![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
53 Cards in this Set
- Front
- Back
|
Motor System |
There are parallel circuits that flow up and down through the system (it is hierarchical) Sensory feedback and feedforward are crucial for modulating the output of the motor system |
|
|
Sensorimotor Spinal Circuits |
Consists of Muscle, neuromuscular junction It is the lowest level of hierarchy = motor unit = where motor neurone and muscle fibres it innervates. Ach is the neurotransmitter |
|
|
Muscle |
Muscle fibres with membrane attach to tendon, which pulls the bone |
|
|
Neuromuscular Junction |
Point of Innervation |
|
|
Descending Motor Pathways |
Signals descend to muscles through pairs of Dorsolateral Tracts and pairs of Ventromedial Tracts in spinal cord |
|
|
Dorsolateral Tracts |
Terminate in contralateral half of one spinal cord segment and sometimes directly on motor neurone Two Types: Corticospinal and Corticorubrospinal Important for movements of limbs and independent movement for fine tune |
|
|
Corticospinal Tracts |
Direct Tracts in Dorsolateral System that go from motor cortex and go straight to distal limb muscles - they cross over at the medullary pyrmaid |
|
|
Cortocorubrospinal Tracts |
Indirect Tracts in Dorsolateral System that go through red nucleus (where they cross over), some leave to control controlateral facial muscles, via the nuclei of cranial nerve, others go to distal limbs |
|
|
Lawrence & Kuypers (1968) Transecting dorsolateral tracts in Monkeys |
After transecting dorsolateral corticospinal tracts in medullary pyramids monkeys could stand, walk and climb but could not use limbs for activities i.e. reaching for objects |
|
|
Ventromedial Tracts |
More diffuse with axons innervating interneurones in several segments of spinal cord Two Types: Ventromedial Corticospinal and Cortico-brainstem-spinal |
|
|
Ventromedial Corticospinal |
Direct tracts in Ventromedial system: from primary motor cortex they are ipsilateral and diffusion doesn't occur until the spinal cord They activate proximal (close muscles) like thighs Important for posture and whole-body movements |
|
|
Cortico-brainstem-spinal |
Indirect tracts in Ventromedial system, they stop at the tectum (reticular formation) where they diffuse and have bilateral representation |
|
|
Lawrence & Kuypers (1968) Transecting ventromedial tracts in Monkeys |
After transecting ventromedial tracts, monkeys had postural abnormalities and impaired walking/sitting. |
|
|
Cerebellum |
Important for sequencing, orientation, and navigation, fine tune movement, balance and learning functions Takes input from primary and secondary motor cortex Feedbacks from motor responses from somatosensory and vestibular systems |
|
|
Cerebellar Ataxia |
Fine tune walking is destroyed - more shaky for fine tune movement rather than when not moving. |
|
|
Basal Ganglia |
Complex heterogeneous interconnect nuclei - this makes it a highly interconnected with nuclei that work together in own individual way Modulates movement and cognitive functions including habitual responses and implicit learning |
|
|
Feedback loop of Basal Ganglia |
It is an ongoing feedback/feedforward loop that has two pathways Direct: Selection of actions that goes straight to the thalamus (just excitation) Indirect: Inhibition of actions, that has multiple pit stops, so many nuclei are involved (has a balanced system of excitation and inhibition) Basal Ganglia > Thalamus > Supplementary Motor Area > Primary Motor cortexs |
|
|
Putamen |
Putamen receives signals from Substantia Nigra, which produces dopamine Putamen has two dopamine receptors D1 = excitation = Direct D2 = inhibition = Indirect |
|
|
Parkinson's Disease |
Imbalance between the activation of nuclei in the intact system of basal ganglia which leads to extra or reduce movements Loss of Neurones and Pigmentation |
|
|
Indirect Connections from Basal Ganglia |
The output of one nucleus either excites (enhances) or inhibits (suppresses) the output of the next nucleus in the system |
|
|
Positive Symptoms of Parkinson's Disease |
Symptoms that you see that shouldn't be there Tremor at resting - disappears when use limb Rigidity - resistance to passive movement = postural problems Rigidity + Tremor = cogwheel Forward/Backward Leaning Postural Hypotension = many falls |
|
|
Negative Symptoms of Parkinson's Disease |
Hypokinesia: Reduction in spontaneous movement Akinesia: Slow initiation of movement Progressive slowing or freezing during movement Reduction of range and scale of movement Dull weak voice with no inflections (hypophonia) Unemotional Expression |
|
|
L-Dopa Side Effects |
Disorientation Affect Auditory/Vision Hallucinations Poor working memory Paradoxical Movement Problems Dyskinesias at peak dose End -of-dose dysfunction On-off cycles Freezing Eventual drug failure |
|
|
Huntington's Disease Components |
Hereditary Nature: Autosomal dominant with complete lifetime penetrance, chromosome 4 Manifestation in Adulthood Tendency to 'insanity and suicide' |
|
|
Huntington's Disease Neurological Components |
Destruction of GABAergic/cholinergic within caudate and putamen Progressive striatal atrophy Defective Metabolism precedes loss of tissue |
|
|
Signs of Huntington's Diseas |
First: Depression, anxiety, irritability, impulsivity and aggression Then: Restlesness/poor coordination Altered Speech Bradyphrenia and Bradykinesia Poor motor/reduced speed Athetosis, Chorea |
|
|
Athetosis, Chorea |
Often appear to be fragments of normal behaviour, that look voluntary but are actually involuntary Increase with stress and voluntary movements Quasi-undulating character is idiosyncratic to individuals |
|
|
Neuropathology of Huntington's Disease |
The caudate nucleus shrinks to a sharp thin strip, below the ventricle; there is ventricular enlargement |
|
|
Tourettes |
Affects: Motor and Verbal, otherwise normal sensory and cognition Effects: Echolalia, Coprolalia, involuntary (worse under stress), partly suppressible, sleep deprivation increases, premonitory sensory phenomena Causes: Genes and environment Imbalance of GABA in basal ganglia Management when severe |
|
|
Cortical Areas involved in Tourettes |
Before tic onset: mesial and lateral pre-motor activation At tic onset: sensorimotor including superior parietal lobe activation Plus basal ganglia |
|
|
Primary Motor Cortex |
Located: Precentral Gyrus of Frontal Lobe Major hub of convergence of cortical motor signals and outgoing point of signals Mapped by homunculus |
|
|
Hemiplegia |
Damage to Primary Motor Cortex Results in weakness (loss of power) in the body part represented by that site on body map |
|
|
Secondary Motor Cortex |
Input from association cortex Output to primary motor cortex Consists of: preSMA Dorsal and Ventral Premotor 3 x cingulate motor areas Programming of specific patterns of movement |
|
|
Sensorimotor Association Cortex Input |
Posterior Parietal Lobe Input from more than one sensory system: integrations knowledge of position of objects, position of body parts and direct attention Damage: results in ataxia and impaired body representation |
|
|
Sensorimotor Association Cortex Ouput |
Posterior Parietal Lobe Output to Dorsolateral prefrontal association cortex, secondary motor cortex and frontal eye fields Damage: results in apraxia and contralateral neglect |
|
|
Dorsolateral Prefrontal Association Cortex |
Involved in decision to make an action - not the action itself and not processing the target Input: Posterior parietal cortex Output: Secondary motor, primary motor, and frontal eye fields |
|
|
Ataxia |
Inability to use visual information Deficit is more severe in periphery of visual field Visual fixation preserved Results in: Awkward or incorrect movements and errors in accuracy |
|
|
Patient AT and Ataxia |
Had a stroke Had to reach out to dots whilst fixating on centre dot Deficit more severe in periphery of visual field and often over/undershot |
|
|
Apraxia |
Inability to act in a meaningful/purposeful way A disorder of skilled movement resulting from neurological dysfunction |
|
|
Intrinsic Spatial Coding |
Knowing what our own body parts are doing is essential when a body part is obscured from vision during planning and execution of movement |
|
|
Wolpert, Goodbody & Husain (1998) Maintaining Internal Representations |
Patient had head injury and had cyst enroaching on cortex - there was no visual neglect or extinction - on left superior parietal lobe Complaint: perceives her right arm and leg to drift and fade unless she is able to see them So in bed - loss of limb position knowledge Conclusions: Superior Parietal Lobe is critical for sensorimotor integration by maintaining an internal representation of body's state |
|
|
Components of Motor Control System |
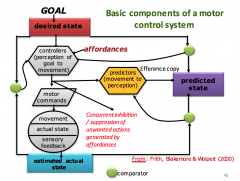
Desired, predicted and estimate state talk via comparator Efference copier: know you have touched your own skin Affordances = environment evokes action Inappropriate actions are suprressed |
|
|
Affordances |
Controllers (perception of goal to movement Links to motor commands and predictors (efference copy) |
|
|
Efference Copy |
Predictors of movement to perception Links to predicted state |
|
|
Why can't you tickle yourself |
Because of the efference copier, you know you are about to touch yourself so you are prepared for it |
|
|
Anarchic Hand Syndrome |
Can't suppress the actions of the hand There is no connection between goal and affordances, so there is no efference copy to go to parietal lobe (it is unexpected) Activation of actions by irrelevant affordances which are not suppressed by intended actions |
|
|
Mirror Neurone System |
A basis for action comprehension and action imitation The action observation system William James - every mental representation of a movement awakens to some degree the actual movement which it is object |
|
|
Gallesse, Rizzolatti et al. (1980) Mirror Neurones in Monkeys |
They respond to sight of only goal-directed actions, as long as the goal is achieved (even out of sight), to sound of an action and when action is performed by hands but not tools Premotor and Parietal Cortices activated by perception and greater activation when replicating movement Allows for understanding and planning of actions |
|
|
Gallesse, Rizzolatti et al. (1980) Mirror Neurones in Monkeys Physical Results |
Did not occur when used pliers Delayed execution Activated when sees the action even when behind screen, but not when there is no object there |
|
|
Mirror Neurones in Humans |
If you give people time to learn about pliers/robots then people can learn/elicit the action context matters experience matters indivudal differences matter |
|
|
Lahv, Saltzman and Schlaug - Newly acquired actions |
Hearing - doing system that is highly dependent on the individuals motor repertoire Used trained (knew how to play) and untrained music sequences Frontoparietal motor regions were observed in trained but not when untrained Activation was more active during listening of trained music than untrained |
|
|
Influence of Visual and Motor Familiarity in Action Observation |
Experience-Specific - movements are not goal-directed but they are meaningful e.g. dances have meaning of the final body position of the people doing the moves |
|
|
Mirror Neurons and Robots |
Humans can respond to 'robotic' stimuli as well as other humans if we have experience with those stimuli |