Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
54 Cards in this Set
- Front
- Back
|
1. Adult Polycystic Kidney Disease
2. Autosomal dominant 3. APKD1 on chr. 16 4. HTN, Hematuria, palpable, renal masses, Secondary Polycythemia |
1.What is the diagnosis?
2.What is the inheritance? 3.What is the mutation? 4.What is the clinical presentation? |
|
|
Adult Polycystic Kidney Disease
|
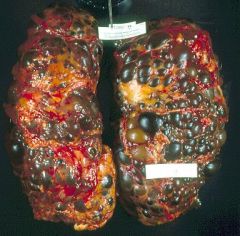
What disease?
|
|
|
Polycystic Kidney Disease
-cysts lined by flattened epithelium that you cannot classify as proximal or distule tubule |
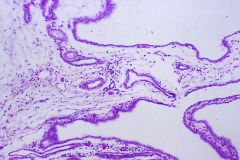
What is this?
|
|
|
A 10-year old boy presents with red tinge to his urine. History reveals that he was diagnosed with mild nerve deafness 2 years earlier and also developed posterior cataracts 1 year ago. Lab studies confirm hematuria as well as the presence of erythrocyte mass.
|
Alport Syndrome
-Nephritis -Nerve deafness -various Eye disorders |
|
|
What is the cause of Alport Syndrome?
|
mutation of alpha-5 chain of Type IV Collagen
|
|
|
What is the typical clinical presentation of Poststreptococcal Glomerulonephritis?
|
1. Pharyngitis 2-3 wks ago
2. Periorbital edema 3. HTN 4. Hematuria *Nephritic Syndrome |
|
|
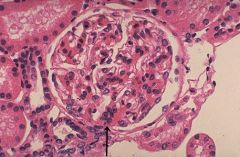
Poststreptococcal Glomerulonephritis = Acute Proliferative Glomerulonephritis
Enlarged, hypercellular, swollen glomeruli with proliferation of mesangial and endothelial cells -Basement membranes are not thickened |
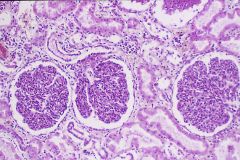
What is this?
How do you know? |
|
|
Post-streptococcaly Glomerulonephritis
Hypercellular -> capillary lumen compression -> GFR decreases -> Blood pressure increases due to Renin secretion -> Angiotensis = constriction of arterioles and Aldosterone secretion = retention of sodium |
What is the cause of this?
What would be a consequence? |
|
|
Post-streptococcal Glomerulonephritis
-Subepithelial deposits of immune-complexes = electron dense HUMPs |
What disease is this?
|
|
|
What is the significance of RBC casts in the urine?
|
Indicates hematuria that is of Renal origin
*differentiates from urinary bladder or pelvis bleeds |
|
|
Crescentic Glomerulonephritis = Rapidly Progressive Glomerulonephritis
|
What is this?
|
|
|
Crescentic Glomerulonephritis = Rapidly Progressive GN
**worst type of GN |
What is this?
|
|
|
Goodpasture Syndrome
-linear pattern |
What disease is this?
|
|
|
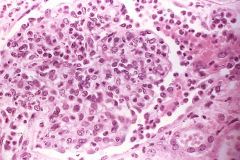
Lupus
Skin, Kidney, Hematopoietic |
What typically would be the diagnosis?
What 3 organ systems are most frequently involved? |
|
|
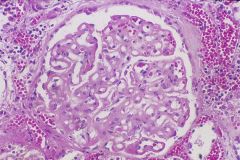
Lupus Nephropathy = Proliferative GN
|
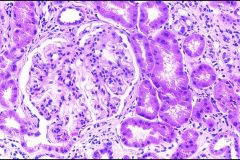
What is this?
|
|
|
Lupus Nephropathy
Wire-loops = thickening of the basement membrane Capillary has thrombi on the inside which are aggregates of immune-complexes that have gelled |
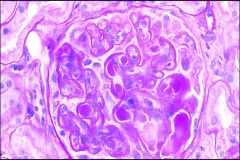
What is this?
How do you know? |
|
|
Lupus Nephropathy
Wire-loops |
What is this?
|
|
|
Lupus Nephropathy
Deposits are everywhere -subendothelial, subepithelial, intramembranous, intramesangial |
What is this?
How do you know? |
|
|
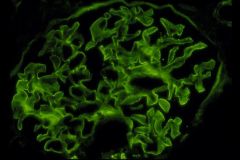
Lupus Nephropathy
staining is everywhere |

What is this?
How do you know? |
|
|
What may Hyaline Casts indicate?
What are Lipid Casts associated with? |
Hyaline = Proteinuria (may also be normal)
Lipid = Hypercholesterolemia = Nephrotic syndrome |
|
|
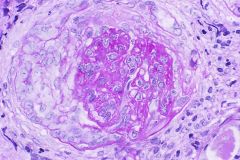
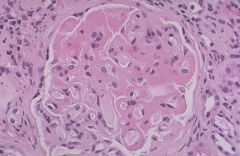
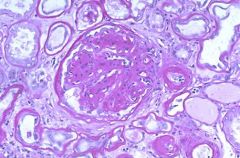
Diabetic Nephropathy with Nodular Sclerosis (Kimmelsteil-Wilson nodules) = nodular accumulations of Mesangial Matrix material
|
What is this?
How do you know? |
|
|
Diabetic Nephropathy with Diffuse Glomerulosclerosis
|
What is this?
|
|
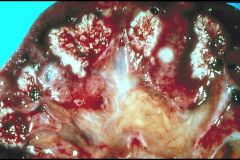
What is seen here?
What will it cause? |
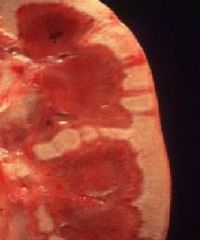
Papillary Necrosis
Piece will slough off and drop into the renal pelvis -> obstruction -> colic of the ureter |
|
|
Papillary Necrosis
1. Diabetes Mellitus 2. Acute Pyelonephritis 3. Chronic Phenacetin (Acetaminophen) 4. Sickle Cell Anemia |
What is seen here?
What 4 things is it associated with? |
|
|
Papillary Necrosis
The pale white areas involving some or all of many renal papillae are areas of papillary necrosis. This is an uncommon but severe complication of acute pyelonephritis, particularly in persons with diabetes mellitus. Papillary necrosis may also accompany analgesic nephropathy |
What is this?
|
|
|
IgA Nephropathy
-Hematuria 1-6 days post-infection **Post-strep GN is 2-3 wks post-infection |
Diagnosis?
Why? |
|
|
IgA Berger Disease
Mesangial widening & hypercellularity = focal proliferative GN with diffuse Mesangial widening |
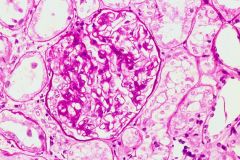
What is this?
How do you know? |
|
|
IgA Nephropathy = Berger Disease
Mesangial deposition of IgA |
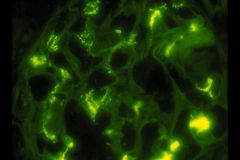
What is this?
How do you know? |
|
|
IgA Nephropathy = Berger Disease
IgA deposits in the mesangium which increases the cellularity |
What is this?
|
|
|
Membranous GN (Nephrotic syndrome)
**thick capillary walls and basement membranes |
What is this?
|
|
|
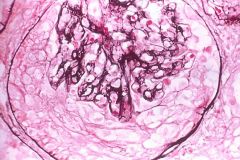
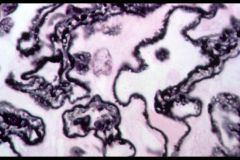
Spike-and-Dome appearance of Membranous Glomerulonephritis on Silver Stain
|
What is this?
|
|
|
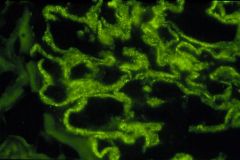
Membranous Glomerulonephritis
Granular pattern of IgG or C3 deposits = Lumpy-bumpy |
What is this?
How do you know? |
|
|
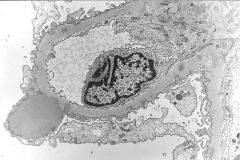
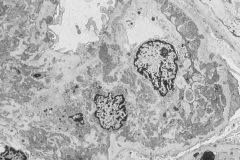
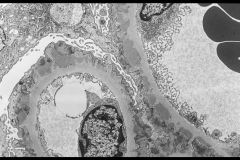
Membranous Glomerulonephritis
-Subepithelial deposition |
This is an EM of what disease?
|
|
|
Acute Pyelonephritis
-WBC casts are indicative |
What is the diagnosis?
|
|
|
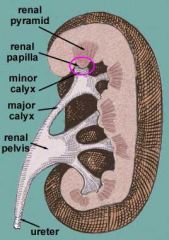
Hydronephrosis = dilation of renal pelvis or calyces
|
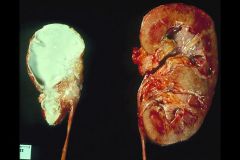
What is shown here?
|
|
|
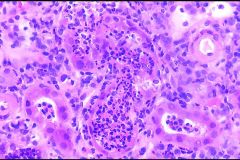
Acute Pyelonephritis
-tubules are destroyed by Neutrophilic infiltration -Glomeruli are spared |
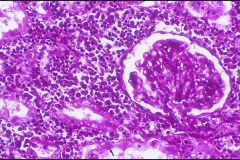
What is this?
|
|
|
Acute Pyelonephritis
Fever and Flank pain with CVA tenderness **CVA = Costovertebral angle |
What is shown here?
How would the patient present clinically? |
|
|
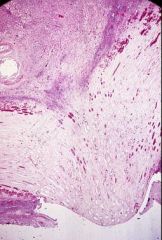
Chronic Pyelonephritis
Corticomedullary Scarring |

What is this?
How do you know? |
|
|
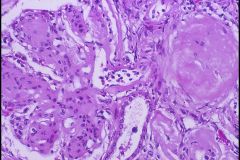
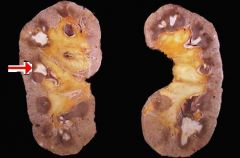
Benign Nephrosclerosis
The smaller arteries in the kidney have become thickened and narrowed. Hyaline arteriolosclerosis with hypertension or diabetes mellitus is usually present. This leads to patchy ischemic atrophy with focal loss of parenchyma that gives the surface of the kidney the characteristic granular appearance as seen here Most common renal disease associated with hypertension |

What is this?
|
|
|
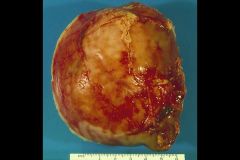
Renal Cell Carcinoma
|
Diagnosis?
|
|
|
Renal Cell carcinoma
|
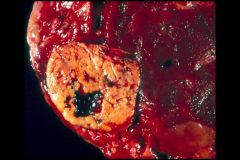
What is this?
|
|
|
Renal Cell Carcinoma
Polygonal Clear Cells arising from Tubular epithelium |
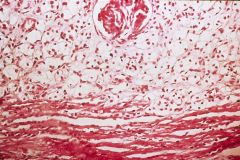
What is this?
|
|
|
Renal Cell Carcinoma has invades the Renal Vein and IVC
|

Describe this picture
|
|
|
WAGR complex
-Wilms tumor -Aniridia = absence of iris -GU malformation -Mental-motor Retardation |
Discuss this case
|
|
|
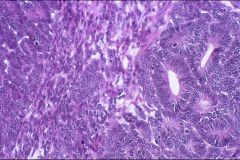
Wilms tumor
|
What is this?
|
|
|
Wilms tumor
|

What is this?
|
|
|
Wilms tumor
-immature fetal-like cells = Primitive Mesenchyme |
What is this?
|
|
|
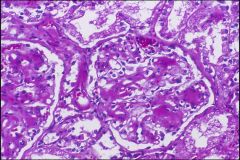
Diffuse Glomerulosclerosis in Diabetic Nephropathy
There is an increase in mesangial matrix, a slight increase in mesangial cellularity, and capillary basement membrane thickening. These changes gradually advance until the entire glomerulus is sclerotic. |
What is seen here?
|
|
|
Most common renal disease in Essential HTN
Sclerosis of arterioles and intrarenal arteries |
Nephrosclerosis
|
|
|
Chronic use of Acetaminophen plus Aspirin for 3 or more years
|
Analgesic Nephropathy
*Acetaminophen --> free radicals damage renal tubules in medulla *Aspirin -> inhibits renal synthesis of PGE2 leaving Angiotensin II unopposed = decreased blood flow to renal medulla |
|
|
Drug that commonly causes Acute drug-induced interstitial nephritis
|
Penicillin derivatives --> Methicillin
|
|
|
What is the cause of Bilateral Cortical Necrosis (Diffuse Cortical Necrosis)?
|
Complication of an Obstetric emergency
-preeclampsia or abruption placentae **due to DIC limited to the renal cortex -fibrin clots in arterioles and glomerular capillaries -bilateral, diffuse, pale infarct of the renal cortex |
|
|
A childhood kidney disease in which there is progressive symmetrical destruction of the kidneys involving both the tubules and glomeruli, characteristically resulting in anemia, polyuria, polydipsia, isosthenuria (decreased ability to concentrate the urine), progressive renal failure and death in uremia. Hypertension and proteinuria are conspicuous by their absence. The chronic kidney failure affects growth and leads to short stature. The age at death ranges from around 4 to 15 years.
|
Nephronophthisis
|
|
|
Fever and skin rash develop in a 32-year-old man. Several days later, he has rising serum levels of urea nitrogen and creatinine along with oligouria. Urinalysis reveals proteinuria, hematuria, no glucose, no ketones, and no nitrite. The leukocyte esterase result is positive. Urine microscopic examination shows RBC's and WBC's, some of which are Eosinophils.
|
Drug ingestion --> Drug-induced Interstitial Nephritis
|