![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
531 Cards in this Set
- Front
- Back
|
List some forms of Non-surgical therapy |
Plaque Control Supra and subgingival and root planing Adjunctive use of chemotherapeutic agents Occlusal Adjustment |
|
|
List some forms of surgical therapy |
Pocket reduction surgery (MWF, ORS, Ging) Mucogingival Regenerative Pre-prosthetic Implant |
|
|
What are the main objectives of periodontal surgery? |
-Create accessibility for proper professional SRP -Establishing a gingival morphology conducive to plaque control - Pocket depth reduction May Aim at regeneration of periodontal attachment |
|
|
Indications for Surgical Approach |
1) Mucogingival deformities 2) Areas with irregular bony contours, intrabony pockets or deep craters 3 )Pockets on teeth in which complete removal of local irritants not possible non-surgically 4) Deep pockets on grade II or III furcations for complete removal of irritants or root removal 5) Pre-prosthetic surgeries-for creation of favourable restorative environment (e.g. biologic width) 6) Establishment of tissue contours that facilitate oral hygiene measures (ex. Overgrown/fibrotic tissues) 7) Placement of endosseous implants |
|
|
What are three things that need to be completely removed in order for therapy to be effective regardless of Non-Sx vs. Surgical tx? |
1. Calculus 2. Plaque 3. Diseased Cementum |
|
|
Why is it not a good reason to jump into surgical tx? |
1) Removal of calculus + Bacterial plaque will decrease local inflammation. Therefore edema, hyperemia, tissue excess-->improved assessment of gingival contours+pocket depths 2) There is a threshold below which surgical therapy is actually more destructive. 3) Decrease in gingival inflammation in deep pockets makes soft tissues more fibrous+ firmer, makes surgical handling of tissue easier 4) Phase 1 can be used to assess home care efficiency. No home care= no point |
|
|
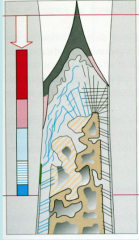
What is the definition of critical probing depths? |
Initial Probing depths (for a theurapeutic modality) below which loss of clinical attachment is likely to occur and above which attachment gain often results. |
|
|
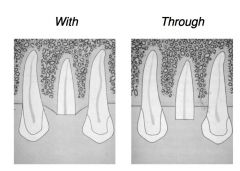
What is the Critical probing depth for the MWF technique? |
4.2mm (less than that and you'll cause CAL, above that you're more likely to get attachment gain) |
|
|
What is the Critical probing depth for SRP technique? |
2.9mm |
|
|
In the Kaldahl study that compared surgical methods and pocket depth reduction, which surgical technique sustained the most pocket reduction after phase II therapy? |
Osseous Resective surgery 1) Mean change in pocket depth for probing depths >7mm was around -3.7mm in the first year after surgery, followed by stability at -3.3mm 2) Mean change in pocket depth for probing depths 5-6mm was around -2.3mm in the first year after surgery, followed by stability at -2.0mm |
|
|
When comparing mean changes in attachment levels, which surgical techniques generated a loss of Clinical attachment when performed on probing depths at 1-4mm? |
Both Osseous resective surgery and Modified Widman saw loss of clinical attachment when performed on probing depths of 1-4mm. Hence the trend towards destructive effect of surgery in shallow pockets |
|
|
When comparing mean changes in attachment levels, which technique was least effective in terms of gaining attachment in pockets with probing depths that are greater than 7mm? |
Coronal Scaling alone. Generally ineffective for treating sites with deep probing depths! (Subgingival plaque is not removed). Many deep probing depths ended up with periodontal abscesses with just coronal scaling. |
|
|
Which surgical technique has been demonstrated to have the best reduction in probing depths and maintenance of clinical attachment gain over time? |
Osseous resective surgery. Everything else had 7mm pockets or got worse over time. |
|
|
For probing depths ranging from 1-6mm, which surgical technique showed the best maintenance of clinical attachment levels? |
Osseous resective surgery |
|
|
Rank the tx in terms of effectiveness at Pocket reduction from most effective to least effective |
ORS>MWF>RP>CS |
|
|
Rank the tx in terms of how much gingival recession they generate, from most recession to least recession |
ORS>MWF>RP>CS |
|
|
Rank the tx in terms of which ones are more likely to have periodontal abscess from least likely to most likely |
ORS>MWF>SC/RP>CS (NB: Perio abscesses occurred in initially deep pockets) |
|
|
Which tx had the most attachment gain? |
In >7mm: Equivalent, In <7mm MWF+RP>ORS |
|
|
Which Tx had the best PD reduction and maintenance of AL for PD over 7years for PDs>5mm? |
ORS |
|
|
Which Tx had the best PD reduction and maintenance of AL for PD over 7years for PDs< 5mm? |
RP |
|
|
Rank the tx in terms of which ones are more likely to have site breakdown in PD>5mm |
CS>RP>MWF>ORS |
|
|
Which patients had a majority of sites with breakdown? |
Smokers! |
|
|
T/F Furcation sites have loss of attachment over time regardless of tx |
True. Which is why furcated molars are not good abutments! |
|
|
Which tx were most effective at reducing PD in furcated molars? |
ORS>MWF>RP>CS |
|
|
Based on the Metal-analysis on surgical vs. Non-surgical therapy, which tx results in less attachment in shallow pockets? |
Non-Sx tx. |
|
|
Based on the Metal-analysis on surgical vs. Non-surgical therapy, which tx results in more gain in attachment but less pocket depth reduction in moderate pockets? |
Non-surgical tx |
|
|
Based on the Metal-analysis on surgical vs. Non-surgical therapy, which tx results in more gain in attachment AND more pocket reduction in deep pockets? |
Surgical tx |
|
|
What is typical sequela following most periodontal procedures? |
Appearance of Gingival recession but remember that recession is NOT caused by Periodontal tx! Perio Tx uncovers recession previously induced by the disease |
|
|
What are three potential problems that gingival recession brings? |
1. Esthetics 2. Sensitivity 3. Root caries |
|
|
What are the Basic necessities of surgery? |
1) Adequate visibility 2) Adequate knowledge and training 3) Appropriate instrumentation 4) Aseptic Technique |
|
|
What is the problem with overthinning flaps? |
results in compromise of blood supply and sloughing |
|
|
Two general factors that help decrease post op pain? |
Decreased Surgical time Decreased trauma during surgery |
|
|
Why should you avoid heating bone? What is the temperature threshold? |
You risk inducing osteonecrosis. Keep temperature under 47 degrees Celsius. Keeping it above this temperature for more than 1 minute will induce osteonecrosis |
|
|
Why do you want to avoid unnecessary exposure of bone? |
You will have increase resorption! |
|
|
What are three main ways peridontal flaps can be classified? |
1) Bone exposure after flap reflection -Full thickness (mucoperiosteal) -split thickness (mucosal) 2) Placement of flap after surgery -Nondisplaced flaps(returned to original position) -Displaced flaps (placed apically, laterally or coronally)
3) management of papilla -Conventional (removal of interdental tissue) -Papilla preservation
|
|
|
What is a full thickness flap? |
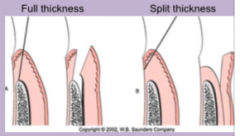
All soft tissue +periosteum is reflected to expose underlying bone
|
|
|
What is a Split thickness flap? |
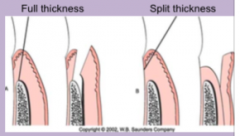
Reflection of epithelium and a layer of connective tissue leaving some connective tissue and periosteum on the bone |
|
|
What are some indications for Full thickness of flap? |
-Osseous resective surgery • Regeneration • Crown lengthening |
|
|
What are some indications for soft thickness flaps? |
Mucogingival surgery • Apically displaced flap |
|
|
T/F Whether or not you lose bone after the periosteum is raised depends on the surgical procedure |
False. You always lose bone when periosteum is raised. There Full thickness results in more surgically induced bone loss than split thickness |
|
|
How much bone loss is lost on average when mucoperiosteal flaps are used? |
0.8mm |
|
|
When are some situations where a conventional flap can be used? |

Used when esthetics is not an issue – posterior quadrants |
|
|
When are some situations where a papilla preservation flap should be used? |
Used in anterior sextants when possible • Need fairly large width of tissue |
|
|
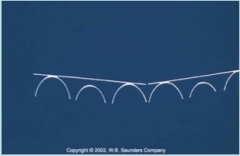
What is negative (reverse architecture)? |
abnormal gingival and/or osseous marginal contours; commonly not parabolic in form with the inter proximal tissue located in an abnormally apical position |
|
|
What is positive architecture? |

normal gingival and osseous marginal contour; commonly parabolic in form with the apex of the parabola located at mid buccal/lingual surfaces and interproximal tissue in the most coronal. |
|
|
What is one of the most important aspects of ORS? |
Correcting negative architecture |
|
|
Why is negative architecture so bad? |
The interproximal sites get deeper and deeper, making it impossible to clean. |
|
|
How what is the minimum amount of teeth that should be included in a flap? |
always extend at least one tooth mesial and distal to the area that you are working |
|
|
What is the benefit of increasing the amount of teeth involved in a flap? |
↑ visualization of site |
|
|
Benefits of vertical releasing incisions? |
↑ visualization of site
|
|
|
Which locations can vertical releasing incisions be used? |
Can be used on one or both ends of the horizontal incision (As long as the area permits it) |
|
|
Areas where vertical releasing incisions shouldn't be used? |
Mental Foramen, lingual of the mandible (Lingual nerve), distal of 7/8 in the maxillary (Greater palatine nerve), Canine Prominence |
|
|
How does vertical releasing incisions affect post op discomfort? |
↑ significantly post of discomfort (cuts off lateral blood supply) |
|
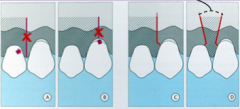
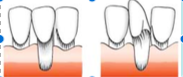
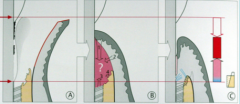
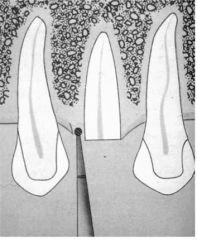
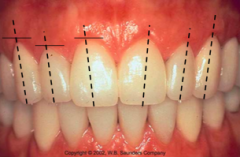
What is wrong with A? |
Danger of losing papilla |
|
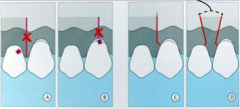
What is wrong with B? |
Danger of increased recession |
|
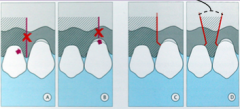
What is the incision in C called? |
Paramedian incision. Much better compromise than A or B |
|
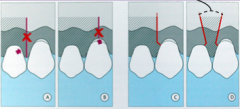
What is the problem with the black hashed lines in D? |
Far too close! |
|
|
Should vertical incisions be convergent or divergent from eachother? |

Divergent from eachother (Hashed black lines). (red is bad design). This helps to maximize blood supply |
|

What are some types of monofilament/ pseudomonofilament? |
steel, nylon, polyglycolic, Vicryl, Gore-tex |
|

What are some Advantages and disadvantages of monofilament/pseudomonofilament? |
• Advs: Ease of use, strength, minimal tissue rxn Disadvs: Poor knot strength |
|
What are some types of complex fibers? |
Silk |
|
|
What are some Advantages and Disadvantages of complex fiber? |
• Advs: Excellent knot security, ease of use, strength |
|
What is a type of twisted fiber? |
Catgut |
|
|
What are the advantages and disadvantages of Twisted fibers? |
• Advs: Soft, resorbable Not suitable if you want suture to last greater than 4-5 days time. |
|
|
What are the most common suture size used for periodontal surgery? |
Size 4 and 5 |
|
|
What are the three components of a surgical needle? |
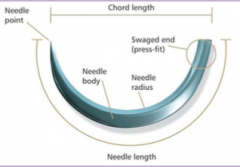
-Press fitted end (swage) -Body (Circle size) -Needlepoint |
|
|
What are the most common needle sizes used? |

3/8 and 1/2 |
|
|
Why should only Reverse needles be used in dentistry? |

prevents suturing material from tearing through surgical flaps. |
|
|
Difference between conventional and reverse cutting needles? |
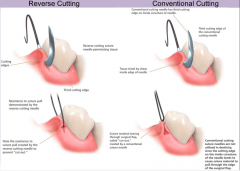
Conventional: Needle is square in cross section Reverse cutting: triangular cross section. |
|
|
What chemical can be used for suturing? |
Cyanoacrylate/Histoacryl. Specificially butyl and isobutyl. Do NOT used ETHTYL ('Super glue'). Toxic!!! |
|
|
How long does Cyanoacrylate last? |
exfoliated 4-7 days following use |
|
|
What is rationale for using Periodontal dressing? |
Rationale for use: Protect site from trauma ↑ Patient comfort if exposed bone present Keep debris out of wound Stabilize + protect grafts Help control post-op bleeding |
|
|
What is a contraindication for using Coe-Pack periodontal dressing? |
Patients with peanut allergies (Contains peanuts!) |
|
|
What does the scientific evidence say about periodontal dressing? |
No evidence to show improved healing and actually most patients prefer no pack (They hate the taste) |
|
|
What are the two kinds of healing that can occur? |
Primary and Secondary healing. |
|
|
Some features of healing by primary intention |
-Wound edges are replaced essentially in same position before the incision (No Gap) -Allows for wound repair with minimal scar formation -Decrease re-epithelization, collagen deposition, contraction+remodeling -Faster healing with decreased risk of infection+ scar formation Typical of: Periodontal flap surgeries, CTGraft harvest sites, GTR, most implant surgeries |
|
|
Some features of healing by secondary intention |
A gap is left between the edges of the incision Requires large amount of epithelial migration, collagen deposition, contraction and remodeling Slower healing More scar tissue Typical of: extraction sockets, FGG harvest sites |
|
|
Does administration of antibiotics (pre or post op) increase or decrease the prevelance of infections? |
tends to increase. Two possible reasons: 1) disturbs oral flora 2) Surgeons think they can be sloppier because patient is on Anti-Biotics |
|
|
What are other factors that may help decrease risk of infection |
Chlorhexidine Periodontal dressing (Not statistically significant in the study that looked at infection factors however) |
|
|
How much blood is lost on average during periodontal surgery? |
134mL |
|
|
Why is more blood lost in mandibular surgery versus maxillary surgery? |
Local infiltration used for maxillary which is better for hemostasis than blocks |
|
|
At what point should you consider IV fluid replacement for the patient? |
If greater than 500mL of blood lost during surgery |
|
|
Why should 1:50,000 epi not be used for LA? |
Rebound bleeding: 1:50,000 is really powerful. When you use |
|
|
What is the cause of the initial hemorrhaging during surgery? |
presence of granulation tissue |
|
|
What are some reasons for excessive hemorrhaging? |
• Lacerated capillaries and arterioles • Damage to larger vessels (palatine, incisal, inferior alveolar, lingual • Patients taking non-selective anti-inflammatory, blood thinners • High Blood pressure • Recent alcohol consumption • Bleeding disorders |
|
|
What are some methods that can be used to obtain hemostasis? |
-Pressure with Gauze -Sutures (deep with strong suture, vicryl, goretex, silk) -Surgical dressings (all stimulate coagulation physically rather than physiologically stimulating clotting cascades) -Epinephrine -Electrosurgery |
|
|
What are some methods for post-op pain control? |
Advil 600 mg q6h (2-3 days, continuously) Tylenol #3 1-2 tablets q6h (for break through pain only) Toradol 10 mg q6h (most effective if started IV...but GP won't use this generally) |
|
|
When is the only time that you would prescribe percocet or percodan? |
Extensive surgeries |
|
|
What are some things to help control swelling? |
Ice pack on for 10 minutes and off for 10 minutes for 1-2 hours May give tapering dose of dexamethasone depending on body dose for sinus grafts or osseous harvesting surgeries |
|
|
What should be used to help control Oral hygiene after surgery? |
-Peridex (chlorohexidine 0.12%) as a mouthrinse 10 ml BID for 7-14 days following surgery. • Grafts: Q-tip area |
|
|
List the post operative expectations of surgery |
discomfort – peak intensity in 2-3 days Bruising + Swelling – peaks in 2-3 days Swelling and bruising not common following flap surgery but possible following grafting Sensitivity to percussion not likely ↑ in tooth mobility Dentin sensitivity |
|
|
Main Objectives of Periodontal surgery? |
Creating accessibility for proper professional SRP Establishing a gingival morphology conducive to plaque control Pocket depth reduction May aim at regeneration of periodontal attachment |
|
|
Definition of Gingivectomy |
The excision of the soft tissue wall of a pathologic periodontal pocket without exposure of underlying bone. (NOT TO CROWN LENGTHEN!) |
|
|
Definition of Modified Widman Flap |
The excision of periodontal pocket with minimal alveolar bone exposure. |
|
|
Definition of ORS? |
The excision of periodontal pocket with osseous recontouring and the possibility of apical displacement on the flap |
|
|
What techniques can not be used to treat infrabony pockets? |
Gingivectomy or MWF. Only ORS can be used to treat Infrabony pockets |
|
|
What techniques can be used to treat gingival or suprabony pockets? |
Gingivectomy or MWF. |
|
|
Indications for Gingivectomy: |
Elimination of soft tissue pocket wall in suprabony pockets where a sufficient width of attached gingiva exists Elimination of soft tissue interdental craters and reverse architecture (ie. in necrotizing disease) Elimination of gingival tissue which is distorted because of a fibrous hyperplastic response to chronic irritiation |
|
|
Contraindications for Gingivectomy: |
Base of pocket approaches or extends beyond the MGJ (i.e. inadequate AG) When infrabony pocket or osseous craters exist Cannot be used for cosmetic crown lengthening (altered passive eruption) if osseous reduction necessary When regeneration of tissues is of interest |
|
|
What is the exception where Gingivectomy may be used for Crown lengthening? |
When it is to crown lengthen areas with gingival hypertrophy |
|
|
List the Healing timeline for Gingivectomies: |
• 0-5 hours: Clot formation, acute inflammation → clearance of necrotic cells |
|
|
When should Gingivectomy be probed again? |
4-6 weeks after surgery |
|
|
Indications for Modified Widman Flap? |
Elimination of soft tissue pocket wall in suprabony pockets while maximally maintaining attached/keratinized tissues Elimination of soft tissue interdental craters and reverse architecture Allows complete removal of subgingival calculus as well as smoothing and planing of root surface with direct vision Used in areas where minimal gingival recession is desired (ie. Maxillary anteriors) |
|
|
Contraindications for Modified Widman Flaps? |
When infrabony pocket or osseous craters exist Cannot be used for cosmetic crown lengthening (altered passive eruption) if osseous reduction necessary When regeneration of tissues is of interest |
|
|
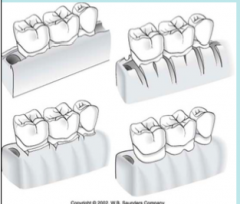
What type of surgery uses a external bevel incision? |

Gingivectomy ( solid black line) |
|
|
What type of surgery uses a internal bevel incision? |

MWF (------) |
|
|
T/F: In MWF there is a incison made around the base of the pocket |
False: in MWF the base of pocket undisturbed |
|
|
What sutures knots are generally used to close Modified WIdman Flaps? |
Single interrupted or Continuous sling |
|
|
Indications for Osseous Resective Surgery |
• Elimination of soft tissue pocket wall in suprabony and infrabony pockets while maximally maintaining attached/keratinized tissues • Elimination of soft and hard tissue interdental craters and reverse architecture • Allows complete removal of subgingival calculus as well as smoothing and planing of root surface with direct vision • Allows for elimination of infrabony osseous defects and all negative architecture |
|
|
Contrindications for Osseous Resective Surgery |
• When regeneration of tissues is of interest • When working in a region/patient where cosmetics is of utmost importance |
|
|
ORS initial incision: Why is incision location on buccal more forgiving than on palate? |
Buccal tissue is more |
|
|
What are the four steps to Osseous resection? |
1. Vertical Grooving 2. Radicular Blending 3. Flattening interproximal bone 4. Gradualizing Marginal bone |
|
|
Definition of Ostectomy? |
the removal of supporting bone designed to minimize post-operative sulcus depth, and attain positive architecture |
|
|
Definition of Osteoplasty? |
the removal of non- supporting bone designed to minimize post-operative sulcus depth and maximize gingival contour |
|
|
What is the most common intrabony defect? |
Interdental craters |
|
|
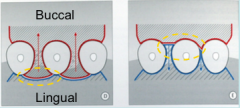
Reasons why interdental craters in Mx Molars are ramped palatally? |
Existence of abundant keratinized tissue Greater surgical access to wider palatal embrasures Cleansing effect of tongue Less post-surgical bone resorption → Palate contains ↑ cancellous bone |
|
|
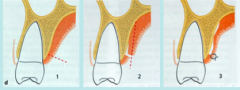
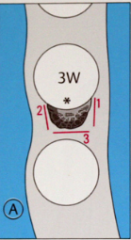
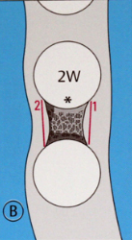
What is a class I interdental crater and how is it treated? |

2-3 mm deep osseous cavity with thick buccal + lingual walls. Tx: Complete palatal ramping (black part is removed) |
|
|
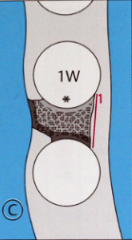
What is a class II interdental crater and how is it treated? |
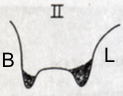
4-5 mm deep osseous cavity. Wider cavity = thinner walls + more abrupt slope into cavity. Most common defect. Tx: Removal of buccal bone to level of furcation and gross reduction of palatal bone. |
|
|
What is a class III interdental crater and how is it treated? |
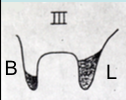
Class 3: 6-7 mm deep osseous cavity. Even more severe than class 2. Tx: Removal of buccal bone to level of furcation and gross reduction of palatal L bone as much as possible. May not be able to completely erradicate |
|
|
What is a class IV interdental crater and how is it treated? |
Crater of varying depth but with very thin B/L walls. Least common. Tx: As above, buy more conservative removal on buccal due to possible post-op resorption |
|
|
Give the healing time points for post ORS |
0-4 days: Clot formation b/w flap + bone. epithelial attachment initiated. |
|
|
What are the 2 main methods to eliminate pockets distal to the last maxillary molar |
Distal Wedge and Modification |
|
|
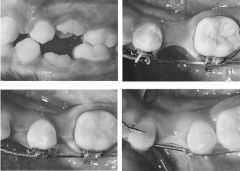
Describe the distal wedge technique on the last maxillary molar |

Distal Wedge: 1st incision delineates wedge. 2nd incision undermines it. N.B. Very important to conduct osseous resection, otherwise will not get significant pocket resolution. |
|
|
Describe the modification technique on the last maxillary molar |

Modification: 1st incisions are two parallel lines straight back. 2nd is perpendicular and 3rd incision undermines flap. Osseous resection just as important. |
|
|
What anatomical structure(s) complicates Distal pocket elimination in the mandible? |
Lingual nerve |
|
Which of these distal wedge incisions in the mandible is the preferred method? |
The bottom one! Incision remains in attached gingiva(N.B.!) and in a buccal direction which reduces the chances of severing the lingual nerve! |
|
|
What is the most common location of the lingual nerve relative to the last mandibular molar? |
86% of cases present with lingual n. 2 mm and 3 mm away in a horizontal + vertical distance from the lingual plate and crest in 3rd molar region. |
|
|
Does doing a distal wedge incision straight back or buccal completely eliminate the risk of severing the lingual nerve? |
NO! Reason: 14% of cases lingual n. is above osseous crest In 1/669 cases the lingual n. was in the retromolar pad |
|
|
What sensory information does the lingual nerve supply? |
– Anterior 2/3 of the tongue – Lingual mucosa and gingiva of the mandible |
|
|
What special sensory information does the lingual nerve supply? |
Taste to the anterior 2/3 of the tongue |
|
|
What procedures does not generally lead to an increase of tooth mobility? |
SRP, currettage, modified widman surgery |
|
|
What procedures will generate a significant decrease in mobility? |
SRP/curretage. ie. Non-surgical tx |
|
|
Which procedures will usually cause a temporary increase in mobility? |
Pocket reduction/Osseous resective surgery |
|
|
What is the typical progression of mobility post ORS/pocket reduction surgery? |
Peak at 2 weeks • Continue to ↓ for up to 2 years post op |
|
|
In which situations are there more likely to have residual deep PDs even after pocket reduction surgery? |
-Deep pockets greater than 9mm (DO NOT LET IT PROGRESS TO THIS STAGE IN THE FIRST PLACE. SUPERVISED NEGLECT!!!!) -If surgical access is poor -Post operative infection -poor oral hygiene (contraindicates surgery!) -Endodontic component to the lesion
|
|
|
Histology of Keratinized Gingiva? |
Thick stratified squamous Keratinized epithelium |
|
|
Histology of Non-Keratinized Gingiva? |
Thin Non-keratinized squamous epithelium |
|
|
Which locations in the mouth have keratinized gingiva? |
Attached and free gingiva, hard palate |
|
|
Which locations in the mouth have non-keratinized gingiva? |
lining mucosa of lips, vestibule, cheeks, floor of mouth |
|
|
What is the prevailing but contentious concept on the role of keratinized gingiva? |
To protect the periodontium from injury caused by wear and tear (mastication) To dissipate the pull on the gingival margin created by muscles of mastication on adjacent alveolar mucosa To protect against attachment loss + soft tissue recession b/c of ↑ tissue resistance to plaque associated gingival lesions |
|
|
How do we measure attached gingiva? How do we confirm? |

Measuring AG Step 1: Measure Pocket Depth Step 2: Measure distance from gingival margin to Mucogingival line/junction Step 3: Subtract step 1 measurement from step 2 Confirmation of lack of AG Coronal traction on probe |
|
|
Which has more attached gingiva? the Maxilla or mandible? |
Maxilla |
|
|
Which areas in the mouth have the smallest width of attached gingiva? |
Cuspid and 1st bicuspids on both arches |
|
|
Which areas in the mouth have the largest width of attached gingiva? |
Centrals and laterals |
|
|
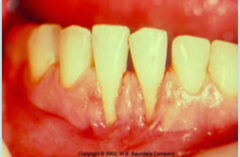
Definition of Recession |
Location of marginal gingiva apical to the cemento-enamel junction |
|
|
Mucogingival defects are generally the result of _____________? |
recession of attached gingiva |
|
|
What are the etiology of recession? |
Periodontal disease Traumatic oral hygiene Tooth position and angulation Cortical bone dehisences/ fenestrations of overlying roots Iatrogenic treatment Frenum pull |
|
|
What are some iatrogenic causes for dehiscences? |
Ortho: buccal version of teeth can cause dehisences |
|
|
What are some options for treating the cause of recessions? |
Txing periodontal disease Changing oral hygiene routine Tooth repositioning repositioning frenum |
|
|
Why are frenum pulls considered disadvantageous to OH? |
Thought to act as a trap door 1. Opens up during muscular movements = potential plaque trap 2. Closes and locks plaque in = facilitates subgingival plaque formation |
|
|
How does frenum pulls affect orthodontics? |
Orthodontically may lead to relapse of tx. or inability to close diastema |
|
|
Why are shallow vestibular depths considered disadvantageous to OH? |
1. Accumulation of food particles during mastication 2. Impedes proper oral hygiene measures (with recession you have shallow vestibular depth and it's hard for the patient to angle the toothbrush to allow the bristles to get into the sulcus) |
|
|
What are some indications for Mucogingival surgery? |
To increase the width of attached gingiva To attain root coverage To increase vestibular depth To manage high frenum pull Pre-orthodontics (if buccal tooth movement is planned + thin attached gingiva) To develop better soft tissue contours around teeth, pontics or dental implants. |
|
|
Is there a difference between grafted sites and un- grafted sites in progression of recession? |
YES! Maintained: both treated (FGgraft) and recession sites remained stable Unmaintained: FGgraft sites remained stable but sites with recession had inflammation and increased recession over time. |
|
|
What is the current consensus on what is considered inadequate keratinized tissue. |
Inadequate keratinized tissue(gingiva) is defined as < 2mm in width of which less than 1 mm is attached gingiva. |
|
|
Is there a minimal amount of attached tissues required around subgingival restorations? |
YES! If subgingival restorations placed, teeth with MAG had ↑ marginal inflammation than teeth with adequate attached gingiva (more plaque accumulation) |
|
|
Is there a minimal amount of attached tissues required around supragingival restorations? |
no differences in marginal inflammation noted between regular sites and sites with MAG |
|
|
if a tooth is moved orthodontically from a prominent buccal position to lingual, how does it affect bone/tissue height? |
You will increased bone height and tissue height. (Reverse is also true!!) |
|
|
under what conditions should a patient be treated with a graft as a part of pre-orthodontic care? |
Marginal tissue comprised of alveolar mucosa with a frenum pull Exposed root surface with minimal keratinized tissue and no attached Labial incisor eruption with minimal keratinized tissue and no attached and no lingual movement planned Thin periodontium and labial movement is planned Root exposure during tooth movement All of the above may progress with age |
|
|
When to consider grafting? |
Evidence of progression (noted longitudinally) In areas where oral hygiene is limited (lack of vestibule / frenum pull) Pre-prosthetic – in areas of subgingival restorations or where a denture flange may cause irritation (controversial) Pre-orthodontic Patient demands: Esthetics, root sensitivity Combination of: Minimally attached/keratinized tissues with presence of inflammation (BOP) and inadequate home care ± strategically important teeth Restorative: In areas with recession and shallow class V restorations – consider excavation of decay and root coverage |
|
|
Why can tissue grafting only be used to restore shallow class V restorations? |
deep it wont work because soft tissue wont flow into defects greater than 1mm. |
|
|
What are the tx options for recession in kids? |
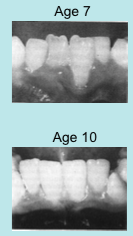
In children – observe recession defects longitudinally – will most likely improve. No general need for therapy |
|
|
What is class I recession? |
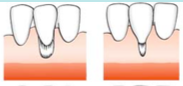
Marginal tissue recession that does not extend to the MGJ. There is no periodontal loss (bone or soft tissue in the interdental area |
|
|
What is Class II recession? |
Marginal tissue recession that extends to or beyond the MGJ. There is no periodontal loss (bone or soft tissue in the interdental area. |
|
|
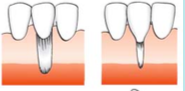
What is class III recession? |
Marginal tissue recession that extends to or beyond the MGJ. – Bone or soft tissue loss in interdental area or there is malpositioning of teeth. |
|
|
What is class IV recession? |

Marginal tissue recession that extends to or beyond the MGJ. Bone or soft tissue loss in interdental area is so severe that root coverage cannot be anticipated. |
|
|
In which classe(s) of recession can we expect to have 100% root coverage after grafting? |
Class I +2 can anticipate 100% root coverage Class 3 cannot predictably gain 100% root coverage Class 4 cannot predictably gain any root coverage |
|
|
indications for free gingival grafting? |
-To increase width of attached gingiva -Root Coverage -Frenectomy -Vestibular extension. |
|
|
Why are the first 48 hours in the healing of a Free gingival graft most critical? |
First 48 hours are most critical period since no vascularization |
|
|
What the sources of nutrition and hydration for the graft in a free gingival graft? |
Nutrition and hydration to graft provided by fluid diffusion from vessels of periosteal bed (called plasmotic circulation) |
|
|
What occurs during phase 1 (0-48 hours) of healing in a free ginigval graft? |
Blood clot forms between graft and underlying periosteal bed CT in graft is disorganized and undergoes some remodeling |
|
|
What occurs during phase 2 (3-5) days of healing of free ginigval grafts? |

Get sloughing of the epithelium + survival of underlying CT which contains genetic information for keratinized tissue Re-vascularization starts in 2-3 days. Get anastomosis between vessels in graft and underlying tissue bed |
|
|
What occurs in the 11-21 days after free gingival grafts? |
Graft and wound bed have joined + decrease in inflammatory response in underlying host CT |
|
|
What occurs 28 days after a free gingival graft? |

Epithelium appears normal , with surface keratinization, increased thickness and rete peg formation |
|
|
how long does it take for a free gingival graft to be fully repaired? |
4-6 weeks |
|
|
How does free gingival graft compare to connective tissue graft for root coverage? |

May not get full root coverage and not as aesthetic because it's thick |
|
|
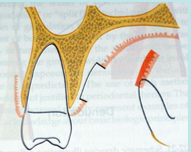
What are some safe donor sites to get a connective tissue graft from? |

-Safe zone=canine-2nd premolar (GP nerve+ vessel) -Typically want 2mm thickness (will contain more glandular tissue thanFGG) -Heal by primary intention
|
|
|
What are some safe donor sites to get a free gingival graft from? |

-Larger grafts can be acquired (not near vital structures) -Variable thickness (thicker grafts needed for root coverage, generally better CT) -Heal by secondary intention (Takes longer to heal) |
|
|
How does the depth of incision compare for FGG vs. CTG? |

|
|
|
Cross section of a connective tissue graft? |
|
|
|
Cross section of a free gingival graft? |
|
|
|
Which procedures is technically easier to do? FGG or CTG? |
FGG |
|
|
Which is more esthetic, FCG or CTG? |
CTG |
|
|
Blood supply for FGG? |
Periosteum |
|
|
What are two sources of blood supply for CTG? |
From Periosteum (split thickness flap) From overlying flap |
|
|
Which has better root coverage? CTG or FGG? |
CTG (Over avascular root, flap provides blood supply) |
|
|
Indications for Guided Tissue regeneration? |
-Increase width of Attached Gingiva -Root coverage -Root sensitivity. |
|
|
How is a Guided tissue regeneration performed? |
A flap is raised, a membrane is placed is around the necks of the teeth, sutures are placed and the idea is to let CT migrate. |
|
|
Indications for Coronally Advanced flap? |

– Class I recessions (Very minor cases) |
|
|
Rank the order of mean root coverage from least root coverage to most root coverage for the different surgical techniques |
Coronally advanced flap (61%) Lateral pedicle flap (67%) Free gingival graft (69%) Guided tissue generation (73%) Connective tissue graft (84%) |
|
|
What is alloderm? |
acellular dermal graft processed from cadaver skin Only the dermis layer(CT) present including the basement membrane Cellular components removed (therefore just a scaffold) Integrity of ECM maintained to avoid induction of inflammatory response |
|
|
What are the indications for Alloderm? |
Root coverage -Augment Width of attached gingiva (very poor because it's a different tissue!) |
|
|
Which had more PD reductions? Alloderm vs. CTG? |
CTG |
|
|
What had better root coverage between Alloderm vs. CTG in the short term? |
Comparable (Alloderm=93.4%, CTG=96.6%) |
|
|
What had better root coverage between Alloderm vs. CTG in the long term? |
CTG (97.0%)! (Alloderm (65.8%) only) |
|
|
Does Alloderm have more or less root coverage when multiple roots are covered? |
More root coverage! (Multiple=70.8 vs. One root 50.0%) |
|
|
Only in what type of pockets can you perform regeneration sx? |
Infrabony pockets! |
|
|
Definition of Repair and a clinical example? |
Healing of a wound by tissue that does not fully restore the: • Architecture • Function Ex: Long junctional epithelium (after OFD) |
|
|
Definition of Regeneration and a clinical example? |
Reproduction or reconstitution of a lost or injured part in such a way that the architecture and function of the lost or injured tissues are completely restored. Clinically → New Cementum, PDL, Alveolar bone |
|
|
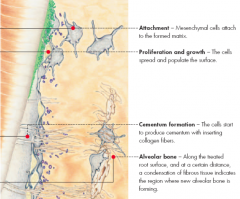
What are the 4 types of cells that involved in the "race" after Sx or Non-sx tx? Which of these are the fastest? |
Oral Epithelium cells (FASTEST!) Gingival connective tissues PDL cells Osseous cells |
|
|
what is the result if oral epithelium cells win the race and are the first to bind to the root surface? |
Formation of Long junctional epithelium |
|
|
what is the result if gingival connective tissues win the race and are the first to bind to the root surface? |
possible root resorption |
|
|
what is the result if Periodontal ligament cells win the race and are the first to bind to the root surface? |
Potential for new CT attachment |
|
|
what is the result if Osseous cells win the race and are the first to bind to the root surface? |
potential for ankylosis |
|
|
What are the 4 different possible manifestations of repair post perio tx? |
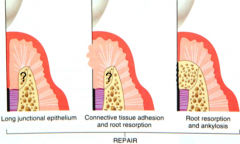
A LJE CT adhesion/Root resorption Ankylosis/Root resorption Unpredictable amount of osseous healing in repair |
|
|
List the 4 tissues that make up the periodontium |
• Epithelium • Gingival Connective Tissues • Periodontal Ligament Cells • Alveolar Bone |
|
|
what is the requirement needs to be met for the 4 tissues in order for healing to be classified as regeneration? |
All tissues must be involved and compartmentalized to allow for reconstitution of lost tissues |
|
|
What cells need to be excluded in order for regeneration to occur? |
Epithelial and Gingival connective tissue cells. This allows re-population of the site by PDL and osseous cells |
|
|
What is used in GTR that helps create space for cells to repopulate and regenerate tissues? |
Membrane (resorbable or non-resorbable) |
|
|
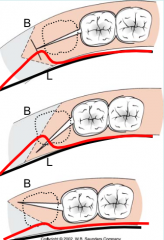
draw diagram that shows how repair occurs post conventional surgery |
B: race of tissues C: repair |
|
|
draw diagram that shows how repair occurs post GTR |

T: exclusion of epithelial and GCT by membrane to create space for PDL +osseous healing R=regeneration |
|
|
Potential benefits of regeneration vs. conventional surgery |
Improvement in both clinical attachment and bone levels Reduction in amount of recession → improved esthetics (mx. anterior) Less post-op sensitivity Reduced furcation involvement No compromise of osseous structure on adjacent teeth Both however lead to decreased probing depths and more maintainable sites |
|
|
List the requisite parameters for regeneration |
Pocket type: Infrabony pocket • Character of bone loss: Vertical bone loss • Defect type • Proximal bone levels |
|
|
What are the two main reasons why regeneration can only be achieved in infrabony pockets? |
-Improved vascularization (Surrounded by blood) vs suprabony where blood has to move vertically which is hard -Containment of materials |
|
|
What do bony walls provide in regeneration? |
increased protection/compartimentalization increased vascularity increased sources for pluripotential cells |
|
|
In the study where infrabony defects were treated with GTR, how many of the sites gained at least 2mm of bone? |
90% |
|
|
In the study where infrabony defects were treated with GTR, 3 wall defects gained how much % of the original depth? |
95% fill of original depth |
|
|
In the study where infrabony defects were treated with GTR, 2 wall defects gained how much % of the original depth? |
82% |
|
|
In the study where infrabony defects were treated with GTR, 1 wall defects gained how much % of the original depth? |
39% |
|
|
How deep must a intrabony defect be in order for the site to benefit from GTR? |
greater or equal to 4mm deep. This is the depth from the crest of the bone down to base of the infrabony pocket. NOT PD! |
|
|
Extent of regeneration is critically dependent on __________________ levels |
Proximal bone |
|
|
What type of flaps should be used for GTR and why? |
Papilla preservation flaps (preserves interproximal tissue!) |
|
|
Why is primary closure critical for regeneration? |
protection of biomaterials and exclusion of epithelium |
|
|
What is a autogenous graft? |
Graft obtained from the same patient |
|
|
What is a allogenic graft? |
graft obtained from other human, stored and processed in tissue banks |
|
|
What is a xenogenic graft? |
graft obtained from other species eg. Bovine, porcine |
|
|
What is a alloplast |
graft obtained from synthetic and inert material eg. Tricalcium phosphate and hydroxyapatite. |
|
|
Definition of Osteogenic |
Contain bone forming cells (marrow cells, undifferentiated cells) |
|
|
Definition of Osteoinductive |
Contains bone-inducing substances, ex. BMPs. |
|
|
Definition of Osteoconductive |
Serves as a scaffold for bone formation |
|
|
What type of properties does Autogenous graft have? |
Osteogenic, Osteoinductive, Osteoconductive |
|
|
What type of properties does Allogenous graft have? |
Osteoinductive, Osteoconductive |
|
|
What type of properties does Xenogenic graft have? |
Osteoconductive |
|
|
What type of properties does alloplast graft have? |
osteoconductive |
|
|
What are post-op complications unique to autografts? |
-Sequestration • Root resorption(when natural teeth present): Undifferentiated marrow cells – stimulated to generate odontoclasts |
|
|
What are the two types of allograft: |
Freeze dried bone allograft (FDBA) Demineralized freeze dried bone graft (DFDBA) |
|
|
List two ways demineralized freeze dried bone allograft(DFDBA) is different from Freeze dried bone allograft (FDBA) |
DFDBA: Oinductive and Oconductive + radiolucent( no minerals!)
FDBA: Oconductive only and radiopaque |
|
|
What allows Demineralized freeze dried bone allograft to be Osteoinductive? |
Demineralization exposes protein necessary for osteoinduction |
|
|
Are allografts safe? |
Very very safe. Materials used for >20 years and not a single case of dx transmission |
|
|
What are some uses/benefits for Xenograft? |
High degree of osteoconductivity Stabilizes blood coagulation Space maintenance function for membranes |
|
|
How predictable is GTR in furcations? |
•Substantial bone fill in mandibular and maxillary buccal class II furcations • Limited clinical improvements in maxillary interproximal class II furcations • Unpredictable for class III furcations |
|
|
What is emdogain? |
Porcine derived enamel matrix derivative containing a protein complex belonging to Amelogenin family. Attempt to mimic events during development of the dental root. By applying to denuded root surface, possible to regenerate acellular cementum → necessary for PDL and bone re-formation |
|
|
How does Emdogain work? |
Allows for attachment of PDL and proliferation of cells to exclusion of epithelial cells |
|
|
What are some patient factors affecting clinical outcomes of regeneration in intrabony defects |
Oral hygiene Smoking status (esp > 10 cigs/day) Level of residual periodontal infection |
|
|
What are some defect factors affecting clinical outcomes of regeneration in intrabony defects |
Morphology, i.e. depth/width # of residual bony walls Hypermobility Endodontic status of tooth |
|
|
What are some technique/healing related factors affecting clinical outcomes of regeneration in intrabony defects |
Careful flap design Correct placement of the material Optimal wound closure Optimal post-operative plaque control |
|
|
In general, rank GTR, GTR+bone substitute and OFD from most to least effective in terms of AL change, PD reduction and Hard tissue probing at re-entry? |
GTR+bone substitute> GTR alone >OFD |
|
|
In general which is more effective, Emdogain or OFD in terms of positive AL change and PD reduction? |
EMD>OFD |
|
|
What are the three way the pulp and the periodontium communicate? |
1. Apical Foramen 2. Lateral (aka accessory) Canals 3. Patent dentinal tubules |
|
|
What is marginal periodontitis? |
An inflammatory response to an infection in dentogingival region |
|
|
What is apical periodontitis? |
An inflammatory response to an infection of the root canal space |
|
|
What are two ways apical and marginal periodontitis communicate? |
Deep periodontal pockets lateral/accessory canals |
|
|
What are the most common routes of communication between PDL and the pulp? |
Apical third of root Furcation area |
|
|
What is a primary endo lesion? |
It is a chronic apical lesion due to a necrotic pulp that is exacerbated, leading to a endodontic abscess. Periodontal support may be lost in the process |
|
|
What are the 2 possible routes by which a primary endo lesion can drain? |

can drain either through sulcus or pocket |
|
|
What is the typical tx for primary endo lesions? |
RCT alone. Can even resolve perio damage done by the primary endo lesion |
|
|
Generally, what are the statuses of the pulp involved in periodontal lesions? |
Generally Vital |
|
|
What is a primary perio lesion? |

Begins as marginal periodontitis that progresses to involve the apical foramen. Plaque and calculus on root surface |
|
|
What is usually the pulpal status of primary perio lesions? |
Start off as vital, but subsequently necrose |
|
|
What is the typical treatment for primary perio lesions? |
RCT, followed by Perio Tx. |
|
|
What is a primary perio and 2ndary endo lesion? |

Marginal periodontitis progresses apically, which exposes lateral canals. This leads to pulp pathosis -->pulp necrosis (Contentious pathogenesis) |
|
|
Are primary perio and 2ndary endo lesions common? |
No. they're controversial and unlikely to occur |
|
|
Does Marginal periodontitis cause pulp pathosis? |
Several studies have failed to find a correlation between periodontal disease and tissue changes in pulp. Perio lesions almost never affect pulp unless apical foramen is involved! |
|
|
What needs to be present in order for a pulp to withstand marginal periodontitis? |
a intact blood supply via apical foramen |
|
|
What is a true combined lesion? |
Tooth has marginal periodontitis but then subsequently develops apical periodontitis. |
|
|
In teeth with true combined lesions, what should be the order of tx? |
RCT first, then perio. |
|
|
What occurs in the PDL during ortho tx despite our best efforts to prevent it? |
Necrosis and Undermining resorption |
|
|
In dentition that is periodontally susceptible, how often should the maintenance period be? |
3 months |
|
|
how does aligning crowded anterior teeth help a periodontal patient? |
Allows adult patient better access for adequately cleaning all surfaces of their teeth |
|
|
Vertical orthodontic tooth repositioning can improve ____________ in periodontal patients |
Osseous defects. (note. moving teeth towards teeth can also increase lesions) |
|
|
How can ortho tx be beneficial in severe fracture cases? |
Forced eruption allows crown prep to have sufficient form and retention for final restoration |
|
|
True/false? ortho can help regain lost papilla |
True |
|

Patient has a gummy smile. What is a perio tx you can do to fix this? What parameter must be checked before you do this tx? |

Gingivectomy. Must ensure that they have enough attached gingiva and sulcular depth! |
|
|
What are some common perio surgical procedures done in preparation for ortho tx(5)? |
Frenectomy Supracrestal fibrotomy Free gingival graft Apically positioned flap Closed Eruption technique |
|
|
When is a apically positioned flap required as part of orthodontic tx? |

used to uncover labially impacted maxillary anterior teeth. |
|
|
When is closed eruption technique used? |

Used to uncover labially impacted maxillary anterior while maximally preserving attached gingiva |
|
|
What are 5 things that Ortho perio procedures can be used to correct (5)? |
1) Bony defects 2) Molar uprighting 3) Forced Eruption 4) Intrusion 5) Preimplant ortho |
|
|
What are the two main ways with which forced eruption can occur? |
With bone or through bone |
|
|
What is the speed at which you want to do forced eruption? What is the problem with this? |
Eruption needs to be done slowly. The problem is that doing this is that the bone surrounding the tooth will be brought down as well. Solution to this: remove excess bone with file or bur. |
|
|
If you intend to do forced eruption through the bone what fibers need to be removed in order for the tooth to erupt while not bringing bone down with it? |

supracrestal fibers |
|
|
During forced eruption the tooth needs to be continually grinded down as it's erupting. What needs to be added to the newly erupted tooth as a result of poor C:R? |

Fixed retention |
|

Patient has ankylosed molars that need to be extracted and later replaced with a implant. What is the sequence of the tx? |
Extract ankylosed primary molar. Move the 4 posteriorly, converting it into 5. The process of moving the 4 distally will improve the bone deficiency caused by the ankylosis. The space where the 4 previously occupied now because the space for the implant. Place implant |
|
|
What are some aesthetic evaluation criteria for teeth that are evaluated? |
1) Midline (ON?) 2) Tooth axis 3) Incisal edge location 4) Interincisal angle 5) Shape and Outline of teeth |
|
|
What are some aesthetic evaluation criteria for gingiva that are evaluated? |
Gingival Margin Gingival Zenith Papillary triangle Interproximal Contact |
|
|
What are some aesthetic evaluation criteria for lips that are evaluated? |
Smile line (high or low)? |
|
|
What is the the magic number for Golden proportion? |
When the ratio between B and A is in golden proportion, then B is 1.618 times larger than A |
|
|
What is the significance of the golden proportion? |
human proportions that follow the golden proportion are aesthetically pleasing to the eye. |
|
|
What aspect of anterior teeth should ideally be in golden proportion? |
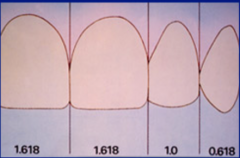
Their widths. (Central is 1.618 times wider than the lateral. Lateral is 1.618 times wider than the canine). The anterior sextant also should be 1.618 times wider than posterior sextant |
|
|
How much longer should the canines and central incisors be than the lateral incisors? |
20% Canine and Canine incisor avg length: (10.5-12mm)
Lateral incisors average length (9-10.5mm) |
|
|
How much wider is the centrals compared to laterals and canines? |
* Centrals are 25% wider than laterals and 10% wider than canines (Centrals are the widest teeth!) |
|
|
What is the length to width ratio of the anterior teeth? |
L to W ratio: Central-1.1:1 Lateral- 1.2:1 Canines-1.2:1 |
|
|
What line should the line drawn across the canines be parallel to? |
interpupillary line |
|
|
How much gingiva should be exposed during a smile? |
* Smile should expose interproximal papilla or (~1 mm) of gingiva apical to centrals and canines. |
|
|
how much further apical should the gingival margin of the central be compared to the lateral and canines? |
* Gingival margins of centrals should be 1-1.5 mm apical to laterals and in line with or slightly coronal to canines. |
|
|
What is the Gingival zenith and position should they ideally be relative to the center of the margin? |
Zenith: highest point of the crest. Should be slightly distal relative to the center of the margin |
|
|
What the treatment plan flow for esthetic cases requiring Crown lengthening? |
1. Consultation with patient regarding treatment outcomes 4. Surgery |
|
What is the significance of the 3mm measurement shown here? |
3mm distance away from the margin to re-establish new biological width |
|
|
How long should you wait for healing to ensure stability of gingival margins after crown lengthening? |
Should be O.K. after 3 months – if wanted to be extra cautious wait 6 months.
|
|
|
What's the problem with placing a restoration too early after crownlengthening? |
Recession. Patient won't be happy! |
|
|
For cosmetic cases requiring post and core + endo. What should be performed first? CL or RCT? Under what circumstance would the choice be reversed? |
1) RCT FIrst! Want to see if there are any endo complications (no point doing CL if endo is going to cause case to fail)
EXCEPTION: CL first if you know you can't get seal after endo. |
|
|
What is the definition of Passive eruption? |
Is the exposure of the teeth by apical migration of the gingiva. |
|
|
Stages of Passive eruption? |

1. Base of sulcus (BOS) and JE are on enamel 2. BOS on enamel and part of JE is on the root 3. BOS is at CEJ and entire JE on cementum 4. Both BOS and JE on root |
|
|
Of the stages of passive eruption, which stage is pathological? |
4 (Recession) |
|
|
Of the stages of passive eruption, which is normal in an adult? |
2 and 3 |
|
|
* Is there an age beyond which a diagnosis of altered passive eruption can be made? |
* 24 ± 6.2 years |
|
|
Tx for delayed altered passive eruption? |
Raise flaps, remove bone covering crown and suture |
|
|
for patients that had 4mm or less distance between contact point and gingiva, how many of them had papilla present? what about 5mm, 6mm and 7mm? |
4mm-100% of patients had papilla 5mm-98% of patients 6mm-56% of patients 7mm-27% of patients |
|
|
You placed implants to replace 21 and 11. The distance between the contact point and gingiva is 6.5mm. Patient has a black triangle...what is the most predictable way of eliminating it? |

Place more square shape restorations. Papilla regeneration surgery is unpredictable! |
|
|
What is the definition of Biological width? |
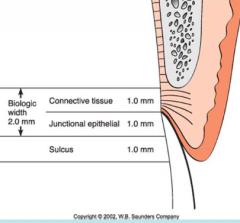
The dimension of space that the healthy gingival tissues occupy above the alveolar bone.
|
|
|
What are the two components of biologic width and what are their average dimensions? |
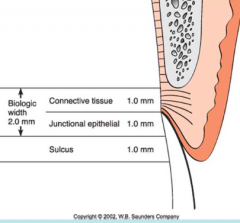
1) Junctional Epithelium (JE)=0.97mm 2) Connective tissue Attachment = 1.07mm Sulcus is NOT part of it! |
|
|
Of the components of biologic width, which is most variable? |
JE |
|
|
How is biological width assessed clinically? |
Bone sounding with LA sulcus depth on a number of teeth with gingival health.
|
|
|
What is violation of biologic width? |
Violation of BW will occur if the margins of a restoration impinge on the minimum distance required for the respective tissues (CT, JE) |
|
|
What is the body's response to violation of biologic width? |
Body doesn’t like violation and you’ll get a zone of chronic inflammation and the inflammation will cause BL and try to create new BW. Bone Loss will generate soft tissue loss, leading to recession and black triangles. |
|
|
On average, how much distance is needed from margin of restoration to alveolar crest to prevent violation of Biologic width? |
3mm (BUT on we should still do bone sounding) |
|
|
What is the typical response seen in people with thin biotype after biological width violation? |
Unpredictable amount of bone loss accompanied by soft tissue recession (unphysiologic re-establishment of biologic width)
|
|
|
What is the typical response seen in people with thick biotype after biological width violation? |
Bone level appears unchanged but gingival inflammation develops and persists.
|
|
|
What is expected if you place a restoration and the margin is at the bone crest? |
Expect to see significant loss of attacment and increase in recession due to violation of BW
From study: 3.16mm recession and 1.17mm bone loss |
|
|
What are two methods of correcting violated biologic width? |
1) Removing bone away from proximity of the restorative margin (To allow for ~ 3 mm of space b/w margin and bone). If anterior crowns= may have to replace! Since we are creating recession
2) Ortho extrusion of tooth |
|
|
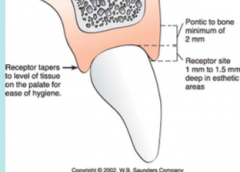
What are the soft tissue requirements needed in order to use a ovate pontic? |
|
|
|
How long is the scultping period for an ovate pontic? |
3-4 months |
|
|
What are 2 methods to ensure pontic height is preserved? |
1) Ovate pontic site development OR 2) Ridge preservation procedure (ie. Place a graft at time of extraction) |
|

Pictured here is a patient who got extraction of 11 and had a FPD placed. Patient isn't happy with the results. What could have been done differently to avoid this result? What can you do to fix this? |
Avoid it: Wait at least 8 weeks after extraction prior to taking final impression!
Alternatively we can crown lengthen the abutments |
|
|
What is it a good idea to do a free gingival graft as a ridge augmentation procedure? |

FGG=good for vertical and horizontal ridge augmentation |
|
|
What is it a good idea to do a Connective tissue pedicle as a ridge augmentation procedure? |

Good for horizontal ridge augmentation |
|
|
What is it a good idea to do a Pouch graft procedure as a ridge augmentation procedure? |

Good for both horizontal and vertical ridge augmentation |
|
|
What are the Goals of Periodontal Maintenance |
* Prevent or minimize recurrence of disease * Prevent or reduce incidence of tooth or implant loss * To ↑ probability of locating and treating disease in a timely fashion * Monitor peri-implant status * Assess condition of implant-supported prostheses * Evaluate plaque control |
|
|
T/F: Maintenance phase can be performed on a periodontium with active disease |
F: Can only maintain a stable periodontium! if periodontium is unstable then this patient is NO LONGER A MAINTENANCE PATIENT!!! |
|
|
What are the criteria for a stable periodontium? |
1. Stable (preferably shallow) PDs + ALs 2. No inflammation 3. No abscesses |
|
|
List the 7 components of Periodontal maintenance |
A) Update Med/Dent Hx B) CLinical exam and compared to baseline C) Radiographic Exam D) Assessment of Oral Hygiene E) Tx F) Communication G) Planning |
|
|
List the things that are done during "Treatment" in periodontal maintenance |
* Removal of bacterial plaque – supra/subgingival * Behavioral modification: OHI, Counseling, adherence to PM intervals * Selective Root planning + Implant debridement * Occlusal adjustment * Use of systemic antibiotics, local antimicrobial agents * Surgical therapy (discontinuation of PM + treatment of recurrent disease). |
|
|
In private practice, how often should a patient have their periodontium evaluated? |
every 6 months |
|
|
What are biological basis behind Periodontal maintenance? |
* PM can limit recurrent periodontitis * Patients on PM have ↓ PDs, ↓ CAL, ↓ tooth loss, compared to those who are not * Patients rarely effective in completely removing plaque * Pocket debridement suppresses subginginval microflora, but pathogens return to pretx. levels in 9-11 weeks * It is not possible to predict progression of perio disease ∴PM provides periodic monitoring |
|
|
Is there a set time for how long a Periodontal maintenance should be? (ie. All maintenance appointments should be 1 hour) |
NO! Time required should be individualized! based on:
– # of teeth/implants – Systemic health – Hx. Of disease |
|
|
T/F: Periodontal maintenance is not necessary if the surgery was successful |
F: Any surgical procedure no matter how proficiently done will fail without PM |
|
|
How much faster do patients who aren't treated and maintained lose teeth compared to patients that ARE treated and maintained? |
Patients who aren't treated or maintained lose teeth approx 3.5X faster
Tx and maintained =(lose tooth every 9.1 years) No Tx and maintenance = lose tooth every 2.8 years |
|
|
How much faster do patients who are treated but not maintained lose teeth compared to patients that are both treated and maintained? |
approx 2x faster
Tx and maintained =(lose tooth every 9.1 years) Tx and but no maintenance = lose tooth every 4.5 years |
|
|
What are some proposed reasons for why compliance is so poor with Periodontal maintenance? |
Possibly because Perio dz is chronic and non-threatening -Economics -Fear -Others (Lack of compassion or re-enforcement from dental team) |
|
|
What factors tend to decrease patient compliance with periodontal maintenance? |
young age, smokers, non-surgically treated patients (Sx: patient don't want have to do surgery again)
|
|
|
The study that came up with the 3 month recall...what is a problem in the patient selection for that study? |
Patients with Non-Sx and Sx Tx were placed in the same recall pool. therefore: study doesnt' suggest Non-Sx therapy is only kind of therapy needed! |
|
|
What was the conclusion from the study about 3 month recalls? |
Personal OH/plaque scores not critical for maintenance of periodontal support if pt. received PM every 3 months |
|
|
What is effect of gingival inflammation if have 3 month recall? |
* OH which impacts on levels of GI has no effect on PD and ALs if 3 month maintenance
* Provides further evidence that gingivitis doesn't lead to periodontitis |
|
|
What does the data suggest about the periodontal maintenance of patients who have a history of perio dz? |
4x/year |
|
|
What are the 4 parameters that must exist before you can make the dx of recurrent gingivitis? |
* No deep probing depths * BOP / Suppuration / Redness or other signs of inflammation * No progressive attachment loss or marginal recession * Persistent damage from previous periodontitis and associated treatment in the form of gingival recession and some radiographic evidence of bone loss |
|
|
Patient comes to you during a new patient exam and you make the dx of recurrent periodontitis. Is this possible? |
NO! At a single visit it is not possible to determine if previously treated periodontitis is recurring
|
|
|
What are some clinical indicators of recurrent periodontitis? |
-Bleeding on probing at multiple PM visits (these sites are more likely to develop attachment loss) -↑ in Probing Depths |
|
|
Patient probing depths of 2s and 3s, no signs of BOP or edema, but there are clear signs of attachment loss(Exposure of root surface). What is the Dx? |
Marginal recession. |
|
|
What is definition of Recurrent/Refractory periodontitis? |
Disease that is not readily yielding to treatment |
|
|
What is refractory periodontitis characterized by? |
Progression of :
– Clinical attachment loss Despite seemingly adequate therapy |
|
|
List the 7 etiologies of Recurrent/Refractory Periodontitis? |
1) Inadequate or inappropriate treatment • Ex. Non-surgical treatment only 2)Inadequate maintenance • Non-compliance or too long of an interval 3) Inadequate plaque control • Recall effect of poor supragingival plaque control (Lecture #3) 4) Undetected systemic disease • Diabetes, neutrophil abnormalities, blood dyscrasias, etc. 5) Poor immune/host response 6) Persistent pathogens 7) Smoking |
|
|
What's a type of host modification therapy? |
low dose doxycyclin |
|
|
If a patient has been diagnosed with recurrent periodontitis and doesn't require sx, what is the staple treatment they require? |
Non-Sx treatment with antibiotics! Followed by OHI and a tight 3 month recall schedule |
|
|
What is the typical regimen for clindamycin when it is used as tx for recurrent periodontitis? |
150 mg qid X 7 days |
|
|
What is the typical regimen for Amox + Metronidazole when it is used as tx for recurrent periodontitis? |
Amoxicillin 375 mg tid + Metronidazole 250 mg tid X 7 days |
|
|
What is the typical regimen for Amox + Clavulin when it is used as tx for recurrent periodontitis? |
Amoxicillin/Clavulin 250 mg tid X 2 weeks |
|
|
What is the rationale behind using plastic currettes to maintain implants? |
Metal and ultrasonic instruments were found to scar implant surfaces. Plastic currettes are thought to be cause minimal or no significant changes to implant surface. However there is No clinical data to support hypothesized relationship between implant maintenance technique and implant failure. |
|
|
Pt has recurrent gingivitis or mild chronic periodontitis...who should do the Periodontal maintenance? |
GP |
|
|
Pt has hx of chronic periodontitis and moderate attachment loss...who should do the Periodontal maintenance? |
Alternate between GP and Periodontist |
|
|
Pt has hx of severe periodontal Attachment loss or aggressive periodontitis...who should do the Periodontal maintenance? |
Periodontist |
|
|
Pt with dental implants + extensive periodontal prostheses+ concurrent ortho therapy who should do the periodontal maintenance? |
Periodontist |
|
|
Describe the process responsible for dentin hypersensitivity after SRP? |
Initiation: smear layer that develops over root dentin follow SRP, but dissolves over 1 week= exposed dentin tubules.
Remission: Natural occlusion of tubules by mineral deposits |
|
|
How long does dentin sensitivity last? |
Peaks within 1 week of therapy and then disappears |
|
|
2 proposed mechanisms behind dentin hypersensitvity? |
1) Open tubules = ingress of bacteria --> increase pulpal inflammation --> sensitization of pulpal nerves
2) Hydrodynamic theory (fluid shift in dentinal tubules) |
|
|
What are the factors which impact degree of dentinal hypersensitivity? |
1) Open tubules 2) Tubular Sclerosis 3) Tertiary Dentin |
|
|
What are the four main treatments for Dentin hypersensitvity? |
* K+ containing agents (nerve desensitiziation) * F- containing agents (promotion of tubular occlusion, sclerosis) * Bonding/filling materials (tubular occlusion) * Root coverage (tubular occlusion) |
|
|
What is the last resort to tx dentin hypersensitivity? |
Endo |
|
|
Definition of Osseointegration
|
Direct structural connectionat the light microscopiclevel between bone + thesurface of a load carryingimplant
|
|
|
What is the typical % of osseointegration observed between bone and implant?
|
50-60%
|
|
|
What are the requirements for osseintegration? (6)
|
1. Biocompatible (Titanium)
2. Implant design (Cylindrical + threaded) 3. Healthy and vital bone 4. Atraumatic and low Temp sx technique 5. Surface finish: rougher>smoother 6. Loading conditions: No movement during healing |
|
|
What the 2 types osteogenesis that occur during the process of osteointegration?
|
Distance Osteogenesis
Contact Osteogenesis |
|
|
What is distance osteogenesis?
|
New bone is formed on the surfaces of the 'old bone' in the peri-implant site (Bone is grown from outside in towards implant surface)
|
|
|
What is contact osteogenesis?
|
New bone forms 1st on the implant surface and thenprogresses outwards (towards edge of osteotomy)
|
|
|
what process recruits osteogenic cells onto the implant surface prior to contact osteogenesis?
|
Osteoconduction
|
|
|
Briefly list the 5 steps of implant healing immediately following surgery (5)
|
1. Bleeding
2. Blood clot, platelets--> growth factors induce contact osteogenesis 3. blood clot forms fibrin network 4.Mechanical stability 5. Coagulum fills chamber b/w threads |
|
|
Criteria for implant success (5)? |
1 An individual, unattached implant should be immobile whentested clinically 2. No per-implant radiolucency 3. Vertical bone loss around implant should not exceed 0.2mm per year following the implant's first year of service 4. Need to be absence of persistant S&S or sensation 5. At the end of 10 years, 80% of individually placed implants should be successful in the context of these criteria |
|
|
List the 4 classifications of bone quality for implants |
Type 1 bone: Almost the entire jaw is composed of homogenouscompact bone (found predominantly in Md. anterior) Type 2 bone: A thick layer of compact bone surrounds a core ofdense trabecular bone (Mx. anterior, md. posterior) Type 3 bone: A thin layer of cortical bone surrounds a core of densetrabecular bone (mx. anterior, md. posterior, mx. posterior) – Type 4 bone: A thin layer of cortical bone surrounds a core of low-density trabecular bone (mx. posterior) |
|
|
Of the different types of bone quality, which types are the best for implant success? |
Types 1-3 |
|
|
How do the supracrest fibers differ between tooth and implant? |
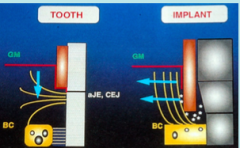
Tooth: oriented at different angles and fan out but some perpendicular to the tooth
Implant: Supracrestal fibers: Oriented predominantly parallel to the tooth |
|
|
How does the orientation of the supracrestal fibers in implants affect perio probing? |
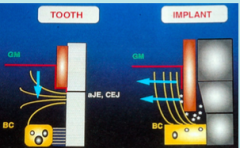
-There will be ↓ resistance towards perio probing onimplant vs. tooth sites
-The tip of the probe will consistently be positioned deeper in the connective tissues on implants than on teeth.
|
|
|
What is the distance between probe tip and bone in teeth? in implants? |
Teeth: 1.2mm Implants: 0.2mm |
|
|
What is the type of proprioception used in real teeth? What about implants? Which one is better? |
Teeth: Periodontal Mechanoreceptors Implants: Osseoperception -Teeth have better proprioception. |
|
|
What does most of the stress concentrate when an implant is being loaded? |
Stress concentrates at the crestal bone |
|
|
What is the axial mobility of an implant? what about a tooth? |
Implant: 3-5um Tooth: 25-100um |
|
|
What are some signs of implant overloading? |
Screw loosening or fracture, abutment or prosthesis fracture, bone loss, implant fracture |
|
|
What is the mean bone loss for implants during the 1st year of function? |
1mm |
|
|
What is the mean bone loss for implants between 1 and 20 years post op? |
1-2mm |
|
|
When looking at success rates for initial endo treatment, which conditions/factors negatively affected the success rate? |
presence of Peri-apical lesions, >2 roots, complications present (aberrant anatomy, crack in pulp chamber, perforation, file breakage, calcified canals) |
|
|
with regards to initial Endo treatment, which of the following has the highest odds ratio for failure? Peroperative radiolucency, # of roots or Complications? |
Radiolucuency! (3.55) followed bt number of roots (2.17) and complications (2.23) |
|
|
When looking at success rates for endo Non-surgical retreatment, which conditions/factors negatively affected the success rate? |
Periapical lesions pre-op, perforations pre-op, temporary restoration at follow-up |
|
|
with regards to Endo treatment, which of the following has the highest odds ratio for failure? Peroperative filling quality, Preop perf or restoration at follow up? |
Perf (26.52) followed by restoration (14) and last is pre-op filling quality (6.61) |
|
|
When is surgical re-treatment conducted for previously endo treated teeth? |
When large periapical lesion (>5mm) |
|
|
How many more times likely is a surgical re-treatment likely to fail if you have a >5mm lesion vs. <5mm lesion? |
2x more likely |
|
|
Is the overall success rate higher for NSRCT re-treatment or surgical retreatment? |
NSRCT re-treatment |
|
|
What factors are associated with only a 75-85% success rate for endo treatment |
-Teeth with periapical pathology (≤ 5mm) -Teeth requiring initial, non-surgical or surgical re-treatment -Multi-rooted teeth |
|
|
What factors are associated with only a >90 % success rate for endo treatment? |
-Teeth without any periapical pathology -Teeth requiring initial or non-surgical re-treatment -Teeth without any complications -Single rooted teeth |
|
|
What factors are associated with only a 40-65% success rate for endo treatment? |
-Teeth with large (> 5mm) periapical pathology --Teeth for surgical re-treatment -Teeth with complications -Teeth with Multiple roots |
|
|
In the meta-analysis that looked at 92 papers that evaluated success of implants vs. fixed partial dentures, what was the overall success rate for single implant restoration? |
95.1% |
|
|
In the meta-analysis that looked at 92 papers that evaluated success of implants vs. fixed partial dentures, what was the overall success rate for fixed partials of all designs? |
84.0% (include maryland bridges) |
|
|
What is the typical failure pattern with conventional fixed partial dentures? |
Small early failure rate, followed by increasing failure with time |
|
|
What is the typical failure pattern with Implant supoorted restorations? |
Small but rapid early failurerate followed generally stable long-term service |
|
|
List 3 complications that can cause implant failure (most common to least common) |
1) Screw loosening or fracture 2) Material wear/Cement failure 3) Implant fracture (rare) |
|
|
List 4 complications that can cause fixed partial dentures (most common to least common) |
1) Caries 2)Endodontic pathology 3) Material wear/Cement failure 4) Loss of abutment teeth |
|
|
What are some factors that may make us sway for implants over fixed partial dentures for tooth replacement? |
• Young patient (18+) • Unrestored dentition • Patient with high caries risk • ↑ Endodontic complications • ↑ Loss of abutment teeth |
|
|
What are some factors that may make us sway for fixed partial dentures over implants for tooth replacement? |
-Older patient -Heavily restored dentition -Teeth already RCT |
|
|
What are the 3 broad categories of implant placement? |
1) Immediate (right after exo) 2) Early (after soft tissue healing 4-8 weeks) 3) Late (beyond 8 weeks) 2&3 are delayed implant placement |
|
|
2 main driving forces behind immediate implant placement? |
1) Reduce tx time 2) improve esthetic outcomes |
|
|
Which types of implant placement (early, late etc.) may need bone subtitute and membrane? |
Immediate and Early |
|
|
Of the different timings of implant placement, which one is the easiest to achieve ideal implant positioning? |
Late |
|
|
How is primary stability achieved in immediate and early implant placement? |
Apical + lateral stabilization |
|
|
Are immediate implants successful? |
They are predictable with only 5-8% lower than delayed implants |
|
|
T/F: Immediate implants are more esthetic because they preserve bone and prevent remodeling of the socket |
False. Remodelling ocurs no matter what and occurs more on the buccal than lingual |
|
|
Are immediate implants more esthetic? |
No definitive evidence to prove this. Many studies find no difference in esthetics of immediate implants versus delayed implants |
|
|
How many mm reduction in buccal-lingual width is observed in a socket post extraction within the first year? |
2.7-5.2mm |
|
|
Which socket sites in the mouth have increased bone loss post exo? |
Molar sites have more loss than non-molar sites |
|
|
How much bone height is lost on average during socket remodeling? |
0.8-0.9mm |
|
|
How much of the remodeling occurs within the first 6 months? |
85% |
|
|
What is a potential consequence of immediate placement of implant without doing any ridge augmentation? |

dehiscence |
|
|
How do we minimize bony remodeling following extraction? |
Use of a bone graft within the socket and an overlying membrane to ensure lack of epithelial or connective tissue downgrowth. In general, it's always good idea to place bone at time of exo. It's easier to preserve bone rather than trying to regain it |
|
|
How much more bone loss is observed in sockets without ridge augmentation procedures compared to those that received it? |
1.6 mm and 2.2 mm greater loss of ridge width and height(respectively) without ridge preservation |
|
|
What is the prognosis of placing an implant in an infected site (due to previous PA pathology)? |
Some evidence says it's possible but make sure you debride the site effectively and rebuild the buccal bone with grafting to achieve primary stability.
|
|
|
What are the different loading protocols for Implants? |
Immediate (within 1 week) post implant placement Early (1-8 weeks) Conventional (>8 weeks) |
|
|
Can you immediately load full arch implant cases? |
Yes but usually it requires multiple long splinted units with x-arch stabilization |
|
|
How are multi-unit cases or single fixture implants typically loaded? |
first immediately restored and then immediately loaded |
|
|
Can you achieve success with immediately loading? |
Yes but there is a high failure rate for inexperienced providers! |
|
|
What are the 3 factors that help with success of immediate loading? |
-Achieving high primary stability >30 Ncm2 - Multiple long splinted units with x-arch stabilization(typically full arch cases) – If single fixtures used (no occlusal loading, ie. non-functional provisional) |
|
|
When is the bone-Implant interface the weakest? |
Most implant failures occurrs within 3-5 weeks following loading |
|
|
Does immediate restoration = improved esthetics throughsculpting/support of tissues during healing? |
Studies Found no differences in interproximal papilla or bone levels inimmediate vs delayed restoration -most important factor was distance from contact point to pre-op bone level on adjacent teeth |
|
|
What is a benefit of immediate restoration? |
Provides a fixed provisional |
|
|
What is the minimum distance between the edges of 2 implants placed side by side? Why? |
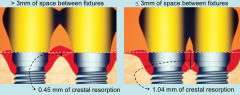
3mm. Less than this and the two remodeling sites will overlap, leading to increased crestal resorption and interproximal bone loss. |
|
|
What is the minimum distance required between a tooth and implant? What is the problem of placing an implant too close to the tooth? |
1.5mm-2mm. Less than this and this is a high risk of losing the interproximal papilla |
|
|
If you were to place a standard platform (4mm in width) implant in a site with neighbouring teeth, what is the minimum mesial distal width required? |
7 mm (1.5+4+1.5) |
|
|
If you were to two standard platform (4mm in width) implants in a site with teeth on either side of the edentulous site what is minimum mesial distal width required? |
14 mm (1.5+4+3+4+1.5) |
|
|
If you were to place a narrow platform (3.3mm in width) implant in a site with neighbouring teeth, what is the minimum mesial distal width required? |
~6.5mm (1.5+3.3+1.5) |
|
|
How far below the buccal gingival is the platform on a single piece fixture implant typically placed? |
1-2mm |
|
|
How far below the buccal gingival is the platform on a 2 piece fixture implant typically placed? |
3-4mm |
|

for a patient with excessive loss of hard/soft tissue loss such as the one shown here, what are some procedures they need before they can receive implants? |
– Vertical ridge augmentation (unpredictable) – Soft tissue grafting (may be multiple) |
|

For the compromised anterior implant case such as the one shown here, what are some keys to success for managing this case? |
– Provision of a wax – up and honest discussion with patient about realistic expectations – Assessment of smile line – Consideration for provision of bridge work instead of single fixtures |
|

Why might be a good idea to consider an implant supported bridge versus single fixture implants in this case? |

Papilla fill is much easier obtain in pontic-pontic situations compared to implant to implant |
|
|
Definition of Implant survival? |
Applies to those implants which are still in function butwhich do not meet (in 1 or more ways) the definedcriteria of implant success |
|
|
Definition of Implant failure? |
When the performance of an implant measured in somequantitative way falls below a specified, acceptable level.(great deal of arbitrariness). In general, mobility is considered failure |
|
|
What are typical rates of implant success from long term studies? |
Machine surfaced implants (oldest type):
70% Maxillary and 76% success rate TiUnite (Nobel), Osseotite and SLA (straumann) have overall success rates of greater than 95% |
|
|
What are the 4 general categories of implant failure? |
1. Biological 2. Mechanical (fractures of the different components) 3. Iatrogenic 4. Inadequate patient adaptation (psychologica |
|
|
What are the two subcategories within Biological implant failure? |
Early: Failure to establish Osseointegration Late: Failure to maintain osseointegration |
|
|
What are 4 reasons for early failures of implants? |
improper preparation of site (surgical) Bacterial Contamination (sterilization) Lack of primary stability Premature loading |
|
|
What are 2 reasons for late failures of implants? |
Excessive load (prosthetics) Infection (perimplantitis) |
|
|
What are the factors that can cause excessive load type failures? |
1) Insufficient bone volume (width + height) 2) Deficient bone quality (density) 3) Occlusal Overload |
|
|
What is the failure rate of implants in the maxilla versus the mandible? |
3X more failures in the maxilla than mandible |
|
|
What are some clinical signs of an early infection after implant placement? |
Swelling Fistulas Suppuration Mucosal Dehiscences None of these are a good sign. |
|
|
What are the four diagnostic criteria for implant failures? |
1) Clinical sign of early infection 2) Pain or sensitivity 3) Mobility (always a clear sign of failure) 4) Radiographic signs (peri-implant radiolucency) |
|
|
What are the 3 diagnostic criteria for a failing implant |
1. Progressive X-ray bone loss (If bone loss is >1.5 mm in 1st year or >0.2 mm everysubsequent year) 2. Clinical signs of late infection (Hyperplastic soft tissues, suppuration, swelling) 3. Probing depth (progressive increase) |
|
|
What are some endogenous factors that impair bone healing or interfere with maintenance of bone healing in implants? |
Age, Systemic Health (diabetes, smoking), Periodontal disease, Bone quality (Grafted/non-grafted, radiation) |
|
|
What are some exogenous factors that contribute to implant failures? |
Operator experience Operator technique + policy |
|
|
How old should a patient be to undergo implant placement? |
-Most important criteria is make sure skeletal and dental growth is completed. (study found eruption occurred even at 19) -Also make sure there is no delayed passive eruption |
|
|
What is the leading causes of implant failure? |
Smoking, but seems to be have less of a negative impact on rough surface implants |
|
|
How does smoking cessation affect chances of implant failure? |
If smokers are able to stop for 1 week prior to implantplacement and continue for 8 weeks afterwards theirimplant failure rate ~ non-smokers |
|
|
Are there higher failure rates in patients with Type II diabetes? |
Maybe, but there are no definitive conclusions from studies yet |
|
|
How do the SURVIVAL rates and SUCCESS rates of patients with treated periodontitis disease differ? |
Survival rates are the same but success rates ARE lower |
|
|
Can you predict success failure in patients who have active periodontitis? |
No predictions can be made to patients withuntreated periodontitis but inferences arestrongly implicated (History of Chronic PDz success rate is 71% but No previous PDz success rate is 95%. Secondly, if you have history of PDz, your chance of Peri-implantitis is 29% but only 6% if you don't have a history of periodontal disease) |
|
|
List the clinical features of Peri-implantitis |
Presence of plaque • Bleeding on probing • Changes in contour and color • Presence of deep probing depths (Progression more important than absolute!) • Radiographic evidence of bone loss |
|
|
What cells are significantly affected by Radiation therapy? |
Bone cells and Blood vessels. The tissues become hypocellular, hypoxic and hypovascular |
|
|
Rank the following in terms of their implant survival rates: irridiated residual bone,non-irradiated residual bone, grafted bone (irradiated residual) |
1. Non-irradiated residual bone = 95% survival 2. Irradiated residual bone = 72% survival 3. Grafted bone (irradiated residual) = 54% survival |
|
|
How many times higher are failure rates of implants performed by inexperienced surgeons compared to those with experience? |
2X |
|
|
Do angulated abutments increase implant failure rates? |
No |
|
|
should you prescribe antibiotics prophylaxis before implant placement? |
no good scientific evidence to recommend or discourage antibiotic prophylaxsis for implant surgery |
|
|
what impact does Chx have on implant failure rates? |
Chx rinse bid for 2 weeks reduces infections by 2.5x. This decreases implant failure rates because early infections increases implant failure rates by 6x. |
|
|
What are the effects of leaving behind cement? |
increased tissue inflammation, abscess and bone loss |
|
|
List some things that can cause overloading of an implant |
Overextended cantilever -Parafunction -excessive premature contacts -Large occlusal table -steep cusp inclination -poor bone density/quality -Inadequate number of implants |
|
|
Does splinting implants improve success rate? |
No human clinical trials demonstrating thatsplinting implant restorations has + long-term effect. |
|
|
Does length of an implant affect implant failure rates? |
-<10mm fail more than >10mm implants -If there is adequate bone: consider putting in >10mm fixtures |
|
|
What is a failing implant? |
An implant that exhibits progressive bone loss, but is still immobile |
|
|
What is Peri-mucositits? |
Reversible inflammatoryreaction to mucosa adjacent to implant |
|
|
What is Peri-implantitis |
IrreversibleInflammatory process additionallycharacterized by loss of peri-implant bone |
|
|
How common is Peri-mucositis? |
50% |
|
|
How common is Peri-implantitis? |
12-25% |
|
|
what is the Peri-mucositis analogous to and what are its clinical features? |
Gingivitis -Presence of plaque - Bleeding on probing -Changes in contour and color -Shallow probing depths - No radiographic evidence of bone loss |
|
|
What is the evidence that peri-mucositits is equivalent to gingivitis? |
Study asked implant patients to stop OH for 3 weeks. Results: 1) Similar amounts of plaque formed on both implants+teeth 2) Composition of plaque formed was similar on both implants+ teeth 3) Resultant inflammatory in filtrate was equal in size on bothimplants + teeth |
|
|
what is the Peri-implantitis analogous to? |
Periodontitis |
|
|
What strain of bacteria are found around implants with per-implantitis? |
Same as those found within periodontitis! -P. ginigvalis -P. intermedia -P.Actinobacillus Aa |
|
|
how do the inflammatory infiltrate differ between peri-implantitis and |
Similar but peri-implantitis the infiltrate is deeper |
|
|
Average value for the biological width for an implant? |
3.8mm GM-JE=2.14mm CT=1.6mm |
|
|
How much How much force should be used when probing implants? |
0.2-0.3N (if you apply the same force on your fingernail, the fingernail should just start to blanch) |
|
|
How much more sensitive are implants compared to teeth when it comes to probing? |
2X |
|
|
How many days does it take for the JE to reattach to the surface of the implant after probing? |
5 days |
|
|
What clinical sign observed around an implant is an indication for systemic antibiotic tx? |
Suppuration |
|
|
What sign found during your clinical exam of an implant is a cardinal sign of inflammation? |
Bleeding on probing (0.25N). Presence of BOP is a good indicator of disease progression around implants. |
|
|
What clinical sign is a good indicator of clinical stability of an implant? |
Absence of BOP |
|
|
What is suppuration at an implant site an indication of? |
active disease destruction. You have a inflammatory mediate destruction of collagen+tissue necrosis that leads to pus formation |
|
|
List the intervals that radiographs should be taken post implant placement |
1) Abutment connection 2) Following crown/bridge installation 3) Within 6-12 months of prosthetic function 4) In intervals of every 2-3 years in asymptomatic patients |
|
|
What are 3 reasons radiographs are a important component of your evaluation of a implant? |
Ensuring maintenance of crestal bone • Evaluation of continued osseointegration • Evaluation for prosthetic complications |
|
|
Although mobility is the definitive test for implant failure, why can it not be used as a stand alone measurement? |
NOT sensitive. You can lose 90% of bone around the implant and it can still be rock solid |
|
|
What are some features of Clinically stable implants? |
-Presence of clinically healthy peri-implant tissues - Absence of Plaque - Absence of BOP - Absence of suppuration - Probing depth ≤ 3mm |
|
|
Why is a deeper PD value (ie. 4-5mm) alone not really indicative of disease in a implant? |
A deep PD might be deliberate because the surgeon placed the platform deeper to achieve a better emergence profile for the restoration. However, really deep probing depths (ie. 10mm) is not good because it's hard to clean. |
|
|
What is the name of the tx protocol that was developed to treat peri-implantitis? |
CIST: Cumulative Interceptive Supportive Therapy |
|
|
What is the hierarchy of CIST tx for implants? |
1) Mechanical Debridement 2) Antiseptic Therapy 3) Antibiotic Therapy 4) Regenerative or resective therapy |
|
|
An Implant has: Plaque and calculus BOP No suppuration PD<3mm and stable. What CIST protocol should you employ? |
CIST Protocol A: Mechanical Debridement |
|
|
What is material is recommended to mechanically debride implants? |
Titanium |
|
|
Implant has Plaque and calculus, BOP positive, Suppuration negative and Probing depths of 5mm. What CIST protocol should be employed? |
CIST Protocol A+B: Mechanical Debridement (A) + Antiseptic cleaning (B). Antiseptic cleaning involves 0.1% CHX gel BID for 3-4 weeks |
|
|
Implant has Plaque and calculus, BOP positive, Suppuration positive and Probing depths of 5mm. What CIST protocol should be employed? |
CIST Protocol A+B: Mechanical Debridement (A) + Antiseptic cleaning (B). Antiseptic cleaning involves 0.1% CHX gel BID for 3-4 weeks |
|
|
Implant has Plaque and calculus, BOP positive, Suppuration positive and Probing depths of >6mm and Radiographic signs of bone loss. What CIST protocol should be employed? |
CIST Protocol A+B+C. C is systemic antibiotic therapy. OR CIST Protocol A+B+C+D D is regenerative or resective therapy. (if CIST protocol ABCD is chosen, infection should be resolved first before doing resection/regeneration) |
|
|
Is re-osseointegration possible with regenerative surgery in failing implants? |
No histological evidence currently demonstrates that this occurs |
|
|
Why is it so hard to detox a implant? |
implants are much more rough and rugged than cementum. The scalers and cavitron will only clean the peaks but not the valleys of the implants. (air embrasure can potentially hit those valleys0 |
|
|
When is CIST protocol E (Extraction) employed for an implant? |
- If implant becomes clinically mobile during active phase of treatment -If peri-implant infection cannot be controlled(Suppuration, BOP, PD ≥ 8 mm, ± pain) |
|
|
How successful is the CIST protocol in treating implants with peri-implantitis? |
ranges from 87-58%. In a study with 26 Perimplantitis cases, 7 ended being extracted 4 lost more bone 9 were unchanged 6 gained bone |
|
|
If a patient lost teeth due to chronic periodontitis and replaced them with implants, how much more likely are they going to get peri-implantitis compared to healthy patients? |
5x more likely |
|
|
Do Patients who have lost teeth due to chronic periodontitis and replaced them with implants have a lower success rate compared to healthy patients?
|
Yes. there is a 11% difference in success rates in patients with a hx of Chronic periodontitis versus healthy patients |
|
|
How do we avoid peri-implantitis in a patient with a history of chronic Pdz? |
1) Complete Perio exam prior to implant 2) Treat the Pdz before the implant! 3) Patients with history of treated periodontal disease that nowhave a stable peridontium should be maintained closely |
|
|
In a 10 year study that looked at implants in chronic PDz versus healthy patients, was there a difference in cumulative bone loss? |
Yes. Periodontitis patients lost an average of 1.7mm while only 0.7mm in healthy patients. |
|
|
In a 10 year study that looked at implants in Generalized aggressive periodontitis versus healthy patients, was there a difference in cumulative bone loss and success rate? |
Yes. -Aggressive perio lost 3.37mm of bone while healthy patients lost 1.24mm -Implant survival rates were only 83% for aggressive PDz compared to 100% for healthy patients |
|
|
Which implant patients should be placed on a 3 month recall frequency? |
-Patients with some risk factors and/or a history ofperiodontal disease -Patients with a history of peri-implant diseases |
|
|
Which implant patients should be placed on a 6 month recall frequency? |
No hx of PDz, single or multiple fixtures |
|
|
What cells do Osteoblasts become once they are trapped in their newly formed bone matrix? What is the name of the connection between a Osteophyte and Osteoblast? |
Osteocytes. They connect to Osteoblast by canaliculus |
|
|
What happens to the osteoblasts after distant osteogenesis occurs? |
They die a horrible death. The process of making bone cuts off their own blood supply. |
|
|
What is the cement line in osteogenesis and where do you see it? |
Cement line is a calcium collagen free matrix that seperates old bone from new bone. It is seen on the surface of the implant |
|
|
what are the first things that bind to the surface of an implant. What do they release? |
Platelets. They release cytokines and growth factors such as : 1) platelet derived growth factor 2) transforming growth factor beta 3) Neutrophil activating peptide. |
|
|
what on the implant activates the platelets to release cytokines? |
The Implant surface topography. The smaller the topography, the more activation of platelets there is |
|
|
What is activated as a result of the release of the cytokines from the platelets on the implant surface? |
White blood blood cells and other platelets in the periphery of the implant are activated. |
|
|
What directs the Osteogenic progenitor cells to find its way to the surface of the implant? |
The density gradient of cytokines generated by platelets. The concentration of cytokines gets larger as you get closer and closer to the surface of the implant. They travel to the site via a fibrin network created by the blood clot |
|
|
What is critical for osteoblasts in order for them to maintain their metabolism? |
Angiogenesis and blood supply
|
|
|
What is generated within the fibrin network as the Osteoprogenitor cells migrate along it to the implant surface? Why is this important? |
Tension and stress. Therefore, it is important the fibrin be firmly attached to the implant surface. If not, then Osteogenic cells movement can cause detachment of the connection between the implant and the fibrin. |
|
|
What happens to the Osteogenic cells reach the implant surface after migration from the periphery? |
They differentiate into osteoblasts |
|
|
What is the most important factor dictating how strong the adhesion is between the fibrin network and the implant? |
The Implant topography.. likely why SLA (rough) implant has earlier implant stability than Turned implants because you have higher degrees of contact osteogenesis. |
|
|
Is there a difference in the final bone pattern on the surface of SLA and Turned implants? |
No. They are indistinguishable once healing is complete |
|
|
Why might Single piece implant designs not get as much crestal remodeling compared to 2 piece fixtures? |
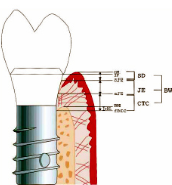
Single piece implants have a microgap placedmuch higher up than two piece fixtures. -This is because the transmucosal component ofimplant attached to fixture. |
|
|
When placing an single piece implant, what is the expected distance between the marginal of the restoration and the crest of the alveolar bone post resorption? |
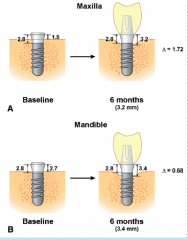
Around 3mm (ie. 3.2mm in the maxilla and 3.4mm in the mandible) |
|
|
Why is understanding the biological width of implants important? |
-You need to be able to predict where your bone levels post implant restorations is going to be! -You always need to anticipate osseous resorption and soft tissue recession especially interproximally in the anterior region. |
|
|
What is the mean papilla height between Tooth to implant? |
4.2mm |
|
|
What is the mean papilla height between implant to implant? |
3.4mm |
|
|
What is mean papilla height between implant and pontic? |
5.5mm |
|
|
What is the mean papilla height between pontic and pontic? |
6mm |
|
|
Patient missing 11 and 21 and wishes to have implants to replace them. Patient is a thin biotype with triangular shaped teeth. What should you be concerned about and what is the only option you can do to prevent it? |

You're worried about formation of a black triangle because of the poor papilla fill between implants and implants. Your only choice is to have a long contact connector. |
|
|
2 piece implants have higher osseous remodeling. What are some ways to decrease amount or remodeling? |
1) Concept of Platform switching 2) Scalloped Implant design (mimics morphologyof CEJ) |