![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
46 Cards in this Set
- Front
- Back
|
Provide 1 example of something an OT would do in practice that reflects the "art" of our work |
Therapist has to be innovative to create plansthat are individually catered to our client. Plans are developed based on thetherapist’s previous experiences and knowledge. Plans should inspire and motivateclients. |
|
|
Provide 1 example of something an OT would do in practice that reflects the "science" of our work |
Therapist has to develop plan for optimalsuccess after gathering information and referring back to evidence basedresearch. Use of hard data and facts are needed as concrete reference |
|
|
Describe the 5 qualities that make up The Nature of Occupation as described by Molineux |
1 – Occupation as active engagement 2 – Occupation as purposeful 3 – Occupation as meaningful 4 – Occupation as contextualised 5 – Occupation as human |
|
|
Describe what is meant by "It is important to appreciate that actual meaning may not be congruent with apparent meaning" by Molineux |
Actual vs. Apparent meaning: meaning attached can be derived from a myriad of sources that many not resemble actual meaning for the individual |
|
|
Name and describe each aspect of the Taxonomic Code of Occupational Performance (TCOP) |
TCOP is to categorise the various levels of complexity of occupational performance and place them in relationship to each other Occupation: an activity or set of activities that is performed with some consistency and regularity, that brings structure, and is given value and meaning by individuals and a culture Activity: a set of tasks with a specific end point or outcome that is greater than that of any constituent task Task: a set of actions having an end point or a specific outcome Action: a set of voluntary movements or mental processes that form a recognisable and purposeful pattern Voluntary movement or mental processes: a simple voluntary muscle or mental activation |
|
|
What are roles? |
a pattern of behaviour that involves certain rights and duties that an individual is expected, trained, and often encouraged to perform in a particular social situation normative models for behaviour shaped by culture and society |
|
|
Name and describe the 8 aspects of environment |
Physical: natural or built/non-human (i.e. temperature or buildings) Social: contributions by behaviours and social interactions (i.e. friends or communities) Cultural: customs, beliefs, activity patterns, behaviour stands and expectations accepted by society defining norms, expectations of roles, social routines, rituals Institutional: associated rules/regulations/policies/practices Socioeconomic: income, financial situation of family, individual, society, country, access to resources Temporal: location of occupational performance in time (i.e. life cycle or time of day) Virtual: technology (i.e. social media or texting) Personal/context: features that impact on performance but aren't part of their health condition/health status (i.e. age or personality) |
|
|
What is a personal theory? |
beliefs held by individuals formed through the experience, perspectives, observations, and exposure to ideas and beliefs |
|
|
Identify the 5 ways Turpin & Iwama describe how models serve practice |
1. Make the professionals assumptions explicit 2. Defines the scope of practice 3. Enhance professionalism and accountability 4. Assists OTs to be systematic and comprehensive 5. Guidance about what could be ideally done |
|
|
Why is enablement important to OT practice? |
enablement is our core competency considered part of our paradigm as the basis of client-centred practice |
|
|
What 6 foundations underpin enablement? |
1. Choice, risk, responsibility: safe, satisfactory engagement in just-right risk-taking 2. Client participation: exerting human agency to participate through individualistic or collectivist engagement 3. Vision of possibility: potential to engage beyond what was imagined to spark readiness and openness to make new changes 4. Change: effecting person, environment, and occupation through means of above foundations 5. Justice: recognition of diversity and inequity shaped by social norms and naming situations PWD encounter 6. Power-sharing: client-centred collaborations |
|
|
Name the 10 enablement skills identified in the CMCE |
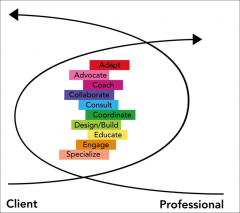
Adapt Advocate Coach Collaborate Consult Coordinate Design/build Educate Engage Specialise |
|
|
Describe the CMOP-E model |
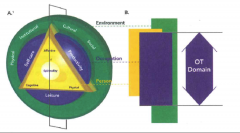
Dynamic interaction of person and occupation embedded within the environment resulting in occupational performance and engagement Spirituality: essence of self Person-cognitive Person-affective Person-physical Occupation-self-care Occupation-productivity Occupation-leisure Environment-cultural Environment-institutional Environment-physical Environment-social |
|
|
Describe the PEO model |
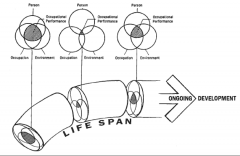
Shift from biomedical model of health where the consideration is in the relationship between the person, environment, and occupation Person: roles and competencies Environment: considers each environmental domain from perspective of the person, household, neighbourhood/community Occupation: activity (basic unit), task (purposeful activity), occupation (groups of activities to engage in) |
|
|
Describe the Kawa model |
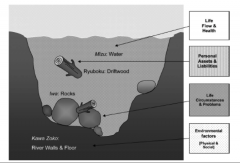
Life flows depicting life's obstacles and challenges Water: life flow and health Driftwood: personal assets and liabilities Rocks: life circumstances and problems River walls and floor: environmental factors (physical and social) |
|
|
Describe the similarities and differences between the 3 models |
Similarities: enacted to enable people to engage in meaningful occupations Differences: CMOP-E: specifically outlined Kawa: client involvement PEO: looks at the interrelationships |
|
|
Describe and differentiate between groups, communities, organisations, and populations |
Group: shared characteristics, expectations, and obligations with a common identity Community: bond between people with shared backgrounds, interests, or experiences sharing a common identity Organisation: social structures created to manage certain functions Population: general society/membership of a broad group of people |
|
|
Name the 6 types of collective occupation |
1. Occupations that express cultural rituals & rules 2. Occupations that offer artistic expression 3. Occupations that sustain social groups 4. Volunteer occupations 5. Work and employment 6. Occupations that generate social capital |
|
|
Describe the 0-1-3 method and describe how this approach fits within Rothman's Framework for community practice |
Forming a basic structural unit of social action |
|
|
Name and describe the key characteristics of the late 1800s to early 1900. Your description should consider what conditions led to each of these periods and how they have benefited the profession as it exits today. |
Philosophical roots Moral treatment: work, rest, play - Participation could restore health and satisfaction Arts and Crafts Movement: re-focus on beauty, craftsmanship and pride in work Mental Hygiene Movement: improving treatment for mental health through 'survival of the fittest' |
|
|
Name and describe the key characteristics of the 1950s to 1980s. Your description should consider what conditions led to each of these periods and how they have benefited the profession as it exits today |
Post WW2: increase pressure to use medications to treat mental illness Mechanistic period: "exact science" rehab focus of "body as machine"treating physical conditions rather than psychosocial wellbeing Reductionism: working with people with acute injuries rather than chronic refocusing on occupation |
|
|
Name and describe the key characteristics of the current period. Your description should consider what conditions led to each of these periods and how they have benefited the profession as it exits today
|
Occupation-focused models WHO new terminology focusing on activity and participation rather than handicap and disability Holistic viewpoint of interdependence of mind, body, and environment |
|
|
Describe 'cultural safety' as discussed in both the Kawa and Culture sessions and how you might deliver 'culturally safe' services as an occupational therapist |
Cultural safety: applying cultural sensitivity so that patients from culturally diverse backgrounds are empowered to determine what sort of care is most appropriate for them spiritually, socially, emotionally, and physically safe no challenges or denial of their identity and what they need shared respect, meaning, knowledge, and experience of learning together |
|
|
Define culture according to the session with Simone and Shameera. |
describes the knowledge, beliefs, values, assumptions, perspectives, attitudes, norms and customs that people acquire through membership of a particular society or group subjected to continuous changes on external and internal dimensions |
|
|
Describe the 'iceberg' model of culture |
Visible part: supported by a much larger and invisible part Cannot immediately realise what the foundations are Major impact into interaction between a health care team and a client or carer and rehab process |
|
|
Name Tymchuk's 7-step process for dealing with a possible ethical issue |
recall: WHHIP COD 1. Who: Describe the parameters of the situation 2. What: Describe the potential issues involved 3. How: Describe the guidelines already available that might affect each issue 4. Imagine Possibilities: enumerate the alternative decisions for each issue 5. Consequences: enumerate the short-term, ongoing, and long-term consequences for each alternative 6. Occurrence: present evidence - or lack thereof- for those consequences and the probability of occurrences 7. Decide: Rank order and vote/decide on decisions |
|
|
Draw and describe the complete "Canadian Practice Process Framework". Please ensure all action points and contextual elements are named and described |
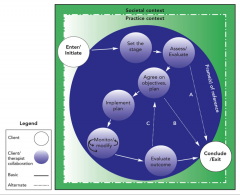
A structured framework for how OTs enable occupation 4 key elements: 1. societal context 2. practice context 3. frame of reference 4. 8 action points: the explicit process you go through from 1st contact to discharge |
|
|
Describe Freire's "banking" concept of education. Describe how this relates to occupational therapy |
Concept of education as an instrument of oppression The narrating subject's (teacher) task is to "fill" the listening objects (student) with the contents of his narration. Contents which are detached from reality. Education becomes an act of depositing instead of communicating. Students patiently receive, memorise, and repeat |
|
|
Name and describe the 3 phases of an interview |
Opening: introduction, purpose of the interview/consent Body: open vs. closed questions, exploration and development phase Closure: summarise, communicate the plan, thank the client |
|
|
Name 5 of the questioning techniques described in the lecture and provide an example of each from your Standardised Patient Interview |
**Pick your favourites** 1. Descriptive questioning (often used at the start) –asking them to describe 2. Background demographic questions 3. Probing or secondary questions 4. Opinion/value questioning 5. Feeling questioning 6. Hypothetical questions 7. Reflective questions 8. Transitional questions 9. Structural questioning – looks at different steps of anactivity 10. Contrast questioning – pain in morning vs night 11. Choice questioning – I notice you’re looking tired, doyou need a break 12. Sensory questioning – scales |
|
|
Name and briefly describe the 3 different interview styles used in therapeutic settings |
Formal: structured interviews Semi-formal: semi-structured Informal: open-ended interviews |
|
|
Identify 1 benefit and 1 drawback of each interview style |
Formal - Pro: provides specific questions, sequence and quantification of responses, focused Con: gives the impression that the interviewer is more interested in getting the answers than hearing about the client Semi-formal - Pro: feels like a conversation; can adjust the interview and probe into different aspects Con: therapist has to know the questions well enough not to rely on them during the interview Informal - Pro: open-ended and less structured, develop questions in response to client information, shows a genuine interest in how clients see things from their own vantage point Con: must be planned, based on earlier info gathering, must be informed by deep working knowledge of specific theory |
|
|
List and describe the four (4) parameters for analysingperformance. |
Value: importance or significance of the task to the individual, will assist in establishing priorities for intervention and target outcome Independence: level of assistance required to perform tasks, consideration for sequence of tasks, practical requirements, location of tasks, how to assess for achievement/breakdowns Safety: extent to which risk is involved when performing tasks, consider frequency of exposure, probability of adverse events, consequence of an adverse event, history of adverse effect Quality: efficiency (quality of action) and effectiveness (outcome); measurable |
|
|
Describehow you could apply these four (4) parameters to the CPPF and the practiceprocess |
Setting the stage you want to find occupations that the client rates as important (finding the value) Assess and evaluate the level of safety occurs during the occupational performance and how much independence |
|
|
Define “narrative” |
a story/verbal report to make sense of life experiences in a client's perspective |
|
|
Identifyfour (4) contributions a narrative approach can bring to the practice of occupationaltherapy |
**Pick your favourite** Address spiritual dimensions of human experiences Provide a means of eliciting values and beliefs from others Help facilitate communication of experience to others Illuminate meanings associated with disability or illness Provide a structure for creating new meaningful experiences in the OT practice context Underpin a narrative process in which therapy becomes part of dramatic plot-line of client life Shape action Provide rich depictions of complex information (i.e. sense of self) Recover voices that illness and treatment often take away |
|
|
Oneof the reasons therapists tell stories is to help persuade others about a pointof view, describe the other reasons therapists tell stories. |
To communicate hope To encourage problem solving/trying things out/teaching a principle To communicate empathy, show you understanding (as much as is possible) To communicate collective nature of the situation To persuade others about a point of view To process our own experience |
|
|
Describewhat a standardised assessment is and then list two (2) benefits ofstandardised assessment. |
Standardised assessment: - To identify/understand occupational performance strengths and challenges Benefits: - To help with goal setting (how much of a change do we want to see?) -To know how effective we've been (did our intervention make a difference?) |
|
|
Describetwo (2) reasons you might choose an observational assessment instead of astandardised assessment. |
Observational assessments must be carried out in context to identify the difference between actual performance and the desired performance Ability to systematically collect and organise data about occupational performance |
|
|
Nameand describe the four (4) major purposes of documentation |
1. Clinical: to facilitate effective treatment 2. Financial: to justify reimbursement 3. Legal/ethical: to stand as a legal document 4. Communication: with treatment team, client, and family |
|
|
Nameand describe the parts that make up a SOAP note |
Subjective: information reported by the patient or carer through client/family centred interview Objective: measurable, quantifiable, and observable data Assessment/analysis: therapist's professional judgement or opinion on functional expectation or limitations Plan: specific plan of action to address problems. May be staged with short and long term goals. |
|
|
Describethe four (4) types of reliability from the lecture and then describe theimportance of reliability for OTs |
Test-retest: same results are obtained with repeated administration Rater reliability: interrater (variation between 2 or more raters who measure the same group of subjects) and intrarater (stability of data recorded by 1 individual across 2 or more trials) Alternate forms: equivalent or parallel versions exist for and instrument Internal consistency: extent to which the items measure various aspects of the same characteristic and nothing else Importance: - Different outcome for client - Different results might not be due to genuine change in the client - has there been an improvement? - Assessments might be administered across services |
|
|
Describe the four (4) types of validity from the lecture and thendescribe the importance of validity for OTs. |
Face: instrument appears to test what it is supposed to Content: items that make up the instrument adequately sample the universe of content that defines the variable being measured Criterion-related: outcome of 1 instrument, the target test, can be used as a substitute measure for an established gold standard (concurrent and predictive) Construct: establishes the ability of the instrument to measure and abstract construct and the degree to which the instrument reflects the theoretical components of the construct Importance: - To determine which assessment tool is appropriate for the questions needed to be answered - Be able to interpret scores meaningfully - Able to demonstrate small changes or improvements |
|
|
Howis occupation incorporated and/or considered in Jo (eating disorders) and Dane’s (ICU and cardio thoracic surgery) work with theirclients/patients? |
Jo: - Improving self-care tasks - Educating on food choices and making food Dane - No active involvement however major focus on future occupational involvement (i.e. prevention of pressure sores) |
|
|
What is the triple jump? Complete the triple jump activity from tutorial George and Stella Lopinski. |
The triple jump is a systematic process of clinical reasoning Step 1: Referral information (formulate a pre-assessment image) - Information on the condition (scientific/procedural reasoning) - Information on the person (narrative reasoning) - What do you imagine your role as an OT would be in that setting? Why? Step 2: Information gathered during the 1st encounter through observation and interview - Identify the cues collected - Develop hypotheses about what the cues mean - How could you test these hypotheses? Step 3: Further information gathering, hypothesis testing and planning intervention - Generate some idea about what occupational issues are and what might be important and how the impairments might impact upon them - Is there anything else you might want to explore? - What goals might be appropriate? |
|
|
Identify three (3) points of critique for the followingoccupational therapy goal set for your client, Mr George Williams, a 79 yearold male who has sustained a fractured neck of femur: Goal:OT will assist Mr George Williams to independently use a long-handled reacher |
Recall: SMART goals 1. Not specific: does not explain how it addressed the identified problem 2. Not measurable: does not explain how the goal will be assessed for success 3. No time: does not indicate a time frame for when the goal will be achieved |