Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
30 Cards in this Set
- Front
- Back
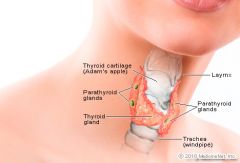
Histology:
Follicles |
The thyroid is composed of spherical follicles that selectively absorb iodine (as iodide ions, I-) from the blood for production of thyroid hormones, but also for storage of iodine in thyroglobulin. Twenty-five percent of all the body's iodide ions are in the thyroid gland. Inside the follicles, in a region called the follicular lumen, colloid serves as a reservoir of materials for thyroid hormone production and, to a lesser extent, acts as a reservoir for the hormones themselves. Colloid is rich in a protein called thyroglobulin.
|
|
Thyroid epithelial cells
(or "follicular cells") Follicles |
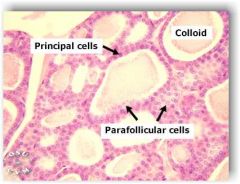
The follicles are surrounded by a single layer of thyroid epithelial cells,
• Which secrete T3 and T4. • When the gland is not secreting T3 and T4 (inactive), the epithelial cells range from low columnar to cuboidal cells. • When active, the epithelial cells become tall columnar cells. |
|
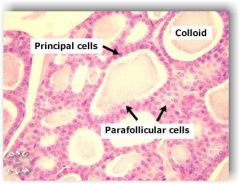
Parafollicular cells
C Cells |
Scattered among follicular cells and in spaces between the spherical follicles
• are another type of thyroid cell, parafollicular cells, which secrete calcitonin. |
|
|
T3 and T4
|
• Thyroxine (T4) is synthesised by the follicular cells from free tyrosine and on the tyrosine residues of the protein called thyroglobulin (Tg). Iodine is captured with the "iodine trap" by the hydrogen peroxide generated by the enzyme thyroid peroxidase (TPO)
• Thyroid hormone secreted from the gland is about 80-90% T4 and about 10-20% T3. • T3 does most of the work • When T4 gets to target organ, it is converted to T3 and then gets to work! • T4 is 99% bound to binding globulins and is only active as FREE T4 |
|
|
Calcitonin is produced in humans primarily by the parafollicular cells (also known as C-cells) of the thyroid
|
More specifically, calcitonin lowers blood Ca2+ levels in three ways:
• Inhibits Ca2+ absorption by the intestines[7] • Inhibits osteoclast activity in bones[8] • Inhibits renal tubular cell reabsorption of Ca2+ allowing it to be excreted in the urine[9][10] However, effects of calcitonin that mirror those of PTH include the following: • Inhibits phosphate reabsorption by the kidney tubules[11] |
|
|
What does the Thyroid do?
|
The primary function of the thyroid is production of the
• hormones triiodothyronine (T3), • thyroxine (T4), and • calcitonin. • Up to 80% of the T4 is converted to T3 by peripheral organs such as the liver, kidney and spleen. • T3 is several times more powerful than T4, which is largely a prohormone, perhaps four[9] or even ten times more active.[10] |
|
McCance page 711-712
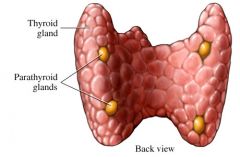
Parathyroid PTH: |
• Usually 2 pairs, but can range from 2-6 pairs
• PTH: Increase serum calcium and decrease serum Phosphorous • Sustained PTH stimulation leads to reduction in bone density • However, intermittent administration of rPTH ( daily) increases bone turnover such that the net effect that Osteoblast receive more stimulation than Osteoclast and there is more bone remodeling |
|
Papillary thyroid cancer
|
• Papillary thyroid cancer or papillary thyroid carcinoma[1] is the most common type of thyroid cancer,[2] representing 75% to 85% of all thyroid cancer cases.[1]
• It occurs more frequently in women and presents in the 20-55 year age group. • It is also the predominant cancer type in children with thyroid cancer, and • Patients with thyroid cancer who have had previous radiation to the head and neck.[ |
|
|
MTC
C Cell cancer |
Medullary thyroid cancer (MTC)
• is a form of thyroid carcinoma which originates from the parafollicular cells (C cells), which produce the hormone calcitonin.[1] • Medullary tumors are the third most common of all thyroid cancers. They make up about 3% of all thyroid cancer cases. |
|
|
Solitary nodule Goroll page 736
And DDX |
• Benign adenomas, cancer, or multi nodular disease in early stages
• Hard and immovable is a bad sign in most cases • Look for Toxic adenomas > 3 cm: think thyrotoxicosis: Hot nodule • DDX: ademoma, cancer papillary or mixed ,follicular, medullary, lymphoma |
|
|
Multiple nodules
Goroll page 736-7 And DDX |
• Hashimoto’s thyroiditis
• Multi-nodular goiter : starts out as general hyperplasia and progresses to enlarged nodules • Cancers, thyroid , lymphoma ( related to Hashimotos) |
|
|
Evaluation of thyroid nodules
Lab studies |
• TSH
• FNA and BX: best method Do this one 1st in most cases • Radionuclide test • US |
|
|
Evaluation for hypercalcemia Goroll page 741
SS |
SS: fatigue, weakness, abdominal discomfort, constipation, cognitive , and depression : stones, bones, and psychic moans
• Primary hyperparathyroidism or malignancy • Parathyroid cancer < 1% for all hypercalcemia |
|
|
MEN 1 and 2
Multiple- endocrine- neoplasms |
• MEN 1: hyperplasia of adenoma of pituitary and pancreas
• MEN 2: parathyroid hyperplasia with medullary cancer of thyroid, and adrenal Pheochromocytoma • Thiazide diuretics inhibit calcium excretion and can result in elevated serum calcium |
|
|
Cancers and hypercalcemia
|
• Most common cause among hospital patients
• Breast, lung and kidney • Mechanism: increased Osteoclastic bone resorption, even with NO Bone mets. PTH like hormone • Some bone mets do not result in hypercalcemia • Hypercalcemia presenting with cancer is a Grave sign: survival < 2 months |
|
|
Other causes of hypercalcemia
|
• Sarcoidosis
• Milk alkali syndrome : too much supplemental calcium per diet • Medication: thiazide, high dose calcium, theophylline excess , lithium • Hyperthyroidism • Immobility, Pagets disease, L |
|
|
Test for elevated calcium
|
• PTH level
• Bone scan for mets • TSH |
|
|
TX for hypercalcemia
|
• Surgery for bad parathyroid
• Estrogen and progesterone for post-menopausal women • PO phosphate • Lasix • Calcitonin: NOT useful over long term |
|
|
Hyperthyroidism
Goroll page 788 Clinical expression of a heterogeneous group of disorders that produce excess T3-T4 |
• Grave’s disease
• Toxic adenoma , • Excessive ingestion of synthroid • Iodine excess • Transient hyperthyroidism with Hashimotos thyroiditis, post-partum thyroiditis • May be found incidental to new onset AFIB • Women > Men |
|
|
Hyperthyroidism
H&P |
• Heat intolerance, nervousness, hyperactivity, tremor, increased appetite, weight loss, sweating, lid lag, diarrhea,( more likely frequent defecation ) muscle weakness
• Apathetic hyperthyroidism of the elderly: not too many symptoms • Recent iodine exposure • Goiter history • Anterior neck pain • Thyroid replacement therapy • Family history of thyroid disease • Pregnancy • Height/weight • Vital signs • Cardiovascular • Thyroid enlargement • Proximal muscle weakness • Eye exam • Skin exam |
|

Grave’s disease
|

• Autoimmune
• Bug eyes • Pretibial myxedema ; thyroid dermapathy: non pitting swelling Orange peel, red, dark pink • Diffusely large goiter with Bruit • Toxicosis: skin is velvety, skin silky, onychholyis , vitilago, gynamastia , cardiomyopathy |
|
|
Other causes for hyperthyroidism
|
• Toxic Multinodular goiter : no exophthalmos- exposure to Iodides or amiodarone
• Single toxic nodule • Look at table on page 795 for DDX |
|
|
TX: graves’ disease
|
Regardless of etiology for adrenergic symptoms
• Beta blocker • Graves disease: methimazole with beta blocker; continue for 12-24 months ; keep an eye on labs • Pregnant: PTU • For bad exophthalmos: high dose steroids • Consider Iodine -131 |
|
|
Hypothyroidism: Goroll page 798
Risk factors |
Down syndrome
Elderly Use of certain medications Female gender Postpartum period History of head and neck XRT Family and personal history of autoimmune disease |
|
|
Primary hypothryoidism
|
• Note to David: In primary hypothyroidism, the original problem is in the thyroid which means that T3-T4 is low; most often due to an autoimmune disease.
• Then: Hypothalamus produces high amount of TRH→ pituitary ↑ TSH → thyroid enlargement , goiter ; all of this as the thyroid struggles to make enough T3T4 Reduction in the amount of circulating free thyroid hormone. There is resistance to the action of the thyroid hormone. Most common cause is Hashimoto’s thyroiditis. Hypothyroidism is the second most common endocrine problem with 2-5 cases per 100 persons in the US. • |
|
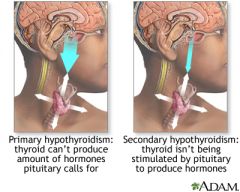
Secondary hypothyroidism
|
• ↓ TSH
• Gland is normal or even small and T3 and T4 production is reduces Adrenal insufficiency can also result in hypothyroid symptoms without affecting the thyroid itself secondary (central) due to the failure of adequate thyroid-stimulating hormone (TSH) secretion from the pituitary gland or thyrotrophin-releasing hormone (TRH) from the hypothalamus. Secondary hypothyroidism can be differentiated in pituitary and hypothalamic by the use of TRH test. |
|
|
TX guidelines for Primary hypothyroidism
page 803-804 |
• If possible ; stop all drugs that impair the thyroid
• Replace thyroid: start 50-100mcg and increase in increments of 25-50 mcg; do less for elderly: too much is bad for CAD • Evaluate TSH + clinical presentation TSH changes lag clinical changes by months : goal is normalization of TSH • Allow 4-6 weeks for dose changes to take effect • For neuropsychiatric problems ; consider a mix of T3 and T4 • If TSH is too low: <0.5 this can cause osteoporosis • Once dose is OK : check Q6-12 months • Mild to moderate uncorrected low thyroid and CAD can proceed with surgery • Pregnancy: consider lower doses |
|
|
H&P for low thyroid
|
HX:
Autoimmune disorders Prior history of pituitary or thyroid disease Thyroid surgery Prior treatment with radioactive iodine or other radiation exposure Physical: Palpation of thyroid gland Vital signs--bradycardia Change in voice quality such as hoarseness Facial edema Slow speech Skin changes Delayed DTR relaxation |
|
|
Screening for low thyroid
|
Goiter
Previous thyroid dysfunction DM Surgery or XRT Vitiligo Leuotrichia Medications Hyperprolactinemia Elevated creatine phosphokinase, LDH Hypercholesterolemia Hyponatremia Anemia |
|
|
TX secondary hypothyroidism
|
• ACTH stimulation test to look at adrenals
• Replace thyroid as in primary disease • Monitor clinical signs + free T4 |