![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
85 Cards in this Set
- Front
- Back
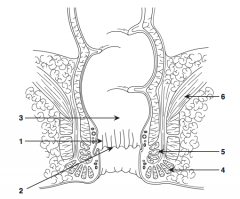
What is structure 1?
|
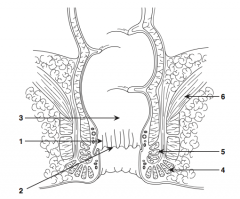
Anal columns |
|
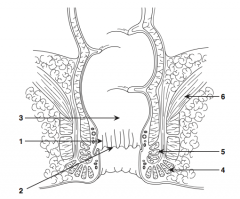
What is structure 2?
|
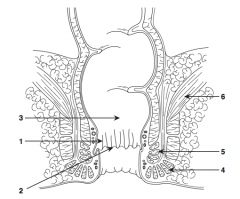
Dentate line |
|
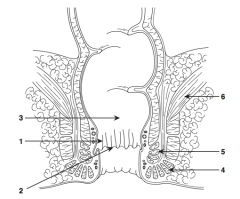
What is structure 3?
|
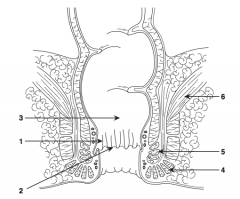
Rectum |
|
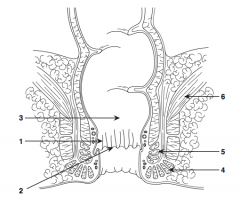
What is structure 4?
|
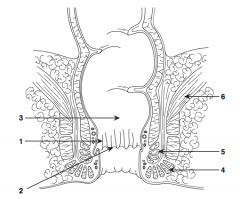
External sphincter |
|
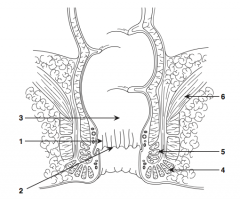
What is structure 5?
|
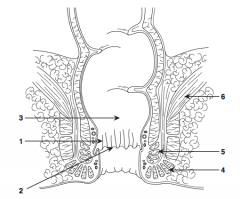
Internal sphincter |
|
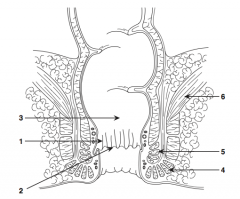
What is structure 6?
|
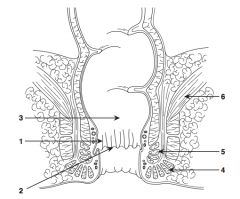
Levator ani muscle |
|
|
What is the most common carcinoma of the anus? |
Squamous cell carcinoma (80%) |
|
|
What cell types are found in carcinomas of the anus? |
1. Squamous cell carcinoma (80%) 2. Cloacogenic (transitional cell) 3. Adenocarcinoma / melanoma / mucoepiermal |
|
|
What is the incidence of anal carcinoma? |
Rare (1% of colon cancer incidence) |
|
|
What is anal Bowen's disease? |
Squamous cell carcinoma in situ |
|
|
How is Bowen's disease of the anus treated? |
With local wide excision |
|
|
What is Paget's disease of the anus? |
Adenocarcinoma in situ of anus |
|
|
How is Paget's disease of anus treated? |
With local wide excision |
|
|
What are the risk factors for anal cancer? |
- HPV - Condyloma - Herpes - HIV - Chronic inflammation (fistulae, Crohn's) - Immunosuppression - Homosexuality in males - Cervical / vaginal cancer - STDs - Smoking |
|
|
What is the most common symptom of anal carcinoma? |
Anal bleeding |
|
|
What are the other signs/symptoms of anal carcinoma? |
Pain, mass, mucus per rectum, pruritus |
|
|
What percentage of patients with anal cancer is asymptomatic? |
~25% |
|
|
To what locations do anal canal cancers metastasize? |
Lymph nodes, liver, bone, lung |
|
|
What is the lymphatic drainage below/above the dentate line? |
Below to inguinal lymph nodes (above to pelvic chains) |
|
|
Are most patients with anal cancer diagnosed early or late? |
Late (diagnosis is often missed) |
|
|
What is the workup of a patient with suspected anal carcinoma? |
- History - PE: digital rectal exam, proctoscopic exam, colonoscopy - Biopsy of mass - Abdominal/pelvic CT scan, transanal U/S - CXR - LFTs |
|
|
What is a "margin cancer"? |
Anal verge out 5 cm onto perianal skin |
|
|
What is "canal cancer" |
Proximal to anal verge up to border of internal sphincter |
|
|
How is an anal canal epidermal carcinoma treated? |
NIGRO protocol: 1. Chemotherapy (5-FU and mitomycin C) 2. Radiation 3. Post-radiation therapy scar biopsy (6-8 weeks post XRT) |
|
|
What percentage of patients have a complete response with the NIGRO protocol? |
90% |
|
|
What is the 5-year survival with the NIGRO protocol? |
85% |
|
|
What is the treatment for local recurrence of anal cancer after the NIGRO protocol? |
May repeat chemo / XRT or salvage APR |
|
|
How is a small (<5 cm) anal margin cancer treated? |
Surgical excision with 1-cm margins |
|
|
How is a large (>5 cm) anal margin cancer treated? |
Chemoradiation |
|
|
What is the treatment of anal melanoma? |
Wide excision or APR (especially if tumor is large) +/- XRT, chemo, post-op |
|
|
What is the 5-year survival rate with anal melanoma? |
<10% |
|
|
How many patients with anal melanoma have an amelanotic anal tumor? |
Approximately 1/3, thus making diagnosis difficult without pathology |
|
|
What is the prognosis of anal melanoma? |
<5% 5-year survival rate |
|
|
What is fistula in ano? |
Anal fistula, from rectum to perianal skin |
|
|
What are the causes of fistula in ano? |
Usually anal crypt/gland infection (usually perianal abscess) |
|
|
What are the signs/symptoms of fistula in ano? |
- Perianal drainage - Perirectal abscess - Recurrent perirectal abscess - Diaper rash - Itching |
|
|
What disease should be considered with fistula in ano? |
Crohn's disease |
|
|
How is the diagnosis of fistula in ano made? |
Exam, proctoscope |
|
|
What is Goodsall's rule? |
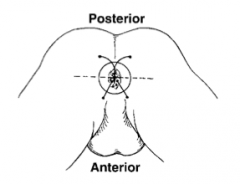
- Fistulas originating anterior to a transverse line through the anus will course STRAIGHT ahead and exit anteriorly
- Fistulas exiting posteriorly have a CURVED tract
|
|
|
How can Goodsall's rule be remembered? |
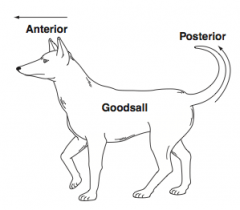
Think of a dog with a STRAIGHT nose (anterior) and a curved tail (posterior)
|
|
|
What is the management of anorectal fistulas? |
1. Define the anatomy 2. Marsupialization of fistula tract (ie, fillet tract open) 3. Wound care: routine Sitz baths and dressing changes 4. Seton placement if fistula is through the sphincter muscle |
|
|
What is a seton? |

Thick suture placed through fistula tract to allow slow transection of sphincter muscle; scar tissue formed will hold the sphincter muscle in place and allow for continence after transection
|
|
|
What percentage of patients with a perirectal abscess develop a fistula in ano after drainage? |
~50% |
|
|
How do you find the internal rectal opening of an anorectal fistula in the OR? |
Inject H2O2 (or methylene blue) in external opening - then look for bubbles (or blue dye) coming out of the internal opening! |
|
|
What is a sitz bath? |
Sitting in a warm bath (usually done after bowel movement and TID) |
|
|
What is a perirectal abscess? |
Abscess formation around the anus / rectum |
|
|
What are the signs/symptoms of perirectal abscess? |
- Rectal pain - Drainage of pus - Fever - Perianal mass |
|
|
How do you diagnose perirectal abscess? |
Physical / digital exam reveals a perianal / rectal submucosal mass / fluctuance |
|
|
What is the cause of perirectal abscesses? |
Crypt abscess in dentate line with spread |
|
|
What is the treatment of perirectal abscesses? |
As with all abscesses (except simple liver amebic abscess) DRAINAGE, sitz baths, anal hygiene, stool softeners |
|
|
What is the indication for post-op IV antibiotics for drainage with perirectal abscess? |
- Cellulitis - Immunosuppression - Diabetes - Heart valve abnormality |
|
|
What percentage of patients develop a fistula in ano during the 6 months after surgery for perirectal abscess? |
~50% |
|
|
What is an anal fissure? |
Tear or fissure in the anal epithelium |
|
|
What is the most common site for an anal fissure? |
Posterior midline (comparatively low blood flow) |
|
|
What is the cause of an anal fissure? |
Hard stool passage (constipation), hyperactive sphincter, disease process (eg, Crohn's disease) |
|
|
What is a sentinel pile? |
Thickened mucosa / skin at the distal end of an anal fissure that is often confused with a small hemorrhoid |
|
|
What is the anal fissure triad for a chronic fissure? |
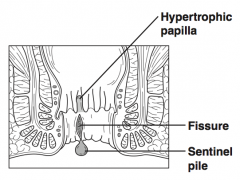
1. Fissure 2. Sentinel pile 3. Hypertrophied anal papilla
|
|
|
What is the conservative treatment for anal fissures? |
- Sitz baths - Stool softeners - High fiber diet - Excellent anal hygiene - Topical nifedipine - Botox |
|
|
What disease processes must be considered with a chronic anal fissure? |
- Crohn's disease - Anal cancer - STDs - Ulcerative colitis - AIDS |
|
|
What are the indications for surgery for anal fissure? |
Chronic fissure refractory to conservative treatment |
|
|
What is one surgical option for an anal fissure? |
Lateral internal sphincterotomy (LIS) - cut the internal sphincter to release it from spasm |
|
|
What is the rule of 90% for anal fissures? |
- 90% occur posteriorly - 90% heal with medical treatment alone - 90% of patients who undergo an LIS heal successfully |
|
|
What are perianal warts? |
Warts around the anus / perineum |
|
|
What is the cause of perianal warts? |
Condyloma acuminatum (HPV) |
|
|
What is the major risk associated with perianal warts? |
Squamous cell carcinoma |
|
|
What is the treatment of perianal warts if they are small? |
- Topical podophyllin - Imiquimod (Aldara) |
|
|
What is the treatment of perianal warts if they are large? |
Surgical resection or laser ablation |
|
|
What are hemorrhoids? |
Engorgement of the venous plexuses of the rectum, anus, or both; with protrusion of the mucosa, anal margin, or both |
|
|
Why do we have "healthy" hemorrhoidal tisue? |
It is thought to be involved with fluid/air continence |
|
|
What are the signs/symptoms of hemorrhoids? |
Anal mass / prolapse, bleeding, itching, pain |
|
|
Which type of hemorrhoids, internal or external, are painful? |
External, below the dentate line |
|
|
If a patient has excruciating anal pain and history of hemorrhoids, what is the likely diagnosis? |
Thrombosed external hemorrhoid (treat with excision) |
|
|
What are the causes of hemorrhoids? |
- Constipation / straining - Portal HTN - Pregnancy |
|
|
What is an internal hemorrhoid? |
Hemorrhoid above the (proximal) dentate line |
|
|
What is an external hemorrhoid? |
Hemorrhoid below the dentate line |
|
|
What are the three "hemorrhoid quadrants"? |
1. Left lateral 2. Right posterior 3. Right anterior |
|
|
What is a "first-degree hemorrhoid"? |
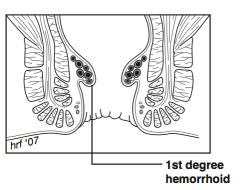
Hemorrhoid that does not prolapse
|
|
|
What is a "second-degree hemorrhoid"? |
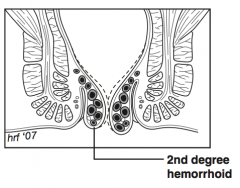
Hemorrhoid prolapses with defecation but returns on its own |
|
|
What is a "third-degree hemorrhoid"? |
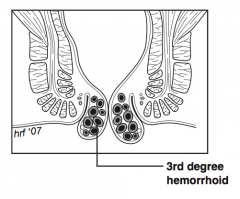
Hemorrhoid prolapses with defecation or any type of Valsalva maneuver and requires active manual reduction (eat fiber!)
|
|
|
What is a "fourth-degree hemorrhoid"? |
Hemorrhoid prolapsed and cannot be reduced |
|
|
What is the treatment of hemorrhoids? |
- High fiber diet, anal hygiene, topical steroids, sitz baths - Rubber band ligation (in most cases anesthetic is not necessary for internal hemorrhoids) - Surgical resection for large refractory hemorrhoids, infrared coagulation, harmonic scalpel |
|
|
What is a "closed" vs an "open" hemorrhoidectomy? |
- Closed (Ferguson) "closes" the mucosa with sutures after hemorrhoid tissue removal - Open (Milligan-Morgan) leaves mucosa "open" |
|
|
What are the dreaded complications of a hemorrhoidectomy? |
- Exsanguination (bleeding may pool proximally in lumen of colon w/o any signs of external bleeding) - Pelvic infection (may be extensive and potentially fatal) - Incontinence (injury to sphincter complex) - Anal stricture |
|
|
What condition is a contraindication for a hemorrhoidectomy? |
Crohn's disease |
|
|
Classically, what must be ruled out with lower GI bleeding believed to be caused by hemorrhoids? |
Colon cancer (colonoscopy) |