![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
152 Cards in this Set
- Front
- Back
|
Where is gastric carcinoma especially prevalent? |
Japan China Eastern Europe South America |
|
|
How does gastric carcinoma present? |
Non-specific (possibly dyspepsia, weight loss, vomiting, dysphagia, anaemia) |
|
|
When do most patients with gastric carcinoma present? |
Too late – when cancer has spread to lymph nodes |
|
|
Name 4 signs of gastric carcinoma. What is the significance of their presence? |

Presence of these signs typically suggest inoperable disease: Signs of stage Troisier's sign (Virchow's node enlargement on the left) Epigastric mass Hepatomegaly Jaundice Ascites Signs of disrupted growth hormone axis Acanthosis nigricans (displayed) |
|
|
How and where do gastric carcinoma spread? |
Locally Lymphatic coeliac lymph nodes ➙ preaortic lymph nodes ➙ intestinal lymph trunk ➙ thoracic duct ➙ Virchow's node Blood-borne Liver (mostly) Transcoelomic (through the cavity) Peritoneum Ovaries |
|
|
Name four imaging modalities used in gastric cancer and explain what they are used for. |
1) Endoscopy + Biopsy (try and biopsy all gastric ulcers) for diagnosis 2) Endoscopic USS to evaluate depth 3) CT/MRI for staging |
|
|
A patient of yours has been diagnosed with gastric cancer and you would like to investigate whether he has peritoneal mets. What test would you request? |
Cytology of peritoneal washings |
|
|
5 year survival of gastric cancer |
< 10% |
|
|
Indication for surgery in gastric cancer |
Can be offered to all but is only possibly curative if the tumour is confined to muscle wall (no involvement of serosa) and limited to lymph nodes in the vicinity (< 3cm) with no mets |
|
|
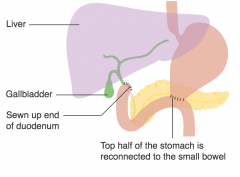
What surgery is done in gastric cancer? Is chemo/radio therapy also used? |
Laparoscopic total gastrectomy + Chemo Pre/Post Note that total gastrectomy also involves removal of the lymph nodes in the vicinity Local resection may be used in symptoms control for palliative purposes.Ou |
|
|
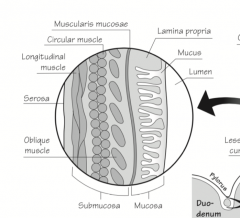
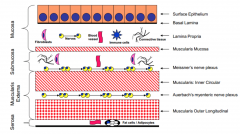
Outline the different layers of the intestinal wall |
|
|
|
Outline the different layers of the gastric wall |
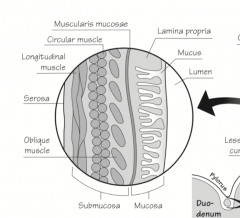
Only the oblique muscle layer differ compared to the intestinal wall |
|
|
Distinguish the function of the body, antrum, and fundus of the stomach and localise them. |
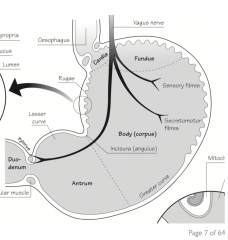
Fundus – Storage Body – Secretes pepsinogen (Chief cells) and HCl (Parietal cells) Antrum – Secretes gastrin (G cells) |
|
|
A patient has had full gastrectomy for early gastric cancer. He now presents with symptoms of peptic ulcer. What has happened? |
Recurrent ulceration, a complication of gastrectomy |
|
|
A patient has had gastrectomy for early gastric cancer. He now presents with upper abdominal pain and vomiting of bile. What has happened? |
Afferent loop syndrome, a complication of some gastrectomy (depending on approach) The afferent loop fills with bile after the meal |
|
|
A patient has had full gastrectomy for early gastric cancer. He now presents with episodes of fainting and sweating after eating. What has happened? How does it happen? |
Dumping syndrome Early dumping: Food of high osmotic potential (esp. sugars) is dumped in the jejunum causing rapid fluid shift and hence reduced circulatory volume. Late dumping: Enormous amount of food reaching the duodenum stimulates inappropriately high insulin secretion thus causing late rebound hypoglycaemia. |
|
|
How can dumping syndrome be improved (3)? |
Eat smaller amounts at a time Eat less sugar and more guar (a form of bean) and pectin (e.g. in apples) |
|
|
What anaemia can occur secondary to gastrectomy? |
Iron deficiency (since iron requires acidic environment to be converted to its absorbable form and is mostly absorbed in the duodenum that is partially resected) => Iron deficiency microcytic anaemia |
|
|
Name one acute and one chronic complication of gastrectomy |
Acute Dumping syndrome Diarrhoea Malabsorption + Complications of any surgery (sepsis, abscess, haematoma) Chronic Anaemia Recurrent ulcers Dumping syndrome Weight loss |
|
|
Outline the two components of the dumping syndrome and their pathogenesis |
Early dumping Food of high osmotic potential (esp. sugars) is dumped in the jejunum causing rapid fluid shift and hence reduced circulatory volume. Late dumping Enormous amount of food reaching the duodenum stimulates inappropriately high insulin secretion thus causing late rebound hypoglycaemia. |
|
|
In which part of the stomach is gastric cancer most likely? |
Pylorus |
|
|
Which peptic ulcer may convert into cancer? |
Those of H. pylori origin (mostly cagA positive H. pylori) NSAIDs is found to slightly decrease the risk of gastric cancer (cancerresearchuk.org) |
|
|
Name 4 RF for gastric cancer |
◾ H. pylori infection (mostly cagA positive) ◾ Smoking ◾ Pernicious anaemia (=> Less acid => More proliferation of bacteria) ◾ Male ◾ Age > 55 (Not alcohol and not NSAIDS – cancerresearchuk.org) |
|
|
Among the following, select those that are recognised risk factors for gastric cancer: H. pylori infection NSAIDs Alcohol Pernicious anaemia |
H. pylori infection Smoking Pernicious anaemia |
|
|
#1, #2 and #3 cancer in males and females and #1 and #2 cancer-related deaths in general UK population |
Cancers #1 Prostate (M) and Breast (F) #2 Lung #3 Colorectal Deaths #1 Lung #2 Colorectal |
|
|
Lifetime incidence of bowel colorectal cancer in the UK |
1:15 |
|
|
Name 3 diseases which are risk factors for colorectal cancer |
Neoplastic polyps UC Crohn's |
|
|
Name 2 lifestyle factors that are risk factors for colorectal cancer |
Alcohol Low-fibre diet Red meat (Smoking is contentious) |
|
|
Name one established preventative treatment for colorectal cancer. Does it reduce incidence or mortality? |
Aspirin reduces incidence and mortality Supposed mechanism: inhibits polyp growth |
|
|
Presentation of colorectal cancer |
Whatever the side Abdominal mass Perforation (emergency) Haemorrhage Fistula Left-sided Bleeding and mucus PR Mass PR (60%) Altered bowel habits Obstruction (Emergency) Tenesmus (feeling like emptying one's bowel) Right-sided Weight loss Anaemia Abdominal pain (Obstruction less likely) |
|
|
What is Tenesmus |
Feeling of incomplete defecation usually due to mass in rectum (e.g. tumour) |
|
|
For the following signs and symptoms of colorectal cancer, name whether they are more likely to present when the tumour is on the left or on the right: Abdomina pain Altered bowel habit Anaemia Bleeding PR Mass PR Mucus PR Tenesmus Weight loss |
Abdomina pain – Right Altered bowel habit – Left Anaemia – Right Bleeding PR – Left Mass PR – Left Mucus PR – Left Tenesmus – Left Weight loss – Right |
|
|
Top 3 likely location of colorectal cancer |
Rectum – 27% Sigmoid colon – 20% Caecum – 14% |
|
|
What may blood tests show in colorectal cancer? |
Microcytic anaemia |
|
|
Name one test that can be used to help diagnose colorectal cancer |
Faecal occult blood test |
|
|
Outline screening program for colorectal cancer |
Faecal occult blood test Positive => Sigmoid colonoscopy |
|
|
Two likely causes of blood streaked on (on the surface of) stool. How can they be distinguished? |
Must be anorectal Rectal tumour: painless Anal tumour: painful |
|
|
Two likely causes of painless blood mixed with stool |
UC Colonic tumour |
|
|
4 causes of painless blood separated from stool |
Haemorrhoids Diverticular disease Angiodysplasia Rapidly bleeding colorectal tumour UC |
|
|
How can UC be distinguished from colorectal tumour clinically? |
UC: typically mucus in stools and may present with pain + extraintestinal signs (2 CLUEs) |
|
|
Two differential for blood on toilet paper. How can they be distinguished? |
Anal fissure: painful Haemorrhoids: painless |
|
|
How can diverticular disease be distinguished from colorectal cancer? |
Diverticular disease: typically blood is separated from stools ("red splash") |
|
|
Name 2 non-modifiable risk factors for colorectal cancer |
Male FHx (e.g. Familial Adenomatous Polyposis) > 60 |
|
|
How and where do colorectal cancers spread? |
Locally Lymphatics Superior and Inferior mesenteric nodes Blood Liver Lung Bone Transcoelomic Peritoneum |
|
|
Most common source of liver mets |
Colon |
|
|
What features of polyps are suggestive of possible conversion to malignancy? |
Polyps suggestive of malignancy arebigger than 1 cm and have a villous component. A benign polyp can turnmalignant due to mutation of DDC and p53 genes. |
|
|
How is colorectal cancer diagnosed? |
Colonoscopy and biopsy |
|
|
Where does lymph from the GIT drain? |
Foregut: Coeliac nodes Midgut: Superior mesenteric nodes Hindgut: Inferior mesenteric nodes |
|
|
How are polyps treated? |
Colonoscopic polypectomy |
|
|
What are polyps? Name two types of polyps. |
Lumps that appear over the mucosa Inflammatory (as seen in IBD) Neoplastic |
|
|
How are colorectal cancer staged? |
Traditionally: Duke's A – Within bowel wall B – Through bowel wall C – A/B + Lymph nodes D – A/B/C + Mets More commonly now: TNM |
|
|
Management of colorectal cancer |
No mets or curable mets – Surgery Right ⟹ Right hemicolectomy Transverse ⟹ Extended right hemicolectomy Left ⟹ Left hemicolectomy Sigmoid ⟹ Sigmpoid colectomy Rectum ⟹ Abdomino-perineal resection + Liver resection if mets in liver Incurable mets – Palliative Chemo Stent Surgery for untreatable symptomatic |
|
|
True or false: if liver mets are present in colorectal cancer, curable surgery is not indicated |
False, it may be indicated if the mets can also be resected |
|
|
Name two histological features of Crohn's |
Fat wrapping Bowel wall thickening Granulomas |
|
|
What two features help differentiate Crohn's from UC? |
Crohn's can involve any part of the GIT (dysphagia, perianal diseases => Crohn's) |
|
|
3 histological features of UC |
Continuous disease Acute mucosal inflammation (limited to mucosa) Crypt architectural distortion (No granulomas) |
|
|
Peaks of diagnosis of Crohn's and UC |
Crohn's: 2nd and 8th decades UC: 2 and 3rd decade and second peak in middle aged men (maybe due to giving up smoking) |
|
|
What non-imaging tests would you do in IBD (6)? |
FBC => Anaemia CRP/ESR => Confirm inflammation U&E LFT Blood culture => Exclude sepsis Stool culture => Exclude C. diff, Campylobacter, E. coli, ... |
|
|
What imaging would you use in IBD? |
Erect XR => Exclude perforation AXR => Toxic megacolon in UC Colonoscopy + Biopsy => Distinguish UC from IBD Small bowel enema => Detects ileal disease in Crohn's MRI => Visualise fistula in Crohn'sH |
|
|
How do symptoms of Crohn's and UC differ? |
UC Diarrhoea with mucus and blood Crohn's Very smelly diarrhoea Both Fever, malaise, weight loss |
|
|
Name one variable that correlates with severity in UC |
Frequency of bowel movements |
|
|
Treatment of IBD |
Tune down the immune system Corticosteroids Non-steroidal immunosuppressants Immune modulators (e.g. infliximab) Surgery |
|
|
When is surgery indicated in Crohn and UC? |
Crohn's – 70% in lifetime Failed therapy Perforation Obstruction from strictures Fistula Abscess UC – 20% in lifetime Failed therapy Perforation Toxic megacolon Massive haemorrhage |
|
|
Name 3 complications of UC and 3 of Crohn's |
Both Haemorrhage Perforation Crohn's Obstruction from strictures Fistula Abscess Malnutrition Iron, B9 and B12 deficiency Osteomalacia (Vit. D deficiency) UC Toxic megacolon |
|
|
How should the diet in IBD be adapted? |
Small frequent meals Plenty of fluids Low-residue diet (white bread, white rice, refined pasta, eggs, cooked vegetables without the peel and seeds) |
|

What is this stoma? What does it drain? |
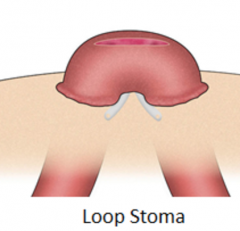
Loop colostomy Proximal end passes stools |
|
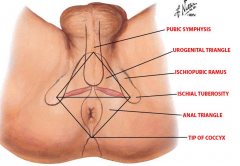
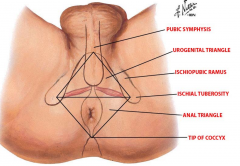
What is this area called? |
Perineum |
|
|
What is the perineum? |
|
|
|
What happens to the distal end of the colon when an end colostomy is placed? |
A) Resected (check perineum for absent anus) B) Closed and left in place C) Exteriorised forming a mucus fistula |
|
|
Name 3 differences that can be observed on examination between an ileostomy and a colostomy |
Content Ileostomy contains a green liquid flowing continuously Colostomy contains solid faecal material that flows intermittently Location Ileostomy: RIF Colostomy: LIF Skin Ileostomy bag is spouted to avoid irritation Colostomy bag is directly by the skin |
|
|
Are colostomy usually permanent or temporary? |
Most are permanent (~ 55%) |
|
|
Name 3 early and 3 late complications of stomas |
Early Haemorrhage at stoma site Stoma ischaemia (of the underlying bowel) High output (=> hypokalaemia) Adhesion and obstruction Stoma retraction Late Obstruction Dermatitis around stoma Stoma prolapse Stomal intussusception Stenosis Fistula Parastomal hernia Psychological problems* |
|
|
What is Hartmann's procedure? Name one example of its application. |

Colonic perforation repair |
|
|
What is resection of the colon called? |
Colectomy |
|
|
Name one indication for colostomy |
Any procedure that requires partial colectomy and for which an anastomosis between proximal and distal end is impractical (e.g. Crohn's, UC, diverticular disease) |
|
|
Name one indication for permanent ileostomy |
Ulcerative colitis that has required panproctocolectomy (removal of colon, rectum, and anus) Uncontrollable rectal bleeding (of any aetiology) |
|
|
Name two indications for temporary ileostomy or colostomy |
They are called defunctioning ileostomies and are used to: Protect (from faecal material) a newly formed anastomosis while it heals and until we test it for leakage |
|
|
Name 3 social consequences of stomas |

Patients should be reassured that the stoma won't change their lifestyle dramatically (for example, they can still go swimming). Patients should be cautious during activities causing pelvic strain (e.g. gardening) Patients are entitled to toilet cards that gives them the right to skip the line and use any bathroom Patients should get used to emptying their stoma. |
|
|
Name 3 psychological consequences of stomas |
Mostly anxiety Quality of life can deteriorate substantially during the first few weeks when the patient does not know what to do if she has to flush the stoma while outside (e.g. shopping) Impact on body image and intimate relationship suffer |
|
|
For the following conditions name what nutrient deficiencies may be present: Crohn's disease Ulcerative colitis Pancreatitis Coeliac disease Gastrectomy |
Crohn's disease Predominantly ileum affected B12 deficiency Iron deficiency due to blood loss and hepcidin (chronic inflammation) Folate, ADEK and fat may be seen if larger portion of intestine affected UC Nothing: it only affects the colon Pancreatitis Fat Protein Iron ADEK B12 (pancreatic enzyme is required to dissociate B12 from stomach-produced haptocorrin that protects B12 from acid) Grossly reduced absorption area Fat Proteins Iron ADEK Folate B12 Gastrectomy Iron B12 Protein |
|
|
What is the pathogen in coeliac? |
Gliadin |
|
|
How does coeliac present ? |
Adults Anaemia, Fatigue, Chronic diarrhoea, Bloating Children Failure to thrive, Diarrhoea, Anaemia |
|
|
How can coeliac be diagnosed? |
IgA against tissue transglutaminase (tTG) + OGD and biopsy |
|
|
Histological presentation of coeliac (3 elements) |
Loss of villi (flatting of mucosal surface) Crypt hyperplasia Intraepithelial lymphocytes ➚ |
|
|
Name 5 signs and symptoms that patients with malabsorption may present with and explain why they arise. |
Steatorrhoea – Fat Metabolic bone disease – Vit D Bruising – Vit K Oedema – Proteins Anaemia – Iron, B12, Folate Neuropathy – B12 Wernicke's encephalopathy – B1 Hypocalcaemia – Ca |
|
|
Three most likely causes of malabsorption in the UK |
Chronic pancreatitis Coeliac Crohn's |
|
|
How does diverticular disease typically present? |
Blood separated from stools ("red splash") or Infection |
|
|
Distinguish diverticulosis, diverticular disease and diverticulitis |
Diverticulosis Presence of diverticula Diverticular disease Symptomatic diverticulosis Diverticulitis Inflammation of the diverticula |
|
|
Most likely location of diverticulum |
Sigmoid colon |
|
|
Prevalence of diverticulosis in elderly? |
50% in 70+ years old |
|
|
How can diverticular disease be diganosed? |
CT – Not endoscopy since there is a risk of rupture |
|
|
What two imaging technology should not be used to investigate diverticulitis and why? |
Colonoscopy Barium injection in rectum⇒ Risk of rupture |
|
|
Histological appearance of diverticulosis |
Mucosa outpouching into muscular layer |
|
|
5 complications of diverticulitis |
Perforation Haemorrhage Fistula (if colovesical, risk of intractable UTI) Abscess Strictures (post-infective) |
|
|
What is thought to cause diverticulosis? |
Increased pressure in the lumen: - Low fibre diet - Constipation |
|
|
Name two diseases that may cause bowel fistula |
Crohn's Diverticulosis |
|
|
How can diverticulitis be diagnosed (from diverticulosis)? |
It's simply the features of inflammation Pyrexia with raised WCC and CRP/ESR Tenderness |
|
|
Name five causes of abdominal perforation |
Pre-bowel Perforated peptic ulcers Bowel Perforated appendicitis Perforated diverticulitis Crohn's Ulcerative colitis Colorectal cancer Extra-bowel Gallbladder perforation |
|
|
A patient with known diverticular disease presents with UTI. What should you suspect? |
Colovesical fistula |
|
|
A patient with known diverticular disease presents with shock. What should you suspect? |
Perforation |
|
|
A patient with known diverticular disease presents with swinging fever. What should you suspect? |
Abscess |
|
|
A patient with known diverticular disease presents with smelly discharge from her vagina. What should you suspect? |
Colovaginal fistula |
|
|
A patient has had surgical operation for a perorated bowel. He now complains of recurrent colickyabdominal pain, distension, and bloating. What should you suspect? |
Strictures |
|
|
A patient with known diverticular disease presents with increased diarrhoea. What should you suspect? |
Entero-colonic fistula (small to large intestine) |
|
|
A patient has had surgical operation for a perorated bowel. He now complains of SOB and has hiccups. What should you suspect? |
Subphrenic abscess |
|
|
What intra-abdominal abscess is particularly concerning? |
Subphrenic abscess "Pus somewhere (i.e. strong evidence of abscess), pus nowhere (i.e. not detected) = pus under the diaphragm (likely occult place)" |
|
|
Why don't diverticulitis occur in the rectum? |
The rectum has a complete outer longitudinal muscle coat |
|
|
Name 3 signs of peritonitis on examination. |
Positive cough test Rebound tenderness Percussion pain Guarding Board-like abdominal rigidity Absent bowel sounds |
|
|
Name 2 signs of peritonitis on general inspection |
Lying still and stretched Shock |
|
|
What is the most important blood test would you request in someone with signs of peritonitis? |
Serum amylase since pancreatitis may present similarly but does not require laparotomy |
|
|
Why would you check serum amylase in someone with signs and symptoms of peritonitis? |
Because pancreatitis may present similarly but does not require laparotomy |
|
|
Commonest cause of peritonitis in young and elderly |
Young: Perforated appendicitis Elderly: Perforated diverticular disease |
|
|
Describe the pain in peritonitis |
Severe generalized abdominal pain radiating to shoulders and back, worse on coughing and moving. |
|
|
Name 3 elements of the immediate management of peritonitis (before establishing the diagnosis) |
Rescucitation IV access Catheterisation Blood (Hb, WCC, CRP, Amylase, U&E, Group and Save) |
|
|
What are the indication for surgery in peritonitis? |
Anything except pancreatitis (contraindicated) |
|
|
Should patients with peritonitis be put on ABx? |
Yes, even if the diagnosis is not clear (most will require ABx prophylactic for the operation anyway) |
|
|
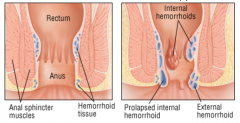
How do haemorrhoids present clinically? |
Some blood on toilet paper Some blood in the toilet that is separated from stools (not a red splash like in diverticulosis though) Painful (external) or painless (internal) |
|
|
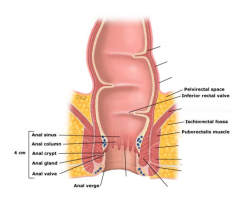
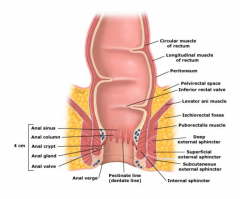
Outline the anatomy of the rectum and anus in a coronal plane and indicate where haemorrhoids form. |
|
|
|
|
|
|
Outline the anatomy of the anus in an axial plane and indicate where haemorrhoids form. |
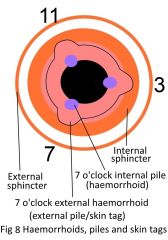
This is where the 3 major arteries feeding the plexus enter. |
|
|
Outline the epithelium of the anal canal. How is this relevant for the diagnosis of haemorrhoids? |
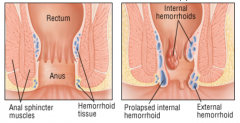
Above dentate line Columnar epithelium (like the rest of the bowel). There is no somatic fibres so that internal haemorrhoids are painless.
Stratified squamous epithelium. There are somatic fibres so that external haemorrhoids can be painful. |
|
|
Significance of painful haemorrhoids |
They must be external, below the dentate lines where the epithelium is stratified squamous. |
|
|
What causes haemorrhoids? |
Increased pressure in the anal canal. Mostly constipation with prolonged straining Vicious circle: vascular cushions protrude through a tight anus ⟹ congestion ⟹ hypertrophy of smooth muscles ⟹ even more congestion |
|
|
What 4 elements of investigation (exam, imaging, tests) would you do in all patients with rectal bleeding? |
1. Abdominal exam 2. PR exam 3. Proctoscopy 4. Sigmoidoscopy |
|
|
A patient presents with small amount of blood separated from the stools. There is no other symptom (no pain, no tenesmus). Abdo exam is unremarkable and so is PR exam. What is it likely to be? |
Internal haemorrhoids (they are not palpable on PR) |
|
|
How would internal haemorrhoids be diagnosed? |
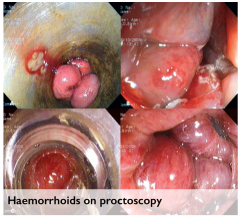
Proctoscopy |
|
|
How would external haemorrhoids be diagnosed? |
Inspection and PR |
|
|
What would you recommend to patients with haemorrhoids to prevent recurrence? |
Avoid constipation ⟹ High fluid and high fibre |
|
|
What is an anal fissure? |
A painful tear in the squamous epithelium of the lower anal canal |
|
|
Where in the lower anus are anal fissure typically located? Why? |
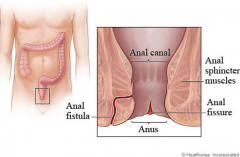
Posterior (90%) as this is a watershed area |
|

|
Haemorrhoids |
|

|
Anal fissure |
|
|
How do anal fissures present? |
Blood on toilet paper and excruciating pain on defecation |
|
|
What is thought to cause and perpetuate anal fissures? |
Hard faeces (possibly worse if poor anal hygiene) The initial fissure may be further perpetuated by spasms that prevent its healing |
|
|
How are anal fissures diagnosed? |

Inspection |
|

|
Perianal haematoma (actually a thrombosed external haemorrhoid) |
|
|
Name 5 conditions that you would look for on inspection of the anus |
Perianal haematoma External haemorrhoids Anal fissure Fistula-in-ano Perianal abscess (as in Crohn's) |
|

|
Fistula-in-ano |
|
|
How do perianal haematoma present? |
The thrombus causes aninflammatory reaction. Sudden onset of pain and oedema (swelling). The pain is: - Sudden onset - Continuous - Worse on sitting and defaecation - Well localised |
|
|
Describe the lump that you expect in perianal haematoma |
Site: anywhere around anal margin Size: 2-4mm (up to 10) Shape: Round Surface: Smooth Skin: Purple Tenderness: Yes Composition: Rubbery and firm Relation: Directly under perianal skin and superficial to external sphincter |
|
|
Name two demographics at risk of perianal fissure |
Young males Mothers after childbirth |
|
|
On examination of what seems to be an anal fissure, a small lump is also detected. What is the diagnosis? |
It is associated with anal fissure so the diagnosis does not change. A small skin tag,often called incorrectly a sentinel pile, may be visibleat the lower end of the fissure. |
|
|
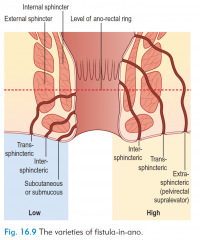
Outline the anal anatomy and show where fistula-in-ano can be |
|
|
|
What causes a fistula-in-ano and why don't they heal? |
An abscess developing in an anal cryptgland in the intersphincteric space that bursts intwo directions – internally into the anal canal, andexternally through the skin. Mucus is forced throughthe fistulous tract as stool is expelled, and this is themechanism that stops a fistula from ever healing. |
|
|
Name one condition that is associated with fistula-in-ano |
Crohn's disease |
|
|
What demographics is at risk of fistula-in-ano? |
Any adult |
|
|
Patient presents with watery orpurulent discharge from his anus. This is small amount at a time and does not look like stool. Likely diagnosis? |
Fistula-in-ano (the description is that of pus from the abscess draining through the fistula) |
|
|
Name 3 elements of the presentation (symptoms) of fistula-in-ano |
- Watery or purulent discharge from the skin around the anus - Tender lump in the perineum - Comes and goes (healing followed by painful dischargesagain) - Itching around the area |
|
|
Characterize the physical signs of fistula-in-ano on examination |
Position: External opening(s) of the fistula visible on the skin Tenderness: the opening is not, but the tissue around it can (as there is pus inside the canal) Discharge visible on the skin or the underwear The internal opening may be palpable in DRE. |
|
|
What are abdominal adhesions? |
Abdominal adhesions are bands of fibrous scar tissue that form on organs in the abdomen. They can cause organs to stick to one another or to the wall of the abdomen. |
|
|
Name the most common, second most common and a random cause of abdominal adhesion |
Surgery #1 Peritonitis #2 Endometriosis #R |
|
|
What are the symptoms of adhesions and what is their timing? |
- Asymptomatic - Obstruction that comes and goes: bouts of crampy abdominal pain - Strangulation: Severe pain, distension and shock |