![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
59 Cards in this Set
- Front
- Back
|
note: general distinctions between childhood cancers and adult cancers |

|
|

|
d |
|
|
note: etiologies of childrens cancer role of the environment/ predisposing syndromes? |

|
|
PRESENTATION |
some symptoms more acute.. eg masses, bruises/petichiae, neurological signs |
|
|
general prognosis of some childhood cancers |

|
|

|
s |
|
|
___% will survive at least 5 y from treatment |
82% |
|
|
general prognosis of childhood cancers is pretty good.. |
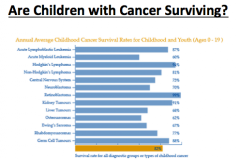
50% is in middle of graph |
|
|
concept in childhood cancer: is cure enough? |
i.e., the quality of the cure is important as the cure itself: need to think about late effects as well. |
|
|
define late effect |
side effects related to tx for cancer that start during treatmetn and persist or occur 5 or more years after treatment for cancer |
|
|
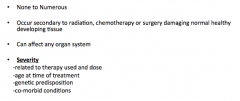
prevalence of late effects |

|
|
|
note: late effects can be related to medical issue, or emotional/psychosocial issue |
d |
|
|
general approach to medical complications of cure |
|
|
|
models of survivorship care...3 |

|
|
|
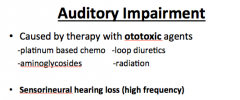
late effects 1. what causes auditory impairment 2. what type of hearing loss |
|
|
|
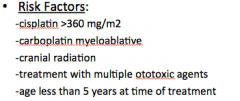
risk factors for auditory hearing loss |

|
|
|
recommended followup in possible ototoxicity |

|
|
|
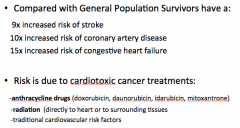
late effects: manifestations of cardiotoxicity |

|
|
|
causes of cardiotoxicity? 2 |
|
|
|
mechanism of anthracycline mediated cardiotoxicity |
loss of myocytes during anthracyclinetherapy impairs myocardial growth leading to gradual increase in LV afterload anddecreased contractility |
|
|
predisposing risk factors for cardiotoxicity 7 |
1. increasing cumulative dose 2. time since treatment 3. mediastinal radiation 4. presence of other cardiac risk factors 5. younger age at treatment 6. pregnancy/new weight lifting: increased load on heart 7. female sex. |
|
|
RT induced cardiotoxicity |
|
|
|
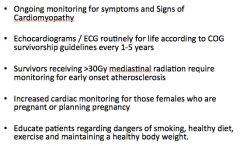
surveillance in cardiotoxicity |
|
|
|
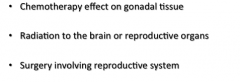
causes of infertility as a late effect? 3 mech |
|
|
|
how does chemo alter fertility? |
damages germinal epithelium |
|
|
fertility and chemo: damage depends on: |
1. age
2. agent 3. dose 4. synergistic toxicity of agents |
|
|
note: chemo and leydig cells |
generally spared: therefore secondary sex char. develop normally |
|
|
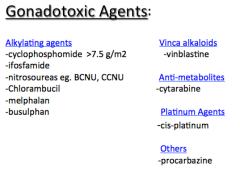
some gonadotoxic agents |
|
|
|
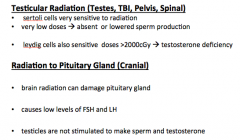
effects of testicular and pituitary gland RT |
|
|
|
Female infertility: can be due to effects of cancer therapy on....3 |
1. ovary 2. uterus 3. brain |
|
|
how does chemo cause ovarian failure |
•Resultsfrom cytotoxic insult depleting ova pool or quickening its decline |
|
|
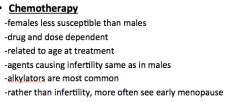
chemotherapy and female fertility: notes 1. susceptibility compared to males 2. DRR 3. age of tx 4. agents? 5. presentation in females ? |
|
|
|
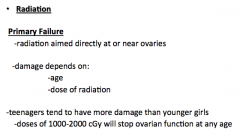
RT and primary ovarian failure note: effects on teenagers vs. younger girls note dose that reliably produces ovarian failure at any age |
|
|
|
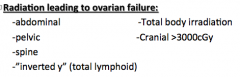
RT and 2ndary ovarian failure? |
-dueto radiation therapy to the brain -doses of > 3000cGy damage pituitarycausing decreased LH/FSH |
|
|
different modalities of RT that lead to ovarian therapy: summary |
|
|
|
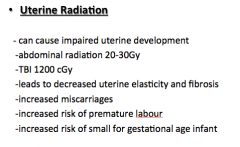
Uterine radiation effects |
|
|
|
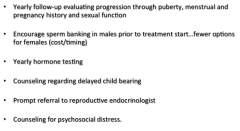
gonadal function surveillance |
|
|
|
2º malignancies in childhood cancer survivors risk increase from general pop? |
incidence of SMN >20% at 30 years post diagnosis primary 6x increased risk |
|
|
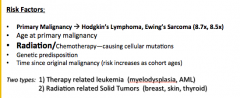
risk factors for SMN 5 |
|
|
|
2 types of 2º malignancies |
1. therapy related leukemia (eg myelodysplasia, AML) 2. radiation related solid tumors (breast, skin, thyroid) |
|
|
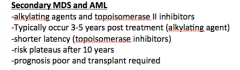
secondary MDS and AML: 1. which agents 2. when does this occur? 3. when does risk plateau? 4. prognosis |
|
|
|
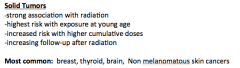
2º solid tumors: relationship with RT |
|
|
|
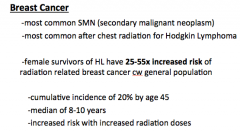
Most common SMN? which patients get this? |
|
|
|
surveillance: skin |
annual physical exam of skin and soft tissue within radiation field |
|
|
surveillance: Leukemias: |
annual CBC |
|
|
surveillance:females with chest radiation |
-monthly breast exams at puberty -yearly mammograms / Breast MRI 8 yearspost radiation or at age 25 whichever is later |
|
|
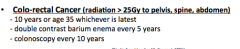
surveillance: RT >25Gy to pelvis, spine, abdomen |
|
|
|
surveillance: other notes |

|
|
|
thryoid abnormalities: 3 |
primary/central hypothryoid benign/malignant thyroid tumors hyperthyroidism can be seen in survivors with radiation to head and neck, spinal, total body |
|
|
surveillance: thyroid |
screen annually |
|
|
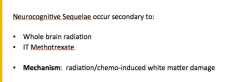
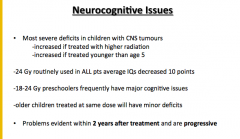
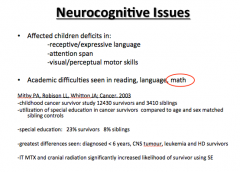
neurocognitive issues: causes 2 |
|
|
|
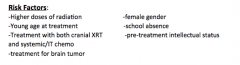
risk factors for neurocognitive sequellae |
|
|
|
|
|
|
surveillance for children receiving therapy potentially affecting their neurocog status |
•Baseline neuropsychological evaluationprior to treatment •Repeat as clinically indicated and at keytransition points •Annualassessments of vocational or educational progress |
|
|
Other medical late effects 1. growth 2. endocrine 3. lungs 3. osteo 5. dental |
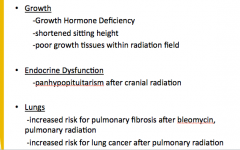
5. osteonecrosis/osteopenia: steroids in ALL 6. dental effects: head and neck cancer, radiation to oropharynx, surgeries involving head and neck region |
|
|
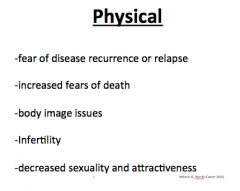
3 categories of psychosocial morbidity among cancer survivors |
1. physical 2. psycholgocial 3. re-entry |
|
|
physical |
|
|
|
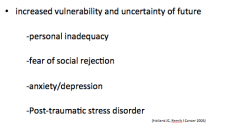
psychological |
|
|
|
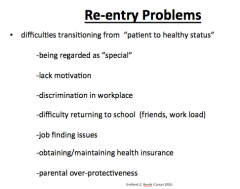
re-entry problems |
|