![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
301 Cards in this Set
- Front
- Back
|
Maximal Intercuspal Position |
The complete intercuspation of the opposing teeth independent of condylar position |
|
|
Centric Occlusion |
The occlusion of opposing teeth when the mandible is in central relation. This may or may not coincide with the maximal intercuspal position. |
|
|
Centric Relation |
The maxillomandibular relationship in which the condyles articulate with the thinnest avascular portion of their respective disks with the complex in the anterior-superior position against the shapes of the articular eminencies. > This position is clinically discernible when the mandible is directed superior and anteriorly. It is restricted to a purely rotary movementabout the transverse horizontal axis. |
|
|
Centric Position |
The position of the mandible when the jaws are in centric relation |
|
|
Retruded Contact Position |
Guided occlusal relationship occurring at the most retruded position of the condyles in the joint cavities. A position that may be more retruded then the centric relation position. |
|
|
Postural Position |
Any mandibular relationship occurring during minimal muscle contraction. |
|
|
Occlusal Vertical Dimension |
The distance measured between two points when the occluding members are in contact |
|
|
Rest Vertical Dimension |
The distance between two selected points (one of which is on the middle of the face or nose and the other of which is on the lower face or chin) measured when the mandible is in the physiologic rest position |
|
|
Physiologic Rest Positon |
The mandibular position assumed when the head is in an upright position and the involved muscles, particularly the elevator and depressor groups, are inequilibrium in tonic contraction, and the condyles are in a neutral, unstrained position |
|
|
Interocclusal Distance |
The distance between occluding surfaces of the maxillary and mandibular teeth when the mandible is in a specified position |
|
|
Interocclusal Rest Space |
The difference between the vertical dimension of rest and the vertical dimension while in occlusion |
|
|
Hinge Movement (rotation) |
The movement in space characterized by two divergent points moving around a central axis of rotation |
|
|
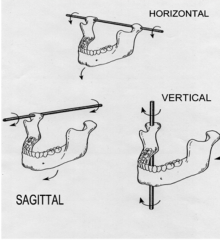
Transverse Horizontal Axis (hinge axis) |
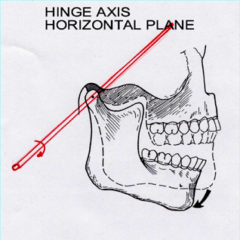
An imaginary line around which the mandiblemay rotate within the sagittal plane. |
|
|
Translatory Movements |
The movement in space characterized by linear motion with no axis of rotation |
|
|
Border Movements |
The most extreme positions to which the mandible is able to move – generally considered to be relatively stable and reproducible (not pathological). These movements have been described from the frontal, sagittal and horizontal planes. |
|
|
Posselt Diagram of Border Movements |
Describe border movements in three planes – sagittal, horizontal and frontal . When combined describe a 3D envelope of motion that represents the maximum range of movement of the mandible. Although this envelope of motion is characteristic in shape, it varies from individual to individual. It must be remembered this is a tracing of the movements of the mandibular incisal point movements. |
|
|
Working Side |
The side toward which the mandible moves during lateral excursion. |
|
|
Non-Working Side |
The side of the mandible that moves toward the median line in a lateral excursion. The condyle on that side is referred to as the non-working side condyle. |
|
|
Balanced Articulation/Occlusion |
The bilateral, simultaneous, anterior, and posterior occlusal contact of teeth incentric and eccentric positions. APPLIES ONLY WHEN REFERRING TO COMPLETE UPPER AND LOWER DENTURES. |
|
|
Mutually Protected Articulation/Occlusion |
An occlusal scheme in which the posterior teeth prevent excessive contact of the anterior teeth in maximum intercuspation, and the anterior teeth disengage the posterior teeth in all mandibular excursive movements |
|
|
Anterior Guidance |
The influence of the contacting surfaces of anterior teeth on tooth limiting mandibular movements. Edge of mandibular teeth sliding along the lingual aspect of maxillary teeth when in maximal intercuspal position. AVG is 1-3 mm in both vertical and horizontal direction. |
|
|
Group Function |
Multiple contact relations between the maxillary and mandibular teeth in lateral movements on the working side where by simultaneous contact of several teeth acts as a group to distribute occlusal forces |
|
|
Protrusion |
A position of the mandible anterior to centric relation |
|
|
Protrusive Movement |
Mandibular movement anterior to centric relation |
|
|
Lateral Excursion |
Sideward movement of the mandible characterized by: (1) Rotation of the working side condyle (2) Forward, inward and downward translation of the non-working condyle |
|
|
Laterotrusion |
Movement of the working side condyle in the horizontal plane. May or may not be used in combination to describe other direction movements (i.e. lateroprotrusion, lateroretrusion, etc) |
|
|
Laterodetrusion |
lateral and downward movement of the condyle on the working side |
|
|
Lateroprotrusion |
lateral and forward movement of the condyle on the working side |
|
|
Lateroretrusion |
lateral and backward movement of the condyle on the working side |
|
|
Laterosurtrusion |
lateral and upward movement of the condyle on the working side |
|
|
Mediotrusion |
A movement of the condyle medially |
|
|
Bennet Movement |
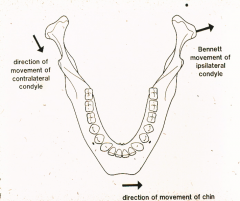
Bodily shift of the mandible toward the working side during lateral excursion. Movement caused by restraint from TMJ ligaments and medial wall of glenoid fossa on the non-working side. Avg lateral mvmt is 0.75 mm |
|
|
Bennet Angle |
The angle formed between the anterior and medial movement of the non-working condyle and the straight protrusive path (s. Related to the degree of Bennet Movement. |
|
|
Functional Movement |
Chewing, swallowing, talking, etc. – all within the confines of the envelope of motion |
|
|
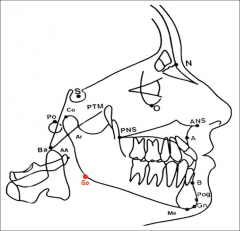
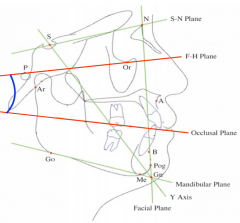
Occlusocranial Relationships |
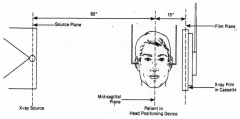
Source Plane to Mid-Sagital Plane >>> 60" Mid-Sagital Plane to Film Plane >>> 15" |
|
|
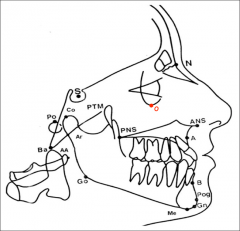
Porion (Po) |
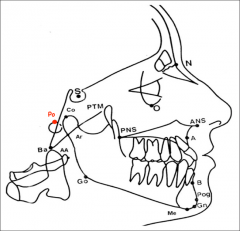
Midpoint of the upper contour of the external auditory meatus |
|
|
Sella (S) |
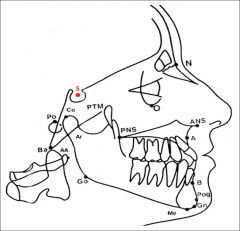
Midpoint of the cavity of sella turcica |
|
|
Orbitale (O) |
The lowest point of the inferior margin of the orbit |
|
|
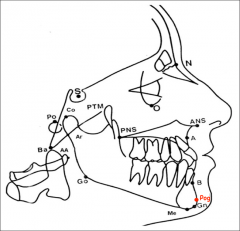
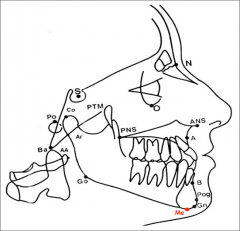
Pogonion (Pog) |
The most anterior point of the contour of the chin |
|
|
Menton (Me) |
Most inferior point on the mandibular symphysis |
|
|
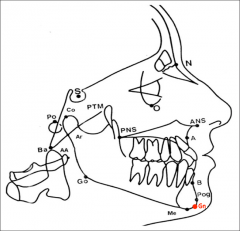
Gnathion (Gn) |
The center of the inferior contour of the chin |
|
|
Gonion (Go) |
The center of the inferior contour of the mandibular angle. |
|
|
Nasion (N) |
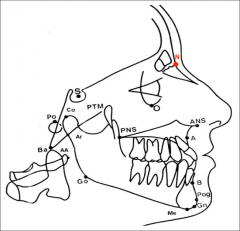
The anterior point of intersection of the frontal bone and nasal bone |
|
|
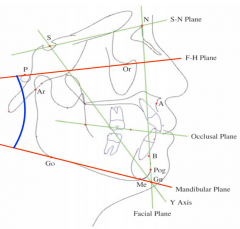
Frankfort Horizontal Plane |
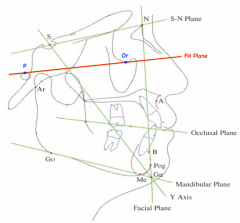
Porion (Po) to Orbitale (O) |
|
|
Occlusal Plane |
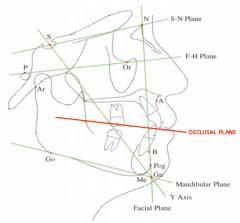
Line bisecting the overlapping cusps of the first molars and incisors |
|
|
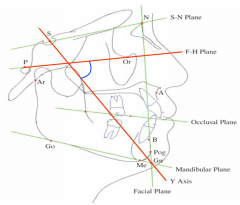
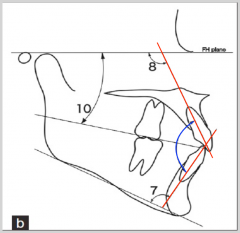
CANT of the Occlusal Plane |
Angle formed between the occlusal plane and Frankfort plane. Mean Angle 9.3 degrees |
|
|
Facial Plane |
Nasion (N) to Pogonion (Po) |
|
|
Facial Angle |
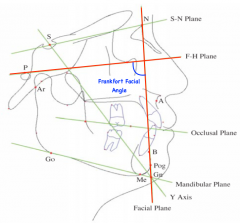
Frankfort-Facial Angle. Indicates degree of protrusion or retrusion of the mandible. Mean Angle 87.7 degrees |
|
|
Axis Orbital Plane |
Plane established by Orbitale (O) and the terminal hinge axis |
|
|
Mandibular Plane |
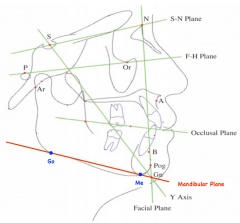
Menton (Me) to Gonion (Go) |
|
|
Frankfort-Mandibular Angle |
Angle between FH plane and mandibular plane. Mean Angle 21.9 degrees |
|
|
Y (Growth) Axis |
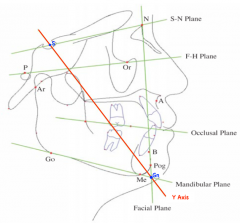
Sella (S) to Gnathion (Gn) |
|
|
Frankfort - Y axis Angle |
Indicates the position of the chin Mean Angle 59.4 degrees |
|
|
Inter-Incisor Angle |
Angle formed by long axis of the upper and lower incisors. Mean Angle 135 degrees |
|
|
Occlusal Plane - Maxillary Central Incisor Angle |
60 degrees |
|
|
Occlusal Plane - Mandibular Central Incisor Angle |
75 degrees |
|
|
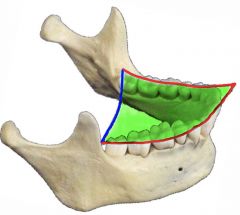
Curve of Spee |
The anterior-posterior curve from the cusp tip of the mandibular canine following through the cusp tips of the posterior teeth |
|
|
Curve of Wilson |
The medio-lateral curve that contacts buccal and lingual cusps of the molars. Lower in the middle due to the lingual inclination of the long axis of mandibular molars. |
|
|
Compensating Curve |
Combination of the Curve of Wilson and Curve of Spee. Used to develop balanced occlusion. |
|
|
Angle's Classification of Occlusion |
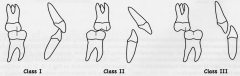
Classification system of occlusion based on the interdigitation of the 1st molars. |
|
|
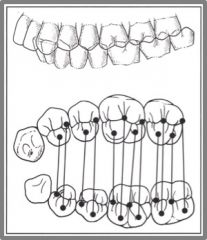
Angle's Class 1 |

NEUTRAL OCCLUSION The maxillary mesiobuccal cusp aligns with the mandibular mesiobuccal groove. |
|
|
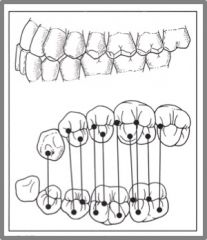
Angle's Class 2 |
ANTERIOR DISPLACEMENT The maxillary mesiobuccal cusp lies anteriorly to the mandibular mesiobuccal groove. |
|
|
Class II Division I |
When Maxillary Anterior Teeth are PROCLINED and a large OVERJET is present |
|
|
Class II Division II |
When Maxillary Anterior Teeth are RETROINCLINED and a deep OVERBITE exists |
|
|
Angle's Class 3 |
POSTERIOR DISPLACEMENT The maxillary mesiobuccal cusp lies posteriorly to the mandibular mesiobuccal groove. |
|
|
Occlusal Table |
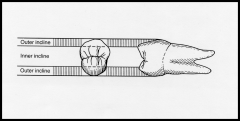
"Inner Incline" of the cusps. 50-60% of the total BL width |
|
|
Supporting Cusps |
OCCLUDING CUSPS (1 mm of contact) MAXILLARY LINGUAL & MANDIBULAR BUCCAL
FUNCTIONAL OUTER ASPECT: outer incline that participates in occlusion |
|
|
Guiding Cusps |
Cusps that do not occlude. MAXILLARY BUCCAL & MANDIBULAR LINGUAL
|
|
|
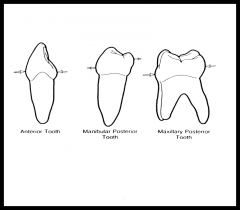
Crown Forms |
BUCCAL-LINGUAL [FRONTAL] > All Teeth: TRAPEZOID MESIAL-DISTAL [PROXIMAL] > Anterior: TRIANGULAR > Post. Max: TRAPEZOID > Post. Man: RHOMBOID |
|
|
Height of Contour |
Facial: > All teeth: cervical 1/3 Lingual: > Anteriors: Cervical 1/3 > Post Max: Middle 1/3 > Post Man: Occlusal 1/3 |
|
|
Over or Under Contouring |
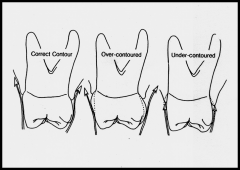
Important for the movement of food away from gingival crevices. |
|
|
Cervical Line Form |
The way the CEJ faces. Flatten as you move posteriorly. [depth decreases] F/L DIRECTED TOWARD THE APEX
M/D DIRECTED TOWARD THE CROWN
|
|
|
Contact Height |
HIGHER ON THE MESIAL THAN THE DISTAL. CONTACT GETS CLOSER TO THE GINGIVA AS YOU MOVE POSTERIORLY |
|
|
Contact Point/Embrasures |
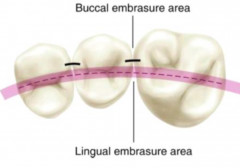
Anterior Teeth: contact divides the tooth equally (B & L embrasures are equal) Posterior Teeth: contact occurs more buccally (lingual embrasure larger than buccal embrasure) |
|
|
Axial Positions |
Mandibular 3rd Molars = largest root inclination [BUCCAL} Maxillary Central Incisors = 2nd largest root inclination [LINGUAL] Maxillary 2nd Premolars = most vertical tooth Mandibular 3rd Molars = tilt mesially & lingually |
|
|
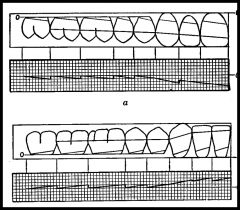
Maxillary Axillary Positions: Lateral View |
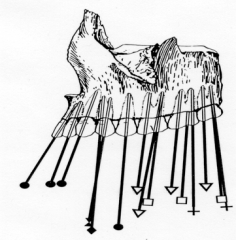
Note that the anteriors are mesially inclined while the most posterior teeth become more distally inclined with reference to the alveolar bone. |
|
|
Maxillary Axillary Positions: Frontal View |
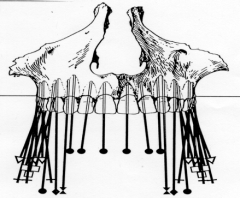
Note that all the posteriors are slightly inclined bucally. Posterior roots incline palatally except for DB root of 1st molar |
|
|
Root Inclination: Maxillary Incisors |
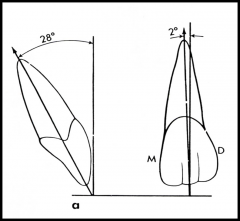
AXIAL: MESIAL INCLINATION Central Incisors = 2 degrees Lateral Incisors = 7 degrees SAGITAL: LINGUAL INCLINATION Central Incisors = 28 degrees Lateral Incisors = 26 degrees |
|
|
Root Inclination: Maxillary Canines |
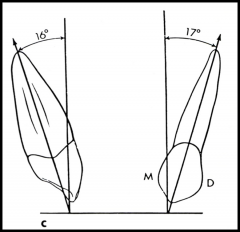
AXIAL: DISTAL INCLINATION Canines = 17 degrees SAGITTAL: LINGUAL INCLINATION Canines = 16 degrees |
|
|
Mandibular Axial Positons: Lateral View |
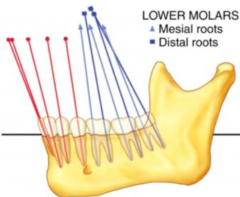
Note that both the anteriors and posteriors are inclined mesially. |
|
|
Mandibular Axial Positions: Frontal View |
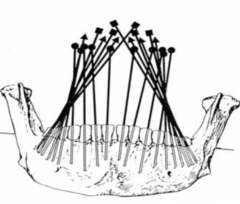
Note that all the posteriors are slightly inclined lingually (with roots inclined buccally). |
|
|
ONLY MANDIBULAR TOOTH WITH LINGUAL INCLINATION TO THE ROOT APEX |
1st PREMOLAR |
|
|
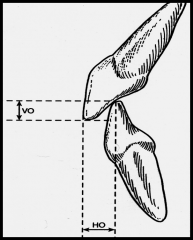
Horizontal & Vertical Overlap |
|
|
|
Overlap and Anterior Guidance |
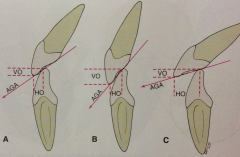
Anterior Guidance INCREASES when: INCREASE VERTICAL OVERLAP DECREASE HORIZONTAL OVERLAP |
|
|
Occlusal Lines |
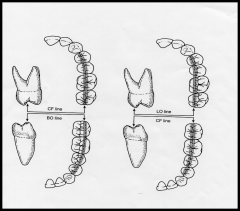
BO line: mandibular buccal cusps LO line = maxillary lingual cusps CF line = central fossa BO-CF line = mandibular buccal and maxillary CF LO-CF line = maxillary lingual and mandibular CF |
|
|
In maximal intercuspal position which teeth occlude with only one opposing tooth? |
Mandibular Central Incisors Maxillary 3rd molars |
|
|
Working Side Condyle |
Rotating Condyle during lateral excursion. |
|
|
Non-woking Side Condyle |
Moves toward median line in lateral excursion. Moves Inward, downward, and forward. |
|
|
Canine Protected Guidance |
Form of mutually protected articulation in which the vertical and horizontal overlap of the canine teeth disengage the posterior teeth in the excursive movements of the mandible. Canines force posterior teeth to disengage during lateral excursion. |
|
|
Mutually Protected Articulation |
An occlusal scheme in which the posterior teeth prevent excessive contact of the anterior teeth in the maximum intercuspation, and the anterior teeth disengage the posterior teeth in all mandibular excursive movements |
|
|
Major Functions Related to Teeth |
|
|
|
What kind of joint is the TMJ? |
COMPOUND JOINT (condylar process, articular fossa, and articular disc) also a synovial joint. |
|
|
2 Joints of the TMJ |
Upper and Lower joint cavities formed by the articular disc. Lower Joint: hinge (ginglymoid joint) Upper Joint: hinge and gliding (ginglymoathroidal joint) |
|
|
TMJ Evolution |
TMJ is a mammalian 'invention'. Vertebrates before mammals formed jaw joint via endochondral bone formation and other portions of jaw via membraneous formation. Immediate mammalian ancestors began forming a second jaw articulation between two bones (mandible and squamous part of temporal bone) developed via membraneous ossification. This new TMJ became dominant, and the endochondral jaw articulation shifted into the middle ear to become the malleus and incus. |
|
|
TMJ Embryology |
TMJ forms between 7th-11th weeks. TMJ malformation caused by teratogens acting during the first trimester. Mesenchymal Formation. Either (1) single mesenchymal formation that differentiates into temporal and mandibular portions or (2) two initially independent mesenchymal condensations termed a temporal blastema and condylar blastema that grow towards each other but remain seperated by other mesenchymal tissue- the tendon of the lateral pterygoid- that becomes trapped between the two bones and separates to form the articular disc. |
|
|
Meckel's Cartilage |
1st pharyngeal arch cartilage that plays indirect role in TMJ formation- acts as central point around which membraneous formation of the mandible occurs. Thus all parts of the mandible are formed around Meckel's cartilage, which ultimately transforms into the sphenomandibular ligament, anterior ligament of the malleus, and the malleus. |
|
|
Development of the TMJ |
Condyle development is secondary cartilage (originates with-in local mesenchymal blastema). This secondary cartilage persists and is gradually replaced by bone until age 17. |
|
|
Mandibular Condyle |
Surface is usually roughened and convex with an ellipsoid shape. The medial pole juts out significantly more than the lateral pole. The long axis of the condylar head is perpendicular to the posteriorly divergent ramus- forming an angle of about 145-160 degrees projecting toward the anterior rim of the foramen magnum (therefore, TMJ radiographs must be taken from an oblique perspective). |
|
|
Pterygoid Fovea |
Shallow cavity located on the anteriomedial aspect of the mandibular neck- where all fibers of the inferior head and most fibers of the superior head attach to the mandible. |
|
|
Blood supply to the condyle |
Inferior alveolar vessels |
|
|
In centric occlusion, the articular surface of the condyles face.. |
the posterior slope of the articular eminence (and not the mandibular fossa) |
|
|
Squamous part of the temporal bone |
Forms the mandibular (glenoid) fossa, which is bound anteriorly by the posterior slope of the articular eminence and posteriorly by the postglenoid tubercle. The roof of the fossa is very thin compact bone with no underlying spongy bone and lined by very thin dense fibrous CT (implies joint is non-weight bearing) It sits anteriorly to the petrotympanic fissure which the chorda tympani and anterior tympanic vessels pass through (not located in TMJ). |
|
|
Articular Disc Attachments |
Biconcave oval structure interposed between the articular surfaces of the TMJ dividing it into inferior and superior joint spaces. It is attach to the condyle at its medial and lateral poles. Posteriorly it is attached to the tympanic plate via the superior retrodiscal lamina and to the mandible via the inferior retrodiscal lamina. Anterior, superior, and inferior attachments are the the articular capsule. |
|
|
Articular Disc Anatomy |
Anterior, Intermediate, and Posterior portions. Posterior is the thickest, Intermediate is the thinnest. Posterior disc in continuous with the highly vascularized and innervated retrodiscal pad. Frontal Cut >> medial portion thicker than the lateral portion |
|
|
Articular Capsule |
Disc merges with joint capsule around its periphery. Firmly attached anteriorly but not medially or laterally. It acts to resist and medial, lateral, or inferior forces. It is highly innervated and thus provides proprioreceptive feedback. |
|
|
Temperomandibular Ligament |
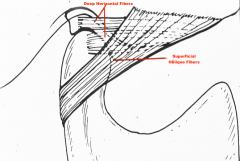
Attaches to the articular capsule laterally providing stability in the posterior-lateral directions. superficial oblique fibers (restrict lateral movement) deep horizontal fibers (limit posterior movement). |
|
|
Accessory Ligaments |
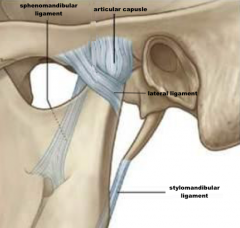
NOT DIRECTLY PART OF THE TMJ BUT PLAY A ROLE IN GUIDING IT. Sphenomandibular ligament attaches to the lingula of the ramus and sphine of sphenoid bone. Stylomandibular ligament attaches to angle of mandible and styloid process. Limits protrusive mvmt. |
|
|
Blood and Nerve Supply |
Blood supply is via branches of the superficial temporal a. and maxillary a. Nerve supply is via the auriculotemporal n. (sensory) with additional branches from nerves supplying muscles of mastication also playing a role in proprioception. Referred pain from the TMJ is frequently to the ear (auriculotemporal n. innervates anterior part of the external auditory meatus) |
|
|
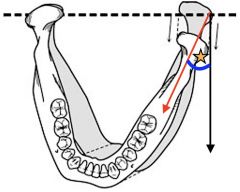
Movements Affecting the Articular Disc |
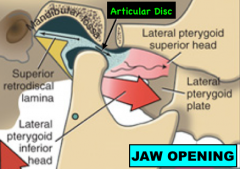
When lateral pterygoid m. contracts to open the jaw it pulls the disc downward & forward along the posterior slope (articular eminence.) Open the jaw a little : bone contact with thick posterior part of the disc. Open the jaw more : bone contact with thick anterior part of the disc. |
|
|
Biomechanics of the TMJ: 2 structurally and functionally distinct systems |
(1) Tissues that surround the inferior synovial cavity (condyle and disc). Disc is tightly bound to condyle by the lateral and medial discal ligaments. Responsible for rotation. (2) Composed of condyle-disc complex functioning against the surface of the mandibular fossa. Because the disc isn't tightly attached to the articular fossa, free sliding movement of the superior portion of the disc and mandibular fossa is possible in the superior cavity. This movement occurs when the mandible is moved anteriorly (translation). |
|
|
TMJ Stability |
TMJ stability is maintained by the constant activity of the muscles of mastication that pull across the joint.
|
|
|
Excessive Condylar Movement During Opening |
During wide yawn or large bite contractions of the lateral pterygoids may pull head of mandible excessive far anteriorly of the convexity of the articular eminence into the temporal fossa. Mandible is protruded and remains fixed in the open position. Muscle of mastication tend to go into spasm. Reduction of this dislocation is achieved by pressing downward and backward on the lower molar teeth. |
|
|
Parotid Gland and TMJ |
Parotid gland divided by facial n. into superficial and deep lobes. The deep lobe is wedged between the mastoid process and TMJ. We avoid impinging it during wide jaw opening through anterior translation. |
|
|
Synovial Fluid Functions |
(1) Provides Lubrication: has viscous, egg-white consistency due to hyalouronic acid secreted by synovial membrane cells. When portion of articular cartilage is compressed it squeezes out fluid that reduces friction. (2) Nourishes the Chondrocytes: normal amount of fluid is very small and must be continually circulated to provide nutrients and waste disposal. Circulates with joint movement and contains phagocytes. (3) Shock Absorber: cushions shocks in the joints subject to compression. When pressure increases it absorbs shock and distributes it evenly across articular surfaces. |
|
|
Types of Cartilage |
(1) Hyaline Cartilage is very spongy making it ideal for compressive forces but susceptible to tearing with friction forces (2) Elastic Cartilage is flexible and snaps back into place but not strong enough for the TMJ (3) FIbrocartilage contains chondrocytes surrounded by tons of collagenous tissue making it ideal for with-standing frictional forces |
|
|
Histology of the TMJ: Articular Cartilage |
Fibrocartilage (not hyaline) covers articular surfaces. Varies in thickness so that it is thicker in locations where bones rub frequently (i.e. condylar eminence) but thinner where we don't need it. |
|
|
Histology of the TMJ: Temporal Bone |
Mandibular Fossa is formed by thin, translucent part compact bone covered by thin dense fibrous CT (no underlying diploic bone or fibrocartilage cover). Articular Eminence is comprised of thick posterior slope and summit. This area has fibrocartilage arranged in two layers: an outer layer with CT fibers arranged in parallel to the bone surface and an inner later with CT fibers perpendicular to the bony surface. |
|
|
Histology of the Articular Disc: Anterior Band |
Smooth surfaces that minimize effects of friction. Anterior band is very vascular and lined by synovial membrane on both sides. It's fibers (collagen/elastin) are oriented anterior-posteriorly and its medial portion is very thick due to tendon of the superior head of lateral pterygoid. |
|
|
Histology of the Articular Disc: Intermediate Zone |
Avascular and not innervated. Consists of fine elastin and collagen fibers oriented anterior-posteriorly. |
|
|
Histology of the Articular Disc: Posterior Band |
Divided into Posterio-inferior and Posterio-superior lamina that surround the retrodiscal pad- which is highly vascular, innervated loose CT lined by synovial membranes on its inferior and superior sides. The posterio-inferior lamina is composed of almost entirely collagenous fibers. The posterio-superior lamina is composed of elastic fibers. Both are arrange in an antero-posterior directions. |
|
|
Why are posterior lamina composed of different types of fibers? |
Condyle and disc displace when jaw opens. Posterior-Superior band has to stretch a ton as it goes from almost vertical to horizontal. Requires elasticity >>> elastin fibers. Posterior-Inferior band doesn't displace much but does have to endure some compressive forces >>> collagen fibers. |
|
|
Histology of the Mandibular Condyle: 3 distinct layers covering the superior aspect |
(1) fibrous articular layer (thick avascular fibrocartilage covering that obscures and smooths bone irregularities. Uniform thickness except in area of contact between condyle and eminence that is compressed during superior joint movement and hence thinner) (2) cellular proliferative layer (6-10 cells thick containing undifferentiated mesenchymal cells w/ potential to form chondroblasts) (3) layer of hyaline growth cartilage (can be divided into an outer zone of matrix formation, middle zone characterized by cellular hypertrophy, and inner zone of calcification and resorption) |
|
|
Histology of the Mandibular Condyle: Bone Type and Formation |
(1) Primary Cartilage Growth Site exhibits interstitial growth where chondrocytes of primary cartilage eventually degenerate and die. (2) Condylar Cartilage exhibits appositional growth from cells produced in the intermediate cellular proliferative layer and cells in condylar cartilage emerge still living at the ossification front Bone marrow of the condyle is hematopoetic type with trabeculae joining compact bone surface at right angles. Posterior-Superior aspect is very vascular. |
|
|
Histology of the Articular Capsule |
Composed of two layers: (1) Outer fibrous capsule termed stratum fibrosum. (2) adjacent to joint spaces is the stratum synovia made up of loosely arranged bundlews and then walled fluid filled spaces |
|
|
Histology of the Synovial Membrane: Structure |
Specialized tissue lining all internal joint surfaces except for the articular surfaces and the disc. It lines the inner surface of the capsule and upper/lower surfaces of the retrodiscal pad (largest surface). Internal surface linings contain vili, or folds that allow the disc to translate by unfolding into a sheet when the jaw opens. The membrane is composed of 2 layers: (1) Intima is adjacent to the joint space and is highly rich in arteriolar/capillary type blood vessels and lymph capillaries. (2) Subintimal/Subsynovial Layer is outer layer composed of fibrous tissue and is poorly vascularized. |
|
|
Histology of the Synovial Membrane: Function |
Major function is to produce synovial fluid which provides nutrition for all non-vascularized portions of the joint, particularly the fibrous CT lining and the disc. Normal joint fluid contains only a few free cells (58% monocytes and 38% macrophages- which remove free fragments that can cause wear and tear). Some cells in the synovial membrane have phagocytic properties and can remove particulate matter- though process may take several months. |
|
|
Synovial Fluid in the TMJ |
Superior Joint Cavity = 1.2 ml Inferior Joint Cavity = .9 ml It is almost impossible to aspirate fluid from either cavity. The synovial fluid function as a shock absorber is minimal in the TMJ (amount of fluid is small and joint is not subject to much compressive force.) |
|
|
Microscopic Innervation of the TMJ: 4 receptors |
(1) Corpuscles of Ruffini located in joint capsule (static mechanoreceptor) (2) Golgi Tendon Organs located in ligaments (static mechanoreceptor) (3) Free Nerve Endings are most abundant and acts as pain receptors. (4) Pacinian Corpuscles are dynamic mechanoreceptors ALL INVOLVED IN REFLEXES PROTECTING JOINT FROM DAMAGE |
|
|
Jaw Openers |
(1) Anterior Digastric (2) Lateral Pterygoid |
|
|
Jaw Closers |
(1) Masseter (2) Temporalis (3) Medial Pterygoid |
|
|
Masseter |
Origin: zygomatic process of the maxilla and inferiorborder of zygomaticarch Insertion: angle of the mandibleinferior, lateral side of ramus Innervation: masseteric n. |
|
|
Temporalis |
Origin: temporal fossa andtemporal fascia (temporal lines of parietal bone) Insertion: coronoid process ofthe mandible Innervation: temporal nerve |
|
|
Medial Pterygoid |
Origin: pterygoid fossa and medial surface of lateralpterygoid plate Insertion: medial aspects of the ramus and angle of the mandible Innervation: medial pterygoid nerve |
|
|
Lateral Pterygoid |
Inferior Head Origin: lateral surface of lateral pterygoid plate Superior Head Origin: infratemporal fossa of greater wing of sphenoid bone Insertion: anterior neck of the mandible Innervation: branch of masseteric or buccal n. Function: pull condyle/diskalong the eminence |
|
|
Digastric |
Origin (posterior digastric): mastoid notch of temporalbone Insertion (anterior digastric): lingual, inferior border ofthe mandible Posterior Digastric Innervation: facial n. Anterior Digastric Innervation: n to mylohyoid (V3) Function: Lowers mandible, elevates hyoid |
|
|
Electromyography: Mechanism |
Muscle Action Potentials Across Membrane: 90 mV (millivolts) Extracellular: 90 uV (microvolts) EMG signal is attenuated at the skin by about 1000 |
|
|
Electromyography: Electrodes |
surface electrodes and needle electrodes |
|
|
Electromyography: Electronics |

1) amplifier 2) analog to digital converter 3) computer 4) display |
|
|
Electromyography: Caveats |
a) Electrical activity must be calibrated to relate directly to muscle force. b) Jaw mm are redundant. SIx jaw closers are all active in jaw adduction. You cannot control the muscle independently. The forces on the jaw must satisfy newtons equations. c) EMG only detects recruitment and frequency (NOT muscle length or contraction velocity) |
|
|
Determinants of Muscle Force |
1) recruitment 2) frequency 3) muscle length 4) velocity |
|
|
Electromyography: Strengths |
(A) know precisely when a muscle is active. (B) know roughly how active. (C) provides insight into MN activity |
|
|
Rest Position Hypothesis |
(1) Passive Elasticity (2) Active Contraction (a) stretch reflex (b) TMJ receptors (c) airway patency |
|
|
Rest Positon: Evidence |
Passive Elasticity:
Active Contraction: FAVORED
|
|
|
Rest Position: Evidence for Active Contraction (Surface EMG and sleep) |
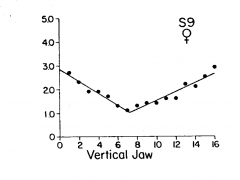
Graph shows EMG activity during jaw opening. Rest Position is 2 mm open. Opening mouth to 7 mm involves decreasing muscle activity indicating it is being actively contracted at rest position. Sleeping shows a similar result (when MN are turned off mouth opens). |
|
|
Mastication Hypothesis |
(1) Alternating Reflex (now disproved) (2) Central Pattern Generator Significance = Part of the theme "be skeptical and critical" |
|
|
Jaw Jerk Reflex |
POSTURAL AND MONOSYNAPTIC
|
|
|
Jaw Opening Reflex |
PROTECTIVE and POLYSYNAPTIC
|
|
|
Electronic Devices for TMD Diagnoses |
Hypotheses: both plausible but no convincing evidence (1) resting EMG greater in TMD patients (2) jaw position differs in TMD patients Evidence to ask for: (a) Sensitivity (ability to detect disease when present) (b) Specificity (ability to detect normal when present) |
|
|
Swallowing (type of activity and control) |
Reflex Activity; Brain Stem |
|
|
Mastication (type of activity and control) |
Rhythmic Activity, Brain Stem |
|
|
Respiration (type of activity and control) |
Rhythmic Activty, Brain Stem |
|
|
Speech (type of activity and control) |
Voluntary Activity, Cortex |
|
|
Deglutition: Purpose |
58% awake but not eating 34% eating 8% sleeping |
|
|
Deglutition: Trigger |
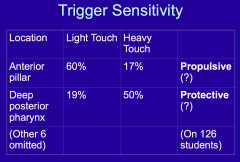
Anterior Pilar = Glossopalatine Arch Posterior Pilar = Pharyngopalatine Arch |
|
|
Deglutition: Afferent and Efferent Input |
AFFERENT (sensory nucleus): CN VII, CN IX, CN X (Nucleus Tractus Solarius) EFFERENT (motor nucleus): CN V (trigeminal motor nucleus) CN VII (facial nucleus) CN IX & CN X (nucleus ambiguus) CN XII (hypoglossal nucleus) C1-C2 (spinal cord) |
|
|
Phases of Swallowing |
Oral: .5 sec, voluntary, facultative Pharyngeal: .7 sec, involuntary, obligate Esophageal: 3 sec (liquid) & 9 sec (solid), involuntary, obligate |
|
|
Obligate Muscles of Deglutition |
Pharyngeal fire at the same time.
Esophageal are delayed and sequential.
|
|
|
Respiration |
One of several activities in the orofacial region competing for attention. Respiratory control center located in the Medulla. a) cyclic contraction/relaxation of the inspiratory mm only (in contrast to alternating of openers and closers in mastication) b) skeletal mm (driven by MN's) c) Typical rate: 15 breathes per minute |
|
|
Control of Respiration |
Respiratory Medulla receives input from mechanoreceptors, chemoreceptors, and the cerebral cortex. It sends nerve impulses to the spinal cord which stimulate respirtatory mm that alter the lungs and chest wall causing ventilation. Alveolar capillary barriers pass oxygen to blood via diffusion. Feedback to mechanoreceptors (chest wall) and chemoreceptors (blood pH and partial pressures. |
|
|
Central Pattern Generator for Respiration |
CPG for respiration in the medulla. 1. Tonic Inspiratory Drive (to inspiratory muscles) 2. Excitation (signals from vagal stretch receptors) 3. Excitation of "cut-off switch" (signal from pneumotoxic center) 4. Inhibition (signal from peripheral and central chemoreceptors) |
|
|
Respiratory Cycle and Swallowing |
Swallowing usually occurs at the end of expiration. It prolongs the respiratory cycle. How frequently we swallow after expiration is based on controls. IT IS NOT RANDOM. |
|
|
Central Pattern Generation |
Neural Input starts and maintains the process. The rhythm generator sets the overall length and duration of the cycle. |
|
|
Speech: Dental Problems |
A) caused by poor dentures... % speech errors after implant prosthesis 1. bilabial sounds (p/b).... 32% 2. labiodental sounds (f/v)... 23% 3. linguopalatal sounds (s/sh)... 33% B) caused by other conditions 1. anterior open bite (f/v) 2. recessive mandible (p/b/m) 3. prognathism (f/v) 4. cleft palate (nasal speech) |
|
|
Speech: Physical Mechanisms |
1. respiration (lungs) 2. phonation (vocal cords) 3. resonance (sinuses) 4. articulation (lips and tongue) CONTINUOUS ACTIVITY is a characteristic of muscles during speech MEDIAL PTERYGOID INVOLVED IN SPEECH, MASSETER/TEMPORALIS MOSTLY UNINVOLVED. |
|
|
Speech: Development |
A. Innate ability to learn language rules. B. Single words at about 1 year. C. Rules of grammar at about 5 years.
D. Speech is uniquely human. |
|
|
Speech: Evolution |
A. All organs evolved for other functions (competition for use) B. Control centers located in the cortex (not brain stem or spinal cord) C. No development across species (origin of language is controversial) |
|
|
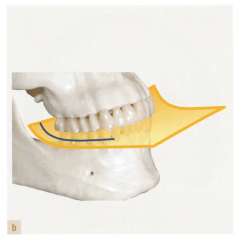
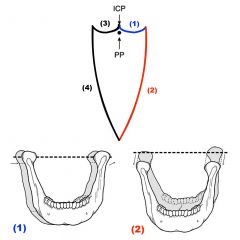
Posselts Sagittal Envelope |
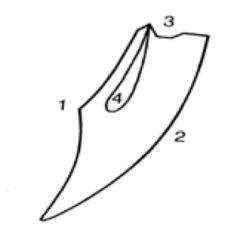
(1) Posterior Opening Border (2) Anterior Opening Border (3) Superior Contact Border (4) Functional Border |
|
|
Anterior/Posterior Borders (Sagittal) |
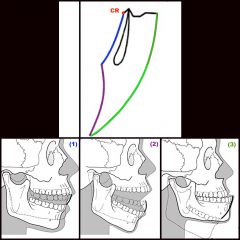
Posterior Border: (1) Rotation (2) Rotation and Translation Anterior Border: (3) Rotation and Translation |
|
|
Superior Contact Border (Sagittal) |

(0) Centric Occlusion (1) Maximal Intercuspation (2) Incisal Guidance (3) Edge-to-Edge Position (4) Beyond Edge-to-Edge |
|
|
What if CO and ICP are the same for an individual? |

There is no upward slide to start the movement. |
|
|
Superior Contact Border varies according to... |
Superior border movement is solely tooth dependent. Changes in the teeth will result in changes in the movement. (1) amount of variation between CR and ICP (2) steepness of the cuspal inclines of the posterior teeth (3) amount of vertical and horizontal overlap of the anterior teeth (4) lingual morphology of the maxillary teeth (5) general interarch relationship of the teeth |
|
|
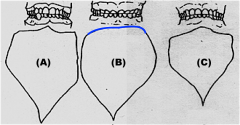
Influence of Head Posture |
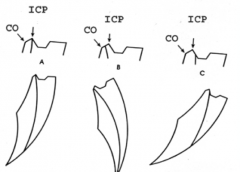
Border movements are not effected by head or body posture. Head posture does, however, influence the final closing position. (A) Neutral Position: close to ICP (B) Chin Up: close posterior to ICP (C) Chin Down: close anterior to ICP |
|
|
Postural Rest Position (PP) |
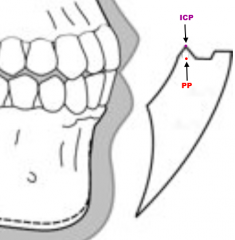
NOT A BORDER POSITION With-in the envelope 2-4 mm below ICP. |
|
|
Horizontal Plane Border |
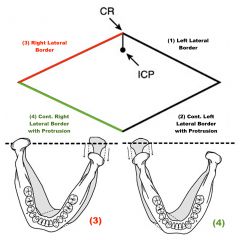
(1) & (3) lateral borders are caused by contraction of the lat. pterygoid on the non-working side- rotating the non-working condyle around the frontal axis of the working condyle. (2) & ( 4) protrusive movement as the working side lat. ptyerygoid contracts bringing the mandible both forward and back toward the midline. |
|
|
How does mandibular positioning affect the horizontal plane border? |

The amount of horizontal border movement decreases as the jaw is opened and you get further from the centric position. |
|
|
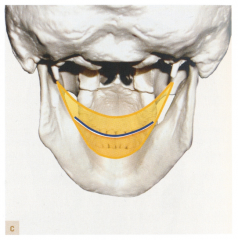
Frontal Plane Borders |
(1) & (3) are superior contact borders determined primarily by tooth contact. Concavity due to incisal edges to dipping to clear the maxillary arch. (2) & (4) are lateral borders that produce convex pathways. The lateral maximum is reached and ligaments tighten pulling the mandible back toward the midline. |
|
|
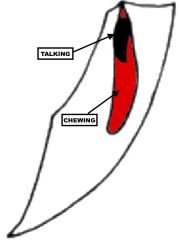
Functional Movements: Sagittal |
|
|
|
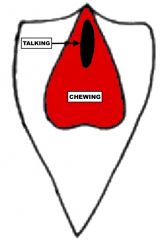
Functional Movements: Frontal |
|
|
|
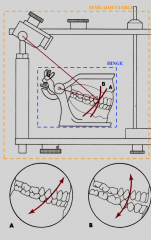
Incisal Guidance and Patient Movement |
(A) Normal (B) No incisal guidance due to worn down teeth (note superior contact border shape) (C) person can't open as wide (could be for number of reasons) Less guidance also causes increased range of functional movements. |
|
|
Side Shift |
When the whole body of the mandible moves (shifts) toward the working side. 2 types: (1) Progressive Side Shift is when the lateral movement of the mandible occurs throughout the entire movement (2) Immediate Side Shift is when the shift occurs early in the movement and is completed before the condyles have finished rotating |
|
|
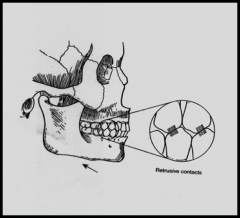
Retrusive Contacts |
|
|
|
Protrusive Contacts |

|
|
|
Mandibular Movements and Effect on Contact with Opposing Arch |

Maxilla: Protrusive = shift anterior Working Side = shift buccally Non-Working = shift mesiolingually Mandible: Protrusive = shift posterior Working Side = shift lingually Non-Working = shift distobuccally |
|
|
Disclusion |
Loss of occlusal contact between opposing teeth during tooth-guided movements or positioning of the mandible. NORMAL CONDITION- EXAMPLE IS POSTERIOR TEETH DISENGAGED DURING PROTRUSIVE MVMT FROM MIP DUE TO ANTERIOR GUIDANCE. |
|
|
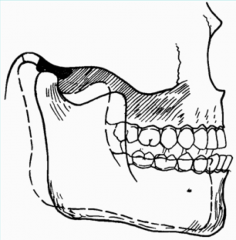
Overbite |
Extension of the maxillary teeth over the mandibular teeth in a vertical direction when the opposing posterior teeth are in centric occlusion [vertical overlap] |
|
|
Overjet |
Projection of the maxillary anterior and/or posterior teeth beyond their protagonists in a horizontal direction when the mandible is in centric occlusion [horizontal overlap]. |
|
|
Occlusal Stability |
Absence of a tendency for teeth to migrate with-in the dentition other than slow physiologic movements usually resulting from tooth wear. |
|
|
Malocclusion |
Any occlusion in which structural characteristics are beyond those established for theoretically ideal occlusion. Doesn't necessarily imply such an occlusion is non-physiologic or that therapy is indicated. [physiologic occlusion = no therapy required] |
|
|
Therapeutic Occlusion |
An occlusion that has been modified by appropriate therapeutic modalities in order to change a non-physiologic occlusion to one that, at the least, falls with-in the parameters of a physiologic occlusion- if not theoretically ideal. Such an occlusion may contain structural modifications not necessarily found in nature, in order to optimize the health and adaptive potential of the masticatory system. |
|
|
Crossbite |
Maxillary BUCCAL cusps contact the CF in the opposing mandibular teeth. Due to discrepancies in skeletal arch size or eruption pattern. |
|
|
Interarch Relationship of Maxillary and Mandibular Teeth |

Mandibular teeth are situated slightly lingual and mesial to their maxillary counterparts. |
|
|
Who Invented the Face Bow? |
George Snow, 1907 |
|
|
Who Invented the first simple articulator? |
Gariot, 1805 |
|
|
Functions of the FaceBow? |
|
|
|
Facebow: Reference Planes |
Axis-Orbitale Plane: true hinge axis Frankfort Plane: arbitrary hinge axis |
|
|
Gysi's Point |
10 mm anterior to the posterior margin of the tragus on a line from the center of the tragus to the outer canthus of the eye |
|
|
Beyron's Point |
13 mm anterior to the posterior margin of the tragus on a line from the center of the tragus to the outer canthus of the eye WHERE TRUE HINGE AXIS IS LOCATED. |
|
|
Fascia Facebow |
- Used orbitale as reference point - Ruler parallel to inter pupillary line - ONLY 2 POINTS OF REFERENCE [basically a bite registration] |
|
|
Ear Facebow |
- anterior reference point is ORBITALE - posterior reference point is PORION ARBITRARY AXIS IS THE CIRCLE 10 mm BEHIND THE EAR PIECE TYPICAL TO USE SPRING BOW INSERT FOR POSTERIOR REFERENCE POINTS MOUNT TO MAXIMAL INTERCUSPATION [ONLY MOUNT TO CENTRIC RELATION FOR COMPLETE DENTURES] |
|
|
Accuracy of an Arbitrary Axis |
"the estimated axis location for most facebows will place the position of the arbitrary axis with +/- 6 mm of the true axis 80% of the time" |
|
|
Open Incisial Pin 3 mm... |
Anterior opening 2 mm Posterior opening 1 mm |
|
|
Weinberg Principle for Selecting Axis |
|
|
|
REARWARD CAST MOUNTING |
CONDYLE BEHIND HINGE AXIS [INFERIOR CONDYLE] ANTERIOR TEETH PREMATURITY POSTERIOR OPEN CONTACT |
|
|
FOREWARD CAST MOUNTING |
CONDYLE IN FRONT OF HINGE AXIS [SUPERIOR CONDYLE] POSTERIOR TEETH PREMATURITY ANTERIOR OPEN CONTACT |
|
|
HIGH CAST MOUNTING |
CONDYLE IS ABOVE HINGE AXIS [RETRUDED CONDYLE] ANTERIOR TEETH PREMATURITY POSTERIOR OPEN CONTACT |
|
|
LOW CAST MOUNTING |
CONDYLE IS BELOW HINGE AXIS [PROTRUDED CONDYLE] POSTERIOR TEETH PREMATURITY ANTERIOR OPEN CONTACT |
|
|
When is True Hinge Axis (terminal hinge axis) required for patients? |
- training programs - very large rehabilitative restorations that require alteration of VDO - high cusp angle interdigitation |
|
|
When is arbitrary hinge axis required? |
- large rehab restorations - to mimimize occlusal error with any restoration - esthetic restorations when visualization and orientation required to fabricate restoration |
|
|
Requirement of an Articulator |
- holds cast in correct horizontal and vertical position - provides a positive anterior vertical stop [incisal pin] - hinge, lateral, and protrusive movements - accept facebow transfer - components move freely/machined accurately - adjustable horizontal/lateral guides - CONDYLAR GUIDES [MECHANICAL FOSSA] AS UPPER FRAME - CONDYLAR ELEMENTS AS LOWER FRAME - ALLOW MECHANISM TO ACCEPT 3rd REFERENCE POINT FROM FACEBOW |
|
|
Limitations of the Articulator |
- mandibular movements are complex 3D movements with the added dimension of TIMING [can't transfer dimension of timing to an articulator] - SIMULATE mandibular movements [CAN NOT duplicate the movements] - Instrument only as good as the operators ability to transfer the information accurately and use the features |
|
|
WEINBERG CLASSIFICATION FOR ARTICULATORS |
1. ARBITRARY 2. POSITIONAL 3. SEMI-ADJUSTABLE
4. FULLY ADJUSTABLE |
|
|
Arbitrary Articular |
- not related to human anatomy - just a mounting of the cast - open and close but NO HINGE MOVEMENT (up & down) - Monson articulator - Hagman Balancer |
|
|
Positional Articulator |
- Only one position is accurate - Stansberry Tripod |
|
|
Arcon Semi-Adjustable Articulator |
*represents the anatomy of the patient - MECHANICAL FOSSA ON UPPER... CONDYLAR SPHERES ON LOWER - angulation of mechanical fossa is FIXED relative to the occlusal plane - set intercondylar distance of 110 mm - adjustable protrusive angle [30 degrees] - centric lock - curved condylar path to represent natural movement - HANUA MODULAR ARTICULATOR |
|
|
Non-Arcon Semi-Adjustable Articulator |
*DO NOT REPRESENT ANATOMY OF PATIENT - MECHANICAL FOSSA ON LOWER/CONDYLAR SPHERE ON UPPER - angulation of the mechanical fossa relative to occlusal plane is NOT FIXED
|
|
|
Limitations of the Semi-Adjsutable Articulator |
- no laterotrusive movement of working side condyle - possible horizontal ridge and groove pathway occlusal interferences [effects angles between medio- and latero- trusive pathways] - designed to have a PROGRESSIVE SIDE SHIFT [can't set immediate shift] - no lateral movement of rotating condyle [possible buccal cusp interference on working side & vertical cusp height determinant] |
|
|
Fully Adjustable Articulator |
- 3D movements can be reproduced with simulataneous pantographic tracings containing 3 planes of space - difficult to use/not really necessary - can't use with facebow and must trace movements - DENAR MK V articulator |
|
|
Limitations of HINGE ARTICULATORS |
1) Distance from condylar axis effects effects the arc of closure contacts [very short distance on hinge articulator] 2) Intercondylar Distance causing disparity in the laterotrusive and mediotrusive pathways. 3) No condylar excursive movement capabilities. |
|
|
Factors of Occlusal Morphology |
1. Neuromuscular [mastication, bruxism, bite force] 2. Diet 3. Age 4. Quality of Occlusal Forces 5. Relationship of Skeletal Components 6. Position of Condylar Axis 7. Vertical/Horizontal Components |
|
|
Mastication |
1. OPENING PHASE - working side rotates/non-working translates - mandible moves forward on working side 2. CRUSHING PHASE - condyle of working side retrudes posterior and laterally 3. GRINDING PHASE - final closure to MIP - bodily movement of mandible on working side [bennett movement] CHEWING HARD FOOD = WIDE CLOSURE/CANINE GLIDING CONTACTS |
|
|
Bruxism |
- bruxism and nothing else = NO BONE LOSS - EMG during nocturnal: bilateral rhythmic bursts followed by 20s of sustained contraction - no cure - teeth flatten and shorten - mouth guard can protect/help prevent additional damage |
|
|
BITE FORCE |
AVG: 150-250 LBS MAX. PARAFUNCTION: 1000 LBS VETERAN EDENTULOUS: 5-8 LBS MAX EDENTULOUS: 50 LBS |
|
|
2. DIET |
When you must grind food more you can wear down your supporting cusps.... - can result in a REVERSE CURVE OF WILSON |
|
|
4. QUALITY OF OCCLUDING SURFACES |
IATROGENIC: problem caused by treatment - rough surfaces can cause problems - zirconium hard to polish/may cause wear |
|
|
6. Position of Condylar Axis |
Length of mandible varies, effecting the posterior cusps. Short Mandible [SMALL ANGLE] = SHARPER CUSPS Tall Mandible [LARGER ANGLE] = SHALLOW CUSPS |
|
|
VERTICAL DETERMINANTS |
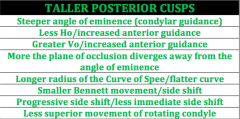
FACTORS THAT INFLUENCE CUSP HIEGHT AND HOW FAR THEY EXTEND INTO DEPTHS OF FOSSA 1. Condylar Guidance [Angle of Eminence] 2. Anterior Guidance 3. Plane of Occlusion 4. Curve of Spee 5. Lateral Translation Movement (1) PCF, (2) ACF, AND (3-5) NEARNESS OF CUSP TO CF's |
|
|
HORIZONTAL DETERMINANTS |
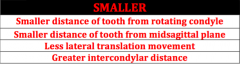
FACTORS INFLUENCING THE DIRECTION OF RIDGES/GROOVES THROUGH THE MEDIO- AND LATEROTRUSIVE PATHWAYS GENERATED 1. Distance between tooth & ROTATING CONDYLE 2. Distance between tooth & MIDSAGGITAL PLANE 3. Lateral Translation Movement 4. Intercondylar Distance |
|
|
Taller Cusp Heights.... |
|
|
|
Smaller Angle between medio- and latero- trusive pathways... |
|
|
|
"Health" [of occlusion] |
structures of occlusal anatomy are in harmony with the structures controlling the movement patterns of the mandible. In any given moment, anatomical relationships [TMJ and anterior teeth] dictate a precise and repeatable pathway. To maintain harmony of occlusal condition = posterior teeth pass close to but don't contact opposing teeth during a mandibular movement |
|
|
Two Structures Controlling Mandibular Movements |
1. Posterior Controlling Factor: TMJ 2. Anterior Controlling Factor: Anterior Teeth - note posterior teeth are in between the two factors, and can be influenced by both... ACF's and PCF's ARE INDEPENDENT OF ONE ANOTHER, BUT STILL FUNCTION TOGETHER TO CONTROL MANDIBULAR MVMT |
|
|
POSTERIOR CONTROLLING FACTORS [PCF's] |
- angle to which condyle moves away from the horizontal reference plane [angle of eminence or condylar guidance angle] - condylar guidance forms a larger angle of mandibular movement during during lateral mvmt than during protrusive movement [medial wall of fossa is steeper compared to fossa anterior to condyle] - FIXED FACTOR |
|
|
ANTERIOR CONTROLLING FACTORS [ACF's] |
- Incisal Guidance VARIABLE FACTOR
* variation of ACF's an important part of treating occlusal disturbances |
|
|
Nearer the tooth is to the TMJ... |
THE MORE THE JOINT ANATOMY WILL EFFECT IS ECCENTRIC MOVEMENT AND THE LESS THE ANATOMY OF THE ANTERIOR TEETH WILL INFLUENCE ITS MOVEMENT. [LIKEWISE FOR NEARNESS TO ANTERIOR TEETH] |
|
|
Ratio/Relationship Between Vertical and Horizontal Determinants |
IMPORTANT TO MANDIBULAR MOVEMENTS BECAUSE: VERTICAL COMPONENT = function of superoinferior movements HORIZONTAL COMPONENT = function of anteroposterior movements ANGLE OF DEVIATION FROM HORIZONTAL REFERENCE PLANE IS WHAT CLINICIANS STUDY IN MANDIBULAR MOVEMENT |
|
|
ORIENTATION OF THE CURVE OF SPEE |
WHERE IS RADIUS FALLS RELATIVE TO LINE PERPENDICULAR TO HORIZONTAL REFERENCE PLANE CAN ALSO HAVE AN EFFECT. All cusps posterior to this line will need shorter cusps than those anterior to it. - If radius is further posterior, more teeth will be located distal to the line and have shorter cusps. - If radius is further anterior, more teeth will be located in front of the line and have longer cusps. |
|
|
DEGREE OF INWARD MOVEMENT OF THE NON-WORKING CONDYLE: |
INFLUENCED BY: 1) Morphology of Medial Wall of Mandibular Fossa 2) Inner Horizontal Portion of TMJ Ligament No Movement when TM LIGAMENT [WORKING SIDE] IS TIGHT and MEDIAL WALL IS CLOSE TO NON-WORKING CONDYLE Lateral movement when ligament loose and non-working condyle moves inward to lateral wall |
|
|
3 ATTRIBUTES OF THE LATERAL TRANSLATION MOVEMENT |
1. AMOUNT 2. TIMING [greatest effect on posterior teeth] 3. DIRECTION |
|
|
Timing of lateral translation... |
If the Side Shift is PROGRESSIVE, amount and direction have little effect on occlusal morphology. But if it's immediate, they have a massive effect. |
|
|
Amount of lateral translation... |
Looser ligament & more medial wall = greater amount of lateral translation movement |
|
|
Direction of lateral translation movement... |
- DEPENDS ON DIRECTION TAKEN BY THE ROTATING (WORKING) CONDYLE DURING THE BODY MOVEMENT - 60 DEGREE CONE ALLOWING COMBINED LATERAL MOVEMENT IN ANTERIOR/POSTERIOR/INFERIOR/SUPERIOR DIRECTIONS LATEROSUPERIOR MOVEMENT --> SHORTER CUSPS LATEROINFERIOR MOVEMENT --> LONGER CUSPS |
|
|
Distance from tooth to Rotating condyle- Maxillary vs Mandibular pathways... |
Maxillary Pathway = generated more distally Mandibular Pathway = generated more mesially |
|
|
Distance from tooth to Mid-sagiital plane- relative effect |
PROXIMITY TO MID-SAGITAL PLANE OUTWEIGHS EFFECT OF DISTANCE FROM THE ROTATING CONDYLE. Generally as one increases the other decreases, but since distance from condyle changes faster PREMOLARS GENERALLY HAVE WIDER ANGLES BETWEEN PATHWAYS THAN THE MOLARS |
|
|
TMD STATS |
- 75% of population - 5-10% diagnosable disorder - most common tx among dentists is splints - women more frequently affected - start to build in teenage years until late 30's then decrease/fade out [not a progressive disease] |
|
|
TMD Symptoms |
Pain in the facial and preauricular area and may include headache Pain aggravated by jaw function Frequently accompanied by: - Limitation of jaw movement - Joint sounds - Pain from palpation of muscles and joints |
|
|
Appropriate Diagnostic Standards |
- Clinical Evaluation [operationalized, reliable, algorithm-driven] - Biomedical Diagnosis [muscle, disk, or arthritic disorder] - Assessment of the Person [function, psychological, co-morbid symptoms, impact of pain on functioning] |
|
|
Dual Axis Classification of TMD |
AXIS I = biomedical model, physical disease AXIS II = biopsychosocial model, bio-behavioral assessment of the person |
|
|
Primary TMD Types |
1. Pain Disorders 2. Mechanical Joint Disorders 3. Degenerative Joint Disorders |
|
|
Pain Disorders |
myalgia: muscle disorder arthralgia: pain in joint |
|
|
Mechanical Joint Problems |
Disk displacement with reduction Disk displacement with locking Disk displacement without reduction |
|
|
Degenerative Joint Disorders |
Osteoarthrosis: observed on radiograph Osteoarthritis: symptomatic - breakdown of condyle and cortical plate - disc breaks down and shreds - for many, still functional is not overdoing the system - opposite mechanism of rheumatoid arthritis |
|
|
Signs and Symptoms of TMD |
Regional pain Limitation in mobility Decreased function Pain on palpation of muscles and joints TMJ noises |
|
|
Why is there no evidence for causation between occlusion and TMD? |
1. Ideal occlusion exist in 5% of population 2. distribution of age & gender of TMD vs Malocclusion 3. Clinical Observational Studies overall have not been replicable, show CNS capacity for adaptation, and individual variability in biology 4. Static occlusion very different from dynamic occlusion 5. Experimental studies showing occlusion interference doesn't trigger new TMD cases & hypervigilance is more important 6. Unpredictable and non-specific treatment response to oral appliances and occlusal adjustment (unknown pathology) |
|
|
STATIC vs DYNAMIC OCCLUSION |
STATICS: account for 5% variance in TMD - anterior open bite - CR to MIP > 2 mm [and asymmetric] - overjet > 4 mm - 5 or more missing teeth DYNAMICS: - degree of orthopedic instability - amount of loading [bruxism, unilateral chewing] - frequnecy of loading - accessory loading |
|
|
Model for Role of Occlusion Affection Masticatory System |
[Normal Function + an 'event'] > [Physiological Tolerance] = TMD SYMPTOMS Normal Function: chew, swallow, speak, emotional expression, breathe Events: a) Local: occlusal changes, sudden strain, overuse, deep pain b) Systemic: emotional, hormonal, general disease Physiological Tolerance: a) Local: departures from stable occlusion [condylar instability, non-longitudinal tooth forces, inappropriate disclusion, iatrogenic/developmental...] b) Systemic: stress, anxiety, depression, personality |
|
|
Occlusal Dysthesia |
Persistant, Uncomfortable Bite Perception or focus leading to perceived symptoms. |
|
|
Bonwill |
|
|
|
Spee |
1. CONTACT SURFACE OF MANDIBLULAR TEETH GLIDE AGAISNT MAXILLARY TEETH 2. AREA OF CONTACT LIE ON SAME CYLINDRICAL SURFACE 3. HORIZONTAL AXIS OF CURVATURE PASS THROUGH MIDDLE OF MESIAL SURFACE OF ORBIT |
|
|
Monson |
|
|
|
Balkwill |
Discovered Bennett Movement |
|
|
Bennett |
Wrote Paper on Bennet Movement |
|
|
Di'Amico |
Canine Protection |
|
|
Christenson's Phenomenon |

|
|
|
Gysi |

|
|
|
Walker |
|
|
|
McCollum |

Kinematic Face Bow |
|
|
Stuart and Stallard |

|
|
|
Schuyler |
- Concluded that balanced contacts of the posterior teeth in either lateral or protrusive eccentric functional movements may be desirable for complete dentures but they are NOT essential for the stability of natural teeth. - The value in distributing functional stress is negative - Shifted away from balanced occlusion in the natural dentition FUNCTIONALISM: sucharrangements of the teeth as will provide the highest efficiency during all the excursions of the mandible which arenecessary to the function of mastication. |
|
|
Beyron |

|
|
|
An evidence-baseddiagnostic system for a disease/disorder such as TMD should include which ofthe following elements: |
Clearly defined procedures Examiner Reliability Biological Plausibility |
|
|
The primary characteristicsof TMD include: |
Preauricular Pain Limitation of Mobility Palpable Tenderness of Muscles |
|
|
A common type of occlusalproblem is the measured discrepancies between the retruded jaw position(centric occlusion) and the maximal position of tooth intercuspation; thesediscrepancies are: |
equally common in individuals with TMD as thosewithout TMD |
|
|
TRUE or FALSE: Limitation ofmovement, one of the primary characteristics of TMD, occurs very often due to mechanicalproblems within the TMJ |
FALSE. Limitation of movementusually has something to do with the brain telling your muscles that theycannot go past a certain point.
It is MYOFASCIAL that primarily accounts forthe majority of TMJ. (can be clenching, etc.) |
|
|
It isoften claimed in the scientific research that TMD is a ___________ disorder,most often without serious morbidity. What evidence supports this claim? |
SELF-LIMITING. Populationepidemiology demonstrates that the prevalence of TMD decreases markedly afterthe age of 40 |
|
|
Accordingto material presented during the lecture, what are the appropriate diagnostic standards for TMD: |
Clinical Evaluation Biomedical Diagnosis Assessment of the Person |
|
|
The primary forms of TMD in terms of prevalence are: |
Myofascial Disorders Arthritis Intracapsular Disorders |
|
|
Anindividual subjected to a severe head and neck trauma that paralyzed his softpalate would most likely demonstrate which of speech issue/s: |
Nasal Speech |
|
|
Defective dentures may cause what speech issues? |
Defective "f" sounds Defective "s" sounds Linguopalatal Sounds [s/sh] |
|
|
Your facebow (Spring bow) is aligned to yourModular Hanau articulator axis via: |
An anterior horizontal mounting offset of approximately 10 mm |
|
|
T or F. Bonwills articulator not only produced balanced occlusion but allowed adjustment of the condylar elements. |
F. No condylar adjustments. |
|
|
Balanced Occlusion Includes the following: |
- Working Side Tooth Contacts - Working Side Cross-Tooth Contacts - Balancing Side Contacts - Protrusive posterior/anterior contacts |
|
|
Bonwill's Triangle... |
10 cm equilateral triangle extending from condyles to MI angle of MANDIBULAR central incisors. |
|
|
In most individuals, when the dentition occludesin centric occlusion, the mandibular arch is: |
POSTERIOR to the MIP |
|
|
In most individuals, when the dentition occludesin maximal intercuspation, the mandibular arch is: |
ANTERIOR to the CR [centric position] |
|
|
Which of the following are remnants of Meckel’scartilage? 1. Condyle 2. Body of mandible 3. Malleus 4. Stylomandibular ligament 5. Sphenomandibular ligament 6. Articular disk 7. Anterior mallear ligament |
Malleus, Sphenomandibular Ligament, and Anterior Mallear Ligament [3, 5, 7] |
|
|
The role of the rhythm generator in the central patterngenerator is: |
Set the overall lengthand duration of the cycle |
|
|
Therole of the cortex in the central pattern generator formastication is: |
Start and Maintain the Process |
|
|
Which of the following are considered trigeminal reflexes: 1. Jaw opening reflex 2. Breathing 3. Blink reflex 4. Jaw closing reflex 5. Gagging 6. Chewing 7. Speaking |
Jaw Opening Reflex, Blink Reflex, Jaw Closing Reflex, Gagging [1,3,4,5] |
|
|
The mandibular border movements along thesuperior border of Posseltt’s envelope of motion is limited by: |
Tooth Contact |
|
|
The reference plane for the hinge axisface bow is: |
AXIS-ORBITAL |
|
|
The anterior reference point for the face bowused with your modular articulator is: |
ORBITALE |
|
|
The occlusal scheme proposed by Bonvillemploying 10 cm equilateral triangle articulator concept was: |
BILATERAL BALANCED OCCLUSION |
|
|
Incisal guidance is best characterized by: |
A. Occurs during protrusive movement B. Is influenced by horizontal and vertical overlapof anterior teeth C. Is influenced by anatomy of maxillary andmandibular teeth |
|
|
Common Pattern of Attrition |
More rapid wear of maxillary lingual and mandibular buccal cusps [supporting cusps] |
|
|
Moving from canines to 3rd molars... [cusp height and MD distance between buccal cusps] |
Mesiodistal Distance between buccal cusps becomes progressively shorter. Cusp Height Gradually decreases [more vertical path during closure] |
|
|
Cross Tooth Balance |
Movement to lateral excursion with simultaneous buccal-to-buccal and lingual-to-lingual cuspcontact on the working side [BALANCED OCCLUSION] |
|
|
Cross Arch Balance |
Movement to lateral excursion with Maxillary Lingual-to-Mandibular Buccal cusp contact on thenon-working side [BALANCED OCCLUSION] |
|
|
Protrusive Balance |
Protrusivemovement with simultaneous contact of maxillary and mandibular incisors, as well as maxillary and mandibularposterior teeth [BALANCED OCCLUSION] |
|
|
The Reference Plane for the Hanau Articulator is: |
Frankfort Horizontal Plane |
|
|
Iffollowing completion of orthodontic treatment, a tooth is not placed in aneutral space position and there are no obstructions to subsequent movement,what is a potential physiologic sequelae? |
The tooth will likely move to aposition where the muscular forces on the tooth are inequilibrium. |
|
Thepicture below illustrates part of the technique used to mount the Hanau Spring Bow. What is the purpose of theoffset depicted in the picture? |
Relate the facebow to arbitrary hinge axis [not relate the facebow to the Frankfort-Orbitale plane for some reason- though that was the arbitrary hinge axis] |