![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
77 Cards in this Set
- Front
- Back
|
What is AI? |
Aortic Insufficiency (regurgitation) |
|
|
What is AS? |
Aortic Stenosis |
|
|
What is ASD? |
Atrial Septal Defect |
|
|
What is CABG? |
Coronary Artery Bypass Grafting |
|
|
What is CAD? |
Coronary Artery Disease |
|
|
What is CPB? |
CardioPulmonary Bypass |
|
|
What is IABP? |
Intra-Aortic Balloon Pump |
|
|
What is LAD? |
Left Anterior Descending (coronary artery) |
|
|
What is IMA? |
Internal Mammary Artery |
|
|
What is MR? |
Mitral Regurgitation |
|
|
What is PTCA? |
Percutaneous Transluminal Coronary Angioplasty (balloon angioplasty) |
|
|
What is VAD? |
Ventricular Assist Device |
|
|
What is VSD? |
Ventricular Septal Defect |
|
|
What is SV? |
Stroke Volume = mL of blood pumped per heartbeat
SV = CO/HR |
|
|
What is CO? |
Cardiac Output = amount of blood pumped by the heart each minute
CO = HR * SV |
|
|
What is CI? |
Cardiac Index = Cardiac Output / Body Surface Area |
|
|
What is EF? |
Percentage of blood pumped out of the left ventricle
EF = SV / EDV
Normal: 55-70% |
|
|
What is compliance? |
Change in volume / change in pressure |
|
|
What is SVR? |
Systemic Vascular Resistance
SVR = (MAP - CVP) / (CO * 80) |
|
|
What is preload? |
LV end diastolic pressure or volume |
|
|
What is afterload? |
Arterial resistance the heart pumps against |
|
|
What is PVR? |
Pulmonary Vascular Resistance
PVR = (PA(mean) - PCWP / CO) * 80 |
|
|
What is MAP? |
Mean Arterial Pressure
MAP = Diastolic BP + 1/3 (Systolic BP - Diastolic BP) |
|
|
What is a normal CO? |
4-8 L/minute |
|
|
What is a normal CI? |
2.5 - 4 L/minute |
|
|
What are the ways to increase CO? |
Remember "MR PAIR": 1. Mechanical assistance (IABP, VAD) 2. Rate - increase HR
3. Preload - increase 4. Afterload - decrease 5. Inotropes - increase contractility 6. Rhythm - normal sinus |
|
|
When does most of the coronary blood flow take place? |
During diastole (66%) |
|
|
Name the three major coronary arteries? |
1. Left Anterior Descending (LAD) 2. Circumflex 3. Right Coronary |
|
|
What are the three main cardiac electrolytes? |
- Calcium (inotropic) - Potassium (dysrhythmias) - Magnesium (dysrhythmias) |
|
|
What is Coronary Artery Disease? |
Atherosclerotic occlusive lesions of the coronary arteries; segmental nature makes CABG possible |
|
|
What is the incidence of CAD? |
CAD is the #1 killer in the Western world; >50% of cases are triple vessel diseases involving the LAD, circumflex, and RCA |
|
|
What are the symptoms of CAD? |
If ischemia occurs (low flow, vasospasm, thrombus formation, plaque rupture, or a combination), patient may experience: - Chest pain - Crushing - Substernal shortness of breath - Nausea / upper abdominal pain - Sudden death - Asymptomatic with fatigue |
|
|
Who classically gets "silent" MIs? |
Patients with diabetes (autonomic dysfunction) |
|
|
What are the risk factors for CAD? |
- HTN - Smoking - HLD (lipids >240) - Obesity - Diabetes mellitus - Family history |
|
|
Which diagnostic tests should be performed to evaluate for CAD? |
- Exercise stress testing (+/- thallium) - Echocardiography - Localize dyskinetic wall segments - Valvular dysfunction - Estimate EF - Cardiac cath with coronary angiography and left ventriculography (the definitive test) |
|
|
What is the treatment of CAD? |
- Medical therapy (beta-blockers, aspirin, nitrates, HTN meds) - Angioplasty (PTCA) - +/- stents or surgical therapy (CABG) |
|
|
What is CABG? |
Coronary Artery Bypass Grafting |
|
|
What are the indications for CABG? |
- Left main disease - ≥ 2 vessel disease (especially diabetics) - Unstable or disabling angina unresponsive to medical therapy / PTCA - Post-infarct angina - Coronary artery rupture, dissection, thrombosis after PTCA |
|
|
What is the difference between CABG and PTCA +/- stents? |
- CABG = survival improvement for diabetics and ≥2 vessel disease, increased short-term morbidity
- PTCA = decreased short-term morbidity, decreased cost, decreased hospital stay, increased re-intervention, increased post-procedure angina |
|
|
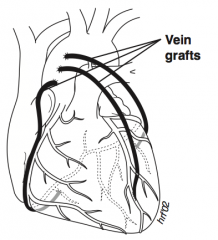
What procedures are most often used in a CABG? |
Coronary arteries grafted (usually 3-6): - Internal mammary pedicle graft and saphenous vein free graft are most often used - IMA 95% 10-year patency vs 50% with saphenous |
|
|
What other vessels are occasionally used for CABG, besides the IMA and saphenous? |
- Radial artery - Inferior epigastric vein |
|
|
What are the possible complications of CABG? |
- Hemorrhage - Tamponade - MI - Dysrhythmias - Infection - Graft thrombosis - Sternal dehiscence - Post-pericardiotomy syndrome - Stroke |
|
|
What is the operative mortality associated with CABG vs acute MI? |
- 1-3% for elective CABG - 5-10% for acute MI |
|
|
What meds should almost every patient be given after CABG? |
- Aspirin - Beta-blocker |
|
|
Can a CABG be performed off cardiopulmonary bypass? |
Yes, today they are performed with or without bypass |
|
|
What is post-pericardiotomy syndrome? |
Pericarditis after pericardiotomy (unknown etiology), occurs weeks to 3 months post-operatively |
|
|
What are the signs/symptoms of post-pericardiotomy syndrome? |
- Fever - Chest pain - Atrial fibrillation - Malaise - Pericardial friction rub - Pericardial effusion / pleural effusion |
|
|
How do you treat post-pericardiotomy syndrome? |
- NSAIDs - +/- Steroids |
|
|
What is pericarditis after an MI called? |
Dressler's syndrome |
|
|
What is cardiopulmonary bypass (CPB)? |
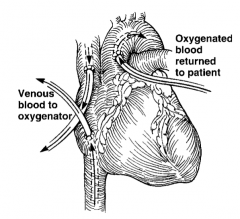
- Pump and oxygenation apparatus removes blood from SVC and IVC and returns it to aorta - Bypasses the heart and lungs, allowing cardiac arrest for open-heart procedures, heart transplant, lung transplant, or heart-lung transplant, as well as procedures on the proximal vessels |
|
|
Is anticoagulation necessary for cardiopulmonary bypass (CPB)? |
Yes, just before and during the procedure, with heparin |
|
|
How is anticoagulation reversed after cardiopulmonary bypass (CPB)? |
Protamine |
|
|
What are the ways to manipulate cardiac output after cardiopulmonary bypass (CPB)? |
- Rate - Rhythm - Afterload - Preload - Inotropes - Mechanical (IABP and VAD) |
|
|
What mechanical problems can decrease CO after CPB? |
- Cardiac tamponade - Pneumothorax |
|
|
What is "tamponade physiology"? |
- Decreased CO - Increased HR - Hypotension - Increased CVP = Increased wedge pressure |
|
|
What are the possible complications of cardiopulmonary bypass (CPB)? |
- Trauma to formed blood elements (especially thrombocytopenia and platelet dysfunction) - Pancreatitis (low flow) - Heparin rebound - CVA - Failure to wean from bypass - Technical complications (operative technique) - MI |
|
|
What are the options for treating post-op CABG mediastinal bleeding? |
- Protamine - Increased PEEP - FFP - Platelets - Aminocaproic acid |
|
|
What is "heparin rebound"? |
Increased anticoagulation after cardiopulmonary bypass (CPB) from increased heparin levels, as increase in peripheral blood flow after CPB returns heparin residual that was in the peripheral tissues |
|
|
What is the method of lowering SVR after cardiopulmonary bypass (CPB)? |
Warm the patient; administer sodium nitroprusside (SNP) and dobutamine |
|
|
What are the options if a patient cannot be weaned from cardiopulmonary bypass (CPB)? |
- Inotropes (eg, epinephrine) - VAD - IABP |
|
|
What percentage of patients go into AFib after cardiopulmonary bypass (CPB)? |
Up to 33% |
|
|
What is the workup of a cardiopulmonary bypass (CPB) post-op patient with AFib? |
- Rule out pneumothorax (ABG, CT scan) - Rule out acidosis (ABG) - Check for electrolyte abnormality (labs) - Check for ischemia (EKG) - CXR |
|
|
What is a MIDCAB? |
Minimally Invasive Direct Coronary Artery Bypass: - LIMA to LAD bypass without cardiopulmonary bypass (CPB) and through a small thoracotomy |
|
|
What is TMR? |
Trans-Myocardial laser Revascularization: - Laser through grain catheter makes small holes (intramyocardial sinusoids) in the cardiac muscle to allow blood to nourish the muscle |
|
|
What is OPCAB? |
Off Pump Coronary Artery Bypass: - Median sternotomy but no bypass pump |
|
|
What is Aortic Stenosis? |
Destruction and calcification of valve leaflets, resulting in obstruction of left ventricular outflow |
|
|
What are the causes of aortic stenosis? |
- Calcification of bicuspid aortic valve - Rheumatic fever - Acquired calcific AS (7th-8th decades) |
|
|
What are the symptoms of aortic stenosis? |
- Angina (5 years life expectancy if left untreated) - Syncope (3 years life expectancy if left untreated) - CHF (2 years life expectancy if left untreated) - Often asymptomatic until late |
|
|
What is the memory aid for aortic stenosis complications? |
Aortic Stenosis Complications = Angina Syncope CHF (5, 3, 2) |
|
|
What are the signs of aortic stenosis? |
- Murmur: crescendo-decrescendo systolic second right intercostal space with radiation to the carotids - Left ventricular heave or lift from LV hypertrophy |
|
|
What tests should be performed to evaluate aortic stenosis? |
- CXR, ECG, echocardiography - Cardiac cath - needed to plan operation |
|
|
What is the surgical treatment of aortic stenosis? |
Valve replacement with tissue or mechanical prosthesis |
|
|
What are the indications for surgical repair of aortic stenosis? |
If patient is symptomatic or valve cross-sectional area is <0.75 cm^2 (normal 2.5-3.5 cm^2) and/or gradient >50 mmHg |
|
|
What are the pros/cons of mechanical valve for aortic stenosis? |
Mechanical valve is more durable, but requires lifetime anti-coagulation |
|
|
What is the treatment option for aortic stenosis in poor surgical candidates? |
Balloon aortic "valvuloplasty" (percutaneous) |
|
|
Why is a loud murmur for aortic stenosis often a good sign? |
Implies a high gradient, which indicates preserved LV function |
|
|
Why might an AS murmur diminish over time? |
It may imply a decreasing gradient from a decline in LV function |