Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
142 Cards in this Set
- Front
- Back
|
What is a problem list?
|
-A true statement.
-At our highest level of understanding. -Can evolve/change, as our understanding deepens. -To be a problem, it must be interfering with the patient's well-being. - It is NOT an abnormality list. -Once the list is formed, consider etiology of the problems. Develop DDx. |
|
|
What is a SOAP?
|
S = Subjective: History taken from owner.
O = Objective: All clinical data generated by vet. A = Assessment: What you think is likely going on. P = Plan: Diagostics done, treatment given, and client education. |
|
|
What is the DAMNIT-V scheme?
|
It is meant to help us come up with DDx.
D = Degenerative A = Anomalous: Usually congenital malformations of tissues, etc. M = Metabolic N = Neoplastic / Nutritional I = Inflammation / Infectious / Immune-mediated / Idiopathic T = Traumatic / Toxic V = Vascular: Thrombosis, ischemia, hemorrhage, etc. |
|
|
Compare true prevalence with apparent prevalence.
|
Apparent prevalence is the proportion of a population that tested (+); it may be inaccurate given that tests have false positives and negatives.
True prevalence is the proportion of a population that tested (+) AND actually had the DZ. |
|
|
What is sensitivity in regards to a test?
|
Sensitivity refers to the likelihood that a person who tested (+) is indeed diseased.
= (True +) / (DZ +) |
|
|
What is specificity in regards to a test?
|
Specificity refers to the likelihood that a person who tested (-) is indeed non-diseased.
= (True -) / (DZ -) |
|
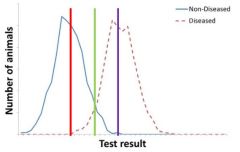
Describe the sensitivity+specificity of the test with the:
Purple test cutoff Green test cutoff Red test cutoff |
Purple test → High specificity; Low sensitivity
Green test → Pretty high specificity and sensitivity Red test → Low specificity; High sensitivity |
|
|
True or False:
Negative predictive value correlates with sensitivity, while positive predictive value correlated with specificity. |
True.
|
|
|
True or False:
Positive predictive value tells us how believable a (+) result is; PPV is higher in places where prevalence is high. |
True.
|
|
|
What happens inside the nucleolus of a cell?
|
rRNA synthesis.
|
|
|
What are the stages of the cell cycle?
|
G0 → Resting phase. Cells hang out here until required growth factors are present.
G1 → Cells increase in size. Majority of cell's time is spent in this phase. Rb checkpoint found here; phosphorylation of Rb renders it inactive, and the cell continues on in the cycle. S → DNA replication occurs. G2 → Cells continue to grow. p53 checkpoint found here. Mitosis → Parent cell divides into 2 daughter cells. |
|
|
What is the role of the rough ER?
|
Protein synthesis. It is called RER because its surface is studded with ribosomes.
|
|
|
What is the role of the golgi apparatus?
|
Once proteins are made in the RER, they move to the golgi apparatus to get packaged and ready for secretion.
|
|
|
What is the difference between isotonic and isosmotic?
|
Isotonic - the 2 solutions being compared contain solutes that exert equal pressure.
Isosmotic - the 2 solutions being compared contain the same number of solute particles. |
|
|
Compare osmolarity with osmolality.
|
Osmolarity measures the number of osmoles of solute particles per unit volume of solution.
Osmolality takes into account only solutes that contribute to a solution's osmotic pressure. It is measured in osmoles of the solute per kilogram of water. |
|
|
Describe tight junctions.
|
Tight junctions:
-Define cell's polarity. -Control the passage of substances b/t adjacent cells. -Belt-like distribution across the apical part cell. -Associated with actin filaments. |
|
|
Describe belt desomosomes / zonula adherens.
|
Belt desmosomes:
-Belt-like distribution across the apical portion of the cell, similar to tight junctions. -Associated with actin filaments. -Keeps epithelium organized in sheets. |
|
|
Describe macula densa / spot desmosomes.
|
Macula densa:
-Associated with intermediate filaments. -Anchors 2 epithelial cells together. |
|
|
Describe hemidesmosomes.
|
Hemidesmosomes:
-Attaches the basal end of an epithelial cell to the basal laminal below it. -Associated with intermediate filaments and plaques. |
|
|
What is standard metabolic rate?
|
SMR is the steady-state rate of heat production by an organism under standard conditions.
Standard conditions = Adult, resting, awake, stress-free, non digesting, neutral temperature zone. Keep in mind that SMR only considers the energy that becomes heat. |
|
|
How do we measure standard metabolic rate?
|
SMR is measured directly by measuring an animal's heat production or indirectly by measuring the animal's O2 consumption.
|
|
|
What is minimal metabolic rate (MMR)?
|
An animal can fall below standard metabolic rate to MMR during sleep, starvation, or anesthetization.
|
|
|
What is maximal metabolic rate?
|
It is the max achievable metabolic rate; it's usually 10-20x SMR.
|
|
|
True of False:
The amount of O2 that an organ uses is proportional to its mass. (AKA, the bigger the organ, the more contribution it makes to SMR.) |
False.
An organ's mass does not dictate its contributions to SMR. Some organs are small, but perform service/maintenance functions, and so, require more O2 to operate. |
|
|
What are catabolic reactions? What are coupling reactions?
|
Catabolic rxns produce ATP.
Coupling reactions are downstream reactions that lead to ATP production. |
|
|
What are anabolic rxns? What are uncoupling rxns?
|
Anabolic rxns use ATP and generate heat.
Uncoupling rxns have downstream effects that lead to ATP loss. These include energy leaks, protein degradation, ion leaks, and muscle relaxation. |
|
|
When ATP stores get low, our bodies prioritize what processes get to continue and which don't. What are the "Big 6" processes that get priority?
|
1) Na+/K+ ATPase → Maintains membrane potential; regulates cell volume; charges battery that other processes rely on.
2) Ca2+ ATPase 3) Actinomyosin ATPase 4) Protein turnover 5) Gluconeogenesis 6) Urea synthesis |
|
|
What is the end result of gastrulation?
|
We get a cranial-caudal axis in the blastula.
|
|
|
What structures arise from ectoderm?
|
Epidermis, nais, cornea, epithelium.
Brain, spinal cord, motor neurons, retina. PNS, adrenal medulla, melanoctyes, facial cartilage, dentin of teeth. |
|
|
What structures arise from the mesoderm?
|
Visceral pleura
Peritoneum Vascular endothelium Epi-, Myo-, Endo- cardium Skeleton Uterus Renal tubules |
|
|
What structures arise from the endoderm?
|
Epithelium of yolk sac and allantois
Salivary glands Epithelial linings of respiratory and alimentary tracts |
|
|
What's the difference between hypertrophy and hyperplasia?
|
Hypertrophy = Cells get larger (a size thang)
Hyperplasia = There are more cells (a number thang) |
|
|
What is metaplasia?
|
When cells change their phenotype.
|
|
|
What's the difference between atrophy and hypoplasia?
|
Atrophy = Organ becomes smaller
Hypoplasia = Organ is small from the start |
|
|
You see hemosiderin in macrophages on a blood smear. What does this mean?
|
Hemosiderin in macrophages means that there was hemorrhage nearby.
|
|
|
You see lipofuscin (fine, light brown granules) in cells. What does this mean?
|
Lipofuscin is oxidized lipid-protein waste material. It indicates atrophy, aging, or free radical damage to lipid membranes.
|
|
|
You see melanin in the epidermis of an animal. What could it mean?
|
Solar injury, or just neural crest cells that migrated to the wrong place.
|
|
|
You see Hgb accumulations extracellularly. What does this mean?
|
There is so much RBC lysis that haptoglobin (which binds free Hgb) is saturated. Hgb is delivered to kidneys, making them gunmetal blue.
|
|
|
What are 2 types of cell death?
|
Oncotic necrosis → Can be caused by hypoxia, ATP shortage, or membrane damage. Inflammatory. Cells swell, then shrink.
Apoptosis → Can be caused by cell reduction, receptor-mediated pathways, cell/nuclear damage. Non-inflammatory. Cells shrink. |
|
|
What are the 4 cell systems that are vulnerable to injury (AKA, if these things happen, they lead to cell death)?
|
1) Decreased ATP → Can't fix membranes.
2) Membrane damage → End-stage sign. 3) Increased intracellular Ca2+ → Activates Ca2+ linked enzymes. 4) ROS breakdown cell proteins and damage DNA. |
|
|
Compare the appearance of a reversibly injured cell with that of an apoptotic cell.
|
A reversibly injured cell will exhibit acute cellular swelling, fatty change, and blebs at the membrane.
An apoptotic cell will be small, eosinophilic, and have nuclear changes. |
|
|
What are the 4 different types of oncotic necrosis?
|
1) Coagulation necrosis → Can lead to other types of necrosis.
2) Liquefactive necrosis → Abscesses; typically caused by extracellular bacteria. 3) Caseous necrosis → Like abscesses, but crumbly. 4) Fat necrosis → Typically seen in pancreatitis. |
|
|
Describe the structure of the nucleus and its components. Mention the nuclear envelope, nuclear pores, and nucleolus.
|
Nuclear envelope → Separates the nucleus from the cytosol. Inner surface is coated with nuclear lamins.
Nuclear pores → Structure is composed of 8 proteins. They are found all over the envelope, and are held in place by lamins. Nucleolus → Contains rRNA and ribosomal units. It transcribes rRNA and combines with protein to make incomplete ribosomes. |
|
|
What's the difference b/t an exocrine and an endocrine gland?
|
Exocrine → Gland product is excreted onto SURFACE of organ. On histo, there will be a nearby duct that reaches up to the surface.
Endocrine → Gland product is excreted into BLOOD. On histo, gland will be surrounded by capillaries. *Both are derived from epithelium. |
|
|
How are EXOCRINE glands classified?
|
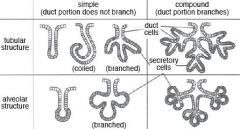
1) Simple vs. Compound → Do ducts branch?
2) Tubular vs. Branched tubular vs. Acinar / Alveolar vs. Tubulo-alveolar/acinar → Secretory region's shape? 3) Mucous vs. Serous vs. Mixed → What does the gland secrete? |
|
|
In reference to exocrine glands: What does it mean when a gland is "simple" or "compound"?
|
Simple gland: Ducts do NOT branch, but the secretory portion can.
Compound gland: Ducts DO branch |
|
|
List the organization of glandular ducts, from large to small.
|
Main duct → Lobar duct → InterLOBULAR duct → Intralobular duct → Striated duct → Intercalated duct → Acinus of gland
|
|
|
What are the 3 methods of glandular secretion?
|
1) Merocrine → Think of typical exocytosis. Vesicle fuses with apical cell membrane and releases contents.
2) Apocrine → Think of budding. Secretion takes a piece of apical cell membrane with it. 3) Holocrine → Cell produces so much secretion that it's released by the cell disintegrating. |
|
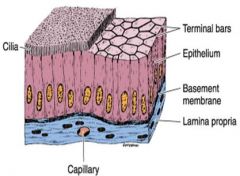
Name this type of epithelium.
|
Simple squamous.
Endothelium → Simple squamous in blood vessels and heart chambers. Mesothelium → Simple squamous lining of pleural, peritoneal, & pericardial cavities. |
|
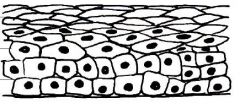
Name this type of epithelium.
|
Simple Cuboidal.
Lines many ducts and tubules. |
|
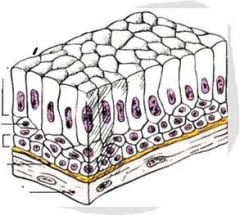
Name this type of epithelium.
|
Simple columnar.
Often have surface modifications like cilia or microvilli. Lines stomach, intestines, and some large ducts. |
|
Name this type of epithelium.
|
(Keratinized) Stratified squamous.
Found on surface of skin and the lining of mouth, cornea, esophagus, and vagina. Non-keratinized version has living, nucleated cells at the surface. |
|
Name this type of epithelium.
|
Stratified columnar.
Rare. Will see where stratified squamous meets simple columnar or pseudostratified columnar. |
|
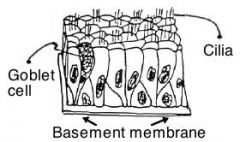
Name this type of epithelium.
|
Pseudostratified columnar.
All cells rest on basal lamina, but may not reach the surface. Found in upper respiratory tract, epididymis, and some large ducts. |
|

Name this type of epithelium.
|
Transitional.
May look different depending on whether the layer is stretched or relaxed. Found in bladder, ureter, & urethra. |
|
|
What type of connective tissue is found in tendons and ligaments?
|
Dense regular.
Collagen bundles. |
|
|
What type of connective tissue is found in spleen, lymph nodes, bone marrow, and liver?
|
Reticular.
Type 3 collagen fibers. |
|
|
What type of connective tissue is found in the dermis, organ capsules, and nerve/muscle sheaths?
|
Dense irregular.
Collagen arranged randomly. |
|
|
What do fibroblasts do, and where are they found?
|
Fibroblasts are found in connective tissues. They produce extracellular matrix.
|
|
|
Describe TYPE 1 collagen. Where is it found?
|
Type 1 = STRENGTH.
Found in: Bone Tendon Ligament Skin |
|
|
Describe TYPE 2 collagen.
|
Type 2 = CARTILAGE.
Thinner fibrils than type 1. |
|
|
Describe TYPE 3 collagen. Where is it found?
|
Type 3 = SUPPORT.
Picks up silver/reticular stains. Found in: Organs Basement membranes |
|
|
Describe TYPE 4 collagen.
|
Type 4 = BASAL LAMINA
|
|

Name this type of muscle.
|
Skeletal muscle.
Striated; multi-nucleated; nuclei are on periphery of fibers. Movement is voluntary. |
|
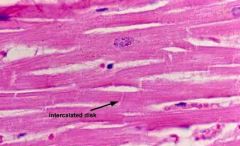
Name this type of muscle.
|
Cardiac muscle.
Striated; fibers branch; one, centrally-located nucleus; intercalated disks connect 2 cells. Movement is involuntary. |
|
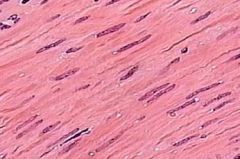
Name this type of muscle.
|
Smooth muscle.
Not striated; one, centrally-located nucleus. Movement involuntary. |
|
|
What is the organization of skeletal muscle?
|
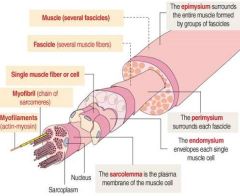
Myofilament → Myofibril → Endomysium (Myocyte) → Perimysium (Fascicle) → Epimysium (Muscle)
|
|
|
Describe the structure of a sarcomere. Discuss the following components:
Actin filaments Myosin filaments Z disks Dark bands / A bands Light bands / I bands |

A sarcomere is the stuff in between 2 Z disks. During contraction, there is more overlap between actin and myosin.
Actin = Thin Myosin = Thick Z disks = Tether actin; hold sarcomeres together. Dark bands = A bands = Myosin length = No change in size Light bands = I bands = Actin only = Length changes |
|
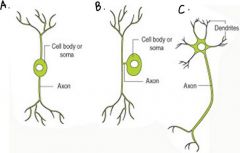
Name the type of neurons A, B, And C.
|
A = Bipolar
B = Pseudo-unipolar C = Multipolar |
|
|
Describe the role of kinesin in transmitting neuronal signals.
|
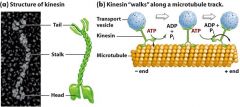
Kinesin "walks" a vesicle of neurotransmitters down an axon, away from the cell body, towards the synapse.
|
|
|
Describe the role of dynein in transmitting neuronal signals.
|
Dynein "walks" vesicles of neurotransmitters retrograde, away from the synapse, back towards the cell body of a neuron.
|
|
|
What is an oligodendrocyte?
|
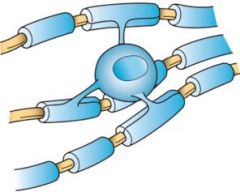
Oligodendrocytes are a type of glial cell (support cell) found in the CNS. One oligodendrocyte wraps around several neuronal axons to provide insulation in the form of a myelin sheath. The gaps in between segments of myelin = Nodes of Ranvier.
|
|
|
What is an astrocyte?
|
Astrocytes are star shaped glial cells in the CNS. Astrocytes have cytoplasmic processes called "end-feet" that cover neurons, inner surface of pia mater (as part of the glia limitans), and every blood vessel of the CNS (as part of the BBB).
|
|
|
What are microglia?
|
They are a type of monocyte that acts like the macrophage of the CNS.
|
|
|
What is a Schwann cell?
|
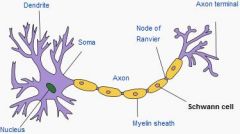
Schwann cells are glial cells of the PNS. One Schwann cell covers / myelinates only ONE neuron. This layer of meylination created by Schwann cells is called the NEUROLEMMA.
|
|
|
Describe neural organization.
|
(Endoneurium (Myelin (Axon) ) ) x Many = (Perineurium (1 Fascicle) )
(Perineurium (1 Fascicle)) x Many = (Epineurium (Nerve) ) |
|
|
On a cross-section of spinal cord, ID:
Dorsal root ganglion Dorsal horn Ventral horn Lateral / Dorsal / Ventral / Medial Funiculi White matter Grey matter Central canal |

|
|
|
True or False:
The spinal cord is lined with dura mater, arachnoid, and pia mater (from outside → in). |
True.
|
|
|
What is the difference between plasma and serum?
|
*The main differences b/t the 2 are:
-Plasma contains fibrinogen, while serum does not. -Plasma is obtained from a blood sample containing anti-coagulant, while serum is not. |
|
|
What are distinguishing characteristics of RBCs in:
Dogs Llamas Goats Birds Reptiles |
Dogs → Larger; prominent central pallor
Llamas → Look like grains of rice Goats → Smaller Birds / Reptiles → Ellipsoid; nucleated |
|
|
True or False:
The bone marrow is the only organ in the entire body to retain its embryological status (i.e., its stem cells can constantly proliferate and differentiate into mature blood cells). |
True.
|
|
|
Define the following terms:
Petechia Purpura Ecchymosis Hematemesis Hematochezia Melena Epistaxis Hematoma Thrombosis Thrombus |
Petechia → Pinpoint hemorrhage
Purpura → < 1cm hemorrhage Ecchymosis → > 1cm hemorrhage Hematemesis → Vomiting blood Hematochezia → Fresh blood in feces; indicates lower GI tract issue Melena → Black, tarry blood in feces; indicates upper GI isseu Epistaxis → Bleeding from nose Hematoma → Localized collection of blood in tissue, usually clotted Thrombosis → Pathological obstruction of blood flow by blood clots Thrombus → Blood clot |
|
|
What is an infarct? What would it look like in heart, kidneys, lungs, intestines?
|
An infarct is tissue necrosis due to lack of O2 from obstructed blood flow.
Heart & Kidney → Infarcts are usually pale Lungs & Intestines → Infarcts are usually red |
|
|
What are the 3 layers of a blood vessel?
|
From inside out:
Tunica intima (Very thin) Tunica media Tunica adventitia |
|
|
What are the steps of angiogenesis?
|
1) Degradation of basal lamina from the sprouting point on parent vessel, & formation of capillary sprout.
2) VEGF causes migration + proliferation of endothelial cells. 3) Endothelial cells mature into endothelial capillary tube. 4) Basal lamina assembles. Smooth muscle cells (periendothelial cells) are recruited. |
|
|
How does a fenestrated capillary differ from a discontinuous capillary?
|
Fenestrated capillaries → While the endothelial cells have incomplete cytoplasm (fenestrations), the basal lamina is continuous.
Discontinuous capillaries → Incomplete cytoplasma + discontinuous basal lamina. |
|
|
What are the four layers of the intestines, from inside → out?
|
From lumen → out:
1) Mucosa 2) Submucosa 3) Tunica muscularis 4) Serosa |
|
|
What is the dorsal root ganglion?
|

The DRG is a collection of cell bodies of sensory nerves in the dorsal root that are transmitting sensory info from the periphery. These sensory nerves synapse onto motor neurons in the grey matter of the spinal cord. Those motor neurons exit the spinal cord via the ventral root to synapse onto muscles.
|
|
|
Where are sympathetic nerve fibers found? What kinds of things do they innervate?
|
Sympathetic nerve fibers are found in the Sympathetic = THORACOLUMBAR region of the spinal cord (T1 - L3).
Sympathetic nerve fibers innervate: Visceral structures Smooth muscle associated with somatic structures |
|
|
Where are parasympathetic nerve fibers found on the spinal cord? What kinds of things do they innervate?
|
Parasympathetic = CRANIOSACRAL
Parasympathetic fibers innervate: Head Thoracic + Abdominal + Pelvic cavities |
|
|
For the SYMPATHETIC nervous system:
1) What neurotransmitter does the pre-ganglionic neuron release? What receptors receive them? 2) What neurotransmitter does the post-ganglionic neuron release? What receptors receive them? |
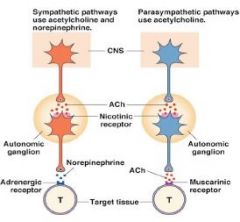
SNS:
1) Preganglionic neurons release ACh onto nicotinic receptors. 2) Postganglionic neurons release norepinephrine onto alpha or beta receptors. |
|
|
For the PARASYMPATHETIC nervous system:
1) What neurotransmitter does the pre-ganglionic neuron release? What receptors receive them? 2) What neurotransmitter does the post-ganglionic neuron release? What receptors receive them? |
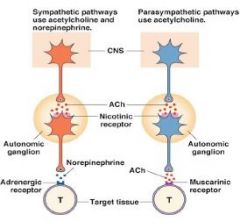
PSNS:
1) Preganglionic neurons release ACh onto nicotinic receptors. 2) Postganglionic neurons release ACh onto muscarinic receptors. |
|
|
What is the only exception to the typical NTs/Receptors that the sympathetic nervous system utilizes?
|
SWEAT GLANDS.
Preganglionic neurons release ACh onto nicotinic receptors (typical). **Postganglionic neurons release ACh (NOT norepi) onto alpha or beta receptors. |
|
|
The 4 interpretive principles of radiology are: Magnification, Distortion, Silhouette, and Summation. What does each of these mean?
|
1) Magnification → The further away an object is from the film, the larger and less distinct it will look on xray.
2) Distortion → Geometry becomes distorted on film. 3) Silhouette → If 2 materials with the same radio-density contact, their borders will be indistinct. 4) Summation → If 2 structures are overlapping/superimposed, their densities will become additive. |
|
|
What does kVp and mAs control on an xray?
|
kVp → Controls the ENERGY of the xray beam. Higher kVp = More exposure (film is darker).
mAs → Controls the amount of xrays that are sent out. Higher mAs = More exposure (film is darker). |
|
|
What is the photoelectric effect?
|
It results in complete absorption of xrays without scatter. Using low energy photons (lower kVp) increases the probability of photoelectric effect happening, leading to increased contrast.
|
|
|
What is Compton scatter?
|
It results in the scattering of x-ray beams, which can decrease image quality. Decrease the amount of Compton scatter that you get by using lower energy photons (lower kVp).
|
|
|
What are the 4 factors contributing to CONTRAST?
|
1) Tissue thickness differences
2) Photoelectric effect 3) Compton scatter 4) Beam energy |
|
|
What technique should we use when radiographing the thorax?
|
-End inspiration to reduce motion.
-Short exposure time, since end-inspiration period is short. -High kVp (80-100), unless patient is small. |
|
|
What technique should you use to radiograph the abdomen?
|
-Take b/t expiration and next inspiration.
-Abdomen doesn't move much with respiration, so longer exposure time is OK. -Use kVp as low as possible (S: < 60; M: 60-80; L: < 90) |
|
|
True or False:
A +/- 15% change in kVp = (kVp/2) or 2(kVp). |
True.
|
|
|
When adjusting our xray technique to correct for over- or under-exposure, where should we start?
|
4x change of kVp
|
|
|
How does frequency and wavelength influence our ultrasound image?
|
A high frequency = Poor penetration, but good resolution. Vice versa for low frequency.
A high wavelength = Good penetration, but poor resolution. Vice versa for low wavelength. |
|
|
Tissues with high acoustic impedance are ___________ on ultrasound.
|
Reflective.
|
|
|
What happens to create a reverberation artifact?
|

US beam is being bounced back and forth between to reflectors. Often, those 2 reflectors are the transducer and gas.
|
|
|
What happens to create a clean shadowing artifact?
|

Shadowing occurs when there is near complete absorption or reflection of US beams. Clean shadowing will be seen to (bright white) mineral or calculi.
|
|
|
What happens to create a dirty shadowing artifact?
|

Shadowing occurs when there is near complete absorption or reflection of US beams. Dirty shadows are seen distal to (white) gas.
|
|
|
What does an acoustic enhancement artifact indicate?
|

We see acoustic enhancement distal to an anechoic structure like fluid.
|
|
|
When would we see an edge shadowing artifact on ultrasound?
|

Edge shadowing occurs distally to a round object.
|
|
|
When do we see mirror image artifacts on ultrasound?
|
Mirror image artifacts occur when the US beam hits a strong reflector. The image that's most distal = the artifact.
|
|
|
True or False:
Radiology and CT rely on differences in tissue densities of structures to produce images. MRI relies on differences in chemical properties of tissues to produce an image. |
True.
|
|
|
When would we use the T1 setting on an MRI?
|
To visualize anatomical detail or when using contrast agents.
|
|
|
When would you use the T2 or FLAIR settings on an MRI?
|
To visualize and ID edema and other fluids.
|
|
|
When would you use the P+ density setting on an MRI?
|
To differentiate grey & white matter in the brain.
|
|
|
True or False:
Enzymes change the equilibrium of a reaction. |
FALSE.
|
|
|
What are the 6 main classes of enzymes?
|
Oxidoreductases → +/- H+
Transferases → +/- functional groups Kinases → +/- phosphate Hydrotases → + H2O Lysases → +/- H2O, NH3, CO2 Isomerases → Rearranges molecule Ligases → Joins 2 groups using ATP |
|
|
In general sense, how do enzymes work?
|
Enzymes lower the activation energy of a given rxn by bringing the reactants together.
|
|
|
What is the K(d) of a reaction?
|
K(d) is the dissociation constant for the enzyme and its substrate. The affinity of an enzyme for its substrate is = 1/K(d).
|
|
|
What does the Michaelis-Menton equation tell us?
|
![It tells us how [substrate] affects the rate of a given enzyme-catalyzed reaction.
To note on image:
1) Vmax → Max rxn rate; this is when all enzyme is saturated with substrate.
2) Vmax/2
3) Km → [Substrate] at which rxn rate is 1/2max. A...](https://images.cram.com/images/upload-flashcards/34/42/97/5344297_m.jpg)
It tells us how [substrate] affects the rate of a given enzyme-catalyzed reaction.
To note on image: 1) Vmax → Max rxn rate; this is when all enzyme is saturated with substrate. 2) Vmax/2 3) Km → [Substrate] at which rxn rate is 1/2max. Also an estimate of the dissociation constant of the enzyme and substrate (smaller Km = higher affinity). |
|
|
What can a Lineweaver-Burk plot tell us?
|
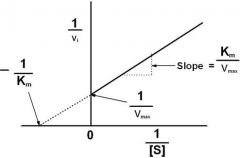
It's just the double reciprocal of MM eqn.
Note on image: → X intercept = -1/Km → Y intercept = 1/Vmax → Slope = Km/Vmax |
|
|
How does a competitive inhibitor affect Vmax and Km?
|
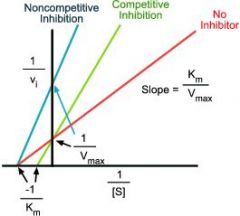
With competitive inhibitors:
Vmax → Same Km → Increases |
|
|
How does a noncompetitive inhibitor affect Vmax and Km?
|
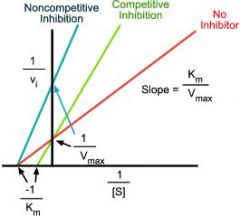
With noncompetitive inhibitors:
Vmax → Decreases Km → Same |
|
|
What are the 4 main principles for regulating [enzyme] in tissues?
|
1) Regulation of gene expression controls quantity and rate of enzyme synthesis.
2) Proteolytic enzyme activity determines rate of enzyme degradation. 3) Covalent modification of pre-existing pools of inactive pro-enzymes produces active enzymes. 4) Compartmentalization of enzymes. |
|
|
In regards to hormones and neurotransmitters:
Which would you expect to have a high Kd, and which a low Kd? |
Hormones have low Kd bc must travel a long way to target receptors. Not much will actually reach the target receptors, so a low Kd (high affinity for receptor) helps them elicit their effect.
NTs have high Kd bc released at high [ ] at synaptic cleft, so don't need high affinity to have effect. Also ensures that signalling is reversible. |
|
|
What is the mechanism behind myasthenia gravis?
|
MA is an autoimmune, neuromuscular DZ. Circulating antibodies block nicotinic receptors at the post-synaptic neuromuscular junction so that ACh cannot bind to them. ACh's normal excitatory effect is blocked.
|
|
|
Describe the events that lead up to an action potential.
|
1) Cell membrane becomes depolarized (more +) from an excitatory neuron synapsing on it, leading to opening of voltage-gated Na+ channels. Na+ rushes into neuron.
2) Voltage-gated K+ channels open, and let K+ out. Membrane potential starts to fall back to resting potential. 3) Na+ channels close at the peak of the AP, while K+ channels remain open, letting K+ out. Membrane potential falls back down and the membrane is hyperpolarized → Refractory period. 4) Resting membrane potential is maintained by K+ leak channels. 4) Since K+ is leaving but not Na+ is coming in, the membrane becomes hyperpolarized. |
|
|
Is glutamate an excitatory or inhibitory neurotransmitter? List glutamate receptors.
|
Glutamate is an excitatory NT; in fact, it's the most abundant excitatory NT in vertebrates.
Glutamate receptors: AMPA receptor NMDA receptor |
|
|
Describe the mechanism behind myotonia congenita (fainting goats / cats).
|
In MC, there's a heritable, genetic mutation of the Cl- channel in muscles that's responsible for shutting off electrical excitation. Muscle fibres have unusually exaggerated response to stimulation → Hyperexcitability.
|
|
|
Describe the mechanism behind hyperkalemia periodic paralysis.
|
HYPP is a heritable mutation that affects Na+ channels in muscle cells and the ability to regulate K+ levels in blood.
When K+ is high (from dietary intake, for ex), Na+ channels fail to inactivate properly; muscles are excitable and the animal may experience sporadic episodes of tremors or paralysis. |
|
|
Describe the mechanism behind malignant hyperthermia.
|
MH is caused by a mutation in the ryanodine receptor 1 channel.
RyRs are intracellular Ca2+ channels that allow Ca2+ to be released from the sarcoplasmic reticulum for skeletal/cardiac muscle contractions. |
|
|
What are ependymal cells?
|
Epithelial lining of the ventricles in brain.
|
|
|
What NTs can a muscarinic receptor bind?
|
Muscarinic receptors can bind:
Muscarine → VERY well ACh → Pretty well Nicotine → Not very well |
|
|
What NTs can nicotinic receptors bind?
|
Nicotinic receptors can bind:
Nicotine → VERY well ACh → Pretty well Muscarine → Not well |
|
|
What makes up the epidemiologic triad?
|
Host, Environment, Agent
|
|
|
What is the difference b/t endemic and epidemic?
|
Endemic → Cases occur regularly with a predictable pattern.
Epidemic → Cases occur in clusters that are in excess of the expected frequency. |
|
|
What is the difference b/t pathogenicity and virulence?
|
Pathogenicity → Ability of an agent to produce clinical DZ.
Virulence → Degree of DZ severity. |
|
|
How does herd immunity work?
|
Being in a group confers resistance bc a critical proportion of the group has been previously exposed / vaccinated / immune. This key fact prevents invasion and spread of an infectious agent.
|
|
|
What are Koch's postulates?
|
1) Suspected agent is in all cases of the DZ.
2) Agent is isolated from the DZ and can be grown serially in pure culture, apart from natural host. 3) Agent produces OG DZ when introduced in experimental host. 4) Agent can be re-isolated from that experimental infection. |
|
|
What criteria must be met in order to deem an exposure "causal"?
|
1) ABSOLUTELY REQUIRED: There must be a temporal relationship; i.e., the exposure must have occurred before the DZ developed.
2) Strong association. 3) Dose responsiveness; i.e., as exposure increases, risk of DZ increases. 4) Findings should be replicable, among different studies and populations. |
|
|
Compare "ratio" with "proportion."
|
Ratio → A:B. Not useful as a probability statistic.
Proportion → A/(A+B). Can use to determine probability. |
|
|
Compare prevalence with incidence.
|
Prevalence → Snapshot in time. Includes all cases at a given point in time.
Incidence → All new cases that occur during a given time interval. |
|
|
How is pharmacokinetics different from pharmacodynamics?
|
Pharmacokinetics = How the tissues affect the drug.
Pharmacodynamics = How the drug affects the tissues. |