ducts, jaundice and severe back pain. ductila carcinoma |
|
|
Why is this condition often inoperable? |
has extensive drainage to innaccesible lymph node it also metastasizes to the liver. pancreatic cancer is not easily detectable. |
|
|
Why pancreatic cancer condition often inoperable?
|
has extensive drainage to innaccesible lymph node it also metastasizes to the liver. pancreatic cancer is not easily detectable.
|
|
|
to which ribs is the spleen related |
9th to 11th ribs |
|
|
The hilum of the spleen lies at the level of
|
L1 vertebra transpyloric plane.
|
|
|
where does the outer concavity of the spleen lie |
on diaphragm |
|
|
where does hilum of spleen lie |
in the angle between the stomach andthe left kidney. |
|
|
The splenic artery reaches the hilum where it divides into four or fivebranches before entering the spleen. Branches from the splenic artery supply the stomach. Which ones? |
short gastric arteries (-left gastroduodenal artery (greater curvature) -anastmoses with righ of the hapatic artery supplying lesser curvature ) - |
|
|
relations of spleen |
Anterior: stomach posterior: part of diaphragm separating it from pleura + lung Inferior: left colic flexure medially: left kidney
|
|
|
Between which vertebral levels does the abdominal aorta extend? |
T12-L3/4 |
|
|
At what vertebral level does this occur?
|
L4 |
|
|
where does the external iliac artery pass to become the femoral artery of the lower limb |
The external iliac artery passes deep to the inguinal ligament to become thefemoral artery of the lower limb |
|
|
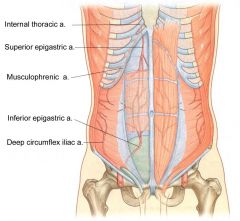
what is the inferior epigastric artery a branch of ? |
external iliac artery |
|
|
Identify inferior epigastric artery. What vessel does this artery anastomose with? |
superior epigastric artery |
|
|
Work outsuch a collateral route involving the inferior epigastric artery. |
The superior epigastric arteries, inferior epigastric arteries, internal thoracic arteries and left subclavian artery and right subclavian artery / brachiocephalic arecollateral vessels to the thoracic aorta and abdominal aorta. |
|
|
The internal iliac artery supplies most of the pelvic viscera, the pelvic and lower abdominalwalls and the perineum, as well as sending branches to the lower limb.Which other arteries supply structures in the pelvis? |
IMA and rectal arteries |
|
|
what does the internal iliac artery supply ? |
most of the pelvic viscera, the pelvic and lower abdominal walls and the perineum, as well as sending branches to the lower limb. |
|
|
The visceral branches of the internal iliac artery supply all of the pelvic organs except the_________ |
gonads ` |
|
|
branches of internal iliac (SUIM) |
Superior vesical artery (there may be several of these) Inferior vesical artery (males)/vaginal artery (females) Uterine artery (females) Middle rectal artery |
|
|
what is the first branch of the internal iliac a. |
superior vesical vessels (becomes obliterated as it heads towards anterior abdominal wall) |
|
|
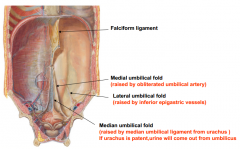
what is the embryological remnant of the obliteration of superior vesicle as it goes to AAB and whats the name given to the fold of peritoneum which it raises? |
This is the remnant of the foetal umbilical artery, and the fold of peritoneumwhich it raises on its way to the umbilicus is the medial umbilical ligament. |
|
|
What forms the median and lateral umbilical ligaments? |
median- obliteraded urachus Lateral: inferior epigastric arteries |
|
|
what does the inferior vesical artery supply in the male |
-fundus of bladder -prostate gand, seminal vesicles and ductus vas deferens and part of the ureter |
|
|
Which branches of internal iliac artery pass out of the pelvis? Which area does each of thesebranches supply? |
1. Lateral sacral artery- exists through greater sciatic notch and supplies piriformis muscle and gluteal m. 2.Obturator a. --> supplies obturator muscle and femoral head, adductor thigh muscles 3.internal Pudendal artery: gives off rectak artery which suplies rectum and anal canal a. perineal brancheal to prostate b. scrotal to skin of prostate c. deep and dorsal arteries to penis and clitoris 4.inferior gluteal --> supplies glut maximus and pelvic floor muscles |
|
|
Which branches of internal iliac artery pass out of the pelvis? Which area does each of thesebranches supply?
|
1. Lateral sacral artery- exists through greater sciatic notch and supplies piriformis muscle and gluteal m.
2.Obturator a. --> supplies obturator muscle and femoral head, adductor thigh muscles 3.internal Pudendal artery: gives off rectak artery which suplies rectum and anal canal a. perineal brancheal to prostate b. scrotal to skin of prostate c. deep and dorsal arteries to penis and clitoris 4.inferior gluteal --> supplies glut maximus and pelvic floor muscles |
|
|
where is the internal pudendal distributed |
perineum and external genitalia |
|
|
Why is the internal pudenal vessel called internal pudendal rather than just pudendal? |
its the termonal branch of anterior division of internal iliac artery |
|
|
Which branches of the internal pudendal artery supply the erectile tissue of the penis inmales and of the clitoris and vestibule in females? |
deep and dorsal arteries |
|
|
Most of the pelvic viscera are surrounded by networks of veins, into which they drain. Fromthese networks, venous blood passes via vessels which mirror the arteries to reach theinternal iliac veins.The gonads are an exception to this. Into which vessels do the gonadal veins drain? |
l gonad drains into renal vein R gonad drains into IVC |
|
|
Lymph from most of the pelvic viscera drains to internal iliac lymph nodes.Where do the internal iliac nodes then drain?
|
they drain to common iliac nodes → lateral aortic → then lumbar
|
|
|
Into which nodes do the gonads drain? |
lateral aortic |
|
|
The nerves present in the pelvis |
the obturator nerve, the sacral plexus and its branchesand sympathetic and parasympathetic autonomic nerves. |
|
|
behind which structure in the female does the obturator nerve run |
ovary |
|
|
through which opening does the obturator nerve leave |
obturator canal and enters the thigh |
|
|
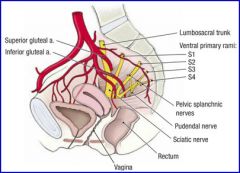
what forms the sacral plexus |
-the ventral rami of the first four sacral nerves -It alsoreceives a contribution from the ventral rami of the fourth and fifth lumbar nerves. |
|
|
what is the pudendal nerve a branch of |
sacral plecuses |
|
|
which nerves leave the pelvis via greater sciatic foramen |
sciatic nerve and the pudendal nerve |
|
|
what nerves are responsible for genital erection |
splanchnic nerves |
|
|
what forms the pelvis splanchnic nerves
|
2nd, 3rd and 4th sacral segmental nerves
|
|
|
Sympathetic fibres to pelvic viscera are supplied by the........ |
thoracic and lumbar splanchnicnerves, which branch off the sympathetic chain and travel down into the pelvis via a numberof midline plexuses, eventually joining the pelvic plexus |
|
|
What nerve controls the external urethral sphincter? |
-its is voluntary (skeletal muscle) -somatic nerves from S2-Se pass through pudendal nerve |
|
|
•Describe the role of the autonomic and somatic nervous system in micturition: Activity in which nerve fibres results in contraction of the detrusor muscle in the bladder walland emptying of the bladder? |
parasympathetic fibres are motor to detrusor muscle and inhibitory to internal unrethral sphincter |
|
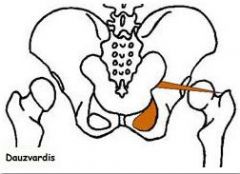
where does the piriformis m arise from and exit from |
the anterior aspect of the sacrum and passing out of thegreater sciatic foramen. |
|
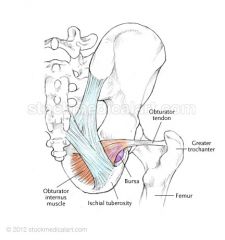
where does the obturator internus originate from ? |
originates from thedeep surface of obturator membrane and the bone surrounding the obturator foramen. Thetendon of obturator internus passes out of the pelvic cavity via the lesser sciatic foramen |
|
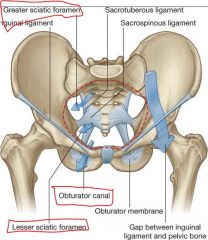
Where is the obturator canal? What travels through it? |
-opening in fascial obturator membrane - obturator vein, nerve and artery |
|
where do tendons of obturator internus insert ? WHATS ITS ACTION ? |
INSERTION: Middle part of medial aspect of greater trochanter of femur ACTION: laterally rotates and stabilizes hip |
|
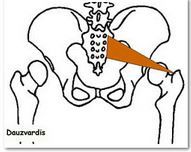
PIRIFORMIS INSERTION AND ACTION |
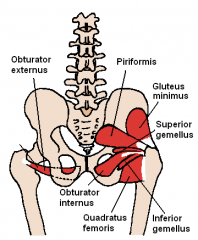
INSERTION: Anterior part of medial aspect of greater trochanter of femur ACTION: laterally rotates and stabilizes hip |
|
|
The pelvic floor or pelvic diaphragm is a sheet of muscle that separates what ? |
the pelvic cavityabove from the perineum below |
|
|
what muscle forms pelvic flor |
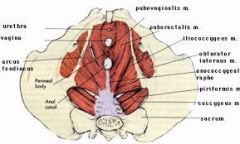
levator ani |
|
|
The two levator ani muscles are attached laterally to the pelvic wall; to which structures? It is formed by the levator ani muscle anteriorly and thecoccygeus muscle posteriorly on each side |
-pelvic aspect of obturator membrane + pelvic bones -rotates external thigh laterally : abducts fixed thigh at hip |
|
|
lev.ani and coccygeus converge in the midline. How are they arranged? |
-they blend together posterior to vagina and around anal aperture (both F&M) -they come together at anococcygeal ligament and attach to coccyx |
|
What is the perineal body? What is its function?
|
-cental tendon of perineum at mid junction of urogenital triangle and anal triangle
-maintain integrity of pelvic floor |
|
|
What are the attachments of coccygeus muscle? . |
ORIGIN: Attaches from the spine of the ischium and the sacrospinous ligament. INSERTION: Anococcygeal body and coccyx ACTIONS: supports pelvic viscera Note that coccygeus is adherent on its gluteal surface to the sacrospinous ligament |
|
|
puborectalis muscle |
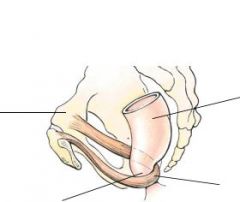
-subdivision of levator ani -forms sling around rectum pulling gut tube anteriorlyso that the anal canal descends at an angle of approximately 900 to therectum. |
|
|
Why is this arrangement of puborectalis muscle important?
|
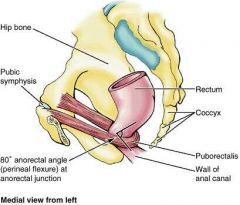
plays a role in maintaining faecal continence
|
|
|
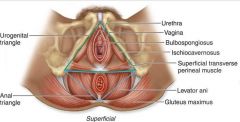
What is the PERINEUM
|
- The perineum is the area inferior to the pelvic floor, bounded by the pelvic outlet and limitedinferiorly by the skin.
|
|
in both sexes anal triangle contains.... |
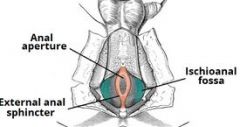
s the anal canal with the ischioanal fossa and itscontents on each side. |
|
|
Where does the rectum become the anal canal?
|
at anorectal junction
|
|
|
What is an episiotomy? When and why is it carried out? |
- a cut in peritoneum and inferoposterior vaginal wall it sis carried out during child birth when child develops foetal distress( increased heart rate before delivery or during) allows baby to come out more easily |
|
|
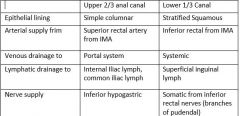
What consequences does this dual origin have for epithelial lining, blood supply, lymphaticdrainage and innervation of the anal canal? |
|
|
|
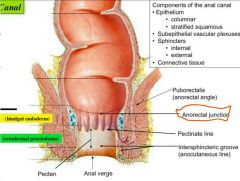
decribe the mucose of anal canal
|
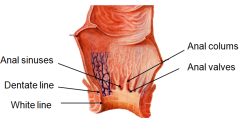
arranged in longitudinal folds/anal columns
- theinferior ends are linked by ridges called anal valves |
|
|
whats the name given to ring formed by anal valves and what does it mark
|
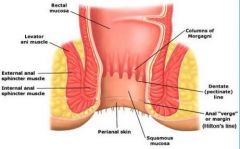
the pectinate line
marks the approximate boundary between the embryologically different regions of the anal canal |
|
|
where abouts is the internal sphincter |
The internal sphincter, around the upper two-thirdsof the canal, is the thickened lower end of the circular smooth muscle of the rectum |
|
|
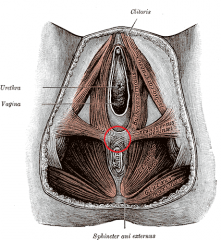
decribe the external sphincter |
Theexternal sphincter of striated muscle surrounds the lower two-thirds of the canal. -Itcomprises subcutaneous, superficial and deep parts. -The deep part is related posteriorlyto the fibres of puborectalis (part of levator ani muscle). |
|
|
What is the nerve supply to: the internal anal sphincter? |
hypogastric and superior rectal plexuses |
|
|
What is the nerve supply to: the external anal sphincter? |
pudendal nerve (2+3) + branches from S4 |
|
|
what are haemorrhoids |
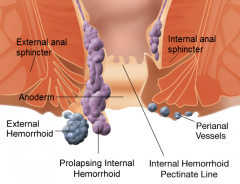
piles prolapse of rectal mucosa containing dilated veins of rectal venous plexuses |
|
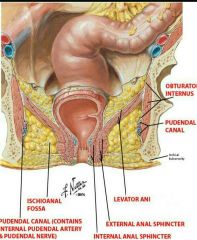
ischial anal fossae
|
-These are wedge shaped spaces in the lateral parts of the anal triangle.
-They Unite posteriorly, behind the anal canal, and anteriorly they extend into the urogenital triangle,above the urogenital diaphragm -The ischioanal fossae are largely filled with fat and are a common site for infection, resultingin abscesses which may rupture to produce a fistula. |
|
|
Which structures form the medial, lateral and inferior borders of the ischioanal fossae |
Lateral: ischium & inferior part of obturator in ternus M: external sphrincter & sloping superomedially |
|
|
What is a fistula?
|
abnormal passage
|
|
|
what travels in the ischioanal fossa |
The pudendal nerve and internal pudendal vessels travel in a fascial canal, the pudendalcanal, in the lateral wall of each ischioanal fossa as they pass anteriorly to supply thestructures of the perineum. |
|
|
By what route does the pudendal neurovascular bundle reach this pudendal canal? Whatbranches come off as the structures traverse the ischioanal fossa?
|
- leaves greater sciatic foramen to travel in gluteal region and re-enter sciatic foramina. |
|
|
How and why would you carry out a pudendal nerve block?
|
- anaesthetic injection into tissues surrounding pudendal nerve when nerve crosses internal aspect
For vaginal deliveries and vaginal operations. Stops sensory and motor innervation to the perineum Nerve targeted as it enters the lesser sciatic foramen |
|
|
THE UROGENITAL TRIANGLE |
- divided into deep and superficial by urogenital diaphragm - |
|
|
what is the urogenital diphragm |
a triangular layer of muscle and dense fascia (the fascial componentis termed the perineal membrane) that extends between the inferior ischiopubic rami and merges with the perineal body posteriorly. It is pierced by the urethra in both sexes and bythe vagina in the female. In both sexes, muscles within the urogenital diaphragm form theexternal urethral sphincter |
|
|
What branches come off the pudendal neurovascular bundle as it travels forwards in theurogenital triangle?
|
IPA: perineal arteries giving off posterior scrotal labia dorsal arteries arteries of the penis, clitoris IPN:deep --> superficial perineal nerve posterior scrotal |
|
|
What is the nerve supply to the external urethral sphincter (* in diagram below)?
|
pudendal nerve (S2+S3) + branch of S4 |
|
|
Which vessel does external pudendal artery branch off? What does it supply? |
anterior scrotal/labia larteries supplies labia and scrotum |
|
|
MALE UROGENITAL TRIANGLE |
in the male, there is a space superficial to the perineal membrane, between it and themembranous layer of superficial fascia (Colles’ fascia), called the superficial perinealpouch |
|
|
what does the superficial perineal pouch contain ? |
testes, vas and root of penis |
|
|
Explain why rupture of the urethra in the bulb of the penis leads to swelling of the scrotum,penis and lower abdominal wall. |
urine goes in the superficial perineal pouch and passes over scrotum beneath colles' fasci --> urine escapes into deep perineal pouch -> upwards around prostate/bladder or downward into superficial perineal pouch |
|
|
Which structures do the bulb of the penis and the crura of the corpora cavernosa attach to? |
deep penile fascia |
|
|
What are the actions of bulbospongiosus and ischiocavernosus muscles? What is theirnerve supply? |
-bulbospongiosus- compresses bulb of penis + corpus spongiosum nerve: branch of pudendal (s2-s4) |
|
|
Which arteries supply the penis? |
artery to bulb of penis, urethral artery, deep artery of penis, dorsal artery of penis ischiovernosus artery: forces blood from cavernous spaces in crura into distal parts of corpa cavernosa |
|
|
What is the mechanism of penile erection? |
1. Upon erotic stimulation, arteriovenous anastomoses, through which blood normally bypasses the erectile tissue of corpora cavernosa, are closed. 2. Smooth muscle in the fibrous trabeculae and coiled helicine arteries relaxes, due to parasympathetic stimulation. 3.This causes the helicine arteries to straighten, dilate their lumen and allow increased blood to flow in the sinuses of the corpora cavernosa. 4. The bulbuspongiosus and ischiocavernosus muscles compress the veins that drain corpora cavernosa, thus impeding the return of blood outside the penis. 5.As a result, all three erectile bodies are engorged with blood at venous pressure causing them to become enlarged and rigid, thus causing an erection. |
|
|
What is the sensory nerve supply to the skin of the scrotum? |
anterior scrotal nerves, posterior scrotal, pudendal and posterior cutaneous |
|
|
From what is the tunica vaginalis derived? How? |
processus vaginalis, formed as peritoneum closes off during development. |
|
|
testes and development |
During development, the testis pushes its way through the anterior abdominal wall, trailing itsductus deferens. As this happens, the testis and ductus deferens acquire a succession ofcoverings derived from the layers of the abdominal wall.
|
|
|
What is the cremasteric reflex?
|
ascent of testis when thigh is stroked |
|
|
In addition to the ductus deferens, what other structures run in the spermatic cord?
|
nerves, arteries, lymphatics + glands |
|
|
Suggest why urinary tract infections are more common in females than in males.
|
shorter urethra closer to anus |
|
|
Deep to the skin and fat of each labium major lies a mass of............ which is attached to ............... |
1. erectile tissue called the bulb ofthe vestibule 2. the underlying perineal membrane. |
|
|
what do the vaginal bulbs overlie |
e the greater vestibular glands and are themselves covered with thin sheetsof muscle, the bulbospongiosus muscles.
|
|
|
the vaginal vestibule bulbs join with ____________ to form glans of the clitoris |
externalopening of the urethra
|
|
|
Two other masses of erectile tissue also contribute to the formation of the clitoris. Whatname is given to these masses? Which part of the clitoris do they form? How is the clitorisanchored in the perineum? |
1. 2 crura and 2 corpora carvernosa 2. root and body 3. anchored posteriorly by the corpora cavernosa embedding it in the perinium |
|
|
What is the function of the vestibular glands (also known as Bartholin’s glands)? Infection ofthese glands is not uncommon – a Bartholin’s cyst is formed. |
secrete mucus into vestibule during sexual arousal |
|
|
To which nodes does lymph from perineal structures drain?
|
*superficial inguinal lymph nodes --> external iliac---> lumbar *deep + external iliac lymph nodes |
|
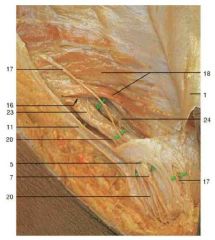
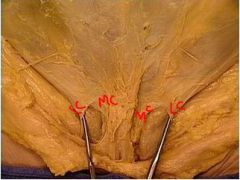
label the female inguinal region canal |
1 Aponeurosis of external abdominaloblique muscle 5 Superficial inguinal ring with fat pad 7 Round ligament (ligamentum teres uteri) 11 Inguinal ligament 15 External pudendal artery and vein 16 Position of deep inguinal ring 17 Ilio-inguinal nerve 18 Internal abdominal oblique muscle 20 Genital branch of genitofemoral nerve 23 Sheath of round ligament(inguinal canal) 24 Transversalis fascia |
|
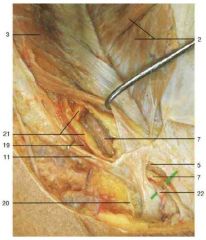
label male inguinal canal |
1 Aponeurosis of external abdominaloblique muscle 2 Internal abdominal oblique muscle(divided and reflected) 3 Transversus abdominis muscle 5 Superficial inguinal ring with fat pad 7 Round ligament (ligamentum teres uteribranch of ilio-inguinal nerve 11 Inguinal ligament 19 Pubic branch of inferior epigastricartery20 Genital branch of genitofemoral nerve 21 Fat pad of inguinal canal 22 Ilio-inguinal nerve |
|
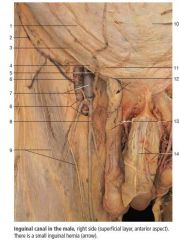
1. 2. 3. 4. 5. 12. 13. 14 15 16-19 |
1 Aponeurosis of external abdominal oblique muscle
2 Superficial circumflex iliac vein 3 Inguinal ligament 4 Lateral crus of inguinal ring 5 Superficial epigastric vein 12 Superficial inguinal ring 13 Spermatic cord and genital branchof genitofemoral nerve 14 Penis with dorsal nerves and deep dorsal veinof penis 15 Aponeurosis of external abdominal obliquemuscle (divided and reflected) 16 Internal abdominal oblique muscle 17 Ilio-inguinal nerve 18 Anterior cutaneous branches of iliohypogastricnerve 19 Superficial external pudendal veins |
|
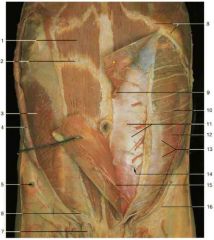
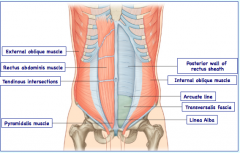
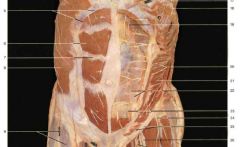
label the abdomina wall muscles |
1 Rectus abdominis muscle2 Tendinous intersection3 Internal abdominal oblique muscle4 External abdominal oblique muscle(reflected)5 Anterior superior iliac spine6 Ilio-inguinal nerve7 Spermatic cord8 Costal margin9 Superior epigastric artery10 Thoraco-abdominal (intercostal)nerves11 Posterior layer of rectus sheath12 Transversus abdominis muscle13 Semilunar line14 Arcuate line15 Inferior epigastric artery16 Inguinal ligament |
|
|
6 Rectus abdominis muscle 7 Tendinous intersection 8 External abdominal oblique muscle 9 Lateral femoral cutaneous nerve 10 Femoral vein 11 Great saphenous vein 12 Medial supraclavicular nerves 13 Pectoralis minor muscle (reflected)and medial pectoral nerves 14 Axillary vein 15 Long thoracic nerve and lateralthoracic artery 16 Internal thoracic artery 17 Intercostal nerves 18 Lateral cutaneous branches ofintercostal nerves 19 Superior epigastric artery 20 Thoraco-abdominal (intercostal)nerves 21 Transversus abdominis muscle 22 Posterior layer of rectus sheath 23 Inferior epigastric artery 24 Lateral femoral cutaneous nerve 25 Inguinal ligament and ilio-inguinalnerve26 Femoral nerve 27 Femoral artery 28 Spermatic cord |
|
|
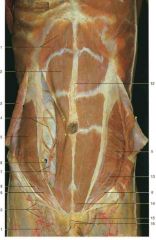
1 Costal margin 2 Rectus abdominis muscle 3 External abdominal oblique muscle(reflected) 4 Thoraco-abdominal (intercostal) nerveswith accompanying vessels 5 Internal abdominal oblique muscle 6 Arcuate line (arrow) 7 Inferior epigastric artery and vein 8 Ilio-inguinal nerve 9 Position of deep inguinal ring 10 Superficial inguinal lymph nodes 11 Great saphenous vein 12 Linea alba 13 Iliohypogastric nerve 14 Pyramidal muscle 15 Spermatic cord 16 Fundiform ligament of penis |
|

label kidney |
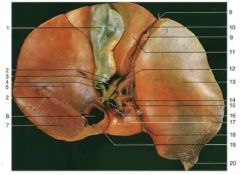
1 Esophagus2 Cardial notch3 Cardial part of stomach4 Lesser curvature of stomach5 Pyloric sphincter6 Angular notch (incisura angularis)7 Pyloric canal8 Pyloric antrum9 Fundus of stomach10 Greater curvature of stomach11 Body of stomach
|
|
|
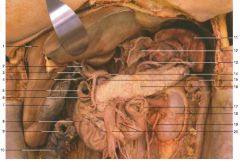
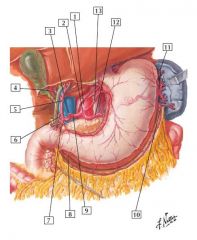
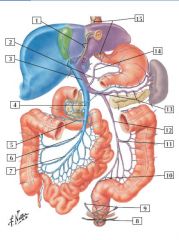
1 Liver 2 Hepatic artery proper 3 Hepatic duct 4 Cystic duct 5 Pylorus6 Gastroduodenal artery 7 Gallbladder 8 Duodenum 9 Transverse colon (cut) 10 Ascending colon 11 Spleen 12 Cardia 13 Splenic artery 14 Common hepatic artery 15 Portal vein16 Pancreas (body) 17 Duodenojejunal flexure18 Kidney (with capsula adiposa)19 Ureter20 Superior mesenteric artery and vein21 Aorta (abdominal part)22 Common bile duct23 Lesser duodenal papilla24 Greater duodenal papilla25 Pancreatic duct |
|
|
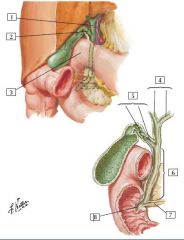
1 Fundus of gallbladder
2 Peritoneum (cut edges) 3 Cystic artery 4 Cystic duct 5 Right lobe of liver 6 Inferior vena cava 7 Bare area of liver 8 Notch for ligamentum teres andfalciform ligament 9 Ligamentum teres 10 Falciform ligament of liver 11 Quadrate lobe of liver 12 Common hepatic duct 13 Left lobe of liver 14 Hepatic artery proper 15 Common bile duct Portal triad 16 Portal vein 17 Caudate lobe of liver 18 Ligamentum venosum 19 Ligament of inferior vena cava 20 Appendix fibrosa (left triangularligament) 21 Coronary ligament of liver22 Hepatic veins |
|
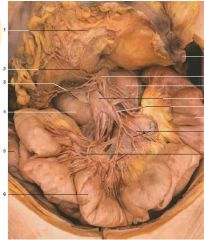
si arteries |
1 Greater omentum2 Middle colic artery3 Right colic artery4 Duodenum5 Ascending colon6 Ileum7 Transverse colon8 Celiac ganglion9 Duodenojejunal flexure10 Superior mesenteric vein11 Superior mesentericartery12 Jejunum13 Jejunal arteries14 Ileal arteries |
|

|
1 Lung
2 Liver (visceral surface) 3 Lymph node 4 Inferior vena cava 5 Ligamentum teres (reflected) 6 Right branch of hepatic artery proper 7 Diaphragm 8 Common hepatic duct (dilated) 9 Cystic duct and artery 10 Gallbladder 11 Probe in epiploic foramen 12 Right lobe of liver 13 Portal vein 14 Right gastric artery 15 Duodenum 16 Pylorus 17 Right colic flexure 18 Right gastro-omental (gastro-epiploic) artery 19 Transverse colon 20 Abdominal part of esophagus (cardiac part of stomach) 21 Fundus of stomach 22 Esophageal branches of left gastric artery 23 Lumbar part of diaphragm 24 Left gastric artery 25 Celiac trunk 26 Splenic artery 27 Pancreas 28 Common hepatic artery 29 Left gastro-omental (gastro-epiploic) artery 30 Gastroduodenal artery 31 Pyloric part of stomach 32 Greater curvature of stomach 33 Gastrocolic ligament 34 Superior pancreaticoduodenal artery 35 Short gastric arteries 36 Aorta 37 Spleen 38 Caudate lobe of liver 39 Left branch of hepatic artery proper 40 Descending part of duodenum (cut) 41 Left inferior phrenic artery 42 Suprarenal gland 43 Kidney 44 Transverse mesocolon |
|

|
1 Lung 2 Liver (visceral surface) 3 Lymph node 4 Inferior vena cava 5 Ligamentum teres (reflected) 6 Right branch of hepatic artery proper 7 Diaphragm 8 Common hepatic duct (dilated) 9 Cystic duct and artery 10 Gallbladder 11 Probe in epiploic foramen 12 Right lobe of liver 13 Portal vein 14 Right gastric artery 15 Duodenum 16 Pylorus 17 Right colic flexure 18 Right gastro-omental (gastro-epiploic) artery 19 Transverse colon 20 Abdominal part of esophagus (cardiac part of stomach) 21 Fundus of stomach 22 Esophageal branches of left gastric artery 23 Lumbar part of diaphragm 24 Left gastric artery 25 Celiac trunk 26 Splenic artery 27 Pancreas 28 Common hepatic artery 29 Left gastro-omental (gastro-epiploic) artery 30 Gastroduodenal artery 31 Pyloric part of stomach 32 Greater curvature of stomach 33 Gastrocolic ligament 34 Superior pancreaticoduodenal artery 35 Short gastric arteries 36 Aorta 37 Spleen 38 Caudate lobe of liver 39 Left branch of hepatic artery proper 40 Descending part of duodenum (cut) 41 Left inferior phrenic artery 42 Suprarenal gland 43 Kidney 44 Transverse mesocolon |
|

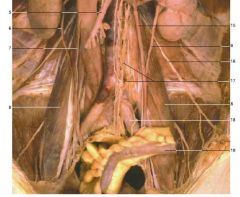
female retroperitooneal organs
|
1 Kidney2 Ureter3 Inferior vena cava
4 Abdominal aorta 5 Ovary 6 Uterine tube 7 Uterus 8 Round ligament and inguinal canal 9 Urinary bladder 10 Vagina |
|
label structures |
1 Diaphragm
2 Inferior vena cava 3 Suprarenal gland 4 Kidney 5 Superior mesenteric artery 6 Ureter 7 Right spermatic Psoas majormuscle 9 Spleen 10 Cardiac part ofstomach 11 Abdominal aorta 12 Splenic artery 13 Celiac trunk andceliac ganglion 14 Renal artery and vein 15 Left spermatic vein 16 Ilio-inguinal nerve 17 Superior hypogastricplexus and ganglion 18 Left common iliacartery19 Sigmoid colon |
|
|
on which side is the SMA and what what level |
right side |
|
|
describe the branches of the SMA and what they supply |
From top to bottom gives off: 1. 1. Inferior pancreaticoduodenal a. o Anastomoses w/ a branch of gastroduodenal a. offthe common hepatic a. 2. 2. Middle colic artery o Anastomoses w/ l. colic a. 3. 3.R colic a 4. 4. Iliocolic a. o Splits into superior and inferior o Superior anastomoses w/ right colic àsupplies a. colon o Inferior branch splits into 4 branches 1. Ilial àileum 2. Caecal àcaecum 3. Appendicular àappendix 4. Colic (ascending) àa. colon 5. 5. Jejunal and ilial vessels on the R side o They form arcades and vasa recta |
|
|
where is the IMA given off ? |
L3 from abdominal aorta |
|
|
describe branches of IMA and what they supply (IMA is LESS) |
3 main branches 1. L. colic artery àvascularises distal 1/3 of transverse colon and descending branch · Anastomoses with middle colic artery 2. Sigmoidal arteries · Form arcades supply sigmoid colon 3. Superior rectal artery · Supplies proximal colon · Crosses over common iliac artey to enter pelviccavity · Divides at S3 |
|
|
Caeliac trunk branches and what they supply |
- 3 main branches ( left Hand Side) -Left gastric artery -common hepatic -splenic artery Left gastroepiploic : supplies lesser curvature of stomach ( can come off proper or common hepatic artery) Common hepatic ( GoD PRops) god makes pain alright -gastroduodenal artery - superior pancreaticoduodenal -right gastroepiploic artey Props- common to be properly rightcys - common hepatic, proper hepatic, L&R hepatic and cyctic artery (from right hepatic) Side: SPLEEN PLS splenic artery - pancreatic branches -left gastro epiploic short gastric arteries |
|
|
descrite the internal iliac artery and its anterior and posterior branches |
S: superior vesical artery (branch of umbilical 2nd branch off anterior internal iliac) O: obturator artery (first branch, exists via obturator canal and runs along obturator m.) IV: inferior vesical artery (vaginal in females) ( arises individually from ant trunk sometimes)- supplies bladder, ureter, and seminal vesicles and vas deferns like superior vesicle. U: uterine artery MR: middle rectal artery P: pudendal (internal) artery- exists g sciatic foramen between ichiococcygeus and piriformis and descends to enter periinal region via lesser sciatic foramen IG: inferior gluteal artery |
|
|
whiich fold overlies the inferior epigastric artery ? |
lateral umbilical fold |
|
|
branches of external iliac artery |
inferior epigastric deep circumflex artery |
|
|
what are the anterior and posterion relations of external iliac artery ? |
-anteriorly (at origin) - gonadal vessels, genital branch of the genitofemoral nerve, deep circumflex iliac vein, round ligament -posteriorly - iliac fascia, psoas muscle |
|
|
1. Abdominal aorta 2. Celiac trunk 3. Left hepatic artery 4. Cystic artery 5. Proper hepatic artery 6. Right gastric artery 7. Gastroduodenal artery 8. Right gastro-omental (gastroepiploic) artery 9. Common hepatic artery 10. Left gastro-omental (gastroepiploic) artery 11. Short gastric arteries 12. Splenic artery 13. Left gastric artery |
|
|
pain from epigstric region refer to what dermatomes ? |
T5-9 or T10 spinal levels. |
|
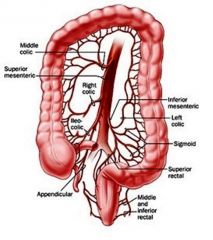
laerge intestine arteries |
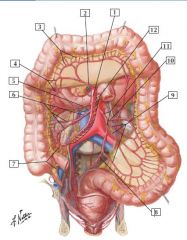
1. Superior mesenteric artery2. Middle colic artery3. Straight arteries (arteriae rectae)4. Marginal artery5. Right colic artery6. Ileocolic artery (Colic branch; Ileal branch)7. Appendicular artery8. Superior rectal artery9. Sigmoid arteries10. Left colic artery11. Inferior mesenteric artery12. Jejunal and ileal (intestinal) arteries |
|
|
why are anastomoses of inferior and superior MAs important ?
|
If the blood flow from one bowel region is compromised, collateral flow from anastomotic branches usually can assist in supplying blood tothe compromised region.
|
|
|
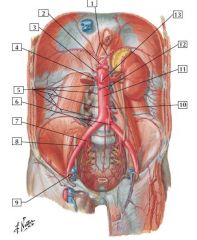
1. Inferior phrenic arteries
2. Celiac trunk with common hepatic, left gastric, and splenicarteries 3. Middle suprarenal artery 4. Right renal artery 5. 1st to 4th right lumbar arteries6. Common iliac arteries 7. Internal iliac artery 8. External iliac artery 9. Inferior epigastric artery 10. Inferior mesenteric artery 11. Abdominal aorta 12. Testicular (ovarian) arteries |
|
|
at what level does Ab aorta enter abdominal cavity
|
T12 and it bifurcates at L4
|
|
|
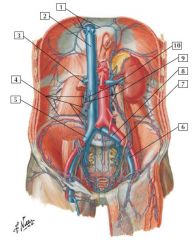
1. Inferior phrenic veins2. Inferior vena cava3. Right renal vein4. 1st to 4th right lumbar veins5. Common iliac vein6. External iliac vein7. Internal iliac vein8. Common iliac vein9. Ascending lumbar veins10. Ovarian (testicular) veins |
|
portal veins and anastomoses
|
1. Paraumbilical Veins
2. Right gastric vein 3. Hepatic portal vein 4. Superior mesenteric vein 5. Middle colic vein6. Right colic vein 7. Ileocolic vein 8. Inferior rectal veins 9. Middle rectal veins 10. Left and right superior rectal veins 11. Left colic vein 12. Inferior mesenteric vein 13. Splenic vein 14. Left gastric vein 15. Esophageal veins |
|
|
1. Common hepatic duct2. Cystic duct3. Superior (1st) part of duodenum
4. Hepatic ducts (Right; Left) 5. Cystic duct (Spiral fold; Smooth part) 6. Common bile duct. 7. Pancreatic duct 8. Hepatopancreatic ampulla (of Vater) |
|
|
route of bile to gallblader |
Bile leaves the liver by the right and left hepatic ducts,draining into a common hepatic duct. The latter drains via the cysticduct into the gallbladder, which concentrates and stores bile.
|
|
|
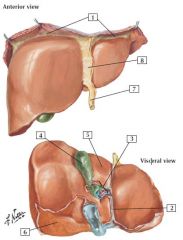
1. Coronary ligament
2. Fissure for ligamentum venosum 3. Porta hepatis 4. Gallbladder 5. Quadrate lobe 6. Bare area 7. Round ligament (ligamentum teres) of liver (obliterated umbilicalvein) forming free border of falciform ligament 8. Falciform ligament |
|
|
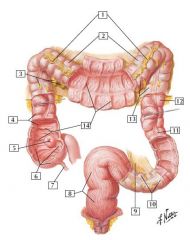
1. Greater omentum (cut away)2. Transverse colon3. Omental (epiploic) appendices (fat)4. Ascending colon5. Ileal orifi ce6. Cecum7. Appendix8. Rectum9. Sigmoid mesocolon10. Sigmoid colon11. Taenia coli12. Descending colon13. Haustra14. Semilunar folds
|
|
|
1. Liver2. Lesser omentum3. Omental bursa (lesser sac)4. Transverse mesocolon5. Transverse colon6. Small intestine7. Urinary bladder8. Rectum9. Inferior (horizontal, or 3rd) part of duodenum10. Pancreas
|
|
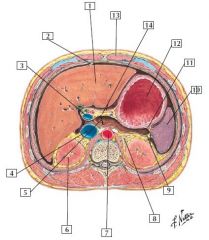
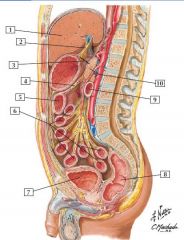
abdomen at T12 |
1. Liver2. Falciform ligament3. Portal vein4. Inferior vena cava5. Omental bursa (lesser sac)6. Right kidney7. Abdominal aorta8. Left suprarenal (adrenal) gland9. Splenorenal ligament with splenic vessels10. Spleen11. Gastrosplenic ligament with short gastric vessels12. Stomach13. Rectus abdominis muscle (in rectus sheath)14. Lesser omentum |
|
|
what is common about right and left kidneys, suprarenal(adrenal) glands, aorta, and inferior vena cava. |
they are retroperitoneal organs |
|
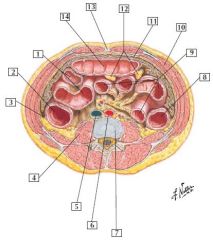
abdomen at L2 |
1. Ileum2. Ascending colon3. Right paracolic gutter4. Psoas major muscle5. Inferior vena cava6. Abdominal aorta7. Intervertebral disc (between L2 and L3 vertebral bodies)8. Descending colon9. Loops of jejunum10. Internal oblique muscle11. Greater omentum12. Omental appendices (fat)13. Linea alba14. Transverse colon
|
|
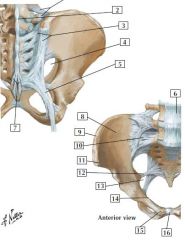
bones and ligaments of pelvis |
1. Iliolumbar ligament2. Supraspinous ligament3. Posterior sacroiliac ligaments4. Greater sciatic foramen5. Sacrotuberous ligament6. Anterior longitudinal ligament7. Posterior sacrococcygeal ligaments8. Iliac fossa9. Iliac crest10. Anterior sacroiliac ligament11. Anterior superior iliac spine12. Sacrospinous ligament13. Lesser sciatic foramen14. Pectin pubis15. Pubic tubercle16. Pubic symphysis |
|
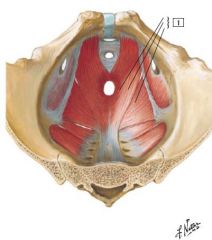
what is this muscle what forms it
|
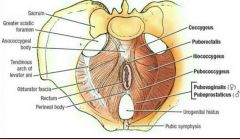
-Levator ani (Puborectalis; Pubococcygeus; Iliococcygeus)
-innervation: s3-s4 -supports pelvic floor It helps maintainthe integrity of the uterus and vagina, as well as support therectum and assist in defecation by straightening the anorectaljunction in both sexes. |
|
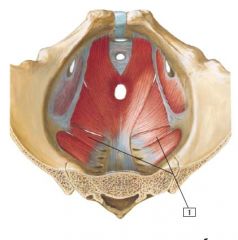
|
1. (Ischio-)coccygeus
Innervation: Ventral rami of S4 and S5. |
|
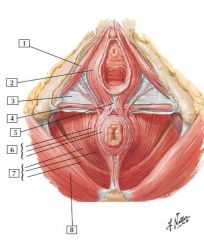
|
1. Ischiocavernosus muscle
2. Bulbospongiosus muscle 3. Perineal membrane 4. Superfi cial transverse perineal muscle 5. Perineal body 6. Parts of external anal sphincter muscle 7. Levator ani muscle (Pubococcygeus; Puborectalis; Iliococcygeus) 8. Gluteus maximus muscle |
|
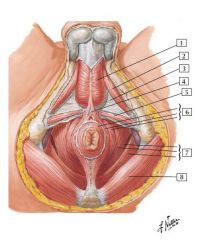
Male perineum
|
1. Bulbospongiosus muscle
2. Ischiocavernosus muscle 3. Perineal membrane 4. Perineal body 5. Superfi cial transverse perineal 6. Parts of external anal sphincter muscle 7. Levator ani muscle (Pubococcygeus; Puborectalis; Iliococcygeus) 8. Gluteus maximus muscle |
|
|
The muscles of the male perineum are skeletal in natureand are innervated by what nerve aand its branches |
the pudendal nerve and its branches. |
|
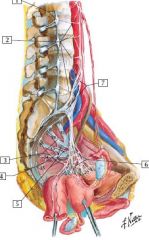
female nerves |
1. Sympathetic trunk and L2 ganglion2. Lumbar splanchnic nerves3. Sacral splanchnic nerves (sympathetic)4. Pudendal nerve5. Pelvic splanchnic nerves (parasympathetic)6. Inferior hypogastric (pelvic) plexus7. Superior hypogastric plexus |
|
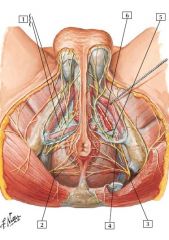
male nerves |
1. Perineal nerves (Superfi cial; Deep)2. Inferior anal (rectal) nerves3. Pudendal nerve4. Perineal nerve5. Superfi cial and deep branches of perineal nerve6. Dorsal nerve of penis (continuation of pudendal nerve supplyingmuscles on superior aspect of perineal membrane)
|
|
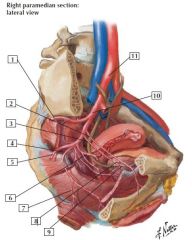
female pelvic arteries
|
1. Superior gluteal artery
2. Obturator artery 3. Umbilical artery (patent part) 4. Internal pudendal artery 5. Inferior gluteal artery 6. Uterine artery 7. Inferior rectal artery 8. Superior vesical arteries 9. Umbilical artery (occluded part) 10. Internal iliac artery 11. Right common iliac artery |
|
|
pelvic drainage |
Veins draining the corresponding structures are similarly identifi edand named. These veins drain into the internal iliac vein and into thecommon iliac vein on each side. |
|
|
branches of IPA in perineum |
In the perineum, the internal pudendal artery gives off the inferiorrectal artery and the perineal artery. Branches of the perineal arterysupply the bulb of the vestibule and clitoris.
|
|
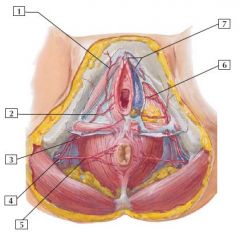
female arteries
|
1. Posterior labial artery
2. Perineal artery 3. Perineal artery 4. Internal pudendal artery in pudendal (Alcock’s) canal 5. Inferior rectal artery 6. Artery to bulb of vestibule 7. Dorsal artery of clitoris All branches of internal pudendal artery |
|
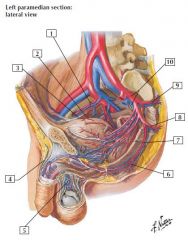
Arteries and Veins of Male Pelvis
|
1. Right obturator vessels
2. Superior vesical artery 3. Umbilical artery (occluded part) 4. Superfi cial dorsal vein of penis 5. Pampiniform (venous) plexus 6. Inferior rectal artery 7. Internal pudendal artery 8. Inferior gluteal artery 9. Superior gluteal artery 10. Internal iliac vessels |
|
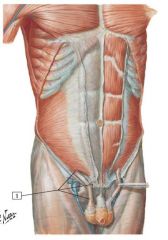
where does the cremastor muscle arise from? |
middle of inguinal ligament |
|
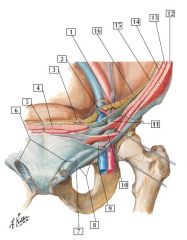
|
1. Testicular vessels and genital branch of the genitofemoral nerve
2. Inferior epigastric vessels 3. Medial umbilical ligament (occluded part of umbilical artery) 4. Rectus abdominis muscle 5. Median umbilical ligament (urachus) 6. Superfi cial inguinal rings 7. Intercrural fibers 8. Inguinal ligament (Poupart’s) 9. Cremasteric muscle 10. Spermatic cord 11. Internal spermatic fascia (from transversalis fascia at deepinguinal ring) 12. External abdominal oblique muscle 13. Internal abdominal oblique muscle 14. Transversus abdominis muscle 15. Transversalis fascia 16. Peritoneum |
|
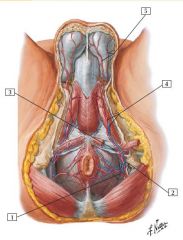
male perineum
|
1. Inferior rectal artery
2. Internal pudendal vessels and pudendal nerve (cut) in pudendal(Alcock’s) canal (opened up) 3. Internal pudendal artery passes superior to perineal membrane 4. Perineal artery and vein 5. Posterior scrotal arteries |
|
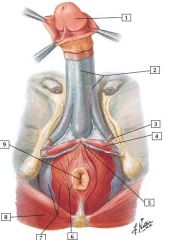
|
1. Glans penis
2. Deep (Buck’s) fascia of penis 3. Ischiocavernosus muscle (cut away) 4. Superfi cial transverse perineal muscle 5. Perineal body 6. External anal sphincter muscle7. Levator ani muscle and inferior fascia of pelvic diaphragmroofi ng ischioanal fossa 8. Gluteus maximus muscle 9. Anus |
|
|
|
1. Glans penis
2. Deep (Buck’s) fascia of penis 3. Ischiocavernosus muscle (cut away) 4. Superfi cial transverse perineal muscle 5. Perineal body 6. External anal sphincter muscle7. Levator ani muscle and inferior fascia of pelvic diaphragmroofi ng ischioanal fossa 8. Gluteus maximus muscle 9. Anus |
|
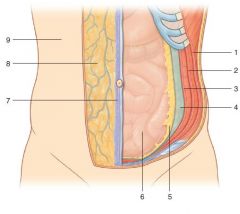
|
1. External oblique muscle2. Internal oblique muscle
3. Transversus abdominis muscle 4. Transversalis fascia 5. Extraperitoneal fascia 6. Parietal peritoneum 7. Superficial fascia—membranous layer (Scarpa’s fascia) 8. Superficial fascia—fatty layer (Camper’s fascia) 9. Skin |
|
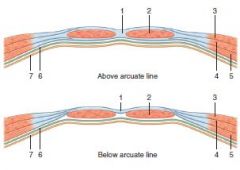
|
1. Linea alba
2. Rectus abdominis muscle 3. External oblique muscle 4. Internal oblique muscle 5. Transversus abdominis muscle 6. Transversalis fascia 7. Parietal peritoneum |
|
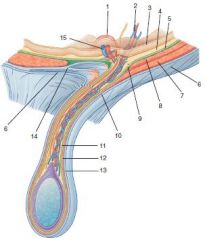
|
1. Ductus deferens
2. Testicular artery and pampiniform plexus of veins 3. Parietal peritoneum 4. Extraperitoneal fascia 5. Transversalis fascia6. External oblique aponeurosis 7. Internal oblique muscle 8. Transversus abdominis muscle 9. Deep inguinal ring 10. Superficial inguinal ring 11. Internal spermatic fascia 12. Cremasteric fascia 13. External spermatic fascia 14. Conjoint tendon 15. Inferior epigastric vessels |
|
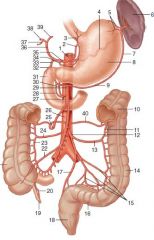
|
1. Celiac trunk2. Left gastric artery3. Esophageal artery4. Splenic artery5. Short gastric arteries6. Spleen7. Left gastro-omental artery8. Stomach9. Right gastro-omental artery10. Transverse colon11. Marginal artery12. Inferior mesenteric artery13. Left colic artery14. Descending colon15. Sigmoid arteries16. Sigmoid colon17. Superior rectal artery18. Rectum19. Appendix20. Appendicular artery21. Ascending colon22. Ileocolic artery23. Marginal artery24. Right colic artery25. Middle colic artery26. Abdominal aorta27. Inferior pancreaticoduodenalartery28. Anterior pancreaticoduodenalartery29. Superior mesenteric artery30. Posterior pancreaticoduodenalartery31. Duodenum32. Supraduodenal artery33. Gastroduodenal artery34. Right gastric artery35. Common hepatic artery36. Hepatic artery proper37. Cystic artery38. Right hepatic artery39. Left hepatic artery40. Marginal artery |
|
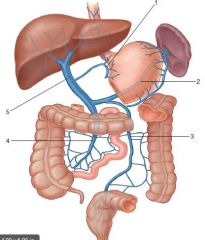
|
1. Left gastric vein2. Splenic vein3. Inferior mesenteric vein4. Superior mesenteric vein5. Portal vein
|
|
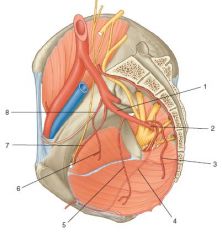
|
1. Anterior trunk of internal iliac2. Inferior gluteal3. Middle rectal4. Internal pudendal5. Inferior vesicle6. Superior vesicle7. Obturator8. Umbilical
|
|
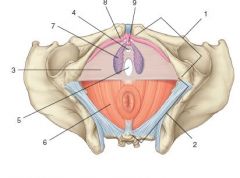
|
1. Urogenital triangle2. Anal triangle3. Perineal membrane4. Opening for urethra in perineal membrane5. Opening for vagina in perineal membrane6. Levator ani muscle7. Bulb of vestibule8. Corpus cavernosum of clitoris9. Glans clitoris
|
|
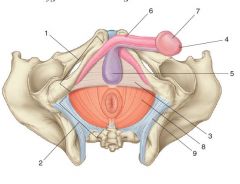
|
1. Urogenital triangle2. Anal triangle3. Perineal membrane4. External urethral orifice5. Bulb of penis6. Corpus cavernosum of penis7. Glans penis8. Levator ani muscle9. Sacrotuberous ligament
|
|
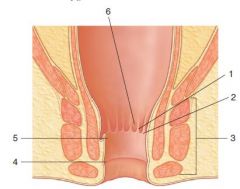
|
1. Anal column2. Anal valve3. External anal sphincter4. White line5. Pectinate line6. Anal sinus
|
|
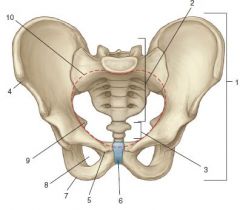
|
1. Pelvic bone2. Sacrum3. Coccyx4. Anterior superior iliac spine5. Pubic tubercle6. Pubic symphysis7. Ischial tuberosity8. Obturator foramen9. Ischial spine10. Pelvic inlet
|
|
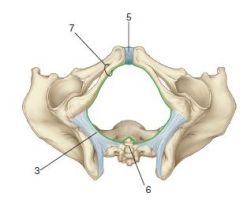
|
3. Sacrotuberous ligament4. Lesser sciatic foramen5. Pubic symphysis6. Coccyx7. Inferior pubic ramus
|
|
|
Ilioinguinal Nerves pass through the inguinal canal and Innervate what?
|
Labia and scrotum (anterior labial in females)
|
|
|
Inferior border of rectus sheath posteriorly
|
Arcuate line
|
|
|
Conjoint tendon
|

Attachment of internal oblique and transversus abdominis
|
|
|
Iliohypogastruic nerves provides sensory innervation to what?
|
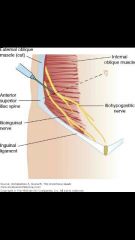
Skin in Lower abdomen upper hip and thigh
|
|
|
Genitofemoral nerve provides innervation to what?
|
Anterior scrotum, labia majora and upper medial thigh
|
|
|
Brances of the sacral plexuses |
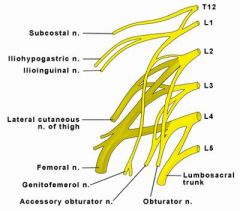
Interested in getting lunch on friday iliohypogastric and ilioinguinal from 1 genital femoral from 1/2 lateral femoral from 2/3 Obturator & femoral 2-4 |
|
|
internal pudendal arteries branches (I Pee Pee But Don’t Dump!) |
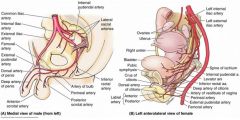
Inferior rectal Perineal Posterior scrotal (or labial) Bulb Deep artery Dorsal artery |