![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
302 Cards in this Set
- Front
- Back
|
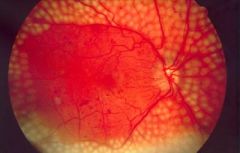
A 54-year-old man with type 2 diabetes mellitus is found on annual review to have new vessel formation at the optic disc. Visual acuity in both eyes is not affected (6/9). Blood pressure is155/84 mmHg.
HbA1c 8.4%
What is the most important intervention to preserve vision in this patient? |
Laser therapy
This patient has proliferative diabetic retinopathy and urgent referral to an ophthalmologist for panretinal photocoagulation is indicated. Good glycaemic control is obviously beneficial in the long-term but this patient needs intervention quickly to preserve his vision. |
|
|
Optic neuritis usually occurs |
over hours or days so not really considered a cause of SUDDEN VISUAL LOSS |
|
|
The most common causes of a sudden painless loss of vision are as follows: |
ischaemic optic neuropathy (e.g. temporal arteritis or atherosclerosis) occlusion of central retinal vein occlusion of central retinal artery vitreous haemorrhage retinal detachment |
|
|
Ischaemic optic neuropathy fxs |
may be due to arteritis (e.g. temporal arteritis) or atherosclerosis (e.g. hypertensive, diabetic older patient) due to occlusion of the short posterior ciliary arteries, causing damage to the optic nerve altitudinal field defects are seen |
|
|
Ischaemic optic neuropathy is associated with |
arteritis e.g. temporal arteritis or atherosclerosis e.g. HTN, DM |
|
|
Central retinal vein occlusion fxs |
incidence increases with age causes: glaucoma, polycythemia, HTN |
|
|
which is more common central retinal artery or vein occlusion |
vein |
|
|
define polycythemia |
increased RBCs causes: - increased RBCs or - decreased plasma |
|
|
difference b/w polycythemia and erythrocytosis |
polycythemia = up rbc numbers erythrocytosis = up rbc mass |
|
|
tx for polycythemia |
venesection |
|
|
different types of polycythemia |
1o and 2o |
|
|
1o polycythemia is due to |
factors INTRINSIC to the RBC precursors |
|
|
examples of 1o polycythemia |
Polycythemia vera (PCV), polycythemia rubra vera (PRV), or erythremia = UP RBC due to bone marrow problem can also get up wbc and platelets |
|
|
Polycythemia vera is classified as a |
myeloproliferative disease complication = acute leukemia (RARE) |
|
|
2o polycythemia is caused by either |
natural or artificial INCREASE IN EPO PRODUCTION |
|
|
2o polycythemia due to natural increase in EPO production aka |
physiologic polycythemia |
|
|
Conditions which may result in a physiologically appropriate polycythemia include: |
altitude related hypoxic disease association iatrogenic (e.g. phlebotomy) genetic |
|
|
pathological causes of 2o polycythemia |
neoplasms anabolic steroids EPO r/t |
|
|
Central retinal vein occlusion KEY Fx
|
severe retinal haemorrhages are usually seen on fundoscopy |
|
|
Central retinal artery occlusion fxs |
include afferent pupillary defect, 'cherry red' spot on a pale retina |
|
|
Differentiating posterior vitreous detachment, retinal detachment and vitreous haemorrhage |
Posterior vitreous detachment = flashing lights peripherally, floaters Retinal detachment = peripheral shadow (moves in), curtain Vitreous hemorrhage = large bleeds cause sudden loss visual loss, dark spots and floaters |
|
|
A 63-year-old man presents to his GP complaining of pain in his right eye. On examination the sclera is red and the pupil is dilated with a hazy cornea. What is the most likely diagnosis? |
Acute angle closure glaucoma |
|
|
Red eye - glaucoma or uveitis? |
glaucoma: severe pain, haloes, 'semi-dilated' pupil uveitis: small, fixed oval pupil, ciliary flush |
|
|
Red eye differentials |
Acute angle closure glaucoma Anterior uveitis Scleritis Conjunctivitis Subconjunctival haemorrhage |
|
|
Acute angle closure glaucoma fxs |
severe pain (may be ocular or headache) decreased visual acuity, patient sees haloes semi-dilated pupil hazy cornea |
|
|
Anterior uveitis fxs |
acute onset pain blurred vision and photophobia small, fixed oval pupil, ciliary flush/fullness |
|
|
Scleritis fxs |
severe pain (may be worse on movement) and tenderness may be underlying autoimmune disease e.g. rheumatoid arthritis |
|
|
AS is associated with |
anterior uveitis |
|
|
Conjunctivitis fxs |
purulent discharge if bacterial, clear discharge if viral |
|
|
Subconjunctival haemorrhage fxs |
history of trauma or coughing bouts |
|
|
A 71-year-old man presents with a burning sensation around his right eye. On examination an erythematous blistering rash can be seen in the right trigeminal distribution. What is the most likely diagnosis? |
Herpes zoster ophthalmicus |
|
|
Herpes zoster ophthalmicus definition |
reactivation of varicella ZOSTER in the opthalmic division of trigeminal |
|
|
Herpes zoster ophthalmicus fxs |
vesicular rash around eye +- the eye Hutchinsons sign: rash on tip/side of nose (due to nasociliary branch of trigeminal) = strong risk factor for ocular involvement |
|
|
Herpes zoster ophthalmicus mgmt |
oral antiviral 7-10days, ideally within 72hrs +- oral corticosteroids (for pain) if eye involved = URGENT OPTHAL R/V |
|
|
Herpes zoster ophthalmicus complications |
ocular: conjunctivitis, keratitis, episcleritis, anterior uveitis ptosis post-herpetic neuralgia |
|

bacterial conjunctivitis tx |
Topical chloramphenicol |
|
|
Conjunctivitis is the most common |
eye problem presenting to primary care |
|
|
bacterial conjunctivitis fxs |
Purulent discharge Eyes may be 'stuck together' in the morning) |
|
|
Viral conjunctivitis fxs |
Serous discharge Recent URTI Preauricular lymph nodes |
|
|
Allergic conjunctivitis fxs |
Bilateral symptoms Itch is prominent May be history of atopy May be seasonal (due to pollen) or perennial (due to dust mite, washing powder or other allergens) |
|
|
mgmt of infective conjunctivitis |
normally settles without tx within 1-2/52 1st line: TOPICAL ABX e.g. chloramphenicol 2nd line and PREG = TOPICAL FUSIDIC ACID |
|
|
with regards to infective conjunctivitis - whats done about contact lens, towels, and school |
dont wear contacts during it dont share towels go to school |
|
|
mgmt of allergic conjunctivitis |
topical or systemic antihistamines topical mast-cell stabilisers, e.g. Sodium cromoglicate and nedocromil |
|
|
Fundoscopy reveals a number of yellow deposits in the left eye consistent with drusen formation. Similar changes but to a lesser extent are seen in the right eye. What is the most likely diagnosis? |
Dry age-related macular degeneration |
|
|
Drusen = |
Dry macular degeneration |
|
|
Age related macular degeneration inV and dx |
optical coherence tomography: provide cross sectional views of the macula if neovascularisation is present fluorescein angiography is performed |
|
|
Age related macular degeneration key is |
degeneration of the macula |
|
|
Traditionally two forms of macular degeneration are seen: |
dry (geographic atrophy) macular degeneration: characterised by drusen - yellow round spots in Bruch's membrane wet (exudative, neovascular) macular degeneration: characterised by choroidal neovascularisation. Leakage of serous fluid and blood can subsequently result in a rapid loss of vision. Carries worst prognosis |
|
|
updated classfication of age related macular degen |
early age related macular degeneration (non-exudative, age related maculopathy): drusen and alterations to the retinal pigment epithelium (RPE) late age related macular degeneration (neovascularisation, exudative) |
|
|
Age related macular degeneration risk factors |
age: most patients are over 60 years of age smoking family history more common in Caucasians high cumulative sunlight exposure female sex |
|
|
Age related macular degeneration fxs |
reduced visual acuity: 'blurred', 'distorted' vision, central vision is affected first central scotomas fundoscopy: drusen, pigmentary changes |
|
|
in age related macular degeneration is central or peripheral vision lost first |
CENTRAL VISION |
|
|
general mgmt of age related macular degeneration |
stop smoking high dose of beta-carotene, vitamins C and E, and zinc may help to slow down visual loss for patients with established macular degeneration. Supplements should be avoided in smokers due to an increased risk of lung cancer |
|
|
Dry macular degeneration tx |
no medical tx just stop smoking next high dose beta carotene, vit C and E and zinc |
|
|
Wet macular degeneration tx |
photocoagulation photodynamic therapy anti-vascular endothelial growth factor (anti-VEGF) treatments: intravitreal ranibizumab |
|
|
Which one of the following is the most common ocular manifestation of rheumatoid arthritis? |
Keratoconjunctivitis sicca |
|
|
Keratoconjunctivitis sicca is characterised by |
dry, burning and gritty eyes caused by decreased tear production |
|
|
Ocular manifestations of rheumatoid arthritis are common, with 25% of patients having eye problems |
true |
|
|
Ocular manifestations of RA |
keratoconjunctivitis sicca (most common) episcleritis (erythema) scleritis (erythema and pain) corneal ulceration keratitis |
|
|
RA drugs can cause what eye problems |
steroid-induced cataracts chloroquine retinopathy |
|
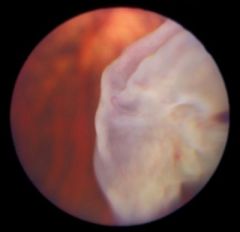
dx |
Treated diabetic retinopathy The fundus shows evidence of previous laser treatment. |
|
|
diabetic retinopathy there are 2 types |
1) non proliferative 2) proliferative |
|
|
diabetic retinopathy - non proliferative type has 2 classfications, an old and a new one - describe the OLD one |
old classfication: Background retinopathy: -microaneurysms (dots) -blot haemorrhages (<=3) -hard exudates Pre-proliferative retinopathy -cotton wool spots (soft exudates; ischaemic nerve fibres) -> 3 blot haemorrhages -venous beading/looping -deep/dark cluster haemorrhages -more common in Type I DM, treat with laser photocoagulation |
|
|
diabetic retinopathy - non proliferative type has 2 classfications, an old and a new one - describe the NEW one |
NEW CLASSIFICATION: Mild NPDR -1 or more microaneurysm Moderate NPDR -microaneurysms -blot haemorrhages -hard exudates -cotton wool spots, venous beading/looping and intraretinal microvascular abnormalities (IRMA) less severe than in severe NPDR Severe NPDR -blot haemorrhages and microaneurysms in 4 quadrants -venous beading in at least 2 quadrants -IRMA in at least 1 quadrant |
|
|
Proliferative retinopathy |
retinal neovascularisation - may lead to vitrous haemorrhage fibrous tissue forming anterior to retinal disc more common in Type I DM, 50% blind in 5 years |
|
|
DIABETIC RETINOPATHY associated maculopathy fxs |
based on location rather than severity, anything is potentially serious hard exudates and other 'background' changes on macula check visual acuity more common in Type II DM |
|
|
Which one of the following is not a risk factor for primary open-angle glaucoma? |
Hypermetropia |
|
|
primary open-angle glaucoma is associated with |
myopia |
|
|
Acute angle closure glaucoma is associated with |
hypermetropia |
|
|
Glaucoma is a group disorders characterised by optic neuropathy due, in the majority of patients, |
to raised intraocular pressure (IOP) |
|
|
Primary open-angle glaucoma (POAG, also referred to as chronic simple glaucoma) risk factors |
over 40yo (2%) family history black patients myopia hypertension diabetes mellitus |
|
|
Primary open-angle glaucoma fxs |
peripheral visual field loss - nasal scotomas progressing to 'tunnel vision' decreased visual acuity optic disc cupping |
|
|
age related macular degeneration vs primary open angle glaucoma |
ARMD = central vision loss, central scotomas POAG = peripheral vision, nasal scotomas |
|
|
Horner's syndrome fxs: |
miosis + ptosis + enophthalmos +/- anhydrosis |
|
|
A patient of yours has been diagnosed with Horner's syndrome. Which of the following is most likely to be seen? |
Miosis + ptosis + enophthalmos |
|
|
heterochromia (difference in iris colour) is seen in congenital Horner's |
true |
|
|
Distinguishing between causes for horners based on anhydrosis |
Central lesions Anhydrosis of the face, arm and trunk Causes: -Stroke -Syringomyelia -Multiple sclerosis -Tumour -Encephalitis Pre-ganglionic lesions Anhydrosis of the face Causes: -Pancoast's tumour -Thyroidectomy -Trauma -Cervical rib Post-ganglionic lesions No anhydrosis Causes: -Carotid artery dissection -Carotid aneurysm -Cavernous sinus thrombosis -Cluster headache |
|
dx |
Retinal detachment |
|

dx |
Age-related macular degeneration |
|
|
mgmt principle for 1o open angle glaucoma |
most managed with eye drops to lower IOP = shown to prevent progressive loss of visual field |
|
|
medical tx of 1o open angle glaucoma |
1st line: Prostaglandin analogues (e.g. Latanoprost) 2nd line: BB e.g. timolol (not for asthma and heart block pxs) others: sympathomimetics e.g. brimonidine (no use if on MAOi/TCA) carbonic anhydrase inhibitors (e.g. dorzolamide) miotics e.g. pilocarpine |
|
|
Prostaglandin analogues (e.g. Latanoprost) moa |
Increases uveoscleral outflow give once daily |
|
|
Prostaglandin analogues (e.g. Latanoprost) AE |
brown pigmentation of the iris |
|
|
Beta-blockers (e.g. Timolol) moa |
Reduces aqueous production |
|
|
Beta-blockers (e.g. Timolol) CI |
Should be avoided in asthmatics and patients with heart block |
|
|
Sympathomimetics (e.g. brimonidine, an alpha2-adrenoceptor agonist) moa |
Reduces aqueous production and increases outflow |
|
|
Sympathomimetics (e.g. brimonidine, an alpha2-adrenoceptor agonist) CI |
Avoid if taking MAOI or tricyclic antidepressants |
|
|
Sympathomimetics (e.g. brimonidine, an alpha2-adrenoceptor agonist) AE |
hyperaemia |
|
|
Carbonic anhydrase inhibitors (e.g. Dorzolamide) moa |
Reduces aqueous production |
|
|
Carbonic anhydrase inhibitors (e.g. Dorzolamide) AE |
Systemic absorption may cause sulphonamide-like reactions |
|
|
Miotics (e.g. pilocarpine, a muscarinic receptor agonist) moa |
Increases uveoscleral outflow |
|
|
Miotics (e.g. pilocarpine, a muscarinic receptor agonist) AE |
constricted pupil, headache and blurred vision |
|
|
Primary open-angle glaucoma: management if refractory cases |
Surgery in the form of a trabeculectomy may be considered in refractory cases. |
|
|
Radioiodine treatment may lead to the development / worsening of |
thyroid eye disease in up to 15% of patients with Grave's disease |
|
|
An 84-year-old man presents with loss of vision in his left eye since the morning. He is otherwise asymptomatic and of note has had no associated eye pain or headaches. His past medical history includes ischaemic heart disease but he is otherwise well. On examination he has no vision in his left eye. The left pupil responds poorly to light but the consensual light reaction is normal. Fundoscopy reveals a red spot over a pale and opaque retina. What is the most likely diagnosis? |
Central retinal artery occlusion |
|

tx |
Papilloedema |
|
|
Papilloedema The following features may be observed during fundoscopy: |
venous engorgement: usually the first sign loss of venous pulsation: although many normal patients do not have normal pulsation blurring of the optic disc margin elevation of optic disc loss of the optic cup Paton's lines: concentric/radial retinal lines cascading from the optic disc |
|
|
Causes of papilloedema |
space-occupying lesion: neoplastic, vascular malignant hypertension idiopathic intracranial hypertension hydrocephalus hypercapnia Rare causes include: hypoparathyroidism and hypocalcaemia vitamin A toxicity |
|
|
Malignant hypertension is |
extremely high blood pressure that develops rapidly and causes some type of organ damage blood pressure that's typically above 180/120. one main cause is stopping antiHTN meds, other common causes: autonomic hyperactivity, collagen-vascular diseases, drug use (particularly stimulants, especially cocaine and amphetamines and theirsubstituted analogues), glomerulonephritis, head trauma, neoplasias, preeclampsia and eclampsia, and renovascular hypertension |
|
|
Colours, especially red, seem 'washed-out'. dx |
Optic neuritis |
|
|
Optic neuritis classic sxs |
Visual loss, eye pain and red desaturation |
|
|
key fx with optic neuritis |
red desaturation ie cant really see red |
|
|
Optic neuritis causes |
MS DM syphilis |
|
|
Optic neuritis fxs |
unilateral decrease in visual acuity over hours or days poor discrimination of colours, 'red desaturation' pain worse on eye movement relative afferent pupillary defect central scotoma |
|
|
Optic neuritis mgmt |
high-dose steroids recovery usually takes 4-6 weeks |
|
|
Optic neuritis prognosis |
MRI: if > 3 white-matter lesions, 5-year risk of developing multiple sclerosis is c. 50% |
|
|
Pituitary tumour associated visual field defect: |
Bitemporal hemianopia, upper quadrant defect |
|
|
Primary open angle glaucoma in right eyeassociated visual field defect: |
Unilateral peripheral visual field loss |
|
|
Patient who has had an extensive stroke with right-sided hemiplegiaassociated visual field defect: |
Right homonymous hemianopia |
|
|
the homonymous hemianopia is always on what side as paresis |
on the SAME SIDE as the paresis |
|

dx |
Hordeolum externum |
|
|
Eyelid problems commonly encountered include: |
blepharitis: inflammation of the eyelid margins typically leading to a red eye stye: infection of the glands of the eyelids chalazion (Meibomian cyst) entropion: in-turning of the eyelids ectropion: out-turning of the eyelids |
|
|
Different types of stye are recognised: |
external (hordeolum externum): -infection (usually staphylococcal) of the glands of Zeis (sebum producing) or glands of Moll (sweat glands). internal (hordeolum internum): - infection of the Meibomian glands. May leave a residual chalazion (Meibomian cyst) |
|
|
STYE mgmt |
includes hot compresses and analgesia if assoc conjunctivitis = ABX |
|
|
A chalazion (Meibomian cyst) is |
a retention cyst of the Meibomian gland. It presents as a firm painless lump in the eyelid. The majority of cases resolve spontaneously but some require surgical drainage |
|
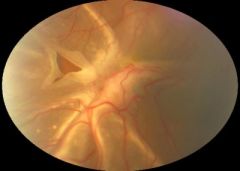
dx |
Retinal detachment |
|
|
A 35-year-old man presents with visual problems. He has had very poor vision in the dark for a long time but is now worried as he is developing 'tunnel vision'. He states his grandfather had a similar problem and was registered blind in his 50's. What is the most likely diagnosis? |
Retinitis pigmentosa |
|
|
px developoing night blindness + tunnel vision - dx |
Retinitis pigmentosa |
|
|
Retinitis pigmentosa mainly affects the |
peripheral retina resulting in tunnel vision |
|
|
Retinitis pigmentosa fxs |
night blindness is often the initial sign funnel vision (the preferred term for tunnel vision) fundoscopy: black bone spicule-shaped pigmentation in the peripheral retina, mottling of the retinal pigment epithelium |
|
|
Retinitis pigmentosa is associated with other diseases - which ones |
Refsum disease: cerebellar ataxia, peripheral neuropathy, deafness, ichthyosis Usher syndrome abetalipoproteinemia Lawrence-Moon-Biedl syndrome Kearns-Sayre syndrome Alport's syndrome |
|
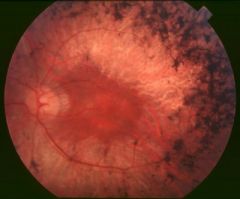
dx |
Fundus showing changes secondary to retinitis pigmentosa |
|
|
Bitemporal hemianopia fxs |
temporal hemianopia lesion of optic chiasm upper quadrant defect > lower quadrant defect = inferior chiasmal compression, commonly a pituitary tumour lower quadrant defect > upper quadrant defect = superior chiasmal compression, commonly a craniopharyngioma |
|
|
Homonymous hemianopia fxs |
incongruous defects: lesion of optic tract congruous defects: lesion of optic radiation or occipital cortex macula sparing: lesion of occipital cortex nb A congruous defect simply means complete or symmetrical visual field loss and conversely an incongruous defect is incomplete or asymmetric. Please see the link for an excellent diagram. |
|
|
Visual field defects The main points for the exam are: |
left homonymous hemianopia means visual field defect to the left, i.e. Lesion of right optic tract homonymous quadrantanopias: PITS (Parietal-Inferior, Temporal-Superior) incongruous defects = optic tract lesion; congruous defects = optic radiation lesion or occipital cortex |
|
|
incongruous defects = optic tract lesion; congruous defects = optic radiation lesion or occipital cortex |
true |
|
|
Smoking is the most important modifiable risk factor for the development of |
thyroid eye disease |
|
|
A 35-year-old female who has recently being diagnosed with Grave's disease presents for review 3 months after starting a 'block and replace' regime with carbimazole and thyroxine. She is concerned about developing thyroid eye disease. What is the best way that her risk of developing thyroid eye disease can be reduced? |
Stop smoking |
|
|
mgmt of thyroid eye disease |
topical lubricants may be needed to help prevent corneal inflammation caused by exposure steroids radiotherapy surgery |
|
|
Thyroid eye disease affects between 25-50% of patients with Graves' disease. |
true |
|
|
Anterior uveitis mgmt |
urgent review by ophthalmology cycloplegics (dilates the pupil which helps to relieve pain and photophobia) e.g. Atropine, cyclopentolate steroid eye drops |
|
|
Anterior uveitis is one of the important differentials of a red eye. It is also referred to as iritis. its associated with |
AS reactive arthritis IBD (both) Bechets dis |
|
|
diagnosis of acute glaucoma. Which of the following should be the aims of treatment? |
Reducing aqueous secretion + inducing pupillary constriction |
|
|
difference b/w anterior uveitis and acute glaucoma in relation to the meds used to manage the pupil |
anterior uveitis - meds for dilating the pupil acute glaucoma - meds used for constricting the pupil |
|
|
In acute angle closure glaucoma (AACG) there is a rise in IOP secondary |
to an impairment of aqueous outflow. |
|
|
Factors predisposing to acute angle closure glaucomaAACG include |
hypermetropia (long-sightedness) pupillary dilatation lens growth associated with age |
|
|
Acute angle closure glaucoma fxs |
severe pain: may be ocular or headache decreased visual acuity symptoms worse with mydriasis (e.g. watching TV in a dark room) hard, red eye haloes around lights semi-dilated non-reacting pupil corneal oedema results in dull or hazy cornea systemic upset may be seen, such as nausea and vomiting and even abdominal pain |
|
|
Acute angle closure glaucoma mgmt |
urgent referral to an ophthalmologist management options include reducing aqueous secretions with acetazolamide and inducing pupillary constriction with topical pilocarpine |
|
|
normal range for intraocular pressure? |
10-21 mmHg |
|

dx |
Sebaceous cyst |
|
dx |
normal |
|

dx |
Background retinopathy |
|
|
A 45-year-old woman with Graves' disease comes for review. She has recently been diagnosed with thyroid eye disease and is being considered for radiotherapy. Over the past three days her right eye has become red and painful. On examination there is proptosis and erythema of the right eye. Visual acuity is 6/9 in both eyes. What complication is she most likely to have developed? |
Exposure keratopathy |
|
|
Exposure keratopathy due to |
radiotherapy for graves dis |
|
|
Ptosis + dilated pupil = |
third nerve palsy |
|
|
ptosis + constricted pupil = |
Horner's |
|
|
A 64-year-old woman presents with bilateral sore eyelids. She also complains of her eyes being dry all the time. On examination her eyelid margins are erythematous at the margins but are not swollen. Of the given options, what is the most appropriate initial management? |
Hot compresses + mechanical removal of lid debris |
|
|
Blepharitis is |
inflammation of the eyelid margins |
|
|
Blepharitis causes |
either meibomian gland dysfunction (common, posterior blepharitis) or seborrhoeic dermatitis/staphylococcal infection (less common, anterior blepharitis) |
|
|
Blepharitis is also more common in patients with rosacea |
true |
|
|
The meibomian glands secrete |
oil on to the eye surface to prevent rapid evaporation of the tear film |
|
|
Any problem affecting the meibomian glands (as in blepharitis) can hence cause drying of the eyes which in turns leads to |
irritation |
|
|
Blepharitis fxs |
symptoms are usually bilateral grittiness and discomfort, particularly around the eyelid margins eyes may be sticky in the morning eyelid margins may be red. Swollen eyelids may be seen in staphylococcal blepharitis styes and chalazions are more common in patients with blepharitis secondary conjunctivitis may occur |
|
|
Blepharitis mgmt |
hot compresses mechanical removal of debri if dry eyes = artificial tears |
|

dx |
Branch retinal vein occlusion Fundoscopy shows flame-shaped haemorrhages on the temporal aspect of the fundus and subretinal haemorrhages |
|
|
A 67-year-old man presents as he has developed a painful blistering rash around his right eye. On examination a vesicular rash covering the right trigeminal nerve dermatome is seen. Currently he has no eye symptoms or signs. Which one of the following is most likely to predict future eye involvement? |
Presence of the rash on the tip of his nose This is Hutchinson's sign which is strongly predictive for ocular involvement. |
|
|
A 43-year-old man with a history of chronic back pain presents to his GP complaining of pain in his left eye and photophobia. On examination the pupil is small, oval shaped and associated with ciliary congestion. What is the most likely diagnosis? |
Anterior uveitis |
|
|
Red eye - glaucoma or uveitis? |
glaucoma: severe pain, haloes, 'semi-dilated' pupil THE GLOC is associated with HELO - COD uveitis: small, fixed oval pupil, ciliary flush - UV light makes you squint = small fixed pupils, you need fluid to keep cool, ciliary makes fluid |
|

dx |
Macular degeneration |
|
|
A 68-year-old man with a history of type 2 diabetes mellitus presens with worsening eye sight. Mydriatic drops are applied and fundoscopy reveals pre-proliferative diabetic retinopathy. A referral to ophthalmology is made. Later in the evening whilst driving home he develops pain in his left eye associated with decreased visual acuity. What is the most likely diagnosis? |
Acute angle closure glaucoma |
|
|
Mydriatic drops are a known precipitant of |
acute angle closure glaucoma |
|
|
Mydriatic drops are applied and fundoscopy reveals pre-proliferative diabetic retinopathy he develops pain in his left eye associated with decreased visual acuity dx |
Acute angle closure glaucoma |
|
|
A 60-year-old woman who has recently started treatment for polymyalgia rheumatica presents with a five day history of headaches and reduced vision on the right side since this morning There is no eye pain but the there is a 'large, dark shadow' covering the superior visual field on the right side. On examination she has a tender, palpable right temporal artery. What is the most likely explanation for the reduced vision? |
Anterior ischemic optic neuropathy |
|
|
Temporal arteritis is large vessel vasculitis which overlaps with |
polymyalgia rheumatica (PMR) |
|
|
Temporal arteritis histology findings |
changes which characteristically 'skips' certain sections of affected artery whilst damaging others. |
|
|
with temporal arteritis you can get visual disturbances how |
secondary to anterior ischemic optic neuropathy |
|
|
A 6-year-old boy is brought to surgery as mum has noticed redness of his right eye. When assessing the child which one of the following features would be most associated with a viral aetiology? |
Preauricular lymph nodes = viral conjunctivitis |
|
|
A 54-year-old woman presents with a persistent watery left eye for the past 4 days. On examination there is erythema and swelling of the inner canthus of the left eye. What is the most likely diagnosis? |
Dacryocystitis |
|
|
Dacryocystitis definition |
infection of the lacrimal sac |
|
|
Dacryocystitis fxs |
watering eye (epiphora) swelling and erythema at the inner canthus of the eye |
|
|
Dacryocystitis mgmt |
systemic abx if px has assoc periorbital cellulitis - give IV abx |
|
|
Congenital lacrimal duct obstruction |
affects around 5-10% of newborns. It is bilateral in around 20% of cases fxs watering eye (even if not crying) secondary infection may occur Symptoms resolve in 99% of cases by 12 months of age |
|
|
Lacrimal duct problems |
Dacryocystitis Congenital lacrimal duct obstruction |
|
|
At what age would the average child be expected to have visual acuity similar to that of an adult? |
2 years |
|
|
vision tests which may be performed when assessing children: |
Birth = Red reflex 6 weeks = Fix and follow to 90 degrees (e.g. Red ball 90cm away) 3 months = Fix and follow to 180 degrees, No squint 12 months = Can pick up 'hundreds and thousands' with pincer grip > 3 years = Letter matching test > 4 years = Snellen charts & Ishihara plates for colour vision |
|
|
A 24-year-old man presents to the emergency department complaining of left eye pain. He has not been able to wear his contact lenses for the past 24 hours due to the pain. He describes the pain as severe and wonders whether he has 'got something stuck in his eye'. On examination there is diffuse hyperaemia of the left eye. The left cornea appears hazy and pupillary reaction is normal. Visual acuity is reduced on the left side and a degree of photophobia is noted. A hypopyon is also seen. What is the most likely diagnosis? |
Keratitis |
|
|
Keratitis describes |
inflammation of the cornea |
|
|
Keratitis causes |
infxn enviro |
|
|
keratitis fxs |
red eye: pain and erythema photophobia foreign body, gritty sensation hypopyon may be seen |
|
|
Infective causes for keratitis |
viral: herpes simplex keratitis bacterial: typically Staphylococcus aureus. Pseudomonas aeruginosa is seen in contact lens wearers fungal amoebic: acanthamoebic keratitis parasitic: onchocercal keratitis ('river blindness') |
|

hypopyon |
exudate in the anterior chamber of the eye |
|
|
enviro causes of keratitis |
hotokeratitis: e.g. welder's arc eye exposure keratitis contact lens acute red eye (CLARE) |
|

dx |
Hypertensive retinopathy |
|
|
Hypertensive retinopathy Keith-Wagener classification of hypertensive retinopathy |
I = Arteriolar narrowing and tortuosity Increased light reflex - silver wiring II = Arteriovenous nipping III = Cotton-wool exudates Flame and blot haemorrhages IV = Papilloedema |
|
|
A 31-year-old man presents with a painful swelling of his right upper eyelid for the past 3 days. On lifting the eyelid a yellow head pointing at the lid margin can be seen. What is the most appropriate management? |
Analgesia + warm compresses dx = stye |
|

dx |
Left-sided ectropion eyelid turned out |
|
|
A 35-year-old man presents with right eye pain which is worse on movement. Examination reveals a relative afferent pupillary defect. Which one of the following is the most likely cause of his problems? |
Multiple sclerosis |
|
|
eye pain which is worse on movement relative afferent pupillary defect. dx |
optic neuritis secondary to multiple sclerosis |
|
|
A 64-year-old woman with type 2 diabetes mellitus presents as she has started to bump into things since the morning. Her medications include metformin, simvastatin and aspirin. Over the previous two days she had noticed numerous 'dark spots' over the vision in her right eye. Examination reveals she has no vision in her right eye. The red reflex on the right side is difficult to elicit and you are unable to visualise the retina on the right side during fundoscopy. Examination of the left fundus reveals changes consistent with pre-proliferative diabetic retinopathy. What is the most likely diagnosis? |
Vitreous haemorrhage |
|
|
Darth Vader is from the Dark Side |
Dark Spots is associated with Vitreous hemorrhage |
|

This diabetic man complained of worsening of his vision. dx |
Proliferative retinopathy |
|
|
A 54-year-old man is noted to have papilloedema on examination. Which one of the following may be responsible? |
Hypercapnia |
|
|
A 40-year-old man presents with bilateral dry, gritty eyes. A diagnosis of blepharitis is considered. Which one of the following is least likely to be associated with blepharitis? |
Viral upper respiratory tract infection |
|
|
Whats the most likely cause of optic neuritis |
MS |
|
|
Which one of the following is least likely to be associated with blepharitis? |
Viral upper respiratory tract infection |
|
|
A 23-year-old female presents with recurrent headaches. Examination of her cranial nerves reveals the right pupil is 3 mm whilst the left pupil is 5 mm. The right pupil constricts to light but the left pupil is sluggish. Peripheral neurological examination is unremarkable apart from difficult to elicit knee and ankle reflexes. What is the most likely diagnosis? |
Holmes-Adie syndrome |
|
|
Holmes-Adie pupil |
is a benign condition most commonly seen in women. It is one of the differentials of a dilated pupil. |
|
|
Holmes-Adie pupil |
is a benign condition most commonly seen in women. It is one of the differentials of a dilated pupil. |
|
|
Holmes-Adie pupil fxs |
unilateral in 80% of cases
dilated pupil
once the pupil has constricted it remains small for an abnormally long time slowly reactive to accommodation but very poorly (if at all) to light |
|
|
Holmes-Adie pupil |
is a benign condition most commonly seen in women. It is one of the differentials of a dilated pupil. |
|
|
Holmes-Adie pupil fxs |
unilateral in 80% of cases
dilated pupil
once the pupil has constricted it remains small for an abnormally long time slowly reactive to accommodation but very poorly (if at all) to light |
|
|
Holmes-Adie syndrome association of |
absent ankle/knee reflexes |
|
|
A 65-year-old man with a history of primary open-angle glaucoma presents with sudden painless loss of vision in his right eye. On examination of the right eye the optic disc is swollen with multiple flame-shaped and blot haemorrhages. What is the most likely diagnosis? |
Occlusion of the central retinal vein |
|
|
Central retinal vein occlusion - fxs |
sudden painless loss of vision,
severe retinal haemorrhages on fundoscopy |
|
|
Adverse effects include brown pigmentation of the iris |
The correct answer is Latanoprost |
|
|
Adverse effects include brown pigmentation of the iris |
The correct answer is Latanoprost |
|
|
Should be avoided in patients taking MAOI drugs
|
Brimonidine |
|
|
Causes pupillary constriction, blurred vision and headaches |
Pilocarpine |
|
|
A mother brings her 8-week-old child in for review. Since birth his right eye has been watering. His symptoms have got worse over the past few days after he picked up a mild viral illness. Clinical examination is unremarkable. What is the most appropriate action? |
Teach nasolacrimal duct massage |
|
|
A mother brings her 8-week-old child in for review. Since birth his right eye has been watering. His symptoms have got worse over the past few days after he picked up a mild viral illness. Clinical examination is unremarkable. What is the most appropriate action? |
Teach nasolacrimal duct massage |
|
|
Nasolacrimal duct obstruction
Most common cause of |
persistent watery eye in an infant |
|
|
Nasolacrimal duct obstruction
Most common cause of |
persistent watery eye in an infant
caused by an imperforate membrane, usually at the lower end of the lacrimal duct |
|
|
Nasolacrimal duct obstruction
Most common cause of |
persistent watery eye in an infant
caused by an imperforate membrane, usually at the lower end of the lacrimal duct
Around 1 in 10 infants have symptoms at around one month of age |
|
|
Management for Nasolacrimal duct obstruction
|
teach parents to massage the lacrimal duct
symptoms resolve in 95% by the age of one year. Unresolved cases should be referred to an ophthalmologist for consideration of probing, which is done under a light general anaesthetic |
|
|
A 70-year-old man is investigated for blurred vision. Fundoscopy reveals drusen, retinal epithelial and macular neovascularisation. A diagnosis of age related macular degeneration is suspected. What is the most appopriate next investigation? |
Fluorescein angiography |
|
|
A 25-year-old woman presents with a one-day history of a painful and red left eye. She describes how her eye is continually streaming tears. On examination she exhibits a degree of photophobia in the affected eye and fluorescein staining demonstrates a small, feathery area of abnormal uptake. Visual acuity is 6/6 in both eyes. What is the most appropriate management? |
Refer immediately to ophthalmology |
|
|
A 25-year-old woman presents with a one-day history of a painful and red left eye. She describes how her eye is continually streaming tears. On examination she exhibits a degree of photophobia in the affected eye and fluorescein staining demonstrates a small, feathery area of abnormal uptake. Visual acuity is 6/6 in both eyes. What is the most appropriate management? |
Refer immediately to ophthalmology |
|
|
This patient may have a corneal abrasion or a dendritic corneal ulcer, particularly given the photophobia. The feathery pattern however points more towards a herpes simplex keratitis. Such a patient should be reviewed immediately by an ophthalmologist. Giving a topical steroid in this situation could be disastrous as it may worsen the infection. |
... |
|
|
Herpes simplex keratitis most commonly presents with a |
dendritic corneal ulcer |
|
|
Herpes simplex keratitis most commonly presents with a |
dendritic corneal ulcer |
|
|
Herpes simplex keratitis
Fxs |
red, painful eye photophobia epiphora visual acuity may be decreased fluorescein staining may show an epithelial ulcer |
|
|
Herpes simplex keratitis
Management |
immediate referral to an ophthalmologist
topical aciclovir |
|
|
A 54-year-old female presents to the Emergency Department concerned about double vision. She is noted to have exophthalmos and conjunctival oedema on examination and a diagnosis of thyroid eye disease is suspected. What can be said regarding her thyroid status? |
Thyroid eye disease affects between 25-50% of patients with Graves' disease.
Pathophysiology it is thought to be caused by an autoimmune response against an autoantigen, possibly the TSH receptor → retro-orbital inflammation the inflammation results in glycosaminoglycan and collagen deposition in the muscles
Prevention smoking is the most important modifiable risk factor for the development of thyroid eye disease radioiodine treatment may increase the inflammatory symptoms seen in thyroid eye disease. In a recent study of patients with Graves' disease around 15% developed, or had worsening of, eye disease. Prednisolone may help reduce the risk
Features the patient may be eu-, hypo- or hyperthyroid at the time of presentation exophthalmos conjunctival oedema optic disc swelling ophthalmoplegia inability to close the eye lids may lead to sore, dry eyes. If severe and untreated patients can be at risk of exposure keratopathy
Management topical lubricants may be needed to help prevent corneal inflammation caused by exposure steroids radiotherapy surgery
Monitoring patients with established thyroid eye disease
For patients with established thyroid eye disease the following symptoms/signs should indicate the need for urgent review by an ophthalmologist (see EUGOGO guidelines): unexplained deterioration in vision awareness of change in intensity or quality of colour vision in one or both eyes history of eye suddenly 'popping out' (globe subluxation) obvious corneal opacity cornea still visible when the eyelids are closed disc swelling Next question |
|
|
A 69-year-old man presents with blurred vision. His GP suspects a diagnosis of primary open-angle glaucoma (POAG). Which one of the following features would be most consistent with a diagnosis of POAG? |
Peripheral visual field loss |
|
|
A 39-year-old woman with a history of rheumatoid arthritis presents with a two day history of a red right eye. There is no itch or pain. Pupils are 3mm, equal and reactive to light. Visual acuity is 6/5 in both eyes. What is the most likely diagnosis? |
Episcleritis |
|
|
Scleritis is painful, episcleritis is not painful |
True |
|
|
Ocular manifestations of RA |
keratoconjunctivitis sicca (most common) episcleritis (erythema) scleritis (erythema and pain) corneal ulceration keratitis |
|
|
Ocular manifestations of RA |
keratoconjunctivitis sicca (most common) episcleritis (erythema) scleritis (erythema and pain) corneal ulceration keratitis |
|
|
A 65-year-old man presents with an acute, painful red eye. Which one of the following features would not support a diagnosis of acute angle closure glaucoma? |
Small pupil |
|
|
Ocular manifestations of RA |
keratoconjunctivitis sicca (most common) episcleritis (erythema) scleritis (erythema and pain) corneal ulceration keratitis |
|
|
A 65-year-old man presents with an acute, painful red eye. Which one of the following features would not support a diagnosis of acute angle closure glaucoma? |
Small pupil |
|
|
A 70-year-old woman presents with loss of vision in her left eye. For the past two weeks she has painful frontal headaches and has been feeling generally lethargic. On examination visual acuity is 6/9 in the right eye but on the left side only hand movements can be made seen. Fundoscopy of the left side reveals a pale and oedematous optic disc. What is the most likely diagnosis?. |
Temporal arteritis |
|
|
Ocular manifestations of RA |
keratoconjunctivitis sicca (most common) episcleritis (erythema) scleritis (erythema and pain) corneal ulceration keratitis |
|
|
A 65-year-old man presents with an acute, painful red eye. Which one of the following features would not support a diagnosis of acute angle closure glaucoma? |
Small pupil |
|
|
A 70-year-old woman presents with loss of vision in her left eye. For the past two weeks she has painful frontal headaches and has been feeling generally lethargic. On examination visual acuity is 6/9 in the right eye but on the left side only hand movements can be made seen. Fundoscopy of the left side reveals a pale and oedematous optic disc. What is the most likely diagnosis?. |
Temporal arteritis |
|
|
A 22-year-old man is referred to urology with possible urinary retention. He is passing huge amounts of urine. Post void bladder ultrasound is normal. |
The correct answer is Lower bitemporal hemianopia
This patient has diabetes insipidus due to a craniopharyngioma. This causes a lower bitemporal hemianopia. |
|
|
diagnosis of herpes zoster ophthalmicus is made and an urgent referral to ophthalmology is made. What treatment is she most likely to be given? |
Oral aciclovir |
|
|
Which one of the following conditions would most predispose you to developing anterior uveitis? |
Crohn's disease |
|
|
A 65-year-old woman presents with visual problems. She suffers from rheumatoid arthritis, depression and takes medication to control her blood pressure. Over the past few days she has been getting troublesome headaches and blurred vision but today has noted a marked reduction in vision in the right eye. On examination her right eye is red, has a sluggish pupil and a corrected visual acuity 6/30. Her medication has recently been changed. Which one of the following drugs is most likely to have precipitated this event? |
Amitriptyline |
|
|
Drugs which may precipitate acute glaucoma include |
anticholinergics and tricyclic antidepressants |
|
|
Drugs which may precipitate acute glaucoma include |
anticholinergics and tricyclic antidepressants |
|
|
dry age-related macular degeneration is reviewed. Unfortunately her eyesight has deteriorated over the past six months. She has never smoked and is taking antioxidant supplements. What is the most appropriate next step? |
Explain no other medical therapies currently available |
|
|
A 34-year-old woman presents complaining of headaches. Examination of her pupils using a light shone alternately in each eye reveals that when the light is shone in the right eye both pupils constrict but when the light source immediately moves to the left eye both eyes appear to dilate.
What is the most likely diagnosis? |
Left optic neuritis
This is the 'swinging light test' and reveals a relative afferent pupillary defect. As there is a defect in the afferent nerve on the left side the pupils constrict less than normal, giving the impression of dilation.
Given her age, multiple sclerosis causing optic neuritis is the likely underlying diagnosis. Optic neuritis typically causes a dull ache in the region of the eye which is aggravated by movement |
|
|
Relative afferent pupillary defect aka |
Also known as the Marcus-Gunn pupil, a relative afferent pupillary defect is found by the swinging light test
It is caused by a lesion anterior to the optic chiasm i.e. optic nerve or retina |
|
|
Relative afferent pupillary defect aka |
Also known as the Marcus-Gunn pupil, a relative afferent pupillary defect is found by the swinging light test
It is caused by a lesion anterior to the optic chiasm i.e. optic nerve or retina |
|
|
Relative afferent pupillary defect causes |
retina: detachment
optic nerve: optic neuritis e.g. multiple sclerosis |
|
|
Relative afferent pupillary defect aka |
Also known as the Marcus-Gunn pupil, a relative afferent pupillary defect is found by the swinging light test
It is caused by a lesion anterior to the optic chiasm i.e. optic nerve or retina |
|
|
Relative afferent pupillary defect causes |
retina: detachment
optic nerve: optic neuritis e.g. multiple sclerosis |
|
|
Pathway of pupillary light reflex |
afferent: retina → optic nerve → lateral geniculate body → midbrain
efferent: Edinger-Westphal nucleus (midbrain) → oculomotor nerve |
|
|
Relative afferent pupillary defect aka |
Also known as the Marcus-Gunn pupil, a relative afferent pupillary defect is found by the swinging light test
It is caused by a lesion anterior to the optic chiasm i.e. optic nerve or retina |
|
|
Relative afferent pupillary defect causes |
retina: detachment
optic nerve: optic neuritis e.g. multiple sclerosis |
|
|
Pathway of pupillary light reflex |
afferent: retina → optic nerve → lateral geniculate body → midbrain
efferent: Edinger-Westphal nucleus (midbrain) → oculomotor nerve |
|
|
A 74-year-old man presents with a severe throbbing headache on the right side of his head. He has now had this pain for around 6-7 days but reports no obvious trigger. There have been no visual disturbances or episodes of limb weakness. Neurological examination is unremarkable. The right side of his head is tender to touch but he cannot remember falling. Given the likely diagnosis what is the most important initial step? |
Give high-dose oral prednisolone
Dx temporal arteritis |
|
|
Each one of the following is a cause of a mydriatic pupil, except: |
Argyll-Robertson pupil |
|
|
Relative afferent pupillary defect aka |
Also known as the Marcus-Gunn pupil, a relative afferent pupillary defect is found by the swinging light test
It is caused by a lesion anterior to the optic chiasm i.e. optic nerve or retina |
|
|
Relative afferent pupillary defect causes |
retina: detachment
optic nerve: optic neuritis e.g. multiple sclerosis |
|
|
Pathway of pupillary light reflex |
afferent: retina → optic nerve → lateral geniculate body → midbrain
efferent: Edinger-Westphal nucleus (midbrain) → oculomotor nerve |
|
|
A 74-year-old man presents with a severe throbbing headache on the right side of his head. He has now had this pain for around 6-7 days but reports no obvious trigger. There have been no visual disturbances or episodes of limb weakness. Neurological examination is unremarkable. The right side of his head is tender to touch but he cannot remember falling. Given the likely diagnosis what is the most important initial step? |
Give high-dose oral prednisolone
Dx temporal arteritis |
|
|
Each one of the following is a cause of a mydriatic pupil, except: |
Argyll-Robertson pupil |
|
|
Argyll-Robertson pupil is one of the classic pupillary syndrome. It is sometimes seen in neurosyphilis and is often said to be the prostitute's pupil - accommodates but doesn't react. Another mnemonic used for the Argyll-Robertson Pupil (ARP) is Accommodation Reflex Present (ARP) but Pupillary Reflex Absent (PRA) |
Features small, irregular pupils no response to light but there is a response to accommodate
Causes diabetes mellitus syphilis |
|
|
Relative afferent pupillary defect aka |
Also known as the Marcus-Gunn pupil, a relative afferent pupillary defect is found by the swinging light test
It is caused by a lesion anterior to the optic chiasm i.e. optic nerve or retina |
|
|
Relative afferent pupillary defect causes |
retina: detachment
optic nerve: optic neuritis e.g. multiple sclerosis |
|
|
Pathway of pupillary light reflex |
afferent: retina → optic nerve → lateral geniculate body → midbrain
efferent: Edinger-Westphal nucleus (midbrain) → oculomotor nerve |
|
|
A 74-year-old man presents with a severe throbbing headache on the right side of his head. He has now had this pain for around 6-7 days but reports no obvious trigger. There have been no visual disturbances or episodes of limb weakness. Neurological examination is unremarkable. The right side of his head is tender to touch but he cannot remember falling. Given the likely diagnosis what is the most important initial step? |
Give high-dose oral prednisolone
Dx temporal arteritis |
|
|
Each one of the following is a cause of a mydriatic pupil, except: |
Argyll-Robertson pupil |
|
|
Argyll-Robertson pupil is one of the classic pupillary syndrome. It is sometimes seen in neurosyphilis and is often said to be the prostitute's pupil - accommodates but doesn't react. Another mnemonic used for the Argyll-Robertson Pupil (ARP) is Accommodation Reflex Present (ARP) but Pupillary Reflex Absent (PRA) |
Features small, irregular pupils no response to light but there is a response to accommodate
Causes diabetes mellitus syphilis |
|
|
Causes of mydriasis (large pupil) |
third nerve palsy Holmes-Adie pupil traumatic iridoplegia phaeochromocytoma congenital |
|
|
Relative afferent pupillary defect aka |
Also known as the Marcus-Gunn pupil, a relative afferent pupillary defect is found by the swinging light test
It is caused by a lesion anterior to the optic chiasm i.e. optic nerve or retina |
|
|
Relative afferent pupillary defect causes |
retina: detachment
optic nerve: optic neuritis e.g. multiple sclerosis |
|
|
Pathway of pupillary light reflex |
afferent: retina → optic nerve → lateral geniculate body → midbrain
efferent: Edinger-Westphal nucleus (midbrain) → oculomotor nerve |
|
|
A 74-year-old man presents with a severe throbbing headache on the right side of his head. He has now had this pain for around 6-7 days but reports no obvious trigger. There have been no visual disturbances or episodes of limb weakness. Neurological examination is unremarkable. The right side of his head is tender to touch but he cannot remember falling. Given the likely diagnosis what is the most important initial step? |
Give high-dose oral prednisolone
Dx temporal arteritis |
|
|
Each one of the following is a cause of a mydriatic pupil, except: |
Argyll-Robertson pupil |
|
|
Argyll-Robertson pupil is one of the classic pupillary syndrome. It is sometimes seen in neurosyphilis and is often said to be the prostitute's pupil - accommodates but doesn't react. Another mnemonic used for the Argyll-Robertson Pupil (ARP) is Accommodation Reflex Present (ARP) but Pupillary Reflex Absent (PRA) |
Features small, irregular pupils no response to light but there is a response to accommodate
Causes diabetes mellitus syphilis |
|
|
Causes of mydriasis (large pupil) |
third nerve palsy Holmes-Adie pupil traumatic iridoplegia phaeochromocytoma congenital |
|
|
Drug causes of mydriasis |
topical mydriatics: tropicamide, atropine
sympathomimetic drugs: amphetamines, cocaine
anticholinergic drugs: tricyclic antidepressants |
|
|
Which one of the following is associated with heterochromia in congenital disease? |
Horner's syndrome |
|
|
A 45-year-old man presents with a two week history of a painless lump in his left lower eyelid. A small lump is noted on examination which is more obvious when the eyelid is everted. There is no erythema or discharge. A diagnosis of a meibomian cyst is suspected. What is the most appropriate management? |
Advise warm compresses + review in one month |
|
|
A 54-year-old man with type 2 diabetes mellitus is found on annual review to have new vessel formation at the optic disc. Visual acuity in both eyes is not affected (6/9). Blood pressure is155/84 mmHg.
HbA1c 8.4%
What is the most important intervention to preserve vision in this patient? |
Laser therapy |
|
|
A 54-year-old man with type 2 diabetes mellitus is found on annual review to have new vessel formation at the optic disc. Visual acuity in both eyes is not affected (6/9). Blood pressure is155/84 mmHg.
HbA1c 8.4%
What is the most important intervention to preserve vision in this patient? |
Laser therapy
This patient has proliferative diabetic retinopathy and urgent referral to an ophthalmologist for panretinal photocoagulation is indicated. Good glycaemic control is obviously beneficial in the long-term but this patient needs intervention quickly to preserve his vision. |
|
|
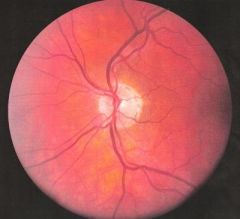
This man presents with unilateral visual loss. On examination he has a relative afferent pupillary defect. Fundoscopy shows the following:
What is the most likely diagnosis? |
Central retinal artery occlusion |
|
|
This man presents with unilateral visual loss. On examination he has a relative afferent pupillary defect. Fundoscopy shows the following:
What is the most likely diagnosis? |
Central retinal artery occlusion
The pale retina is the most obvious sign in this slide. |
|
|
Which one of the following best describes the action of latanoprost in the management of primary open-angle glaucoma? |
Increases uveoscleral outflow |
|
|
Which one of the following is least associated with the development of optic atrophy? |
Ataxic telangiectasia |
|
|
This man presents with unilateral visual loss. On examination he has a relative afferent pupillary defect. Fundoscopy shows the following:
What is the most likely diagnosis? |
Central retinal artery occlusion
The pale retina is the most obvious sign in this slide. |
|
|
Which one of the following best describes the action of latanoprost in the management of primary open-angle glaucoma? |
Increases uveoscleral outflow |
|
|
Which one of the following is least associated with the development of optic atrophy? |
Ataxic telangiectasia |
|
|
Optic atrophy is seen as pale, well demarcated disc on fundoscopy. It is usually bilateral and causes a gradual loss of vision*.
Causes may be acquired or congenital |
True |
|
|
This man presents with unilateral visual loss. On examination he has a relative afferent pupillary defect. Fundoscopy shows the following:
What is the most likely diagnosis? |
Central retinal artery occlusion
The pale retina is the most obvious sign in this slide. |
|
|
Which one of the following best describes the action of latanoprost in the management of primary open-angle glaucoma? |
Increases uveoscleral outflow |
|
|
Which one of the following is least associated with the development of optic atrophy? |
Ataxic telangiectasia |
|
|
Optic atrophy is seen as pale, well demarcated disc on fundoscopy. It is usually bilateral and causes a gradual loss of vision*.
Causes may be acquired or congenital |
True |
|
|
Optic atrophy is seen as pale, well demarcated disc on fundoscopy. It is usually bilateral and causes a gradual loss of vision*. Causes may be acquired or congenital |
Acquired causes multiple sclerosis papilloedema (longstanding) raised intraocular pressure (e.g. glaucoma, tumour) retinal damage (e.g. choroiditis, retinitis pigmentosa) ischaemia toxins: tobacco amblyopia, quinine, methanol, arsenic, lead nutritional: vitamin B1, B2, B6 and B12 deficiency
Congenital causes Friedreich's ataxia mitochondrial disorders e.g. Leber's optic atrophy DIDMOAD - the association of cranial Diabetes Insipidus, Diabetes Mellitus, Optic Atrophy and Deafness (also known as Wolfram's syndrome)
*strictly speaking optic atrophy is a descriptive term, it is the optic neuropathy that results in visual loss |
|
|
A 61-year-old woman presents with bilateral tinnitus. She reports no change in her hearing or other ear-related symptoms. Ear and cranial nerve examination is unremarkable. Which medication is she most likely to have recently started? |
Quinine |
|
|
A 71-year-old man presents with two year history of intermittent problems with swallowing. His wife has also noticed he has halitosis and is coughing at night. He has a past medical history of type 2 diabetes mellitus but states he is otherwise well. Of note his weight is stable and he has a good appetite. Clinical examination is unremarkable. What is the most likely diagnosis? |
Pharyngeal pouch |
|
|
A 61-year-old woman with a history of cardiac problems develops hearing loss after a prolonged admission in hospital. Drug toxicity is suspected. |
The correct answer is Furosemide induced |
|
|
A 71-year-old man presents with two year history of intermittent problems with swallowing. His wife has also noticed he has halitosis and is coughing at night. He has a past medical history of type 2 diabetes mellitus but states he is otherwise well. Of note his weight is stable and he has a good appetite. Clinical examination is unremarkable. What is the most likely diagnosis? |
Pharyngeal pouch |
|
|
A 61-year-old woman with a history of cardiac problems develops hearing loss after a prolonged admission in hospital. Drug toxicity is suspected. |
The correct answer is Furosemide induced |
|
|
A 37-year-old cello player complains of a three month history of vertigo and hearing loss on the left side. On examination he has an absent corneal reflex on the left eye. |
Acoustic neuroma |
|
|
is diagnosed with Bell's palsy. What is the current evidenced base approach to the management of this condition? |
Prednisolone |
|
|
A 42-year-old man with a 3 month history of chronic cough presents with a persistent headache |
Sinusitis
This patient has chronic sinusitis. The cough is secondary to a post-nasal drip |
|
|
does optic neuritis cause SUDDEN PAINLESS LOSS OF VISION |
NO NO |
|
|
what is Ischaemic optic neuropathy |
ischemia to the optic nerve causing damage due to either: - arteritis e.g. GCA aka temporal arteritis or - atherosclerosis in hypertensive, diabetic older patient |