Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
58 Cards in this Set
- Front
- Back
|
What are the two layers surrounding the testes?
|
Tunica albuginea (inner capsule)
Tunica vaginalis (outer sac) |
|
|
What space fills during a hydrocele?
|
Tunica vaginalis
|
|
|
What is the ultrastructure of the testis?
|

250 lobules with 1-4 seminiferous tubules
Rete testis and efferent ductules connect seminiferous tubules to epididymis |
|
|
Where is the location that the sperm acquire motility?
|
Epididymis
|
|
|
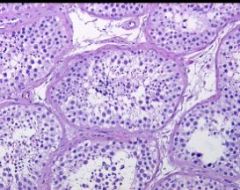
What is the site of sperm production in the testis?
|
Seminferous tubules
|
|
|
In the seminiferous tubules, what is found in the interstitium?
|
Leydig cells
Lymphatics Vasculature |
|
|
What is the function of leydig cells?
|
Testosterone production
|
|
|
In the seminiferous tubules, where are the germ cells found?
|
Outside!
More mature cells are more in the center |
|
|
Where in the seminiferous tubules are the sertoli cells located?
|
Throughout the seminiferous tubule
|
|
|
What's the appearance of the sertoli cells?
|
Triangular or columnar
|
|
|
What's the function of the sertoli cells?
|
Support spermatogenesis
|
|
|
What's the differential diagnosis for testicular problems?
|
MINTS
M: metabolic - infertility associated problems I: infectious/inflammation N: neoplastic T: toxic S: structural/systemic |
|
|
How do you assess metabolic-infertility associated issues of the testis?
|
Biopsy
|
|
|
What are you assessing in a testicular biopsy?
|
Normal spermatogenesis
Hypospermatogenesis Maturation arrest Germ cell aplasia |
|
|
What can cause infertility in the setting of normal spermatogenesis?
|
Duct obstruction
Disordered motility |
|
|
What can cause infertility in the setting of hypospermatogenesis?
|
Altered hormonal states
Heat Varicocele |
|
|
What are causes of germ cell aplasai?
|
CRYPTORCHIDISM
Estrogen therapy Chemoes |
|
|
What kinds of cells will you see on a biopsy if there is germ cell aplasia?
|
Only sertoli cells!
|
|
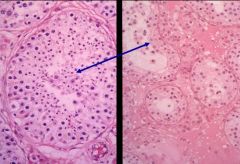
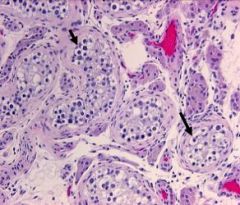
What's happening here?
L: normal R: abnormal |
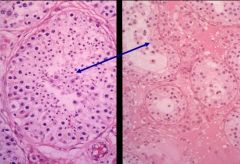
Maturation arrest:
nothing beyond primary spermatocytes on the R |
|
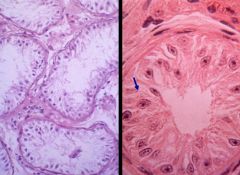
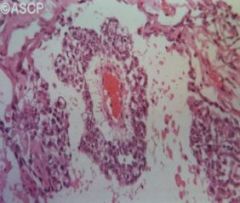
What's happening here? What can cause this?
|
Germ cell aplasia: only sertoli cells are present
Causes: Cryptorchidism Estrogen therapy Chemo |
|
|
What is more common: epididymitis or orchitis?
|
Epididymitis!
|
|
|
What are the most common causes of epididymitis?
|
Chlamydia
Gonorrhea |
|
|
What are causes of orchitis?
|
Bacterial
Mycobacteria Fungal Viral |
|
|
What condition can mimic tumors in the tetes?
|
Granulomatous orchitis:
-Unilateral enlarged tender mass -Granulomas found upon biopsy |
|
|
What is more common: testicular or epididymal tumos?
|
TESTICULAR TUMORS!
|
|
|
What's the most common kind of testicular tumor?
|
Germ cell tumor
|
|
|
What age of people get testicular cancer?
|
15-34
|
|
|
What race of people get testiular cancer?
|
Caucasians more than african-americans
5:1 |
|
|
What are risk factors for testicular carcinoma?
|
Cryptorchidism (the contralateral testis is at risk, too!)
Testicular dysgenesis Genetic (rare) |
|
|
What are some causes of testicular dysgensis?
|
Testicular feminization
Klinefelters syndrome |
|
|
What is the common genetic abnormality to testicular tumors?
|
Isochromosome 12p: only the short arms
|
|
|
What are the types of testicular tumors?
|
GERM CELL TUMORS (95%)
Non-germ cell tumors: -Sex cord -Lymphomas |
|
|
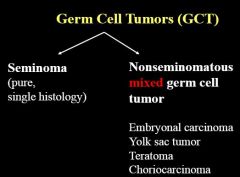
What are the types of germ cell tumors?
|
Seminoma
Embryonal carcinoma Yolk sac tumor Choriocarcinoma Teratoma Mixed germ cell tumor |
|
|
What's the most common type of testicular germ cell tumor?
|
Seminoma
|
|
|
What proportion of testicular germ cell tumors show single histology? Mixed?
|
40% single
60% mixed Seminoma is likely to be pure. |
|
|
What is the common originating cell for all testicular germ cell tumors?
|
Intratubular germ cell neoplasia (ITGCN)
|
|
|
What is the differentiation of germ cell tumors of the testis?
|
|
|
|
What are the properties of an intratubular germ cell neoplasia?
|
Malignant PREINVASIVE form of germ cell neoplasm
Confined to the seminiferous tubules |
|
|
What's the appearance of a seminoma?
|
Homogenous fleshy, gray-white
|
|
|
What's the peak incidence of a seminoma?
|
3rd-4th decade
|
|
|
What's an effective therapy for a seminoma?
|
Radiotherapy
The tumor is vulnerable to this. |
|
|
What's the appearance of a seminoma?
|
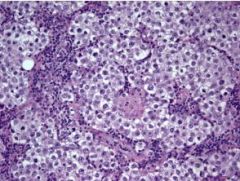
Nests of cells
Clear cytoplasm Hyperchromatic nuclei Fibrous septae infiltrated with lymphocytes NO NUCLEAR CROWDING! |
|
|
What age do people present with an embryonal carcinoma?
|
10 years YOUNGER than with a seminoma: 20-30 YO
|
|
|
What's the gross appearance of a embryonal carcinoma?
|

Variegated growth
Areas of hemorrhage and necrosis (it's not the homogenous appearance of the seminoma!) |
|
|
What is the usual composition of an embryonal carcinoma?
|
They present as a mixed lesion
|
|
|
What type of therapy is especially effective for embryonal carcinoma?
|
Chemo
|
|
|
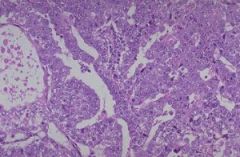
What's the microappearance of embryonal carcinoma?
|
Some gland formation
Solid, sheet tumors Pleomorphic nuclei Crowding Indistinct cell membranes |
|
|
What's the clinical course of embryonal carcinoma?
|
Aggressive, in comparison to seminomas.
|
|
|
What's the most common testicular tumor in kids up to 3 YO?
|
Yolk sac tumor
95% of the time! IT'S ALWAYS THIS. |
|
|
What's the marker for a yolk sac tumor?
|
AFP
|
|
|
What's the prognosis of a yolk sac tumor?
|
Great.
|
|
|
What's the characteristic histologic finding in a yolk sac tumor?
|
Schiller duval body
|
|
|
Other than a yolk sac tumor, what kinds of tumors do kids get?
|
Teratomas
|
|
|
What is the problem with postpubertal teratomas?
|
Malignant!
They can met. |
|
|
If it's a non-seminomatus tumor, what is it, most likely?
|
Mixed germ cell tumor!
|
|
|
What are the following markers used for:
AFP Beta HCG LDH |
AFP: yolk sac tumor
Beta HCG; choriocarcinoma LDH: not specific; assesses tumor burden |
|
|
If someone has a combined elevated beta-HCG AND AFP, what do you think?
|
NSGT
|
|
|
What's the staging of testicular tumors?
|
1. Confined to the testis
2: Retroperitoneal nodes below the diaphragm 3: Mets outside the retroperitoneal nodes; above diaphragm |