Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
124 Cards in this Set
- Front
- Back
|
What are 7 aspects that can be used to figure out the etiology of a tumor
|
-pt age
-location -CT/MR characterisitic -MR signal characteristic -Enhancement -Mass effect -Multiplicity |
|
|
What 3 aspects about location can help determine what type of tumor
|
intra Vs extra
compartment midline crossing |
|
|
What are 3 CT/MR characteristics that can narrow down a tumor type
|
fat, cystic, calcification
|
|
|
What is meant by signal characterisitc
|
T1, T2, DWI
|
|
|
What is the signal characteristic of most brain tumors
|
low on T1 and high on T2
|
|
|
What is the rough approximation of percentage of mets, glioma and non-glial brain tumors
|
33% each
|
|
|
What are the types of glial cells
|
astrocytes, oligodendrocytes, ependymal and choroid plexus cells
|
|
|
What are the main subdivisions of astrocytes
|
Astrocytoma is the most common glioma and can be subdivided into the low-grade pilocytic type, the intermediate anaplastic type and the high grade malignant glioblastoma multiforme (GBM)
|
|
|
What is the most common astrocyte
|
GBM is the most common type (50% of all astrocytomas).
|
|
|
What is the most common glial cell
|
astrocytoma
|
|
|
What is the most common non-glial cell
|
meningioma
|
|
|
What are 3 tumors that tend to occur under 2 years of age
|
Specific tumors occur under the age of 2, like choroid plexus papillomas, anaplastic astrocytomas and teratomas
|
|
|
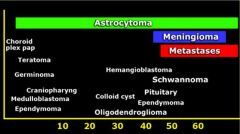
What are the tumors by age
|
|
|
|
What tumors are common during the first decade of life
|
In the first decade medulloblastomas, astrocytomas, ependymomas, craniopharyngeomas and gliomas are most common,
|
|
|
What is rare during the first decade of life
|
mets
|
|
|
What is the MC mets in the first decade of life
|
When they do occur at this age, metastases of a neuroblastoma are the most frequent
|
|
|
What makes up 50% of all CNS lesions in adults
|
mets (notice how since it is less in children it balances out and is 33% overall)
|
|
|
What are the common tumors of adults
|
Other common tumors in adults are astrocytomas, glioblastoma multiforme, meningiomas, oligodendrogliomas, pituitary adenomas and schwannomas.
|
|
|
What is tumor that will occur at any age
|
Astrocytomas occur at any age
|
|
|
What is a tumor that tends to occur in older adults and elderly
|
mets
|
|
|
What is the 3rd most common cancer after leukemia and lymphoma in children
|
primary brain tumors (as a group)
|
|
|
Where do most tumors occur in children
|
Most of the tumors in children are located infratentorially
|
|
|
What are the common infratentorial tumors in children
|
Juvenile pilocytic astrocytoma
PNET (meduloblastoma) Ependymoma Brainstem Astrocytoma |
|
|
What are the common supratentorial tumors that occur in children
|
astrocytoma
pleomorphic astrocytoma PNET DNET Ganglioglioma |
|
|
Do the mets make up 50% of adult brain tumor of which 50% are solitary
|
yes
|
|
|
Where do mets MC appear
|
infratentorial
|
|
|
What are the 2 MC infratentorial cancers in adults
|
hemangioblastoma
mets |
|
|
What are the MC supratentorial cancers in adults
5 |
mets
gliomas (fibrillary astrocytoma, anaplastic astrocytoma, GBM, oligodendroglioma) |
|
|
What 2 tumors make up 80% of extra-axial tumors
|
meningioma and schwannoma
|
|
|
What percent of intra-axial tumors in an adult are mets or astrocytoma
|
75%
|
|
|
Name 6 signs of an extra-axial tumor
|
CSF cleft
Displaced subarachnoid vessels Cortical gray between mass and white matter Displaced and expanded SA space Broad dural tail Bony reaction |
|
|
What extra-axial tumors tend to cause bony changes
|
Bony changes are seen in bone tumors like chordomas, chondrosarcomas and metastases
|
|
|
Can bony change occur from secondary change by a meningioma
|
yes
|
|
|
Why do most extra-axial tumors enhance avidly
|
Extra-axial tumors are not derived from brain tissue and do not have a blood-brain-barrier, so most of them enhance homogeneously
|
|
|
How do astrocytomas spread
|
Astrocytomas spread along the white matter tracts and do not respect the bounderies of the lobes
|
|
|
If you see a 4th ventricle tumor in a child extending through the foramina what should you suspect
|
ependymoma
|
|
|
What is a characteristic spread of a oligodendroglioma
|
Oligodendrogliomas typically show extension to the cortex
|
|
|
Some tumors show subarachnoid seeding and form tumoral nodules along the brain and spinal cord. What tumors do this
|
This is seen in PNET, ependymomas, GBMs, lymphomas, oligodendrogliomas and choroid plexus papillomas
|
|
|
What are PNET
|
Primitive neuroectodermal tumours (PNET) form a rare group of tumors, which develop from primitive or undifferentiated nerve cells
|
|
|
What are 2 common types of PNET
|
These include medulloblastomas and pineoblastomas
|
|
|
What tends to have more mass effect; primary or mets
|
mets
|
|
|
What is the ddx of tumors that cross the midline
5 |
GBM
Radiation Necrosis Meningioma Lymphoma Epidermoid Cyst MS |
|
|
What are some common causes of multifocal brain lesions besides Mets
|
Lymphoma
Multicentric GBM Gliomatosis Cerebri |
|
|
What are the causes of brain tumors that can seed and therefore be multifocal
|
medulloblastomas (PNET-MB), ependymomas, GBMs and oligodendrogliomas
|
|
|
What condition may result in menigioma and schawnomas to become multible
|
NF 2
|
|
|
What tumors are seen in NF 1
|
optic glioma and astrocytoma
|
|
|
What tumors are seen in NF 2
3 |
meningioma
ependymoma choroid plexus tumors (schwannoma?) |
|
|
What tumors are seen in TSC
3 |
subependymal tubers, intraventricular giant cell astrocytomas, ependymomas
|
|
|
What tumor is seen in VHL
|
hemangioblastomas
|
|
|
Why does a tumor being located in the gray matter help narrow the differential ddx
|
because most tumors are located in the white matter
|
|
|
What is the ddx of a tumor in the grey matter
3 |
oligodendroglioma, ganglioglioma and Dysembryoplastic Neuroepithial Tumor (DNET)
|
|
|
What is a DNET and where is it commonly located
|
A DNET is a rare benign neoplasm, usually in a cortical and temporal location.
|
|
|
What is the MC presentation in patients with cortically based tumors
|
seizures
|
|
|
An infiltrative mass with calcification that extends to the cortex
|
oligodendroglioma
|
|
|
What are the most common brain tumors that contain fat
3 |
lipomas
dermoid cysts teratomas |
|
|
Name 3 tumors that may have high density on CT
|
lymphoma, colloid cyst and PNET-MB (medulloblastoma).
|
|
|
Do oligodendrogliomas always have calcification
|
yes
|
|
|
What is the ddx of a calcified intra-axial brain mass
|
oligodendroglioma
astrocytoma mets ependymoma choriod plexus papilloma ganglioglioma |
|
|
What are the 3 most commonly calcified brain tumors
|
oligo...
ependymoma ganglioglioma |
|
|
Does a pineocytoma calcify
|
No, A pineocytoma itself does not calcify, but instead it 'explodes' the calcifications of the pineal gland.
|
|
|
Calcified mass in the suprasellar region
|
craniopharngioma (not in previous ddx)
|
|
|
Describe a craniopharyngioma
|
Craniopharyngiomas are slow growing, extra-axial, squamous epithelial, calcified, cystic tumors arising from remnants of Rathke's cleft
|
|
|
What are 5 lesions that are cystic and can simulate a CNS tumor
|
These include epidermoid, dermoid, arachnoid, neuroenteric and neuroglial cysts
|
|
|
What is a way to differentiate an arachnoid cyst from a necrotic (cystic) tumor
|
Tumor necrosis may sometimes look like a cyst, but it is never completely isointense to CSF.
|
|
|
Do craniopharyngiomas have an enhancing rim
|
yes
|
|
|
Can a high protein cyst be bright on T1
|
yes
|
|
|
What are 2 reasons brain tumors tend to have increased signal on T1
|
hemorrhage or melanin in the case of mets
|
|
|
Why are most tumors bright on T2
|
due to a high water content
|
|
|
What cause tumors to be dark on T2
|
When tumors have a low water content they are very dense and hypercellular and the cells have a high nuclear-cytoplasmasmic ratio.
|
|
|
What are 2 examples of tumors that are dark on T2 because of high cellularity
|
CNS lymphoma and PNET
|
|
|
Do cns lymphoma and PNET appear bright on CT
|
yes
|
|
|
What is the usual appearance of calcification on T2
|
dark
|
|
|
What is the appearance of hemosiderin on MRI
|
dark
|
|
|
Can protieinacious material be dark on T2 imaging
|
yes
|
|
|
What is an example of a proteineous cyst that is dark on T2
|
colloid cyst
|
|
|
What is an example of a tumor that has flow voids (dark on T2)
|
hemangioblastoma (VHL)
|
|
|
What are causes of tumors with low signal on T2
|
hypercellular
flow void melanin certain proteinaceous material certain phases of hemorrhage calcification mucinous mets |
|
|
Does mucinous mets have low signal on T2W images
|
yes
|
|
|
Can meningiomas be either high or low signal on T2
|
yes, depending on cellularity and amount of calcification
|
|
|
What does high intensity on DWI indicate
|
fluid restriction
|
|
|
Name 3 causes of restricted diffusion in the brain
|
abscesses, epidermoid cysts and acute infarction (due to cytotoxic edema).
|
|
|
What is the cause of restricted diffusion of an abscess
|
In cerebral abscesses the diffusion is probably restricted due to the viscosity of pus, resulting in a high signal on DWI.
|
|
|
Do tumors usually have restricted diffusion
|
no
|
|
|
Can perfusion imaging play an important role in malignancy grade
|
yes
|
|
|
What is perfusion dependent on
|
the vascularity of the tumor and not the blood brain barrier
|
|
|
What shows greater association with the grade of malignancy; enhancement or perfusion
|
perfusion
|
|
|
What is the only way contrast leaks into the brain
|
if the blood brain barrier is broken down when a tumor destroys it
|
|
|
Why do extra-axial tumors tend to enhance
|
they are not from the brain tissue and therefore do not have a BBB
|
|
|
What intra-axial tumors commonly enhance
5 |
high grade glioma
low grade glioma (ganglioma, pilocytic astrocytoma) lymphoma mets |
|
|
What low grade gliomas enhance
|
gangliolioma
pilocytic astrocytoma |
|
|
What non-tumours lesion enhance
|
infections, demyelinating diseases (MS) and infarctions.
|
|
|
Does contrast enhancement illustrate the full entension of a tumor
|
no, it wont tumor cells will be found beyond the enhancing margins
|
|
|
In gliomas does enhancement usually indicate a higher degree of malignancy
|
yes
|
|
|
What is a sign of malignant transformation of a low grade glioma
|
enhancement of followup imagin
|
|
|
What is the optimal timing for delay on contrast in brain tumors
|
The optimal timing is about 30 minutes and it is better to give contrast at the start of the examination and to do the enhanced T1WI at the end
|
|
|
What tumors do not enhance
|
low grade astrocytomas
cystic (dermoid, epidermoid, arachnoid cyst) |
|
|
What type of tumors tend to have homogenous enhancement
8 |
Metastases
Lymphoma Germinoma and other pineal gland tumors Pituitary macroadenoma Pilocytic astrocytoma and hemangioblastoma (only the solid component) Ganglioglioma Meningioma and Schwannoma |
|
|
What tumors tend to have patchy enhancement
|
Metastases
Oligodendroglioma Glioblastoma multiforme Radiation necrosis |
|
|
Do GBMs have variable enhancement and heterogeneity on both T2WI and FLAIR.
|
yes
|
|
|
What brain tumors will have ring enhancement
|
Ring enhancement is seen in metastases and high-grade gliomas.
|
|
|
What are the causes of ring enhancement
|
mets
abscess glioma infection chronic hematoma demyelating disease radiation |
|
|
Is leptomeningeal enhancement easy to see on T2
|
NO, only possible to see with T1 plus gad
|
|
|
What are the common skull base brain tumors
|
chordoma
chondrosarcoma esthesioneuroblastoma lymphoma mets myeloma paraganglioma sinonasal carcinoma |
|
|
What is a good way to differentiate a skullbase chordoma from a chondrosarcoma
|
Chordomas will be midline where as chondrosarcomas will be off midline
|
|
|
Is a metastatic lesion a common skull base lesion
|
yes
|
|
|
What would cause lytic destruction of the skull base off midline by the jugular bulb
|
a paraganglioma
|
|
|
Is the normal clivus (bone) bright or black on T1W images
|
bright because of the fatty bone marrow
|
|
|
What are the common sella/suprasellar masses
|
S
Schwannoma sphenoid sinus tumor A aneurysm / adenoma of pituitary T teratoid lesion C craniopharyngioma H hypothalamic glioma / histiocytoma M meningioma / mets O optic glioma |
|
|
Beside SATCHMO what other tumors can be found in the sella/suprasellar region
7 |
Dermoid
Epidermoid Germinoma Rathkes Cyst Hamartoma Arachnoid Cyst Chordoma |
|
|
What is the MC suprasellar lesion
|
craniopharyngioma
|
|
|
Do craniopharyngiomas have a cystic component and variable amounts of peripheral enhancement and calcifications
|
yes
|
|
|
What is a common complication of a suprasellar lesion
|
hydrocephalus
|
|
|
Would you expect to see an inferior displaced normal appearing pituitary gland in a patient with a pituitary macroadenoma
|
no
|
|
|
What are 6 common CP angle tumors
|
schwannoma
meningioma epidermoid arachnoid cyst paraganglioma mets |
|
|
Can a schwannoma be cystic
|
yes
|
|
|
What are the common pineal region tumors
|
pineocytoma
GCT PNET Tectal Glioma Meningioma Dermoid Arachnoid cyst |
|
|
What are the common intraventricular tumors
|
Ependymoma
Subependymoma Choroid Plexus Papilloma Central Neurocytoma Colloid Cyst Meningioma Giant cell astrocytoma |
|
|
What are the most common tumors of the 4th ventricle in children
4 |
astrocytoma
medulloblastoma ependymoma brainstem glioma with dorsal exophytic extension |
|
|
What are the MC adult 4th ventricle tumors
|
Metastases are most frequently seen, followed by hemangioblastomas, choroid plexus papillomas and dermoid and epidermoid cysts.
|
|
|
What percent of ependymomas are supratentorial
|
1/3 supratentorial, majority periventricular WM
|
|
|
Is calcification of a ependymoma common
|
yes they can calcify(50%)
|
|
|
Can ependymomas have cyst and hemorrhage
|
yes
|
|
|
Ependymoma signal
|
MR: iso to hypo T1, iso to hyper T2
|
|
|
Ependymoma enhancement characteristics
|
Enhances heterogeneously
|