Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
60 Cards in this Set
- Front
- Back
|
Discuss VALVULAR DISEASE in general:
|
*Congenital or acquired disorders
*Variable amount of dysfunction *Stenosis: Failure of valve to open completely with resultant obstruction of forward flow. *Insufficiency: Failure of valve to close completely with reverse flow. *Two thirds of all valvular lesions are acquired lesions of the mitral or aortic valves. |
|
|
Most Frequent Valvular Lesions:
|
*Mitral stenosis (MS) – RHD (rheumatic).
*Mitral insufficiency (MI) – MV prolapse (floppy valve).*** *Aortic stenosis (AS) – calcification.*** *Aortic insufficiency (AI) – dilated aortic root, most commonly due to hypertension and/or aging. ***most common |
|
|
Discuss Calcification in valvular disease:
|
*Calcium deposited in areas of wear and tear.
*Most frequent valve abnormality: aortic valve and/or mitral annulus. *Bicuspid AV especially prone. *Lesions also show lipid deposition and resemble atherosclerosis. |
|
|
Discuss Calcific Aortic Stenosis:
risk factors? |
*Most common cause – aging.
*RHD as cause now less common. *Congenitally BICUSPID AV is one of the most common associated anomalies.* *It is prone to calcification and SBE. *Bicuspid AV associated with CoA (coarctation of aorta), dilated aortic root, and aortic dissection. *Only in RHD is there likely disease of the MV when AS present. |
|

|

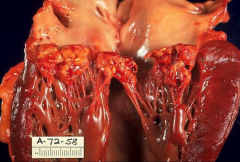
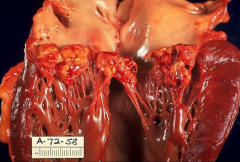
*Tricuspid Aortic Valve with Calcification
*"sinuses of Valsalva. *commissures are free; so that indicates this isn't rhematic valvular disease. |
|
|
*Bicuspid Aortic Valve with Calcification
*Raphe is visible (paritally formed third cusp). |
|
|
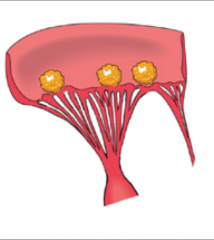
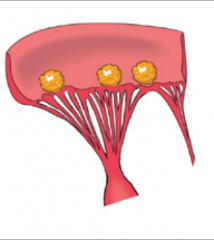
Discuss Mitral Annular Calcification:
|
*Often continuous with calcium deposits in the AV valve cusps.
*Appear as hard, ulcerated nodules. *Often no impairment of valve function but can be MI or MS. *Calcification can extend into skeleton and even into conduction system! |
|
|
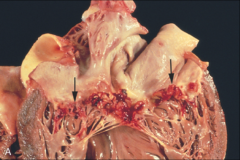
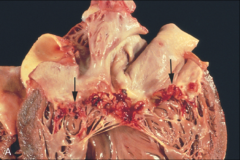
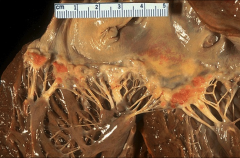
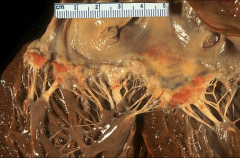
*Mitral Annular Calcification
*Deposits are Ca, lipid, and some inflammatory cells. |
|
|
*Mitral annular calcification
*Yellow grainy spot in middle is the calcification. |
|
|
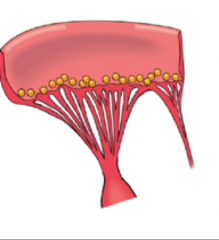
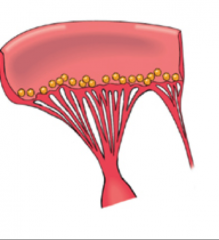
Discuss Mitral Valve Prolapse:
|
*Myxomatous ("mucoidy") degeneration. NOT rheumatic in origin.
*Leaflet(s) large, hooded, floppy. *Serious complications include IE (endocarditis), MR (regurgitation), emboli, arrhythmias. Most patients don't get these complications. *Leaflets thick and rubbery; chordae elongated; annulus dilated. *Lamina fibrosa thin; spongiosa thick with myxoid deposits. |
|
|
Causes of MVP?
|
*Causes include hereditary disorders of connective tissue such as MARFAN syndrome, a disorder secondary to MISSENSE mutations in the fibrillin gene. It's a small subset of these patients.
*Can also be secondary to degenerative changes in myofibroblasts in response to abnormal hemodynamic forces such as chronic regurgitation. |
|
|
What molecules are more abundant in MVP?
What molecules are decreased? |
**HE SKIPPED THIS SLIDE**
*Proteoglycans decorin, biglycan, and versican are more abundant in myxomatous valves. *Expression of the hyaluronan receptor for endocytosis is decreased. |
|
|
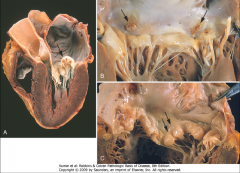
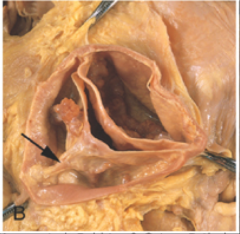
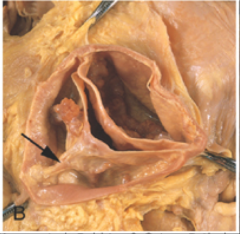
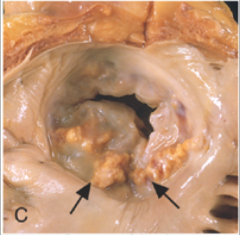
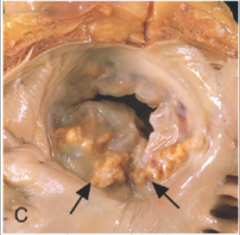
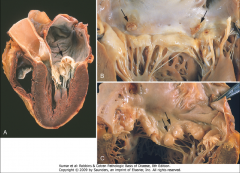
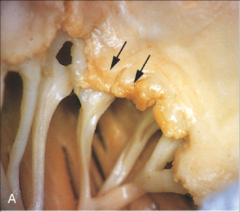
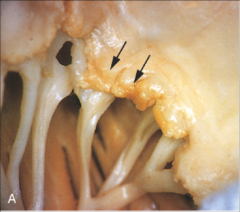
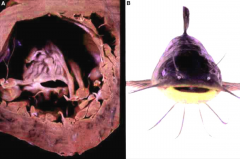
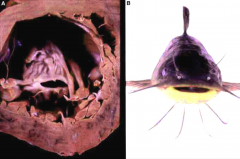
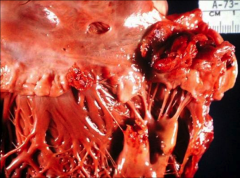
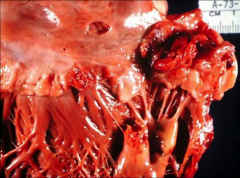
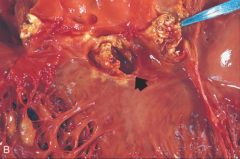
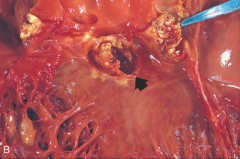
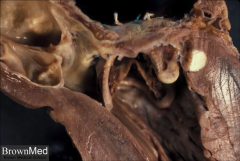
A. Arrow indicates prolapse of MV leaflet into left atrium, which is dilated.
B. Arrows indicate thrombotic plaques at sites of leaflet-atrium contact. Chordee tendinae are really thin. Fibrin deposition visible (gray-ish). C. Double arrows indicate "hooding" of MV leaflets; arrow head shows calcification of the annulus. |
|

|

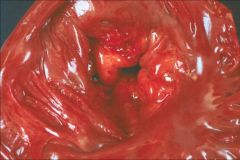
Mitral Valve Prolapse (fixed tissue)
*Hooding is visible. *Thin chordee tendinae, they can eventually rupture. |
|
|
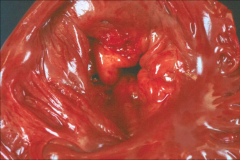
*MITRAL VALVE PROLAPSE VIEWED FROM LEFT ATRIUM.
*Lumen of valve is visible; valve is pouching into LA. |
|

|
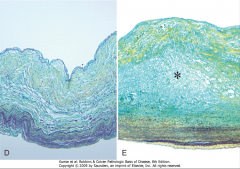
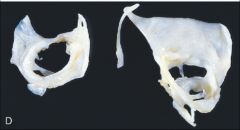
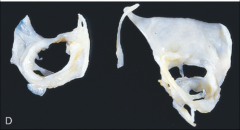
D. Normal valve (luminal layer-fibrosa; middle-spongiosa; outer-continous with chamber).
E. Myxomatous degeneration of mitral valve. *Pentachrome stain shows abundant proteoglycan deposition (asterisk) in myxomatous area, which is stained blue. |
|
|
Discuss Rheumatic Fever and RHD:
|
*Immunologically mediated.
*Presents a few weeks after group A ß-hemolytic strep infection, usually pharyngeal. *Acute RHD (rare) can be fatal but main problem is due to chronic RHD (progression to valvular dysfunction). *Deforming fibrosis of *AV and/or MV* may not present clinically until YEARS later. |
|
|
Probable Pathogenesis of RHD:
|
*Hypersensitivity reaction induced by group A strep.
*Hypothesis – antibodies against M proteins of streptococci cross-react with glycoproteins in heart and other organs. |
|
|
Evidence for M protein theory of RHD:
|
*Hyaluronate in streptococcal wall and human connective tissue is identical.
*Antibodies against streptococci react with sarcolemma. *Streptococcal M protein shares epitopes with cardiac myosin. |
|
|
Autoimmunity Hypothesis of RHD:
|
*Alternative theory.
*Strep M protein a super antigen which activates human T cells expressing genes in the context of class II. *Susceptibility likely controlled by immune response genes – HLA. *Helper T cells expressing class II comprise most of cellular infiltrate in valvular lesions. |
|
|
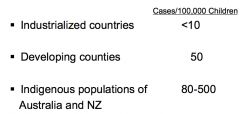
EPIDEMIOLOGY of RHD:
|
|
|
|
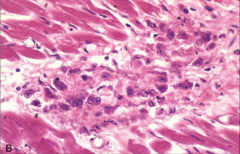
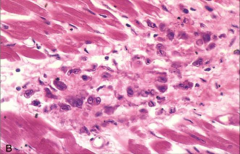
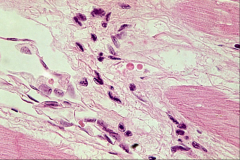
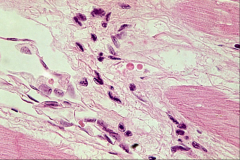
*ASCHOFF BODY in RHD; CLASSIC for RHD.
*FIBRINOID necrosis with lymphocytes, plasma cells, macrophages, giant cells, variable numbers of neutrophils and Anitschkow cells. |
|
|
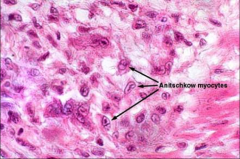
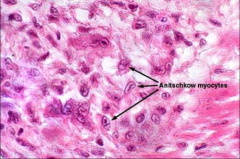
*ANITSCHKOW CELLS
*Large macrophages with abundant amphophilic cytoplasm and clumped nuclear chromatin which forms a central irregular ribbon resembling a caterpillar. |
|
|
*ANITSCHKOW CELLS
*Anitschkow cells are often considered pathognomonic for RHD but these are from a 25 year old woman without RHD. |
|
|
RHD Pathology - what do you see in the Endocardium?
|
*Endocarditis – foci of fibrinoid necrosis in cusps or leaflets, usually AV or MV.
*These foci may extend onto chordae tendineae, making them THICK. *Verrucae (vegetations) along lines of closure of the valves. *Chronically – you see fibrosis of valve with thick, stiff cusps and/or leaflets. *Chordae retract, thicken, and fuse. |
|
|
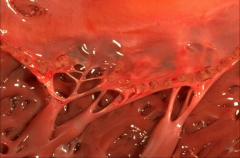
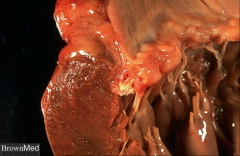
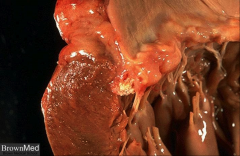
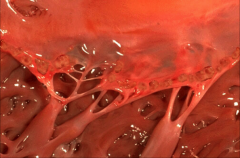
*Acute Rheumatic Endocarditis of MV.
*Note verrucae along edges of valve. *Really rare. |
|
|
*Acute Rheumatic Valvulitis Superimposed on Chronic Mitral Valvulitis
*Thickened leaflets and thick chordee indicate chronic nature of this RHD. |
|
|
*Acute Rheumatic Endocarditis
*With verrucae along lines of closure |
|

|

*Chronic RHD.
*Mitral Stenosis with Diffuse Fibrous Thickening and Commissural Fusion at edges. You would NOT see this fusion in other valvular issues. *LA opened, looking down into valve. |
|
|
*LV looking up to MV.
*“Fishmouth valve” Slit-like lumen of valve showing fibrosis and retraction. |
|

|

*RHD – Mitral Stenosis
*Thickened cusps and chordee give away the fact that this is from RHD. |
|
|
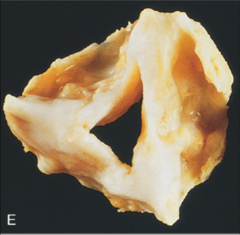
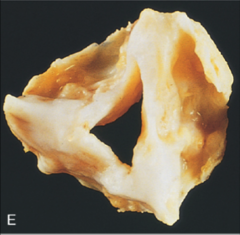
*Healed Rheumatic Aortic Stenosis with Commissural Fusion.
*An extremely distorted AV. Calcified, fibrotic, fused. *Fusion distinguishes this from calcific aortic stenosis! |
|
|
Discuss Acute Infective (Bacterial) Endocarditis:
|
*Due to highly virulent organisms, e.g. Staphylococcus aureus.
*Acute BE can affect previously NORMAL valves. *Risk of septic (bug-containing) emboli. *Risk of perforation of cusp or leaflet with acute regurgitation. |
|
|
What is Infective Endocarditis?
|
*Colonization with or without invasion of the endocardium, not always on a valve.
*Often destruction of underlying tissue. *Vegetations consist of the offending agent and thrombotic debris. *Vegetations may set up on prostheses. *May be associated with infective arteritis. Steps: 1) Injured endothelium 2) Fibrin/platelet adhesion 3) Bacterial vegetation of adhesion |
|
|
*Acute Bacterial Endocarditis with Larger Fungating Lesions.
*Huge vegetation. |
|
|
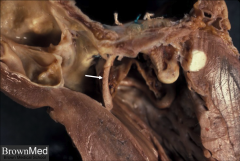
*Acute Endocarditis of Congenital Bicuspid Aortic Valve (S. aureus...he says bicuspid AV is "probably" more likely to get infected).
*Cusps are pretty much destroyed. Arrow indicates beginning of a ring abscess forming. |
|
|
Discuss Subacute Bacterial Endocarditis (SBE):
|
*Organisms of lesser virulence (strep viridans) at sites of endothelial injury, e.g. PREVIOUSLY DEFORMED valves or impact of high velocity flow.
*May smolder and present after months. *Risk of septic emboli. *Less destruction of underlying tissue than in acute BE. *Evidence of HEALING. **GUSTAV MAHLER HAD STREP VIRIDANS SBE**HISTORY LOL |
|
|
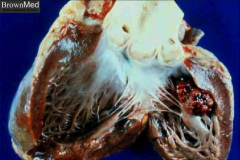
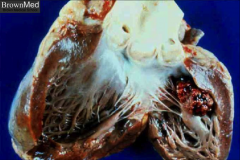
*SUBACUTE BACTERIAL ENDOCARDITIS OF MITRAL VALVE
*Can't tell this is subacute just by the pic. Lots of vegetations visible. |
|
|
*Subacute Endocarditis Mitral Valve (S. viridans)
*Can't tell subacute just by looking grossly. |
|
|
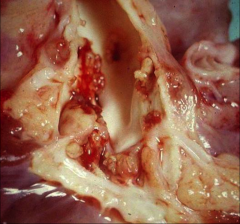
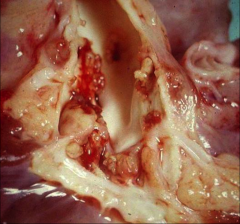
*SUBACUTE BACTERIAL ENDOCARDITIS (AORTIC VALVE).
|
|
|
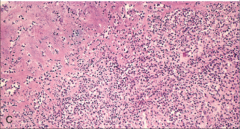
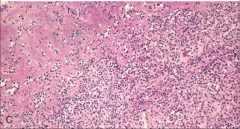
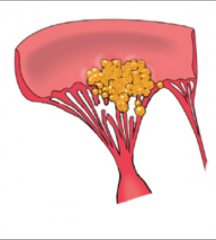
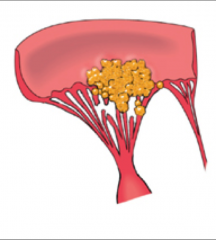
*Infective Endocarditis
*pink = firbin *blue = WBCs |
|

|

*SBE – Aortic Valve
*S. Viridans produced a large, crumbling lesion on an aortic cusp scarred by RHD. *A layer of platelets and fibrin is covered by a layer of mononuclear cells. *A granular mass of S. viridans is enclosed centrally. *Blue lymphoid looking tiny dots = bacteria |
|
|
*Endocarditis due to Candida (you can't tell)
*Point is, you can get IE from lots of things. *Immunosuppressed patient with a huge vegetation. |
|
|
*Infective Endocarditis
*Yellow = large vegetation with destruction of chordae. |
|
|
Complications of IE:
|
*Valvular stenosis or insufficiency
*Abscess in annulus or myocardium *Suppurative pericarditis *Paravalvular leak (prosthesis) *Emboli *Focal and diffuse glomerulonephritis due to antigen-antibody complexes. |
|
|
*Healed Endocarditis of Mitral Valve.
*Valve is distorted. *You can see past perforation of the valve on the right. |
|
|
Discuss Nonbacterial Thrombotic (MARANTIC) Endocarditis (NBTE):
|
*Occurs in debilitated patients.
*Deposition of small noninfected, loosely attached masses of fibrin, platelets, and other blood components on valves. *Often associated with hypercoagulable state, as in mucinous adenocarcinoma. *Histology – bland thrombi; no inflammation or valve damage. |
|

|

*Nonbacterial Thrombotic (marantic) Endocarditis of Mitral Valve.
*Looking along the lines of closure of the MV. *Arrows = verrucae *µscopic view shows fibrin, lymphocytes, inflammatory cells. |
|
|
*NBTE – Mitral Valve
*Vegetations along line of closure *Thrombus adherent to intact leaflet |
|
|
*Nonbacterial Thrombotic (Marantic) Endocarditis
*Note pattern of vegetations. |
|
|
Discuss Libman-Sacks Endocarditis:
|
*Seen only in SLE!
*Small verrucae. *Necrotic vascular tissue and fibrin with macrophages, lymphocytes, and PCs. *May be intense inflammation in underlying tissue. *Mitral Valve most often affected. ***LIBMAN WAS MAHLER'S DOCTOR*** HISTORY!!!!!!111 |
|

|

*Libman-Sacks Endocarditis
*Distribution of vegetations is key to identifying the different endocarditis's on the boards. |
|
|
*LIBMAN-SACKS ENDOCARDITIS
*Note vegetative pattern along lines of closure. |
|
|
Discuss endocarditis in Carcinoid Syndrome:
|
*Fibrous PLAQUE-LIKE endocardial thickening on walls of chambers or valves.
*Lesions usually on RIGHT SIDE of heart. *Lesions composed of smooth muscle and collagen in a mucopolysaccharide matrix. *Carcinoid tumors secrete SEROTONIN. *Lesions correlate with plasma levels of 5-HT. *Lesions on left side if carcinoid tumors are in lung. |
|

|

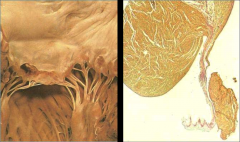
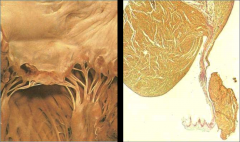
L: Endocardial Fibrosis and thickening of Right Ventricle and Tricuspid Valve (Carcinoid syndrome).
R: Movat Stain with Acid Mucopolysaccharide Areas Stained Blue; lots of MPS deposition. |
|
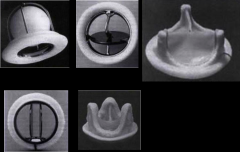
Discuss Prosthetic Heart Valves:
|
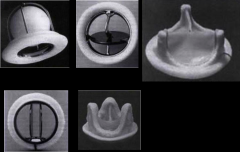
*Mechanical
-Non-physiological biomaterials with caged balls, tilting discs, or hinged semicircular flaps *Tissue (Bioprosthetic) -Chemically-treated animal tissue mounted on a frame Top left: ball and cage valve top middle: disc valve bottom left: bileaflet valve other two are porcine. |
|
|
Complications from prosthetic valves:
|
*Thromboembolism
*Structural deterioration *Overgrowth of fibrous tissue *Hemolysis due to shearing forces *Improper placement or disproportionate size *Prosthetic valve endocarditis |
|
|
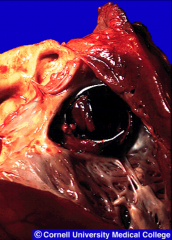
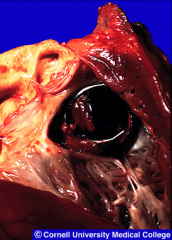
*Thrombosed pivoting disc, Valve prosthesis. This killed the patient.
|
|
|
*Prosthetic mitral valve with a strut (arrow) causing partial obstruction of the left ventricular outflow tract
|
|

|
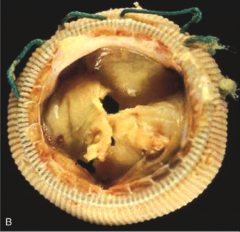
*Calcification and Tear of Prosthetic Porcine Valve.
*Analogous to calcific aortic stenosis. |