![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
75 Cards in this Set
- Front
- Back

|
Rickets |
|

|
Langerhans cell histiocytosis |
|
|
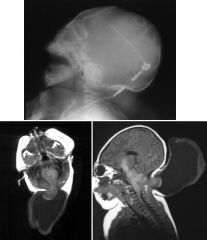
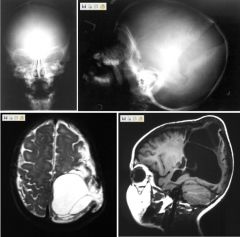
Encephalocele
Case findings: Small posterior fossa with herniation of the cerebellar vermis and brainstem through the foramen magnum Cerebellar tissue herniates through a spina bifida defect posteriorly into a large CSF sac T1 weighted axial images: craniospinal defect and meningoenecephalocele Encephalocele: developmental abnormality in which part of the CNS herniates through a cranial defect, MC occipital (80%) Meningocele: containing only CSF and meninges Meningoencephalocele: neural tissue and meninges Hydroencephalomeningocele: neural tissue, meninges, and ventricle DDX: cystic hygroma Associated with: Meckel-Gruber syndrome: occipital encephalocele, bilateral MCDK, polydactyly Chiari III: Chiari II, encephalocele Klippel Feil anomaly Walker Warburg syndrome: occipital encephalocele, eye malformation, lissencephaly, cerebellar dysgenesis |
|
|
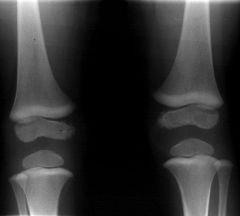
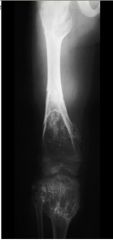
Lead Poisoning
Case findings: Broad transverse bands of increased density representing lead deposits in the metaphyses of long bones Affects both tibia AND fibula, or radius AND ulna In contrast, growth arrest lines should NOT affect all long bones DDX dense metaphyseal lines MC is exuberant calcification of the zone of provisional calcification (normal variant) Growth recovery lines (of Park or Harris) Heavy metal poisoning (lead): affects fibula and ulna in addition to tibia and radius Healing stages of leukemia and rickets Scurvy: vitamin C deficiency Both radiodense (white line of Frankel) and radiolucent lines (Trummerfeld zone) DDx Dense Lines LINES Lead poisoning Infantile growth arrest Normal, 3 yr LEukemia treated Syphillis/Scurvey DDX Lucent Lines “NORMAL TENDER LOVING CARE” Normal (neonates) TORCH Leukemia Chronic illness |
|
|

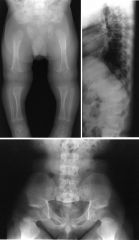
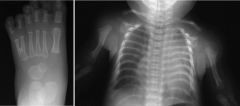
Achondroplasia
Skull: Narrow foramen magnum, small posterior fossa Spine: Narrow spinal canal with spinal canal stenosis Narrowing of the interpedicular distances in the lumbar region Bullet shaped vertebral bodies early, which progress to short flat vertebral bodies Posterior scalloping of vertebral bodies Pelvis: Square iliac wings, horizontal acetabular roofs, narrow sciatic notches Champagne appearance of the pelvis Long tubular bones: Shortening, particularly of femora and humeri rhizomelically Metaphyses slant obliquely upwards and outwards in the lower femora Hands and feet: Short, stubby trident metacarpals and metatarsals MC nonlethal skeletal dysplasia AD, rhizomelic dwarf Large head with prominent forehead (frontal bossing), trident hands, gibbus deformity in the thoracolumbar region, normal mentalation Clinical complications: Hydrocephalus due to obstructed venous return and narrow skull base Symptoms of spinal canal stenosis secondary to narrow spinal canal |
|
Case 6History: newborn with cough since birth and 3 week h/o wheeze
|
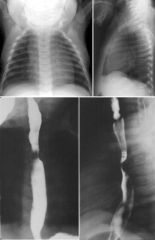
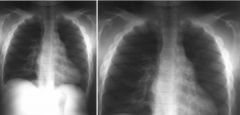
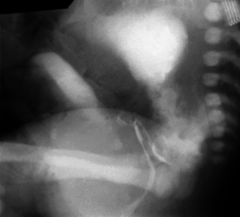
Vascular ring
Diagnosis: vascular ring formed by right aortic arch with aberrant left subclavian artery Posterior esophageal impression is MC with aberrant RSA with a left-sided aortic arch, and LC by an aberrant LSA with a right-sided aortic arch Other vascular impressions: Anterior tracheal impression: from innominate artery arising to the left of the trachea and ascending anteriorly normal finding unless accompanied by symptoms Impression between the esophagus and trachea (excluding lymph nodes and the rare bronchogenic cyst) is pathognomonic of an aberrant left pulmonary artery (pulmonary sling) CHD associated with findings of right aortic arch and aberrant LSA: MC Tetralogy of Fallot (71% ) ASD or VSD (21%) Coarctation of the aorta (7%) True vascular ring: MC double aortic arch (mirror-image arch) Right aortic arch combined with aberrant LSA (this case) Ring is completed by ductus remnant |
|

12 year old girl with recurrent left lower lobe pneumonias
|
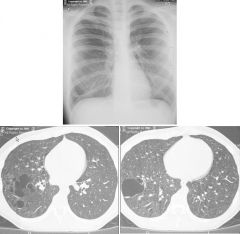
Intralobar pulmonary sequestration
Case findings: CT shows multiple dilated abnormal blood vessels in LLL, area supplied by artery arising from aorta (red arrow) and drainage is to the left inferior pulmonary vein (blue arrow) Congenital anomaly of bronchopulmonary foregut with nonfunctional segment of lung Blood supply is anomalous, arising from the systemic circulation (aorta or bronchial arteries) No typical communication with the bronchial tree or with the pulmonary arteries DDX: Sequestration CCAM Bronchiectasis Tuberculosis Treatment: surgical resection Pulmonary sequestration Both types derive blood supply from systemic arterial circulation Type is based on venous drainage Intralobar: drains to pulmonary veins or left atrium Nonfunctioning portion of lung WITHIN visceral pleura of a pulmonary lobe Manifest during adolescence or adulthood 3X MC with male predominance, LC to have associated anomalies Extralobar: drains to systemic venous system (IVC or azygous) Lung tissue contained in its own pleura Systemic arterial AND venous connection: results in L to R shunt Present at birth with cyanosis, respiratory distress, feeding difficulties, failure to thrive, and recurrent pneumonias Associated anomalies in up to 65% of patients: diaphragmatic defects, pulmonary hypoplasia, bronchogenic cysts, cardiac anomalies |
|
|
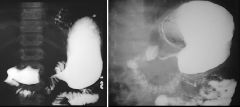
Hypertrophic pyloric stenosis
DDX: Hypertrophic pyloric stenosis Single wall thickness < 3 mm normal Pyloric length < 17 mm normal Infantile Pylorospasm: Wall thickness 1.5-3 mm with partial outlet obstruction and only delayed gastric emptying MC acquired cause of GI obstruction in infant Idiopathic hypertrophy and hyperplasia of the circular muscle fibers of pylorus with extension into gastric antrum Increased incidence in firstborn males Clinical: Presents around 4-6 weeks with non-bilious intractable projectile vomiting Palpable olive-shaped mass is present in RUQ Treatment: pyloromyotomy Cervix sign: indentation of pyloric muscle into the fluid-filled antrum Double track sign: parallel hypoechoic muscle layers with double adjacent echogenic mucosal layers internally Single wall thickness > 3mm, pyloric canal length > 17mm Exaggerated peristaltic waves in the gastric antrum (with little to no fluid passage through the closed outlet) Shouldering or flattening of the pre-pyloric antrum over the hypertrophic pylorus Transverse imaging may demonstrate the target sign (hypoechoic ring of pyloric muscle around the echogenic mucosa) and a transverse pyloric diameter > 13mm when closed |
|

|
Osteogenesis imperfecta
Case findings: Diffuse osteoporosis Bowing deformities Healing fractures Etiology: Impairment of early stages in synthesis of connective tissue fibers Faulty cross-linking of resultant fibers into adult type I collagen Types: I: tarda (Van der Hoeve disease) II: congenita, lethal (Vrolik disease) III, IV (rare) |
|

|
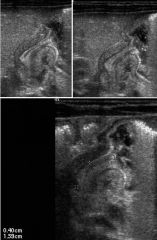
Lenticulostriate vasculopathy (LSV)
Case findings: Linear or branched-linear foci of echogenicity follow course of lenticulostriate branches of the MCA Vessels supplying the basal ganglia normally cannot be seen LSV nonspecific finding: previous insult to developing brain Associated with: TORCH infection Fetal alcohol syndrome Trisomy 21, 18 Non-immune hydrops fetalis |
|

|
Omphalocele
Case findings: Soft tissue mass with herniation of small and large bowel within the mass Multiple segmentation anomalies including hemivertebrae, butterfly vertebrae and rib anomalies Ribs are widely spaced and appear hypoplastic Diastasis of the symphysis pubis: history of bladder exstrophy Failure of return of the intestine to abdominal cavity during intrauterine life (10th week) Midline abdominal wall defect Abdominal organs may herniate into the defect covered by peritoneal and amnion sac Umbilical cord inserts into the apex of the abdominal wall defect Associated anomalies: MC cardiovascular system Complications: malrotation, volvulus Gastrochisis Paraumbilical herniation Normal umbilical cord insertion Lack of covering sac No associated anomalies |
|
|
Leptomeningeal cyst
Case findings: Left diastatic skull fracture with leptomeningeal cyst Skull fractures are associated with tears of the underlying dura, herniation of meninges and brain tissue Interposition of tissue prevents osteoblast from migrating, inhibiting fracture healing CSF pulsation actually results in enlargement of the fracture, with extension of the meninges extracranially results in a growing fracture or leptomeningeal cyst |
|

|
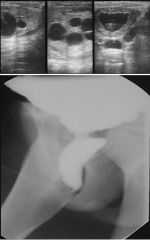
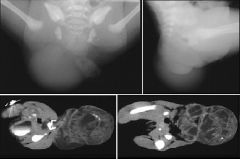
2nd Branchial cleft cyst
Case findings: Well defined, low density unilocular mass with a thin uniformly enhancing rim MC anterior to sternocleidomastoid muscle and lateral to thyroid gland 90% of branchial abnormalities arise from the 2nd branchial cleft DDX neck mass Cystic hygroma: MC in posterior triangle, multilocular septate cyst Branchial cleft cyst: MC anterior to the SCM and lateral to thyroid gland, 90% of branchial abnormalities arise from 2nd branchial cleft Dermoid: midline lesion Hemangioma (capillary): echogenic, minimal if any flow is seen on doppler Neurogenic tumor: MC primary neoplasm of the neck in childhood 90% are neuroblastoma, ganglioneuroblastomas or ganglioneuromas 10% neurofibroma Paraspinal location Lymphoma or rhabdomyosarcoma: produce enlarged nodes with increased doppler signal |
|
|

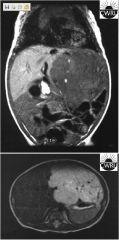
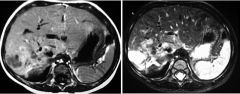
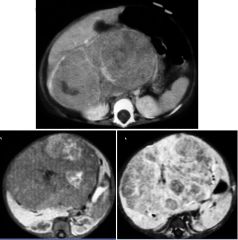
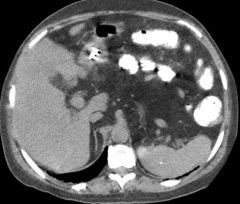
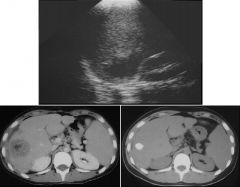
Infantile hemangioendothelioma
Case findings: Axial T2: well circumscribed mass in left lobe with slightly heterogenous, but increased SI. Numerous, prominent flow voids within the mass Coronal T1: large, slightly nodular, well circumscribed mass within the left lobe of the liver, mass is slightly heterogenous, but decreased SI with several punctate regions of increased signal intensity, suggestive of focal areas of hemorrhage Classic: change in caliber of aorta below celiac artery Presents between 1-6 months of age Clinical: abdominal mass or hepatomegaly, CHF Natural history of IHE: Proliferative phase: rapid growth during first 6 months of life Followed by spontaneous regression over next several months Kasabach-Merritt: thrombocytopenia and anemia from consumptive coagulopathy Prednisone: accelerate regression of the lesion Liver transplantation is an option in cases with diffuse tumor involvement or uncontrollable CHF DDX for IHE Hepatoblastoma Rarely seen < 1 year-old. , AFP markedly elevated (AFP normal in IHE) CT: more heterogenous than IHE, especially after contrast administration Mesenchymal hamartoma MC in infant and are NOT associated with elevated AFP Multilocular cystic masses, rarely as a solid lesion When solid, mesenchymal hamartomas are avascular or hypovascular masses on angiography, scintigraphy, and Doppler ultrasound Metastatic neuroblastoma May be confused with the multicentric form of IHE Urinary catecholamines are elevated Enhancing areas represent normal residual liver May see calcifications Infantile hemangioendothelioma US: focal, well-circumscribed hepatic mass containing multiple sonolucent areas with central echogenicity Multiple sonolucent areas with central echogenicity due to enlarged vascular channels Large feeding vessels and a marked decrease in the caliber of the aorta below the celiac axis |
|

|
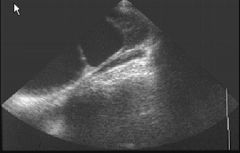
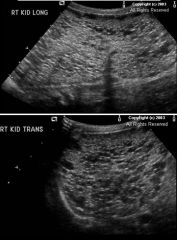
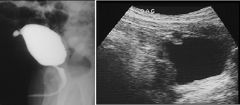
UPJ obstruction
Case findings: LK demonstrates multiple large communicating cysts Renal parenchyma is thinned hydronephrosis Hydronephrosis: MC cause is UPJ obstruction Etiology: Intrinsic: abnormal musculature Extrinsic compression: by either an aberrant vessel (inferior renal vein), a fibrous band, or inflammatory kinks Grade IV or grade V VUR can simulate UPJ (perform VCUG) DDX: Primary megaureter Ectopic ureterocele |
|

|
Duplicated collecting system
Case findings: Two separate central sinus echoes Partial duplication of left collecting system Spectrum: bifid renal pelvis to complete duplication of the ureter and kidney to the level of bladder Weigert-Meyer rule: Drooping lily sign Lower pole moiety: orthotopic insertion of ureter, predispose to VUR Upper pole moiety Ureter inserts heterotopically, medial and caudal to normal ureteric orifice More prone to obstruction secondary to a ureterocele Upper pole moiety may insert ectopically into the uterus, vagina, epididymis or urethra, causing bed wetting or dribbling or urine Grading of hydronephrosis Grading Reflux into the distal ureters Reflux into collecting system without calyceal dilatation/blunting All of the above plus mild dilatation of pelvis and calices All of the above plus moderate dilatation with clubbing of calices All of the above plus severe tortuousity of the ureter Grades I-III resolve with maturation of ureterovesical junction Grades IV and V require surgery to prevent further renal impairment, renal scarring, and hypertension |
|
|

Hunter’s syndrome
Case findings: Broad ribs which taper posteriorly Clavicles are short and broad Dysostosis multiplex: pattern of skeletal abnormalities in mucopolysaccharadoses Skeletal manifestations of Hunter’s syndrome are moderate in severity while those of Hurler’s and Morquio’s syndromes tend to be more severe Dysostosis multiplex Skull: dolichocephaly, underdevelopment of paranasal sinuses and mastoid air cells, J-shaped sella turcica Spine: gibbus deformity at thoracolumbar junction Chest: oar-shaped or paddle-shaped ribs (broad with taperingposteriorly), clavicles which are broad and short, small scapulae Pelvis: increased acetabular angles, coxa valga, delayed and dysplastic femoral head development Long bones: diaphyseal and metaphyseal expansion, delayed ossification centers, cortical thinning (UE > LE) Hands: short and wide phalanges which taper distally (bullet shaped) Hunter’s syndrome Poorly modeled metacarpal bones with expansion of medullary cavities, pointed bases to the metacarpals Thickening of skull vault and J-shaped sella |
|

|

Apert’s syndrome
Case findings: Syndactyly involving fusion of the third and fourth middle phalanges Irregular fusion of distal phalanges (mitten hand deformity) One of the acrocephalosyndactyly syndromes Apert type: craniosynostosis (MC brachycephaly, turricephaly), syndactyly (mitten hands) Craniosynostosis syndactyly (acrocephalosyndactyly) Apert type: craniosynostosis (MC brachycephaly, turricephaly), syndactyly (mitten hands) Carpenter syndrome: craniosynostosis, polydactyly (both brachydactyly and syndactyly with preaxial polydactyly) Pfeiffer's syndrome: stenosis of sagittal and coronal sutures, mild digital ST syndactyly Crouzon’s syndrome (craniofacial dysostosis): NOT part of acrocephalosyndactyly syndromes due to lack of involvement of the hands and feet Brachycephaly (premature closure of coronal/lamboid suture lines), hypoplastic mandible |
|

|
Desmoid fibromatosis
Case findings: Soft tissue mass is seen on plantar aspect AP view: mixed lytic and sclerotic lesions of the 2nd and 3rd metatarsal diaphysis Fibromatosis: category of several entities with various amounts of myofibroblasts and collagen Desmoid tumor: Benign, but has insidious infiltration of the surrounding tissues, especially when located in extra-abdominal sites Extensive infiltration surrounding tissues makes complete resection impossible Recurrence common Types: extra-abdominal fibromatosis, abdominal fibromatosis Fibromatosis types Palmar and plantar fibromatosis Peyronie's disease (penile fibromatosis) Fibromatosis coli (sternocleidomastoid muscle) Intra-abdominal fibromatosis includes: Pelvic fibromatosis Mesenteric fibromatosis Gardner's syndrome Gardner Syndrome Best diagnostic clue: Innumerable, colonic, radiolucent filling defects with extraintestinal lesions Other general features Combination of familial polyposis coli (Colonic adenomatous polyps) and Osteomas; dental abnormalities Desmoid tumor & mesenteric fibromatosis Epidermoid cysts & fibromas of skin Adrenal, thyroid & liver carcinomas Congenital pigmented lesions of retina Not all extracolonic lesions occur in same patient DDx Diffuse Periosteal Reaction DIFFUSE PERIOSTEAL REACTION “SCALPR” Scurvy/infection Caffey Accidental trauma Leukemia PGE2 Rickets |
|
|
Congenital diaphragmatic hernia
Case findings: Multiple gas-filled loops of bowel in the left hemithorax LUL opacification Shift of the mediastinum, cardiothymic silhouette, and trachea to the right OG tube is in the region of the stomach DDX multicystic lung mass: Congenital diaphragmatic hernia Congenital lobar emphysema CCAM Bronchogenic cyst Sequestration |
|

|
Congenital radioulnar synostosis
Case findings: Osseous synostosis of proximal radius and ulna with associated posterior dislocation of the radial head Lateral bowing of the radius Union can be from simple fibrous union to complete ostosis Classification: Type I: Synostosis not involving bone, and associated with a reduced radial head Type II: Visible osseous synostosis associated with a normally reduced radial head Type III: Visible osseous synostosis with a hypoplastic and posteriorly dislocated radial head. Type IV: Short osseous synostosis with anteriorly dislocated mushroom shaped radial head |
|

|
Hirschprung’s disease
Case findings: BE: short transition zone in sigmoid, colon proximal to this region is markedly dilated, no mucosal ulcerations DDX pediatric colonic distention: Hirschprung’s disease Imperforate anus Colonic atresia Meconium plug syndrome (left colon syndrome) Ileal atresia Meconium ileus: associated with CF Acquired Megacolon |
|

|
Retropharyngeal abscess
Case findings: XR: thickening of prevertebral ST CT: large low density mass with thin enhancing wall and multiple septations in prevertebral ST extending into lateral left neck DDX: Pyogenic retropharyngeal abscess Granulomatous retropharyngeal abscess Prevertebral hematoma Neoplasm: cystic hygroma or (capillary) hemangioma |
|
|
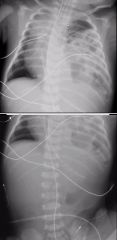
Neuroblastoma
Case findings: Paraspinal large mass occupying upper right chest Extension into neural foramen with an epidural component Multiple areas of calcification within mass Multiple lytic lesions compatible with metastatic disease DDX pediatric posterior mediastinal mass: Neurogenic tumors (90%): Neuroblastoma, ganglioneuroblastoma, ganglioneuroma Neurenteric cysts Rare in children: Schwannoma, neurofibroma, paraganglioma Extramedullary hematopoiesis |
|

|
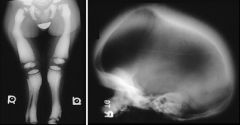
Fibular hemimelia
Case findings: Fibular rays are absent bilaterally Tibias are foreshortened and bowed anteriorly at the mid to distal diaphysis Talar and calcaneal ossification centers are not present on the left and the talar ossification center is not present on the right 3 metatarsals on the right and two on the left 2 digits are present on each foot with musculotendinous orientation of the 1st and 5th digits Lateral rays of the foot are often absent Tibia is usually bowed anteromedially Associated with: PFFD (Proximal Femoral Focal Deficiency), DDH, coxa vara, tarsal coalition DDX: Camptomelia dysplasia: Fatal, large head, short trunk and short limbs Anterolateral bowing of LE Bell-shaped chest Congenital tibial bowing Weyer oligodactyly syndrome: Deficiency of ulnar and fibular rays |
|

|
Inguinal hernia with SBO
Case findings: Supine KUB demonstrates an abnormal bowel gas pattern with air-filled distended bowel seen in the left mid-abdomen Thickened inguinal fold containing air-filled bowel DDX SBO in children (AAIIMM): Appendicitis, adhesions Intussusception, inguinal hernia (often incarcerated) Malrotation with volvulus, Meckel’s diverticulum |
|

|
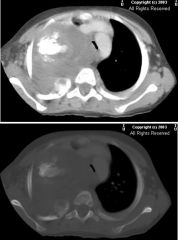
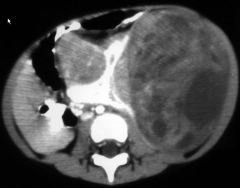
Intra-pericardial teratoma
Case findings: CXR: enlargement of cardiothymic silhouette, RUL opacity CT: heterogeneously enhancing mass with calcification, which distorts the atria and ventricles, and arises from the pericardium Teratoma: contains calcification and fat Calcification and fat suggest but are not guarantees of benignity |
|

|
Eagle-Barrett syndrome (Prune-Belly syndrome)
Case findings: Post-void shows moderate amount of residual urine Large diverticulum off the dome of the bladder (urachal diverticulum) Dilatation of posterior urethra without urethral obstruction Upon physical examination, patient had undescended testicles Triad: Deficiency of abdominal wall musculature Dilated urinary tract Undescended testicles Hypothesis: Transient in-utero obstruction of the urethra leads to Dilatation of posterior urethra Hypoplasia of the prostate Dilation of the bladder with persistence of the urachus (urachal diverticulum) Dilation of ureters with hydronephrosis Dilated bladder prevent testicles from descending Resultant urinary ascites causes stretching and thinning of the abdominal wall musculature Dilated posterior urethra without evidence of PUV or other causes of obstruction Dilated bladder with persistent urachus (urachal diverticulum) Reflux and hydronephrosis Undescended testicles Hypoplastic abdominal wall musculature Malrotation Pulmonary findings associated with oligohydramnios |
|

|
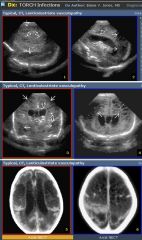
Lenticulostriate vasculopathy
Deposits of amorphous basophilic material within the lenticulostriate vessel walls (echogenic) Linear, non-shadowing echogenic structures within the thalami and/or basal ganglia which correspond to lenticulostriate vessels Etiology: Normal variant TORCH infection Trisomy 21, 13 Intrauterine cocaine exposure Neonatal asphyxia Ischemia |
|
|
Congenital cystic adenomatoid malformation (CCAM)
Case findings: CXR: RLL lucency CT: complex RLL cystic structure with a thin wall (imperceptable in some areas) 80% of cases present less than 6 months Type I: Unilateral single or multiple air filled cysts in the thorax May be large and occupy the entire lung, producing a mass effect Type II: Multiple small uniform cysts Type III: Solid intrathoracic mass rather than as a cystic or air filled structure DDX cystic pulmonary lesion Congenital cystic adenomatoid malformation (CCAM): equal lobe disrtibution CDH: air-filled or contrasted-filled bowel loops above diaphragm Bronchogenic cyst Usually mediastinal; in lung medial one third Usually opaque, occasionally, air fluid level Marked displacement of lung and mediastinum NOT a feature Congenital lobar emphysema LUL > RML > RUL Marked shift of mediastinum and compression of lung If fluid-filled, may simulate CAM type III |
|

|
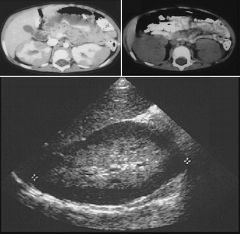
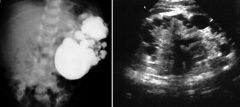
Case findings:
US: solid mass with a low echogenicity CT: large smooth, solid, encapsulated tumor with a small amount of functioning renal tissue posteriorly MC neonatal solid renal tumor (3 months) Benign but with malignant potential Cannot be distinguished from a congenital Wilms' tumor (age is the discriminating factor) |
|

|
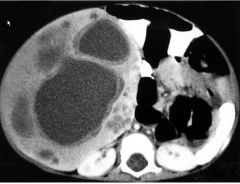
Multilocular cystic nephroma (MLCN)
Case findings: Well-marginated, rounded, or polycyclic cortical mass that extends beyond the normal renal outline Multilocular cystic renal tumor: term that encompasses two histologically distinct entities Multilocular cystic nephroma (MLCN) 1/3 of MLCN theoretical risk of cystic RCC, MC adult women Cystic partially differentiated nephroblastoma (CPDN) CPDN: 2/3 of MLCN, MC young children, theoretical risk of Wilms’ tumor Imaging cannot distinguish between MLCN and CPDN Clinical presentation: Painless abdominal mass with rapid enlargement Features: Well-marginated cysts with multiple septa (only septa enhance) Congenital lesion with large (> 10 cm) cystic lesions Compared with the poorly defined necrotic cystic appearances of a degenerative Wilms' tumor Multilocular cystic renal tumor features: Round, well-encapsulated multilocular cystic mass Central location Invasion into renal sinus Prolapse into collecting system (pathognomonic finding) Contain multiple non-communicating cysts with thin septa separating the cysts DDX: Cystic Wilms' tumor Wilms' tumor coexisting with CPDN Current thinking suggests that cystic nephroma, CPDN (Cystic Partially Differentiated Nephroblastoma) and Wilms’ tumor represent a spectrum of disease MLCN: benign end of the spectrum Wilms' tumor: malignant end of the spectrum CPDN: intermediate stage where blastemal elements are present within internal septa Multilocular cystic nephroma |
|
|
Nephroblastomatosis
Presence of multiple or diffuse nephrogenic rests Classic: Multiple solid subcapsular mass lesions Hypovascular US: hypoechoic Potential of a malignant transformation into a Wilms’ tumor Require close follow-up to 7 years of age to screen for Wilms’ tumor |
|
|

Wilms’ tumor
MC abdominal malignancy Immature renal elements (nephroblastoma): blastema (forms glomeruli), tubules, stroma Clinical presentation: painless abdominal mass, hypertension (from tumor renin production) Features: Well-defined, appears encapsulated, NOT invasive Decreased enhancement compared to renal parenchyma Mostly solid with areas of cystic necrosis Wilms’ tumor: 2-3 years old 10% bilateral < 15% calcification Renal vein invasion 5-10% Neuroblastoma: < 2 years old MC bilateral 85-90% calcification Encases vessels Staging: I: within renal capsule II: outside capsule but resected (local vascular/pelvis invasion may be present) III: residual tumor in abdomen IV: hematogenous metastasis V: bilateral tumors, associated with nephroblastomatosis MC metastasis to lungs (hematogenous: IVC lungs) Associated with: GU anomalies: cryptorchidism, horseshoe kidney Beckwith-Wiedemann: macroglossia, visceromegaly, umbilical hernia, omphalocoele Hemihypertrophy Sporadic aniridia (congenital type) Perlman syndrome: facial dysmorphism (micrognathia, macrosomia, round face) Drash syndrome: male pseudohermaphroditism, glomerulonephropathy WAGR: Wilms’ tumor, aniridia, genital abnormalities, mental retardation Coronal T1: Left kidney replaced by tumor with areas of necrosis Tumor embolus in IVC extending to right atrium |
|
|
Neuroblastoma
Case findings: T1: infiltrative hepatic invasion by a neuroblastoma arising from the right adrenal gland T2: inhomogeneous high T2 mass 2nd MC solid tumor of childhood (< 2 years old) MIBG nuclear scan Classic: Calcification Vascular encasement Paravertebral widening, bony destruction or widening of the interpedicular distances IVP: displaces the kidney without distorting the renal collecting system In contrast, collecting system is usually deformed by Wilms' tumor DDx abdominal calcifications on KUB L-M-N Liver Meconium peritonitis Neuroblastoma Neuroblastoma Evans staging Stage I: Confined to organ of origin Stage II: Extends beyond organ of origin but does not cross midline (defined as contralateral pedicle edge) Stage III: Extends across midline Stage IV: Distant metastasis Stage IV-S (S for skin): Localized tumor in stage I or II, with metastasis limited to skin, liver, marrow (NOT cortex), infants < 9 months Neuroblastoma Metastasis to skull: causes regional resorption of cranial sutures (widened sutures without hydrocephalus) Metastatic syndromes: Pepper syndrome: massive liver metastasis in infants (stage IVS) Blueberry muffin syndrome: blue nontender skin nodules from skin metastasis in infants exclusively Similar skin lesions in leukemia metastasis chloroma) Hutchinson syndrome: widespread bone marrow and cortex metastasis Adrenal mass Neoplasm: Medullary: Neuroblastoma – malignant (ganglioneuroblastoma – intermediate, ganglioneuroma – benign, entirely mature cells) Pheochromocytoma Cortex: Adrenal cortical tumor Non-neoplastic: Adrenal hemorrhage Calcifications Congenital adrenal hyperplasia Wolman’s disease (rare): adrenal calcification and adrenocortical insufficiency Adrenal tumor Neuroblastoma Pheochromocytoma: Older child, non-specific appearance, vascular, MIBG Adrenal cortical tumor: Hormonal activity key to diagnosis Virilization in girls Pseudoprecocious puberty in boys Cushing’s syndrome |
|

|
Wolman’s disease
Rare lipid storage disease affecting the liver, spleen, and adrenal glands Associated with adrenal calcification and adrenocortical insufficiency DDX adrenal calcification: Adrenal hemorrhage Granulomatous disease (e.g., TB) Wolman’s disease |
|
|
Chronic granulomatous disease (CGD) of childhood
Phagocyte oxidase deficiency (AR) with increased susceptibility to infections DDX antral narrowing: CGD of childhood Peptic ulcer disease Crohn’s disease Acid ingestion Eosinophilic gastritis |
|

|
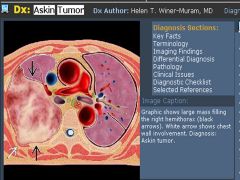
Askin tumor
Case findings: Paraspinal mass in right retrocardiac region Neuroectodermal tumor (PNET) of the thoracopulmonary soft tissues in children Retroperitoneal and pelvic regions and the extremities also may be affected Imaging Findings Best diagnostic clue: Large extrapulmonary mass in an adolescent or young adult May be difficult to determine if mass originates from chest wall or pleura May fill hemithorax With or without rib destruction (25-63%) Rapid growth Pleural effusion, frequent Lung and bone metastases Pathologic fractures Unique metastases to sympathetic chain CT can best delineate bony involvement and metastatic disease MRI best for soft tissue involvement Top Differential Diagnoses Ewing Sarcoma Rhabdomyosarcoma Neuroblastoma, Ganglioneuroblastoma, Ganglioneuroma Pediatric chest wall tumors Langerhans cell histiocytosis Askin tumor (PNET) Neuroblastoma Metastasis Ewing’s sarcoma |
|

|
Multicystic dysplastic kidney
Large non-communicating renal cysts No functioning renal parenchyma Atretic ureter, absence of renal artery Associated with: UPJ obstruction in contralateral kidney Horseshoe kidney |
|
|
Mesenchymal hamartoma
MC neonatal liver lesion < 2 years old, normal AFP Same as cystic hygroma in the neck Findings: multilocular cysts |
|
|
Hepatoblastoma
MC primary liver tumor of childhood < 5 years-old (MC < 2 years-old) 3rd MC abdominal malignancy (after neuroblastoma and Wilms’ tumor) Elevated AFP Enhance less than normal hepatic parenchyma Heterogeneous attenuation Solid mass, no cirrhosis Associated with: trisomy 18, Beckwith-Wiedemann, hemihypertrophy, familial polyposis syndrome |
|
|
Posterior urethral valve
Case findings: Trabeculated bladder Dilated posterior urethra with obstruction caused by posterior urethral valves MC cause of hydronephrosis in neonatal boys MC type 1: fusion of plicae anteriorly |
|
|
Caffey’s disease (infantile cortical hyperostosis)
Case findings: Diffuse swelling of the mandible Gross new bone formation on radius and ulna DDx Diffuse Periosteal Reaction “SCALPR” Scurvy/infection Caffey Accidental trauma Leukemia PGE2 Rickets DDX periostitis Normal variant Osteomyelitis Caffey disease (infantile cortical hyperostosis) Metastatic leukemia or lymphoma Premature infants: prostaglandins, TORCH Hypervitaminosis A Fluorosis |
|
|

Cloacal exstrophy
Severe variant of anorectal malformation Failure of normal separation of the hindgut and urogenital sinus by urorectal septum Results in a common perineal channel for the rectum and vagina in females and occasionally the bladder and urethra Terminology Spectrum of abnormalities resulting from abnormal development of cloacal membrane Imaging Findings Absence of normal bladder Lower abdominal wall defect Herniation of bowel between 2 halves of bladder Omphalocele forms upper part of defect Associated anomalies very common Top Differential Diagnoses Bladder exstrophy Isolated omphalocele Gastroschisis |
|

|
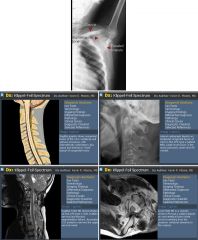
Sprengel deformity
Congenital elevation of a small scapula Associated with Klippel-Feil May have omovertebral bone connecting the scapula to the cervical spine KEY FACTS Terminology Klippel-Feil syndrome, Klippel-Feil spectrum (KFS) Imaging Findings Location: C2-3 (50%) > C5-6 (33%) > CVJ, upper thoracic spine Morphology: Vertebral body narrowing ("wasp waist") at involved disc space +/- "fusion" of posterior elements +/- Omovertebral bone Top Differential Diagnoses Juvenile Chronic Arthritis Chronic Sequelae of Discitis Surgical Fusion Ankylosing Spondylitis Pathology Caused by failure of normal segmentation of cervical somites (3rd → 8th weeks) Sporadic; familial genetic component with variable expression identified in many patients Clinical Issues Classic triad (33-50%): Short neck, low posterior hairline, and limited cervical motion Many patients have normal clinical appearance despite severity of involvement Diagnostic Checklist Much KFS morbidity and nearly all mortality related to visceral system dysfunction Look for instability, progressive degenerative changes, cord/brainstem compression |
|

|
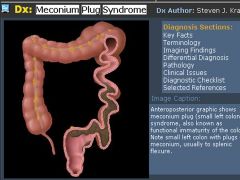
Small left colon syndrome
Case findings: Narrow microcolon to just below the splenic flexure Large meconium plug in the proximal bowel Distensible rectum which is unlike Hirschsprung’s disease, in which the rectum does not distend Small left colon is a variant on the theme of meconium plug syndrome Association with maternal diabetes Meconium plug syndrome Functional intestinal obstruction in the newborn Failure to pass meconium during neonatal period No organic obstructive cause Water-soluble contrast study is both diagnostic and therapeutic Terminology Meconium plug syndrome (MPS), small left colon syndrome (SLCS), functional immaturity of the colon (FIC) Transient functional obstruction of the newborn colon Common cause of distal neonatal bowel obstruction Imaging Findings Multiple dilated bowel loops in neonate Small left colon to the splenic flexure Abrupt zone of transition to dilated proximal colon at the splenic flexure Multiple filling defects may fill left colon, but not required Differential diagnosis long segment Hirschsprung disease Best imaging tool: Water-soluble contrast enema Pathology Distal colon spastic and narrowed, causes functional obstruction usually at splenic flexure Genetics: No association with cystic fibrosis Etiology: Probably immaturity of ganglion cells or hormonal receptors Associated abnormalities: Most with MPS do not have associated abnormalities Clinical Issues Abdominal distention Delayed or failed passage of meconium (> 24-48 hours) Bilious emesis Condition resolves over time, hastened by enemas Microcolon Small caliber colon due to failure of onward transmission of meconium in intrauterine life Associated with: Small intestine atresia Meconium ileus Small left colon syndrome Colonic atresia Long segment of colon with Hirschsprung’s disease Constituent part of the megacystis-microcolon hypoperistalsis syndrome Terminology-Meconium Ileus Neonatal obstruction of the distal ileum due to abnormally thick, tenacious meconium Essentially all patients with MI have cystic fibrosis (CF) Imaging Findings Best diagnostic clue: Distal bowel obstruction with microcolon and meconium-filled terminal ileum (TI) on enema Multiple dilated bowel loops ± Bubbly lucencies right lower quadrant (RLQ) Few, if any air-fluid levels (sticky meconium) Soft tissue mass or gasless abdomen Curvilinear calcifications on peritoneal surface or lining pseudocyst Smallest of microcolons Dilated, thick-walled, echogenic bowel loops Best imaging tool: Water-soluble enema Top Differential Diagnoses Ileal Atresia Total Colonic Hirschsprung Disease (HD) Pathology Mutations in CFTCRG, faulty electrolyte transport across epithelium Clinical Issues Most common signs/symptoms: Failure to pass meconium, abdominal distention, bilious emesis Uncomplicated MI: Serial hyperosmotic, water-soluble enemas vs. surgery Complicated MI: Surgery |
|
|
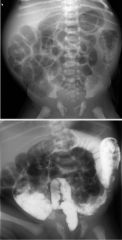
Hirschsprung's disease
Case findings: Transition zone in mid-descending colon, with proximal distension Narrow, nondistensible rectum Congenital absence of the intramural ganglia of the rectum Extending proximally for a variable distance which may involve the entire colon and a portion of the terminal ileum Increased in Down’s syndrome |
|
|

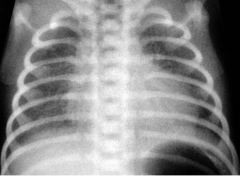
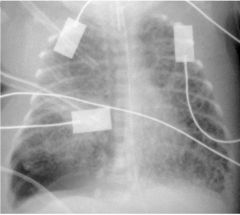
Hyaline membrane disease (respiratory distress syndrome)
Case findings: Increased fine reticular shadowing in the lungs CXR is abnormal by 6 hours of age Normal to decreased aeration In contrast, TTN shows increased aeration Early: fine reticular shadowing within the lungs with accentuation of air bronchogram As condition progresses, the lungs become more radiopaque |
|
|

Pulmonary interstitial emphysema
Case findings: Severe RDS right basal pneumothorax Hyperinflation due to ventilation pressure and PIE on the left Air leaking into interstitial space and spread through the lymphatics along the perivascular sheaths Classic: small bubbles of air radiating out from the mediastinum DDX Diffuse Cystic Lung Disease in Neonate “ Black Dots on a White Background” Week 1 – PIE Week 2-3 –Wilson-Mikity Week 4 – BPD, Wilson Mikity Developing Bronchopulmonary Dysplasia (Chronic Lung Disease) Bubble-like lucencies that are seen with developing bronchopulmonary dysplasia (BPD) can appear similar to PIE Age is helpful: PIE typically occurs during first week of life, BPD later Acuteness of onset: PIE is abrupt, BPD changes are gradual Terminology Abnormal location of pulmonary air within the interstitium and lymphatics; usually secondary to barotrauma Imaging Findings Best diagnostic clue: Bubble-like or linear lucencies within the lung Lucencies typically uniform in size Often radiate from hilum May be focal (one lobe) or diffuse and bilateral Involved lung usually noncompliant: Static lung volume seen on multiple consecutive chest radiographs, even with change in volume of uninvolved lung from radiograph to radiograph Serves as a warning sign for other pending air-block complications: Pneumothorax, pneumomediastinum Finding is typically transient CT findings: Air surrounds pulmonary arterial branches which are seen as soft tissue linear or dot-like densities surrounded by abnormal gas collections Clinical Issues Presence influences care givers to alter support: Switching from conventional to high-frequency ventilation Usually occurs during first several days of life Almost always during first week of life Almost always occurs only in infants on ventilator support |
|

|
Bronchopulmonary dysplasia (chronic lung disease of prematurity)
Case findings: Moderately severe BPD with pulmonary hyperinflation Areas of alveolar consolidation and hyperinflation Changes are evenly distributed Chronic lung disease that develops in infants treated with positive pressure mechanical ventilation and oxygen Classically BPD is defined clinically as a baby with an oxygen dependency at 28 days of age with an abnormal CXR Features: Patchy or linear strands of increased density with localized areas of unequal aeration Generalized hyperaeration |
|
|
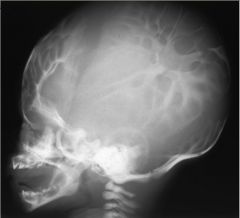
Multiple lacunae:
Physiologic up to 6 months Increased intracranial pressure Mesenchymal dysplasia (lacunar skull, luckenschadel) Abnormal development (dysplasia) of membranous bones of skull Associated with: myelomeningocele, myelocele, encephalocele DDX: Normal convolutional markings seen in the vault during the period of rapid brain growth (3 to 7 years) |
|

|

Primary megaureter
Case findings: Intravenous urogram: gross dilatation of both distal ureters with more modest dilatation of the more proximal collecting system Primary megaureter: Dilatation of the ureter is not related either to VUR or obstruction May be an abnormality in the nerve plexuses in the ureter reducing peristalsis Secondary megaureter: Ureteric dilatation has a cause MC vesicoureteric junction obstruction, post surgical obstruction, ureteric calculus or tumor, bladder outlet obstruction Isotope renogram: full bladder and moderately dilated ureters bilaterally |
|

|

Crossed fused renal ectopia
US: two kidneys lying in the left abdomen, with fusion of lower pole of LK to the upper pole of the transposed RK Two kidneys are on the same side of the body (MC right) Lower element is ectopic Ureter from this lower element crosses the midline to enter the bladder in the normal position Crossed fused renal ectopia Renal ectopia Horseshoe kidney: Two kidneys are joined at their lower poles Renal substance is low in position as ascent of the kidneys is prevented by IMA Prone to infection and scarring than normal kidneys Crossed fused ectopia |
|

|
Osteogenesis imperfecta
Inherited disorder of connective tissue with defective synthesis of collagen Generalized osteoporosis and bone fragility Non-osseous manifestations: laxity of the joints, deafness, brittle teeth DDX: Hypophosphatasia Non-accidental trauma Neurofibromatosis OI congenita type: thickened tubular bones from multiple healing fractures OI tarda type: thin tubular bones Blue sclera, fragile bones, otosclerosis (deafness), poor teeth (dentinogenesis imperfecta) Wormian bones Bowing deformities with multiple healing fractures Decreased bone density (severe osteoporosis) |
|

|
Blount's disease
Progressive varus deformity of the lower extremity Abnormal chondroepiphyseal growth on the medial side of the proximal tibial physis slowed and distorted growth of the medial physis causes a progressive bowing of the leg Types: Infantile: bilateral Childhood: unilateral DDX bowing of the knees in infants or children: Blount’s disease Physiologic bowing Post-traumatic Rickets Osteogenesis imperfecta Up to 2 years of age, the infantile (bilateral) form of Blount’s disease is difficult to distinguish between normal physiologic bowing of the knees Sharply angled appearance of Blount’s disease differs from the gradual curve in physiologic bowing |
|
|
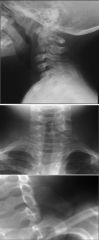
Klippel-Feil
Vertebral fusion may be partial or complete and may affect the vertebral bodies, the pedicles, the laminae or the spinous processes Associated with: Sprengel deformity: elevation of the scapula, associated with an omovertebral bone connecting the scapula and vertebrae |
|

|

Hypophosphatasia
Severe osteoporosis with delayed bone age Poor ossification of the skull vault Multiple fractures and multiple vertebral collapse Autosomal recessive, 4 types Defective skeletal mineralization resembling rickets and osteomalacia MULTIPLE FRACTURES “SHOT” Scurvy Hypophosphatasia OI Trauma |
|

|
Hypothyroidism
Cretinism: untreated hypothyroidism dating from birth Delayed skeletal maturity Fragmentation of femoral capital epiphysis (childhood), and stippled epiphysis (infancy) Wormian bones FRAGMENTED EPIPHYSIS “TWILL” Trauma/hypoThyroidism Warfarin Infection Legg Calve Perthes Leg dysplasia |
|

|

Scurvy
Vitamin C deficiency: deficient collagen synthesis Wimberger’s ring White line of Frankel Trummerfeld zone (lucent metaphyseal line) Pelkan spurs Subperiosteal hemorrhage |
|
|

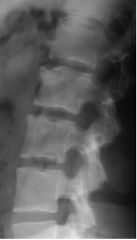
Scheuermann's disease
Osteochondrosis affecting vertebral body epiphysis Thoracic (MC) vertebral body anterior wedging, LC lumbar spine Disc space narrowing with calcifications Multiple Schmorl’s nodes: anterior endplate collapse due to herniated nucleus pulposis At least 3 consecutive bodies with at least 5 degrees of anterior wedging MC affects adolescent males, painful |
|

|

Thanatophoric dwarfism “death-bearing”
Spine: H configuration of the vertebra on the AP view, short pedicles, very flat vertebral bodies with large wide disc spaces Cloverleaf skull (Kleeblattschadel skull) Thorax: long and narrow; thin ribs, flared anteriorly Telephone receiver shaped femurs Thanatophoric dwarfism "clover-leaf" appearance (arrows) Classic radiograph showing spine and upper extremity abnormalities. Anteroposterior radiograph shows flattened vertebrae (one indicated by arrow). The ribs are short and thorax is small. Lungs are not aerated. Long bones of upper extremity are short and curved. Terminology Lethal short-limbed dysplasia Imaging Findings Best diagnostic clue: Severe dwarfism with narrow chest and short ribs Morphology: Severe flattening of vertebral bodies Best imaging tool: Antenatal ultrasound Top Differential Diagnoses Achondroplasia Osteogenesis imperfecta congenita Clinical Issues Most common signs/symptoms: Respiratory distress in neonate with dwarfism Usually fatal shortly after birth; may survive several years |
|

|
Turner’s syndrome
Case findings: short 4th metacarpal, Madelung deformity DDX short 4th metacarpal: Turner’s Pseudohypoparathyroidism Pseudopseudohypoparathyroidism Gorlin’s (basal cell nevus syndrome) Idiopathic DDX Madelung: Status post trauma or infection of the radius Multiple cartilaginous exostoses (osteochondromatosis) Turner syndrome Mucopolysaccharidosis (Hurler) Dyschondrosteosis (Leri-Weill – mesomelic dwarf) MADELUNG DEFORMITY “HITDOC” Hurler syndrome Infection Trauma Dyschondrosteosis Osteochondroma Congenital–Turner’s syndrome |
|
|

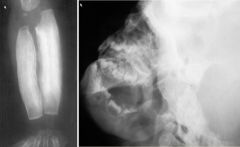
Ollier's disease (enchondromatosis)
Case findings: Osseous expansion and speckled calcifications in the femur, tibia and fibula due to enchondromas Nonhereditary, multiple foci of cartilage within bones and subperiosteal deposition of cartilage Involves one side of the body exclusively or predominantly Risk of malignant transformation to chondrosarcoma Maffucci’s syndrome: Nonhereditary enchondromatosis with soft tissue hemangiomas Maffucci’s syndrome Lack of bone modeling may lead to limb length discrepancies and tubulation deformities Intraosseous lesions are central or eccentric, are radiolucent, and contain variable amounts of calcification Phleboliths may be seen in the soft tissue hemangiomas Middle finger was amputated previously owing to chondrosarcoma |
|

|
Neuroblastoma
Case findings: CXR: Widening of the upper mediastinum and a paraspinal mass Possible erosion of the inferior edges of left ribs 4 and 5 CT: Large paraspinal mass with direct tumor extension through the neural foramen bilaterally Spinal canal stenosis and compression of the cord Mass partially encases descending aorta DDX posterior mediastinal mass Neurogenic tumor Neuroblastoma Ganglioneuroma Ganglioneuroblastoma Nerve root tumors Schwannoma Neurofibroma Paraganglioma Chemodectoma Pheochromocytoma MIBG scan: helpful for detecting metastases |
|
|
Cystic fibrosis
Case findings: Diffuse fatty replacement of the pancreas Fatty replacement of the pancreas (lipomatosis) is common and increases in incidence with age DDX: Pure pancreatic atrophy (e.g. chronic pancreatitis, cystic fibrosis) Congenital pancreatic hypoplasia (Schwachman syndrome) History of pancreatic resection |
|
|
ARPKD
Case findings: US: Large, echogenic kidneys bilaterally with innumerable small, anechoic cysts throughout Loss of the corticomedullary junction Degree of renal and hepatic involvement is inversely proportional Infantile ARPKD is associated with severe renal disease and mild hepatic disease Juvenile ARPKD is the opposite Neonatal death MC due to pulmonary hypoplasia |
|

|
Epidermolysis bullosa
Case findings: Esophogram: stricture of the cervical esophagus Hand XR: osteoporosis, soft tissue atrophy, contractures and pencil-pointing of the terminal phalanges Findings in the hands may resemble scleroderma MC upper esophageal stricture and bullae |
|
|
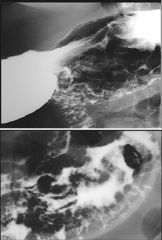
Menetrier's disease
Case findings: UGI: thick gastric folds CT: gastric wall thickening and thick folds Features: Massive enlargement of gastric rugae Thick-walled stomach Excessive mucous secretion Self limiting disease Associated with CMV infection MC presenting sign is edema of eyelids or extremities FOLD THICKENING “LAMAZE CLASSES” Lymphoma Adenocarcinoma Menetriers Zollinger Ellison Eosiniophillic gastritis GASTRIC MASS “CALL ME” Carcinoma Adenoma/Hyperplastic polyps Lymphoma Leiomyoma/Lipoma MEtastasis |
|
|
Chronic granulomatous disease (CGD) of childhood
Case findings: US: hypoechoic right hepatic lesion CT: hypodense right hepatic lesion with calcifications Phagocyte oxidase deficiency (AR) with increased susceptibility to infections Clinical manifestations depend upon the area of infection Chest: chronic or recurrent pneumonia proceeding to bronchiectasis Liver: starts as a granuloma abscess may develop from a granuloma Musculoskeletal: low-grade osteomyelitis with relatively little bone reaction for the extent of infection Gastric antral stricture is a rare manifestation DDX antral narrowing: CGD of childhood Peptic ulcer disease Crohn’s disease Acid ingestion Eosinophilic gastritis |
|
|
Patent urachus
Case findings: Cystogram: urachal remnant at the dome of the bladder US: fluid collection to the bladder Urachal anomalies: Patent urachus Urachal cyst Umbilicourachal sinus Vesicourachal diverticulum Urachal mucosa is transitional epithelium most of the urachal carcinomas are adenocarcinomas due to metaplasia of the mucosa into columnar epithelium and subsequent malignant transformation |
|
|

Sacrococcygeal teratoma
Classification: Type 1: Predominantly external, with minimal presacral componrent Type 2: Predominantly external, with significant intrapelvic component Type 3: Predominantly internal, with abdominal extension Type 4: Entirely internal with no external component Type 1 and 2 include 80 % of the cases DDX presacral cystic mass: Anterior meningocele Neuroectodermal cyst Retroperitoneal tumor of mesenchymal origin Perineuronal cyst (Tarlov cyst) Ovarian cyst Tarlov cyst Terminology Spinal nerve root diverticulum Type II extradural meningeal cyst (MC) Dilatation of arachnoid and dura of spinal posterior nerve root sheath, containing nerve fibers Imaging Findings Best diagnostic clue: Cerebral spinal fluid (CSF) density/intensity masses enlarging sacral neural foramina S2 and S3 nerve roots most commonly involved Widened canal Enlarged foramen Posterior vertebral scalloping Opacification of cyst by intrathecal contrast T1 C+: No enhancement Flow sensitive sequence may demonstrate signal loss within cyst Top Differential Diagnoses Meningocele Facet synovial cyst Pathology Common, incidental, and usually asymptomatic No reliable imaging method to differentiate symptomatic from asymptomatic lesions Rupture may cause spontaneous intracranial hypotension Nabors classification of spinal MC DDX: KIDS WITH SACRAL MASSES “RANT” Rectal duplication cyst Anterior meningocele Neuroblastoma Teratoma |
|

|

Carpal coalition
Case findings: Coalition of the lunate and triquetrum Hypoplastic scaphoid, overgrowth of the capitate and hamate MC lunate and triquetrum 2nd MC is capitate and hamate may be associated with Ellis van Creveld May occur as an isolated or associated with: Acrocephalosyndactyly Ellis van Creveld (chondroectodermal dysplasia) Turner’s syndrome Ellis van Creveld 'Six-fingered dwarfism' ('digital integer deficiency') was an alternative designation used for this condition when it was being studied in the Amish[4] and may have served a useful function in defining this then little known condition for the medical profession, as well as the lay public. |
|
|

Osteopetrosis (marble bone disease, Albers-Schonberg)
Case findings: Expansion of the medullary bone with sclerosis of marrow cavity Erlenmeyer flask Hair-on-end DDX osteosclerosis: Osteopetrosis Pyknodysostosis Melorheostosis Engleman’s (progressive diaphyseal dysplasia) Engelmann’s: affects only diaphysis of tubular bone In contrast, osteopetrosis affects the entire bone Renal osteodystrophy DDX Erlenmeyer flask (“CHONG”): Craniometaphyseal dysplasia: metaphyseal dysplasia (Pyle's syndrome) Hemoglobinopathies: SCD, thalassemia (marrow hyperplasia, hair-on-end skull, Erlenmeyer flask, extramedullary hematopoeisis) Osteopetrosis Niemann-Pick Gaucher’s DDX gracile bones (“NIMROD”): NF Immobilization Muscular dystrophy JRA OI Skeletal dysplasia SCLEROSIS-GENERALIZED “Regular Sex Makes Occasional Perversions Much More Pleasurable and Fantastic” Renal osteodystrophy Sickle cell disease Metastasis Osteopetrosis Pyknodysostosis Mastocytosis Myelofibrosis Pagets Fluorosis Osteopetrosis (marble bone disease, Albers-Schonberg) Types: congenital AR lethal, tarda AD benign Symmetrical generalized dense bones (lack of cortical and medullary differentiation) Bone-in-bone appearance in spine and long bones Sandwich vertebra sign: increased density at vertebral end plates Diffuse vertebral body sclerosis Increased density at skull base and calvaria Squared anterior ends of ribs Hair on end (anemia) Craniometaphyseal dysplasia Autosomal dominant (AD) craniometaphyseal dysplasia (CMD [MIM 123000]) (Jackson et al. 1954) is a rare skeletal condition that involves abnormal bone formation and mineralization in membranous as well as endochondral bones. Increased density of craniofacial bones, beginning at the base of the skull, can be diagnosed during early childhood. Sclerosis is accompanied by progressive thickening of the bones, which can cause narrowing of cranial foramina and can lead to severe visual and neurological impairment, such as facial palsy and deafness. Typical facial features of CMD include a wide nasal bridge, paranasal bossing, and orbital hypertelorism (fig. 1). Metaphyses of long bones are widened (Erlenmeyer flask-shaped) and exhibit decreased density (fig. 1). Diaphyses show normal patterns of trabeculation; however, the cortex can be thicker in some instances. |
|

|
Jeune syndrome (asphyxiating thoracic dysplasia)
Case findings: CXR: narrow thorax and expanded ribs, clavicles have a handlebar appearance Pelvis: acetabular roofs are horizontal with small spurs at the sacrosciatic notches Autosomal recessive Long bones: there is broadening of the metaphysis, cone shaped epiphyses, cupping of the metaphysis Narrow thorax and short, horizontal ribs Handlebar appearance of clavicles Triradiate acetabulum: flat acetabular roofs with downward spur projections Radiographic and histopathologic features similar to chondroectodermal dysplasia (Ellis van Creveld) Patients with asphyxiating thoracic dystrophy tend to have: Shorter ribs, a higher prevalence of progressive renal disease, hepatic fibrosis Less prominent nail changes and less frequent polydactyly |
|
|
Ellis van Creveld (chondroectodermal dysplasia)
Case findings: Small thoracic cavity with foreshortened ribs and humeri bilaterally Polydactyly, fusion of lateral metatarsals Autosomal recessive Features: Short-limbed dwarfism Congenital heart disease Polydactyly Ectodermal dysplasia DDX: Asphyxiating thoracic dysplasia (Jeune syndrome) DDX POLYDACTYLY Can afford to “BET” a finger or two. Trisomy 13 Ellis Van Cleveld Bardet-Biedel (genetic disorder characterized mainly by obesity, pigmentary retinopathy, polydactyly, mental retardation, hypogonadism, and renal failure in some cases.) |