![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
31 Cards in this Set
- Front
- Back
|
Properties of muscle |
Contractility - ability to shorten Excitability - capacity to receive/respond to stim Extensibility - ability to stretch (passive) Elasticity - ability to return to original shape
|
|
|
Functions of muscle |
production of movement Maintaining posture stabilizing joints Generating heat |
|
|
Epimysium |
connective tissue surrounding muscle |
|
|
Perimysium |
connective tissue surrounding muscle fascicles (muscle bundles |
|
|
Endomysium |
connective tissue surrounding muscle fibers |
|
|
Myofibril contractile proteins |
Generated force during contraction
Actin & Myosin |
|
|
Myofibril regulatory proteins |
initiate and terminate contraction
Troponin & tropomyosin |
|
|
Myofibril structural proteins |
maintain alignment, elastic & extensible
Titin, Myomesis, Dystrophin |
|
|
Type I muscle fibers |
Slow oxidative muscle fibers small diameter Lots of capillaries, mitochondria, myoglobin and fat Not much glycogen and creatinine Red meat Aerobic ATP generation Low contraction velocity Primary function postural and endurance |
|
|
Type II A muscle fibers |
Fast Oxidative-Glycolytic Lots of capillaries, mitochondria, myoglobin and fat Somewhere in the middle for glycogen and creatinine Middle ground for ATP Aerobic and glycolysis to generate ATP Primary function sprinting, walking
|
|
|
Type II B muscle fibers |
Fast glycolytic Large diameter few capillaries, mitochondria, myoglobin, fat Lots of glycogen and creatinine kinase White meat generate ATP via glycolysis Use ATP quickly Primary function short term work
|
|
|
What is the sarcoplasmic reticulum? |
Only found in muscle cells Wraps around the T tubules and is where Ca2+ stored and released from after action potential. - 2 terminal cisternae + T tubule = triad cisternae have Calesquestrin - sequestors of Ca2+ |
|
|
Sarcomere anatomy |
Functional unit of muscle - region between two Z lines. 1. A band - composed of thick and thin myofilaments. H zone is only thick filaments, M line contains myomyesin. Titin anchors thick filaments to Z and M lines. 2. I band - composed of thin filaments 3. Z line - anchors thin filaments (Actinin and Nebulin).
|
|
|
Myofilaments |
Thick: composed of myosin - tail (light meromyosin) and head and cross bridges (heacy meromyosin
Thin: composed of Actin (F&G), Troponin (TIC subunits) and Tropomyosin (wraps around F actin) |
|
|
Major differences between cardiac and skeletal muscle |
Fibers are enucleated, branched, and rich in mitochondria and lipids in cardiac. Cardiac have intercalated discs with gap junctions (allows AP to travel between cells so act together) - functional syncytium Cardiac muscle slower to contract than skeletal |
|
|
Major differences in smooth muscle |
Not striated b/c no myofibrils (actin and myosin loosely organized. Slow prolonged contractions No T-tubules, SR poorly developed so have special gated Ca2+ channels instead Actin hooked into dense bodies Can be multi unit (like skeletal with individual innervation; eye) or single units (like a sheet connected by gap junctions so AP rapidly propogated; GI) |
|
|
Anatomical muscle comparison of three types |
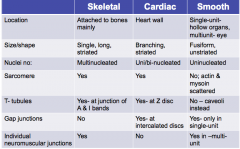
|
|
|
Functional comparison of muscles |
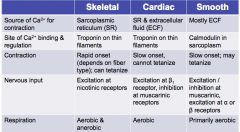
|
|
|
Describe excitation-contraction coupling |
1. Action potential propagates along sarcolemma and down the T tubules. 2. Depolarization opens up/conformational change in DHP receptor in T tubule 3. DHP opening linked/gated to opening of ryanodine receptor in SR. 4. Changes in ryanodine allow for Ca2+ to release from SR. 5. Ca2+ bind troponin > changes tropomyosin > active sites on actin exposed 6. Formation of cross bridges between myosin (ADP + Pi) and actin > Pi released > power stroke 7. Ca2+ removed back to SR 8. Tropomyosin block active sites on actin |
|
|
How does muscle length/tension relationship affect skeletal muscle contraction? |
The further the muscle was stretched or shortened from optimum resting length, the less tension it is capable of applying. Optimum force can be applied when the most number of myosin heads can be in contact with actin filament. When stretched, fewer myosin heads will be in contact with actin filament. When contracted, actin filaments hit the z-line and can't be contracted anymore. |
|
|
How does the force/load -velocity relationship affect muscle contraction? |
With no load can contract quickly, with load will be slower b/c resistance. Load where V=0 |
|
|
Isotonic contraction |
Muscle contracts and produces movement e.g., push up
concentric - dec in muscle length (cross bridges formed btw actin and myosin) -e.g., E2 of step cycle eccentric - inc muscle length -e.g., E3 of step cycle or walking down a steep incline controlling rate of elongation as stretching to next location |
|
|
Isometric contraction |
muscle contracts but produces no movement e.g., holding a plank, postural muscles (maintain body position while opposing gravity) |
|
|
Treppe - wave sumamtion - tetanus |
1. Treppe: muscle stimulated 2nd time imm. after relaxation of 1st phase which inc tension b/c Ca2+ not fully sequestered by SR. 2. Summation: 2nd stim before complete relaxation, 2nd twitch causes greater tension b/c superimposed 3. Incomplete tetanus: individual twitches are distinguishable 4.Complete tetanus: individual twitches indistinguishable b/c no relaxation phase |
|
|
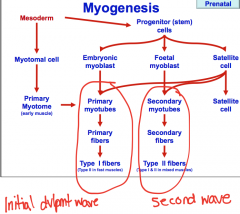
Describe myogenesis |
|
|
|
How does nutrition impact muscle development? |
-All myofibers there from fetal 6 mos+, no new ones -If decrease nutrition during secondary myogenesis (3-6 mths) see decreased myogenesis so fewer fibers for life. -If adequate nutrition later can compensate a bit with muscle hypertrophy but no myogenesis
|
|
|
Muscle hypertrophy |
Double muscling Myostatin mutation so doesn't inhibit muscle hypertrophy and hyperplasia |
|
|
Neurogenic muscle atrophy |
denervation > lysosomal protein degradation > 50% dec muscle mass and EMG abnormalities Fairly immediate compared to myogenic atrophy e.g., Sweeney in horses |
|
|
Myogenic muscle atrophy |
malnutrition, cachexia (weight loss secondary to disease), corticosteroid excess Slow progression, normal EMG (effects at level of muscle mass not innervation), atrophy only type II fibers |
|
|
Muscle necrosis or Rhabdomyolosis or tying up |
-Clinical features: muscle pain, contracture, high RR and sweating; high creatinine kinase & aspartate transaminase in serum, coffee coloured urine -Causes: deficiency of Vit E and selenium, infectious, immune mediated, metabolic |
|
|
Muscular dystrophy |
deficiency in dystrophin which anchors sarcolemma to actin cytoskeleton - don't have anchors so muscle paresis |