Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
30 Cards in this Set
- Front
- Back
|
if a pt has a shoulder tear, is OMT indicated? what about a contusion?
|
NO for both
|
|
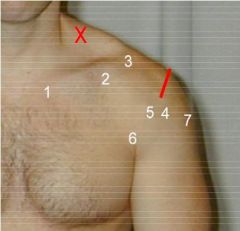
please label
|
1. Sternoclavicular joint
2. Coracoid process 3. Acromioclavicular join Subacromial bursa 4. Greater tuberosity 5. Bicipital groove 6. Lesser tuberosity Subscapularis / Glenohumeral joint 7. Deltoid bursa X. First Rib |
|
|
when do you start to use imaging for diagnosis?
|
after 3 visits with no improvement
|
|
|
list the 5 articulations of the shoulder
|
glenohumeral
acromioclavicular sternoclavicular First rib (costochondral, chondrosternal, costovertebral) Scapulothoracic |
|
|
what are some of the key muscles you must think of when a pt presents with shoulder pain?
|
rotator cuff
supraspinatus (impingement) trapezius rhomboid levator scapulae |
|
|
how do you screen peripheral neuropathy?
|
Spurling's (extend neck rotate head, push down)
positive if pain radiates down same side or Adson's sign (seen when you turn your head to one side, take a deep breath, and the pulse goes away in the arm) |
|
|
in addition to muscular, fracture, or cartilage damage, what is another important consideration when evaluating for shoulder pain
|
neural compression
|
|
|
following history, observation, and palpation, you must make sure to do this in a shoulder pain evaluation
|
Range of Motion testing (major and accessory)
|
|
|
Neer test
|
raise arm over head, look for impingement
|
|
|
Yergason test
|
external rotation of the shoulder against force
|
|
|
when doing ROM testing always make sure to compare
|
active and passive ROM
|
|
|
if pt has reduced shoulder ROM think...
|
adhesive capsulitis
on both active and passive motion |
|
|
when you have shoulder abduction, what is the ratio of scapula rotation to glenohumeral joint abduction?
|
for ever 15 degrees abduction...
5 is scapula; 10 is GH so 1:2 ratio |
|
|
most common SC somatic dysfunction?
|
Anterior and superior glide
|
|
|
Most common AC somatic dysfunction
|
Superior glide
|
|
|
3 counterstrain tenderpoints
Objective |
Supraspinatus
Subscap Levator scap |
|
|
tenderness in bicipital groove alone is clinical of...
|
Biceps Tendonitis
|
|
|
tenderness, position change, edema below AC joint is clinical of..
|
Subacromial bursitis
|
|
|
tenderness at origins and insertions of muscles; MRI evidence can help you find
|
Rotator cuff Strain/Sprain/Tear
|
|
|
pain on abduction, external rotation of humerus and scapula are the clinical findings of?
|
impingement syndrome
|
|
|
limitation of motion in the shoulder on active/passive movement and history can lead you to what diagnosis
|
adhesive capsulitis
|
|
|
what 2 organs can lead to referred shoulder pain?
|
heart and gallbladder
|
|
|
steps for Spencer Technique (in order)
|
Every fat cat tries abduction in pumps
Extension Flexion Compression Traction Abduction Internal rotation Pump |
|
|
for the glenohumeral joint, which way does it glide with aBduction and extension respectively
|
aBduction: inferior
Extension: anterior this can lead to dislocation |
|
|
PAIN IS NEVER A DIAGNOSIS
|
find the cause bro, find the cause
|
|
|
34 year old male presents with right shoulder pain. He has recently resumed an exercise regimen including pushups, rowing machine and free weight curls. Patient has normal reflexes and muscle strength. Glenohumeral joint motion and scapular rotation are normal and elicit no pain. He has positive tenderness at the upper greater tuberosity of the humerus, none at the bicipetal groove or lesser tuberosity. Empty can test is mildly positive. If counterstrain is to be effective for this acute strain, which of the following would represent the usual beginning counterstrain position?
Hold the wrist, flex and adduct the shoulder, and apply slight traction down the arm; Extend arm and rotate the scapula medially with cephalad push abduct the arm about 45°; fine tune with slight arm external rotation Extend, internally rotate and slightly abduct the humerus |
abduct the arm about 45°; fine tune with slight arm external rotation
|
|
|
supraspinatus inserts where
|
greater tubercle of the humerous
|
|
|
A 45 year old female this morning fell off a horse, using an extended arm to break her fall. Radiographs confirm your suspicion from observation of shoulder contour that she has an anterior dislocation, that there is no fracture , and that brachial plexus entrapment is unlikely. Neurological exam is normal. The most appropriate immediate next step would be:
A. Counterstrain OMT B. MRI C. Orthopedic referral D. Rest and ice E. Reduction in the office |
E. Reduction in the office
|
|
|
In palpation of the shoulder:
A. The levator scapula runs from the medial angle of the scapula to C 2 B. The first rib is not a functional part of the shoulder C. The supraspinatus attaches distally to the lesser tuberosity D. The deltoid bursa is best appreciated just below the corocoid process E. The pectoralis minor muscle attaches to the glenoid labrum |
A. The levator scapula runs from the medial angle of the scapula to C 2
|
|
|
List the degrees of ROM for the shoulder
o Extension- o Flexion- o Abduction- o Adduction- o Internal rotation- o External rotation- |
o Extension- 50
o Flexion- 180 o Abduction- 180 o Adduction- 50 o Internal rotation- 90 o External rotation- 90 |