Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
34 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
where do the internal thoracic arteries run?
|
along the sternum; anastomose with intercostal arteries
|
|
|
|
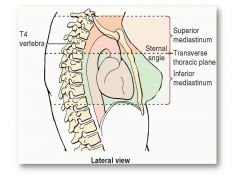
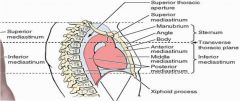
Superior and inferior regions of the mediastinum at the level of the sternal angle
|
|
|
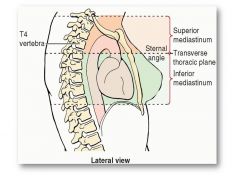
What is contained in the mediastinum?
|
mediastinum = the space between the pleural cavities in the chest; it contains the heart, great vessels, esophagus, airways, nerves and thoracic duct
|
|
|
|
Azygos System/Vein
|
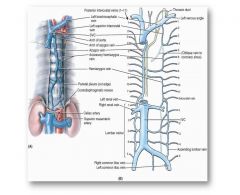
Connects superior vena cava with inferior vena cava; receives blood from intercostals and subcostals
|
|
|
|
Relationship of the azygos system and esophagus
|

Receives blood from esophageal plexi, which anastomse with branches of hepatic portal system
|
|
|
|
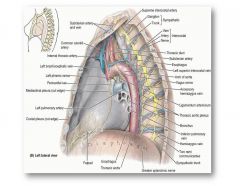
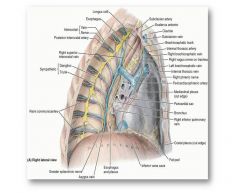
Left Posterior Mediastinum; note ligamentum arteriosum = remnant of fetal ductus arteriosus which enusres a single circulatory system before birth
|
|
|
|
right posterior mediastinum; noite azygos vein, arch of azygos where it connects to superior vena cava
|
|
|
|
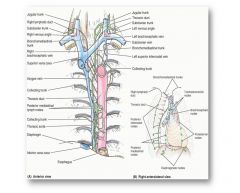
Thoracic Duc tin posterior mediastinum; note that the TD receives lymph from all but the upper right quadrant of the body (which is drained via the right lymphatic duct); crosses from right to left to empty into veins at the left venous angle
|
|
|
|
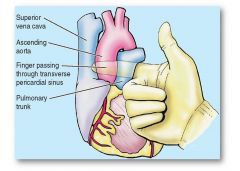
Transverse Sinus; since you can separate the pulmonary trunk and aorta from venous inflow you can connect a heart lung machine here
|
|
|
|
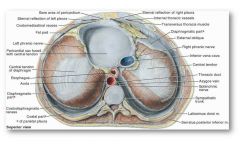
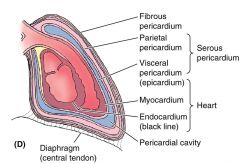
Note how pericardial sac is fused to central tendon of the diaphragm
|
|
|
AlOH
|
antacid, constipation
1. alkalinizes stomach, delays gastric emptying, chelates -->↓ absorption of tetracycline, isoniazid, ketoconazole, fluroquinolones 2. alkalinizes urine which changes urinary excretion of drugs ↑ acidic drug excretion (salicylates) ↓ basic drug excretion (quinidine) Toxicity: hypokalemia, hypophosphatemia, proximal muscle weakness, osteodystrophy, seizures |
|
|
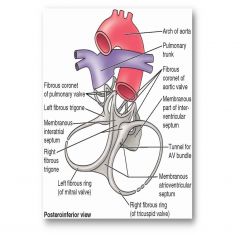
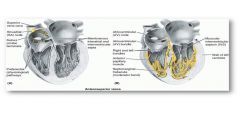
What is the function of the connective tissue of A-V boundary?
|
Fibrous skeleton associated with the valves and atrioventricular septum; provides mechanical support and electrical insulation of the atria from the ventricles
|
|
|
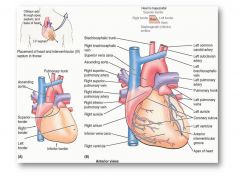
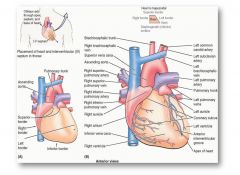
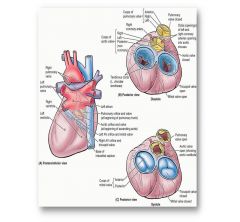
Normal Heart Orientation
|
Base of heart is where the veins and arteries enter/leave
Left ventricle is dorsolateral to right ventricle |
|
|
二
|
èr
|
two
|
|
Which heart valves are not tethered by cordae tendineae?
|
Pulmonic and aortic semilunar valves
|
|
|
What structure may be damaged when a surgeon closes a ventricular septal defect?
|
AV Bundle
|
|
|

Where are the coronary arteries located?
|
Aortic Sinus;
|
|
|
|
Which coronary artery supplies the interventricular septum (which includes most of the AV bundle branches)
|
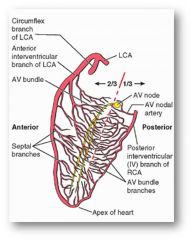
Left coronary Artery
|
|
|
|
Which coronary branch supplies the SA node?
|
right coronary artery
|
|
|
|
What is the most common site of occlusion?
|

Anterior Interventricular Branch
|
|
|
|
where are cell bodies for the first order neurons of the sympathetic nervous system?
|
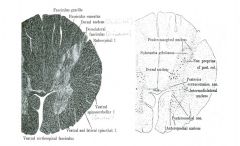
Interomediolateral Nulceus
|
|
|
|
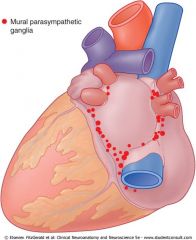
Long preganglionic parasympathetic axons (vagus nerve) with short postganglionic neurons located in the wall of the structure innervated
|
|
|

|
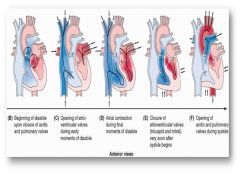
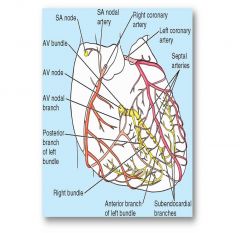
Conducting System of the Heart
If denervated, the heart will spontaneously contract at approximately 30 bpm |
|
|
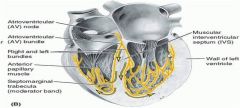
Bundle of His
|
Begins at AV node; bifurcates passing along the interventricular septum to reach the myocardium
blockage here = heart block, which can happen during a procedure to repair a defect in the intraventricular septum |
|
|
|
How does epinephrine affect adrenergic postganglionic sympathetic axons?
|
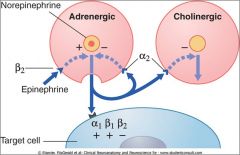
Potentiates the action of NE via B2R
|
|
|
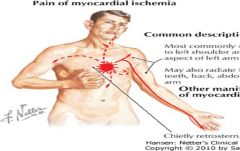
How do you account for the reffered pain of MI?
|

T1-T5 dermatones affected; usually goes down left side bc left ventricles commonly affected (larger oxygen demand due to thick walls from pumping against systemic pressure)
|
|
|
|
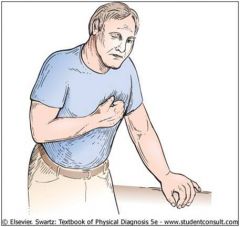
Levine's Sign; pressing on sternum; afferent traffic for pressure diminishes competes w/ pain traffic for conscious perception; diminishes pain in T1-T5(t6)
|
|
|
|
Note the three layers of the pericardium; (outer fibrous, parietal, visceral)
There is pericardial space between the parietal and visceral layers |
|
|
|
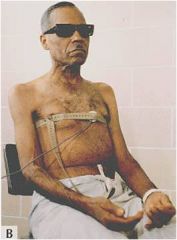
Effusive Constrictive Pericarditis
Exertional fatigue, dyspnea, abnormallly distended neck veins, dependent edema, and hepatic engorgement are almost universally present. Ascites is found in 15-50% of patients. |
|
|
Why might you get left shoulder pain in effusive constrictive pericarditis?
|
Fibrous and parietal layers of the serous pericardium are innervated by the phrenic nerves
|
|
|
|
Where will pain from the ascending aorta radiate?
|
Anterior thoracic wall since it's an anterior structure
|
|
|
|
Where will pain from the descending aorta radiate?
|
Posterior chest wall; descending aorta is a posterior structure
|
|
|
|
Grave prognostic sign of aortic dissection
|
Interscapular pain that moves over time
|
|
|
|
Relative to the mediastinum, where is the arch of the aorta?
|
Superior mediastinum (T4 and above)
|
|