Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
182 Cards in this Set
- Front
- Back
|
lobar segmental atelectasis
|
endobronchial lesions
extrinsic bronchial compression tumor lymphadenopathy mlaignant benign rare bronchial torsion |
|
|
direct signs of lobar atelectasis
|
displacement of interlobar fissure
increase in opacity of the involvement segment |
|
|
indirect signs of lobar atelectasis
|
displacement of hila
mediastinal displacement elevation of hemidiaphragm overinflation of remaining lung approximation of ribs |
|
|
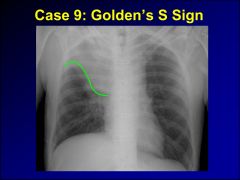
RUL collapse
|
elevation of minor fissure on ap
elevation of minor fissure and proximal major fissure on lateral shift of trachea to the right elevation of hilum thickening of right paratracheal in complete collapse |
|
|
RML collapse
|
best seen on lordotic views
rml syndrome recurrent atelectasis despite an open orifice-absent collateral ventilation, bronchus surrounded by enlarged lymph nodes (TB), mave have coexistent bronchiectasis minor fissure shifts down and major fissure shifts up on AP and lateral |
|
|
RLL collapse
|
triangular opacity in retrocardiac region on pa film with obliteration of the diaphragm
posterior displacement of the right margin posterior displacement of the major fissure on lateral opacity over the spine |
|
|
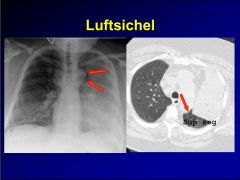
LUL collapse
|
major fissure shifts up on ap and anteriorly on lateral views
maybe difficult to see hazy density, can be easily confused with loculated pleural effusion on PA film luftsichel-radiolucency in upper lung zone that results from upward migration of superior segment of left lower lobe |
|
|
LLL collapse
|
left retrocardiac opacity on pa film
posterior displacement of left major fissure on lateral film |
|
|
CT findings of lobar collapse
|
increased density of collapsed lobe-see primer for pics
|
|
|
types of peripheral atelectasis
|
relaxation
pleural effusion pneumothorax bullous disease atelectasis associated with fibrosis granulomatous infections pneumoconiosis sarcoid resorptive atelectasis secondary to obstruction platelike, discoid atelectasis depletion of surfacant ARDS of newborn radiation injury rounded atelectasis due to pleural disease |
|
|
causes of consolidation
|
fluid in acini
water (edema) cardiac pulmonary edema renal pulmonary edema lung injury, pulmonary edema blood trauma (most common) bleeding disorder; anticoag type II antigen-antibody reaction goodpastures syndrome henoch schonlein purpura pulmonary infarct vasculitis proteinaceous fluid alveolar proteinosis inflammatory exudate in acini infection bacteria infection (pus) nocardia, actinomycosis, TB noninfectious allergic hypersensitivity alveolitis chronic eosinophilic pneumonia BOOP pulmonary infiltration with eosinophilia loefflers sydrome chronic eosinophilic pneumonia pneumonitis ABPA drugs penicillin aspiration of lipid material sarcoid tumor in acini bronchoalveolar carcinoma lymphoma |
|
|
pulmonary renal syndromes
|
syndromes characterized by pulmonary hemorrhage and nephritis
goodpastures (anti-gbm +) wegeners disease (anca +, nodules more common) SLE henoch-schonlein purpura polyarteritis nodosa penicillamine hypersensitivity |
|
|
acute respiratory distress syndrome
characterized by respiratory distress, hypoxemia, opaque stiff lungs diffuse alveolar consolidation--> interstitial fibrosis and scarring |
massive pneumonia
trauma shock sepsis pancreatitis drug overdose near drowning aspiration |
|
|
chronic airspace disease
|
tumors
bronchoalveolar carcinoma lymphoma inflammation tb, fungus eosinophilic pneumonia pneumonitis, boop alveolar sarcoid other causes alveolar proteinosis pulmonary hemorrhage lipoid pneumonia, chronic aspiration |
|
|
approach to pulmonary nodules
|
primer page 88
|
|
|
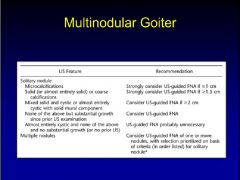
solitary nodules
<6 cm, maybe smooth, lobulated, discrete, circumscribed, calcified, cavitated, or have satellite lesions |
tumor 45%
primary carcinoma 70% hamartoma 15% solitary mets 10% inflammation 53% histoplasmosis tuberculoma coccidiomycosis other 2% vascular 15% AV fistula pulmonary varix (dilated pulmonary vein) infarct, embolism congenital 30% sequestration bronchial cyst miscellaneous 45% round pneumonia loculated effusion in fissure mucous plug enlarged subpleural lymph node silicosis (usually multiple nodules) |
|
|
multiple nodules
multiplicity often indicates hematogenous dissemination |
mets
abscess pyogenic-stapy>kleb>strept immunocompromised pt-nocardia, legionella granulomatous lung diseases infectious tb fungus, aspegillus, histoplasma noninfectious sarcoid rheumatoid nodules silicosis wegeners disease necrotizing granulomatous vasculitis histiocytosis unilateral pulmonary embolism |
|
|
miliary pattern
|
soft tissue opacities
hematogenous-miliary infection, tb, histo hematogenous tumor seeding mets, thyroid, melanoma, breast, choriocarcinoma eosinophilic granuloma bronchioalveolar carcinoma silicosis sarcoid high density opacities |
|
|
calcified lung nodules
|
larger (>1mm)
tumor mets from medullary thyroid cancer mucinous or osteogenic mets infection previous varicella pneumonia histoplasmosis, coccidiomycosis, tb parasites, schistosomiasis other silicosis very small (0.1-1mm; sandlike) alveolar microlithiasis chronic pulmonary venous hypertension metastatic calcification from severe renal disease |
|
|
large (>6cm) thoracic mass
|
pulmonary
tumor bronchogenic carcinoma mets (scc from h&n) abscess round atelectasis intrapulmonary sequestration hyatid disease extrapulmonary fibrous tumor of pleura loculated pleural effusion torsed pulmonary lobe chest wall tumors (askin tumor) AAA mediastinal masses |
|
|
cysts
|
thickness (not always reliable)
<2mm 95% benign 2-15mm 50% malignant >15mm >95% malignant morphology (not reliable) eccentric cavity suggests malignancy shaggy internal margins suggests malignancy |
|
|
cysts
parenchyma-lined spaces, filled with air or fluid |
pneumatocele (posttraumatic, postinfectious), common
bulla (within lung parenchyma), bleb (located within the 9 histologic layers of the visceral pleura) cystic bronchiectasis congenital cysts intrapulmonary bronchogenic cysts (rib and vertebral body anomalies common) cystic adenomatoid malformation (multiple lesions) sequestration hyatid cyst (onion skin appearance) |
|
|
cavity
parenchymal necrosis due to inflammation (benign) or tumor (malignant) |
abscess
pyogenic, staph>kleb>strept immunocompromised pt, nocardia, legionella cavitated tumor SCC (primary scc>head and neck scc> sarcoma mets) sarcoma lymphoma tcc of bladder cavitated granulomatous mass (often multiple) fungus, aspergillus, coccidio (thin wall) tb sarcoid, wegeners, rheumatoid nodules necrotizing granulomatous vasculitis cavitated postraumatic hematoma |
|
|
air crescent sign in cavity
most commonly seen with aspegillosis |
mucormycosis
actinomycosis septic emboli klebsiella pneumoniae tb tumors |
|
|
small cystic disease
|
true cyst wall
eosinophilic granuloma lymphangioleiomyomatosis cystic form of PCP honeycombing in any end-stage interstitial disease no cyst wall emphysema |
|
|
interstitial lung disease: density types
linear or reticular |
thickened interlobular septa, fibrosis
|
|
|
interstitial lung disease: density types
reticulonodular |
inflammation in peribronchovascular interstitium
|
|
|
interstitial lung disease: density types
nodular |
granulomas
|
|
|
interstitial lung disease: density types
ground glass |
usually represents acute interstitial disease (occasionally seen with chronic fibrosis)
hazy density, vessels can be seen |
|
|
interstitial lung disease: density types
honeycombing |
ring shadows 2-10 mm; end stage lung disease
|
|
|
kerley lines (linear densities)
|
kerley B lines, peripehral in interlobular septa
<2cm long peripheral and perpendicular to septa kerley A lines 2-6 cm long central no relationship to bronchioarterial bundles kerley C lines fine network caused by superimposition of kerley B lines |
|
|
interstitial lung disease: approach
|
type of pattern
distribution lung volumes evolution pleural disease lymph nodes |
|
|
interstitial lung disease: general approach
|
due to thickening of interlobular septa (lymphatics, veins, or infiltration by cells), alveolar walls, and interstitium
causes fluid water pulmonary edema venous obstruction (thrombosis) proteinaceous material congenital pulmonary lymphangiectasia (very rare) inflammation infectious (interstitial pneumonia) viral granulomatous (tb, fungal) pcp idiopathic IPF sarcoid collagen vascular disease rheumatoid arthritis scleroderma ankylosing spondylitis extrinsic agents pneumoconiosis (asbestos, silicosis, CWP) drugs tumor interstitial tumors eosinophilic granuloma lymphangitic tumor spread desmoplastic reaction to tumor |
|
|
interstitial lung disease distribution: upper lobes
CASSET P |
cystic fibrosis
ankylsosing spondylitis silicosis sarcoid eosinophilic granuloma (spare cp angles) tb pneumocystis carinii |
|
|
interstitial lung disease distribution: lower lobes
BADAS |
bronchiectasis
aspiration drugs, DIP asbestosis scleroderma, other collagen vascular disease |
|
|
interstitial lung disease evolution: acute
HELP |
hypersentivity (allergic alveolitis)
edema lymphoproliferative pneumonitis, viral |
|
|
interstitial lung disease evolution: chronic
LIFE |
lymphangitis spread
inflammation, infection fibrosis edema |
|
|
interstitial lung disease lung volumes: increased
|
cystic fibrosis
eosinophilic granuloma (20% pneumothorax) lymphangioleiomyomatosis (pneumothorax) |
|
|
interstitial lung disease lung volumes: decreased
|
idiopathic pulmonary fibrosis
scleroderma |
|
|
interstitial lung disease pleural disease
|
pleural plaques
asbestosis pleural effusion chf lymphangitic carcinomatosis rheumatoid disease |
|
|
interstitial lung disease lymph nodes
|
enlarged
malignant adenopathy tb, fungus sarcoid calcified silicosis |
|
|
interstitial lung disease hrct pattern: ground glass opacity
|
allergic hypersentivity
all acute interstitial disease DIP active IPF viral PCP BOOP eosinophilic pneumonia pulmonary edema |
|
|
interstitial lung disease hrct pattern: retriculonodular opacities
peribronchovascular thickening (peribronchial cuffing on cxr) thickening of interlobular septae (kerley lines) |
pulmonary edema
viral, mycoplasma pneumonia, and PCP lymphangitic tumor spread pulmonary fibrosis IPF secondary fibrosis drugs radiation collagen vascular disease hemosiderosis asbestosis |
|
|
interstitial lung disease hrct pattern: nodular opacities
1-2 mm interstitial nodules often associated with reticular opacities |
hematogenous infection
hematogenous mets sarcoid pneumoconiosis silicosis CWP histiocytosis (EG, also cysts) |
|
|
interstitial lung disease hrct pattern: cystic spaces with or without walls
|
lymphangioleiomyomatosis
cystic PCP histiocytosis honecombing IPF any end-stage interstitial disease |
|
|
interstitial lung disease hrct pattern: crazy paving appearance
ground glass with overlying geometric strutures |
pulmonary alveolar proteinosis
ARDS PCP lipoid pneumonia |
|
|
halo pattern of ground glass opacity
|
early invasive aspergillosis in leukemic patient
hemorrhage around a neoplasm post-biopsy pseudonodule |
|
|
peripheral ground glass opacity and consolidation
|
BOOP
infarcts septic emboli collagen vascular disease contusion DIP drug toxicity eosinophilic pneumonia fibrosis sarcoidosis |
|
|
interstitial lung disease hrct pattern: honey combing
|
UIC (IPF)
scleroderma/RA asbestosis chronic hypersensitivity pneumonitis sarcoidosis silicosis EG drug toxicity, bleomycin |
|
|
diseases spreading along bronchovascular bundle
|
sarcoidosis
lymphoma lymphangitic spread of tumor TB kaposi's sarcoma |
|
|
tree-in-bud
|
infection
tb bronchopneumonia fungal asian panbronchiolitis viral pneumonias bronchial disease bronchiolitis congenital disorders cystic fibrosis dyskinetic cilia syndrome other abpf lymphangitic carcinomatosis EG |
|
|
hyperlucent lung
lobar, segmental, subsegmental, generalized, with or without hyperexpansion |
airways
obstruction emphysema, bullae asthma, mucous plug, causes of bronchial obstr. swyer-james syndrome-small in volume, small PA compensatory hyperexpansion of residual lung after surgical lobectomy or chronic lobar collapse cysts congenital hypogenetic lung syndrome congenital lobar emphysema vascular due to oligemia pe pulmonary artery stenosis chest wall abnormalities mastectomy polands syndrome pleural pneumothorax |
|
|
small lung
maybe associated with either decreased or increased density |
hypogenetic lung syndrome
agenesis of pulmonary artery chronic atelectasis bronchiolitis obliterans (Swyer-james syndrome) |
|
|
endobronchial lesions
|
tumors 80%
malignancy 70% scc most common low grade malignancies adenoidcystic carcinoma mucoepidermoid carcinoma small cell carcinoma carcinoid mets 5%, rcc, melanoma, colon, breast, thyroid other, hamartoma, mucoepidermoid carcinoma, hemangioma inflammatory disease 20% tb other mucous plug foreign body trauma broncholith |
|
|
increased tracheal diameter
|
tracheobronchomegaly (Mounier-kuhn disease)
pulmonary fibrosis tracheomalacia |
|
|
decreased tracheal diameter
|
saber-sheath trachea (most common)
tracheopathia osteochondroplastica tracheomalacia (decreased on expiration) relapsing polychondritis amyloidosis sarcoidosis wegeners disease tb and fungal stenosis |
|
|
bronchiectasis
|
postinfectious (most common)
any childhood infection recurrent aspiration abpa: central bronchiectasis chronic granulomatous infection pertussi bronchial obstruction neoplasm foreign body congenital cystic fibrosis bronchial cartilage deficiency, willaims campbell syndrome kartageners syndrome |
|
|
upper lobe bronchiectasis
|
cystic fibrosis
TB radiation abpa, most commonly central, high density mucous plugs highly predictive |
|
|
mucoid impaction
|
asthma
cystic fibrosis abpa congenital bronchial atresia |
|
|
pleural based mass
obtuse angles with chest wall |
tumor
mesothelioma, multifocal, diffuse fibrous tumor of pleural, unifocal maybe locally invasive malignant thymoma, lymphoma mets, breast, lung, prostate, thyroid, renal benign mesenchymal tumore (lipoma, leiomyoma) malignant mesenchymal tumors (fibrosarcoma, MFH, leiomyosarcoma) extrapleural tumors rib tumors children, EG, ABC, ewing's, neuroblastoma adults, mets>multiple myeloma>paget's, fibrous dysplasia plexiform neurofibromas in nf (bilateral) inflammatory infectious, tb asbestos actinomycosis (rib destruction) loculated fluid |
|
|
calcified pleural plaques
TAFT |
tb, usually diffuse plaques
asbestos related plaques, usually focal fluid (empyema, hematoma) talc |
|
|
elevated hemidiaphragm
|
phrenic nerve paralysis
tumor surgery birth defect, erb's paralysis immobility due to pain rib fractures pleuritis, pneumonia pe mass lesions abdominal masses, subphrenic collection, abcess diaphragmatic hernia pleural tumors subpulmonic effusion |
|
|
anterior mediastinal masses
4 T's (thymoma, thyroid lesions, t cell lymphoma, teratoma and germ cell tumors) |
thymic masses
thymic cyst thymolipoma thymoma cystic benign malignant thymic carcinoma thymic carcinoid thymic lymphoma germ cell tumors (m>f) seminoma embryonal cell carcinoma choriocarcinoma teratoma lymphadenopathy due to sarcoid, lymphoma, tb, etc aneurysm and vascular abnormalities (involve both the anterior and superior mediastinal compartments) |
|
|
cystic anterior mediastinal mass
|
thymic cyst (3rd pharyngeal pouch remnant)
cystic thymoma (contains solid components) teratoma bronchogenic cysts (usually in middle mediastinum) pericardial cyst |
|
|
superior mediastinal mass
|
descending through thoracic inlet
thyroid masses adenopathy (1 H&N tumors) lymphatic cysts, cystic hygroma ascending through inlet small cell carcinoma of lung lymphoma aneurysm and vascular anomalies |
|
|
middle mediastinal mass
|
adenopathy (often bilateral)
benign-sarcoid, tb, funal, chronic beryllium exposure malignant-mets, lymphoma, leukemia congenital cysts bronchogenic cysts (subcarinal, anterior trachea) percardial cysts foregut cysts aneurysm aorta, aortic branches pulmonary artery esophagus hiatal hernia neoplasm diverticula megaesophagus other mediastinal hemorrhage mediastinal lipomatosis, lipoma bronchogenic CA aberrant RSA with diverticulum varices neurinoma from recurrent laryngeal nerve malignancy of trachea pancreatic pseudocyst paraganglioma (AP window) lymphangioma and hemangioma tracheal tumor thyroid masses |
|
|
mediastinal adenopathy
|
low attenuation lymph nodes
TB and fungal infections in AIDS necrotic mets lymphoma vascularized lymph nodes castlemans disease vascular mets-renal, thyroid, small cell, melanoma calcified lymph nodes TB histo, fungus sarcoidosis silicosis radiation therapy |
|
|
posterior mediastinal mass
|
neurogenic 90%
peripheral nerves (20-40 years; <2 vert bodies)-schwannoma and neurofibroma 45% sympathetic ganglia (<20; >2 vertebral bodies)-ganglioneuroma, neuroblastoma, sympathicoblastoma paraganglionic cells-pheochromocytoma, paranganglioma lateral meningomyelocele thoracic spine neoplasm hematoma extramedullary hematopoiesis disciitis vascular aneurysm azygous continuation (congenital absence of IV with dilated azygous and hemiazygous) other foregut cyst lymph nodes mass (NHL, mets) esophageal masses and varices |
|
|
cardiophrenic angle mass
|
fat pad (most common)
diaphragmatic hernia morgagni (anterior 90% on right) bochdalek (posterior, more on the left) pericardial cyst cardiophrenic angle nodes (lymphoma usually recurrent s/p radiation) aneurysm dilated right atrium anterior mediastinal mass primary lung or pleural mass |
|
|
fatty mediastinal lesions
|
purely fatty lesions
mediastinal lipomatosis morgagni hernia (omentum) bochdalek hernia (omentum) periesophageal fat herniation tumor with fatty components lipoma liposarcoma thymolipoma (children and young adults) germ cell tumors (also contain ca++, cystic and solid region) |
|
|
high density mediastinal lesions on noncontrast CT
|
calcified lymph nodes
calcified primary mass tumor goiter aneurysm hemorrhage |
|
|
densely enhancing mediastinal mass
|
vascular
aneurysm vascular abnormalities esophageal varices hypervascular tumors-paraganglioma, mets from thyroid cancer, RCC goiter castlemans disease |
|
|
prominent hila
|
tumors
central bronchogenic carcinoma lymphoma adenopathy infectious-tb, fungi, histo inflammatory-sarcoid, silicosis tumor-commonly oat cell, lymphoma, mets pulmonary artery enlargement |
|
|
eggshell calcifications in hilar nodes
|
silicosis, CWP
treated lymphoma granulomatous disease such as histoplasomosis rarely contains egg shell calcifications, diffuse are more common sarcoid (rare and late in disease) |
|
|
pneumomediastinum
|
pulmonary
asthma barotrauma (intubation, diver) childbirth pneumothorax mediastinum tracheobronchial laceration esophageal perforation mediastinal surgery boerhaaves syndrome abdomen intraperitoneal or retroperitoneal bowel perforation retroperitoneal surgery head and neck esophageal rupture facial fractures dental and retropharyngeal infection, mediastinitis |
|
|
asymmetrical interlobular septal thickening
|
lymphangitic spread of carcinoma
|
|
|
idiopathic interstitial pneumonias
|
UI
NSIP OP (organizing pneumonia, BOOP, COP) DIP RB-ILD LIP AIP |
|
|
usual interstitial pneumonia
|
lung volume reduced
reticulation, traction bronchiectasis, and honeycombing GGO uncommon as isolated findings basal, posterior, lower lobe predominance IPF (idiopathic UIP), collagen disease, asbestosis, drug fibrosis, end-stage hypersensitivity pneumonitis |
|
|
honeycombing
|
usually due to UIP
IPF RA, scleroderma, other CVD drug-related fibrosis chronic hypersensitivity pneumonitis asbestosis (uncommon) end-stage sarcoidosis (uncommon) fibrotic NSIP |
|
|
NSIP
|
less common than UIP
homogenous inflammation or fibrosis, cellular (inflammatory) and fibrotic forms common pattern in CVD, drug reaction, idiopathic |
|
|
NSIP imaging findings
|
GGO alone-cellular NSIP
GGO + reticular opacities-cellular or fibrotic NSIP traction bronchiectasis honeycombing = fibrotic nSIP; uncommon, minimal lower lobe, posterior, peripheral predominance sparing of subpleural lung |
|
|
respiratory bronchiolitis and desquamative interstitial pneumonia
|
related to smoking
RB + symptoms = RB-ILD DIP similar histology but more extensive |
|
|
RB-ILD, DIP imaging findings
|
intraalveolar macrophages, little fibrosis
RB-ILD-GGO localized and often centrilobular DIP-GGO more diffuse, maybe patchy and subpleural indistribution |
|
|
consolidation
|
acute
pneumonia edema hemorrhage diffuse alveolar damage chronic organizing pneumonia (OP, BOOP) chronic eosinophilic pneumonia bronchioalveolar carcinoma lipoid pneumonia-fat density or non-fat density, confluent consolidation sarcoidosis, silicosis smoldering infectious pneumonia |
|
|
organizing pneumonia
|
granulation tissue polyps in bronchioles and patchy organizing pneumonia
assoc with BOOP, COP idioapthic, infection, drugs, CVD, fumes |
|
|
organizing pneumonia
|
patchy airspace consolidation or GGO-90%
large nodules or masses-15% peripheral and peribronchial distribution opacities often irregular in shape fibrosis, uncommon, mild atol sign or reversed halo sign |
|
|
chronic eosinophilic pneumonia
|
idiopathic or associated with a known antigen
peripheral eosinophilia months of fever, cough, dyspnea, weight loss identical to BOOP in CT and symptoms peripheral GGO and consolidation upperlobe predominance common |
|
|
ground glass opacity
|
acute
pulmonary edema hemorrhage atypical pneumonia (PCP, viral, etc) diffuse alveolar damage chronic interstitial pneumonia (NSIP, DIP) hypersensitivity pneumonitis organizing pneumonia chronic eosinophilic pneumonia BAC lipoid pneumonia (rare) alveolar proteinosis (rare) |
|
|
hypersentivity pneumonitis
|
acute, subacoute, chronic
repeated exposure leads to fever, chills, dry cough, or dyspnea |
|
|
hypersentivity pneumonitis
imaging findings: subacute stage (typically when imaged) |
patchy ground-glass opacity (75-90%)
ill-defined centrilobular nodules of ground glass opacity (50-60%) mosaic perfusion (patchy lucencies), three types of lucencies (headcheese appearance) air-trapping on expiratory scans diffuse or predominant im the mid lung zones inovles entire cross section of the lung, no subpleural predominance |
|
|
hypersentivity pneumonitis
imaging findings: chronic |
no subpleural predomninance, upper lobes most abnormaly
reticulation and traction bronchiectasis |
|
|
alveolar proteinosis
|
crazy paving appearing
|
|
|
perilymphatic nodules
|
sarcoidosis
lymphangitic spread of tumor silicosis and CWP (uncommon) amyloidosis (rare) LIP (rare) |
|
|
sarcoid
|
mediastinal nodes 60-90%
symmetric hilar LAD, absence of hilar lymph nodes suggest diff dxx, isolated masses unusual 50 % lung disease on cxr cxr staging 1-hilar adenopathy 2-hilar adenopathy + lung dz 3-lung disease only 4-fibrosis perilymphatic nodules, most subpleural, and peribronchovascular, upper lobe predominance upper lobes masses, satellite nodules, "galaxy sign" late-upper lobe fibrosis, fibrotic masses, traction bronchiectasis, cysts, eymphysema |
|
|
silicosis
|
same as sarcoid
progressive massive fibrosis distinguish by history |
|
|
random nodules
|
miliary TB
miliary fungal infections hematogenous metastases sarcoidosis (uncommon) |
|
|
centrilobular nodules (spares pleural surface as opposed to other types)
|
bronchiolitis (ie infectious, inflammatory), most common
respiratory bronchiolitis (smoking) follicular bronchiolitis (cvd, immunosuppression) endobronchial spread of TB, MAC bronchopneumonia (any cause) hypersentivity pneumonitis endobronchial spread of tumor (BAC) pneumoconiosis (ie silicosis) edema, hemorrhage, or vasculitis (uncommon) |
|
|
tree-in-bud
|
endobronchial spread of TB or MAC
bronchopneumonia bronchiectasis, or bronchitis cystic fibrosis aspiration (rare) ABPA, asthma (rare) BAC (rare) |
|
|
emphysema
|
centrilobular-upper lobe predominance, focal lucencies, without walls
panlobular-diffuse, or predominantly lung bases, lung too big, too black, vessels small, cigaretes, alpha 1 paraseptal-beneath pleural surface, involves upperlobes, no fibrosis, can be assoc with centrilobular emphysema |
|
|
lung cysts
|
honeycombing
emphysema (bullae) pneumatoceles associated with pneumonia hypersensitivity pneumonitis (rare) histiocytosis (rare) LAM and TS (rare) Sjogrens syndrome or CVD with lymphoid pneumonia (rare) bronchiectasis misc. causes juvenile trachealaryngeal papillomatosis klippel-trenaunay syndrome neurofibromatosis |
|
|
histiocytosis
|
upper lobe predominance
cysts irregular in shape thick or thin walled sparing of cp angles nodules early smoking related normal to increased lung volumes |
|
|
LAM
|
round cysts
usually thin walled diffuse, random in distribution only in women of childbearing age 1% of TS patients, rarely men 80% recurrent pneumothorax chylothorax death within 10 years from hypoxia |
|
|
LIP
|
round in shape
thin walled diffuse limited in number to a few dozen |
|
|
sonographic evaluation of thyroid nodules
|
|
|
|
relapsing polychondritis
|
diffuse tracheal thickening sparing posterior MB
no ca++ tracheomalacia recurrent pneumonia tx stent |
|
|
focal circumferential tracheal thickening
|
ddx
post intubation stenosis-history wegeners focal, or long concentric thickening subglottic involvement no malacia infection-tb,fungal sarcoid-tracheal inv. 1-3% IBD-rare, late |
|
|
nodular trachea
|
ddx
tracheobronchopathia osteochondroplastica rare, idiopathic, benign no associated malacia spares posterior mb ca++ tracheobronchial amyloidosis nodular irregular or circumferential focal or long ca++ or no ca++ papillomatosis mets |
|
|
tracheobronchomegaly aka munier kuhn
|
atrophy of cartilage and connective tissues of airway wall
tracheomegaly >3cm bronchiectasis malacia |
|
|
tracheal neoplasia
|
90% malignant
primary scc-most common adenoid cystic-posterior maybe circum, ecc mucoepidermoid-airways>>trachea carcinoid-densley enhances, circumscribed, octr scan+ others-sarcoma, adenoca secondary mets direct invasion |
|
|
swyer-james syndrome
|
unilateral bronchiolitas obliterans
due to lower respiratory tract infection in early childhood unilateral lucency lung volume usually decreased, but maybe nl or increased air trapping, bronchiectasis maybe incidental or associated with recurrent infection |
|
|
bronchiolitis obliterans
|
aka constrictive bonchiolitis, not BOOP
fibrosis of peribronchial tissu ddx-transplant rejection, post viral, CVD, inhalation, drugs findings-mosaic perfusion, air trapping, dry bronchiectasis |
|
|
small airways disease (bronchiolitis)
|
ddx
impaction-tree in bud infection, panbronchiolitis inflammation-centrilobular nodules bronchopneumonia, HP, resp bronchiolitis, follicular bronchiolitis, BOOP obstruction-mosaic perfusion pattern, air trapping HP, BO, asthma |
|
|
panbronchiolitis
|
diffuse centrilobular nodules
east asians TIB, nodules bronchiectasis |
|
|
mosaic perfusion
areas of ggo and lucent lung lucent lung sharply distinct vessels diminutive in areas of lucency compared to ggo if lucent lung stays lucent and opaque lung gets denser then mosaic perfusion with small airway dz |
95% result from airways dz-polygonal areas of lucency
rest from small vessel disease-large lucent areas with decreased vascularity ddx asthma hypersentivity pneumonitis constrictive bronchilitis (BO) chronic PE |
|
|
anterior mediastinal masses simplified differential
|
thymoma-thymic tumors and masses
teratoma-germ cell tumors terrible lymphoma-lymphoma and node masses thyroid-thyroid and parathyroid masses tons of other stuff-vascular anomlies, foregut cyst, lymphangioma, hemangioma, benign mesenchymal tumors, sarcoma |
|
|
thymic epithelial tumors
|
most common primary thymic tumor
15-20% primary mediastinal masses peak 50-60 yo, rare < 20 myasthenia gravis-50-60% 10-30% of myasthenia have thymoma types thymoma (invasive/noninvasive) thymic carcinoma spread (local>pleural>extra-thoracic) |
|
|
germ cell tumors
|
10% primary mediastinal masses
teratoma, seminoma, nonseminomatous, mixed most common in anterior mediastinum, 5% posterior 2-4th decades, 80% benign, mostly teratomas benign tumors-m=f malignant tumors m>f benign tumors often asx |
|
|
anterior mediastinal mass-mature (dermoid cyst)
|
60-70% GCT
ca++, fat, soft tissue rupture (pleura, lung, mediastinum) CT-well defined mature elements (fat, fluid) |
|
|
anterior mediastinal mass-seminoma
|
almost entirely men, mean 29yo
20-40% gct large, smooth, or lobulated, homogenous mass sensitive to chemo and rad, good px |
|
|
nonseminomatous GCT
|
mixed bag, similar appearance and behavior
large heterogenous infiltrative mass |
|
|
anterior mediastinal masses: lymphoma
|
hodgkins
85% mediastinal adenopathy prevascular or paratracheal nodes 98% of thoracic disease multiple node groups common low attenuation nodes in 10-20%, ca++ rare nonhodgkins 40-50% thoracic involvement inv of one node group more common than HD inv of posterior nodes more common than HD inv of anterior med nodes less common than HD both types infiltrative, not mass like |
|
|
cardiophrenic angle mass
|
ddx
thymoma and other anterior mediastinal masses pericardial cyst fat pad morgagni hernia lymph node masses lipoma |
|
|
calcified mediastinal lymph nodes
|
ddx
dense ca++-old granulomatous dz, sarcoid egg-shell ca++-silicosis or CWP, sarcoid, TB, treated hodgkins uncommon-metastatic carcinoma or sarcoma (more irregular), untreated lymphoma, PCP, amyloidosis, scleroderma, castleman's disease |
|
|
low-attenuation (necrotic) mediastina lymph nodes
|
ddx
infections (TB and fungus) mets (lung ca, extrathoracic, ie renal cell) lymphoma sarcoidosis (rare) |
|
|
avidly enhancing mediastinal lymph nodes
|
ddx
metastases (renal, thyroid, lung ca, melanoma) TB rare-castleman's disease, angioimmunoblastic lymphadenopathy, sarcoidosis differentiate from enhancing masses (substernal thyroid, carcinoid, lymphangioma, hemangioma, paraganglioma) |
|
|
castleman's disease
|
hyaline vascular and plasma cell types
localized 80% HV type children or young adults enhancing mediastinal mas benign course, resection curative multicentric most PC type adults 40-50 years multiple enhancing nodules, splenomegaly aggressive; associated with anemia, infection, malignancies, LIP, AIDS, neuropathy, POEMS |
|
|
metastatic mediastinal tumor
|
mets from extrathoracic primary to mediastinal or hilar nodes uncommon (3%)
head and neck, GU tract, breast, melanoma location may suggest source paravertebral nodules-abdomen superior med nodes-head and neck internal mammary-breast paracardiac-breast or abdomen |
|
|
mediastinal bronchogenic cyst
|
lined by bronchial epithelium
subcarinal and paratracheal most common may occur in any mediastinal compartment rarely contain air, become infected smoot, round, oval mass fluid (0 HU) or soft tissue attenuation (20-40) MRI or CT (pre and post) for problem solving |
|
|
cystic mediastinal lesions
|
ddx
esophageal duplication cyst-next to esophagus neurenteric cyst-paraspinal cyst, assoc with vertebral anomalies pericardial cyst mesenchymal tumors (leiomyoma) )-looks cystic due to low density, but really enhances |
|
|
distinguishing between posterior mediastinal nerve sheath and ganglion cell tumors
|
nerve sheath
neurofibroma (30yo) schwannoma (40yo) rounded. 1-2 vertebral body segments +/- extension into the neuroforamina pressure erosion of vertebral body or ribs CT-70% low attenuation as low as fluid, heterogenous enhancement ganlion cell neuroblastoma (<5yo) ganglioneuroblastoma (10yo) ganglioneuroma (20yo) long, sausage shaped, multiple vertebral body segments CT similar to nerve sheath tumors |
|
|
causes of pneumothorax
|
traumatic
iatrogenic ie line placement alveolar rupture (ARDS, asthma) bronchopleural fistula (abscess, mets, PCP, lymphangioleiomyomatosis) spontaneous catamenial |
|
|
differentiating lung parenchymal vs pleural/chest wall lesions
|
parenchymal
spherical borders well defined acute angles with periphery pleural/chest wall elliptical/elongated portion of border ill-defined obtuse angles with periphery |
|
|
localized fibrous tumor of the pleura
|
30% malignant
sx's-incidental, chest pain, hypoglycemia, HPO large pleural mass CT solitary pleural mass necrosis +/- ca++ heterogenous but significant enhancement, particularly on delayed images large feeding vessels |
|
|
empyema
|
infected pleural effusion/pus
staph, pneumococcus, tb loculated, exudative effusion thickened enhancing pleura split pleura sign air thoracentesis bronchopleural fistula gas forming organisms treatment epmyema->drainage abcess->antibiotics |
|
|
factors suggesting malignant pleural disease
|
thickening >1cm
significant mediastinal pleural thickening circumferential thickening pleural nodularity chest wall invasion ddx mets lung ca breast ca gi ca melanoma mesothelioma thymoma |
|
|
asbestos related pleural disease
|
pleural effusions
earliest feature often exudative! pleural thickening and enhancement pleural plaques elevated edges high density +/- Ca++ risk for mesothelioma |
|
|
round atelectasis
|
pleural abnormality (ie plaque, effusion)
contact with the pleural abnormality volume loss swirled vessels/bronchi (comet tail sign) must get f/u to exclude cancer |
|
|
fibrothorax
|
calcified pleural with lung volume loss
old tb prior pleural hematoma prior empyema |
|
|
mesothelioma
|
3 types
epithelioid sarcomatoid mixed strong assoc with asbestos exposure 20-40 yr latent period |
|
|
fat containing nodules of the lung
|
hamartoma
lipoma liposarcoma lipoid pneumonia teratoma histoplasmoma (rare) |
|
|
if given a chest x-ray and abnromality is subtle
|
look for notched ribs, missing ribs (lytic lesion) or spine abnormality (osteo)
check trachea and airways look for abnormal air, pneumomediastinum, or in abd consider also congenital absence of pericardium, hiatal hernia or achalasia, anomalous line |
|
|
airway masses
|
ddx
squamous cell carcinoma adenoid cystic carcinoma carcinoid direct invasion, ie esophagus or lung primary mets, melanoma, breast benign tumors ie hamartomas, papillomas |
|
|
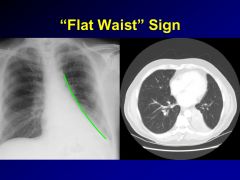
name atelectasis
|
luftsichel-left upper lobe atelectasis
golden s-right upper lobe atelectasis juxtaphrenic peak-upper lobe atelectasis either side comet tail-round atelectasis flat-waist sign-straightening of left heart border in setting of LLL atx |
|
|
pott's disease
|
aka tb spondylitis
destruction of disk and adjacent vertebrae by tb < 1% of tb patients 50% no pulmonary lesions spread via batsons venous plexus subligamentous spread to adjacent vertebrae |
|
|
halo sign and neutropenia
|
angioinvasive aspergillus
|
|
|
bronchiectasis by location
|
upper lobes
cf tb sarcoidosis middle lobe/lingula MAC kartageners central/perihilar abpa williams-campbell lower lobes chronic infection/aspiration, ie blue boater traction bronchiectasis in uip/ipf |
|
|
pneumocystis pneumonia
|
fever, dyspnea, hypoxemia, cough
rare pleural effusions pneumatoceles favoring upper lobes diffuse ggo on cxr in 85% and normal cxr in 15% hrct helps exclude disease in setting of nl cxr |
|
|
ggo centrilobular nodules
|
ddx
hypersensitivity pneumonitis respiratory bronchiolitis atypical infections (acute sx) follicular bronchiolitis (cvd, immunosuppression, rare) |
|
|
dense centrilobular nodules
|
localized, patchy
endobronchial spread of infection (bacteria, mycobacteria) aspiration endobronchial spread of tumor (BAC) diffuse vascular cause (edema, hemorrhage) |
|
|
diffuse tracheal wall thickening
|
sarcoid
amyloid relapsing polychondritis wegener's granulomatosis infection (aspergillus, klebsiella, rhinoscleromatis) tracheobronchopathia osteochondroplastica IBD |
|
|
cystic bronchiectasis lower lungs
|
ddx
post viral infection (childhood) primary ciliary dyskinesia immunodeficiencies ie aggambloulinemia williams campbell tracheobronchomegaly |
|
|
cystic bronchiectasis upper lungs
|
ddx
symmetric cystic fibrosis asymmetric abpa tb endobronchial tumor/stricture bronchial atresia |
|
|
lobar collapse
|
signs
displacement of fissure elevated diaphragm displaced PA mediastinal shift causes mucous plug tumor aspirated foreign body extrinsic compression from tumor or LAD passive collapse and low lung volumes of lower lobes |
|
|
sequestration
|
|
|
|
rml, rll collapse
|

|
|
|
golden s sign
|
|
|
|
luftsichel sign
|
|
|
|
lll collapse
|
|
|
|
crazy paving
|
ddx
acute edema dad/arsp/aip infections hemorrhage hypersensitivity pneumonitis chronic BAC lipoid pneumonia alveolar proteinosis |
|
|
mediastinal soft tissue infiltration
|
ddx
lymphoma leukemia mets ie lung ca acute mediastinitis fibrosing mediastinitis erdheim chester |
|
|
diffuse fibrosing mediastinitis
|
20%
non-calcified not assoc with granulomatous infection associations-autoimmune d/o, retroperitoneal fibrosis |
|
|
focal fibrosing mediastinitis
|
80% cases
paratracheal, subcarinal often ca++ associated with granulomatous infections, ie histoplasmosis |
|
|
perilymphatic nodules
|
ddx
common sarcoid lymphangitic carcinomatosis uncommon silicosis/coal workers pneum amyloid lip |
|
|
progressive massive fibrosis-symmetric bilateral upper lobe masses
|
ddx
silicosis CWP sarcoidosis fungal disease talcosis (high density) |
|
|
multiple cavity nodules
|
ddx
mets infections septic emboli fungal disease (asp) mycobacterial disease nocardia, actino. vasculitis ie wegeners lch rheumatoid nodules tracheobronchial papillomatosis |
|
|
cavitary wall thickness
|
wall thickness
< 5mm benign 5-15mm nonspecific >15mm malignant |
|
|
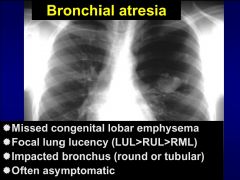
focal lung lucency
|
ddx
bronchial obstruction aspirate fb endobronchial tumor bronchial strictures bronchial atresia sequestration ccam asymmetric bullous diseaes |
|
|
bronchial atresia
|
|
|
|
scimitar syndrome
|
papvr
systemic arterial supply pulmonary hypoplasia small pulmonary artery dextroposition of the heart |
|
|
congenital masses
|
ccam/cpam
cdh sequestration bronchogenic cysts avm |
|
|
ccam/cpam
|
hamartomatous mass
type 1-single or multiple large cysts >2cm diameter type 2-multiple cysts <2cm diameter type 3-solid appearing microcystic maybe assoc with pulmonary hypoplasia or fetal hydrops in adults typically appear as areas of cystic hyperlucency, with recurrent infxn |
|
|
congenital diaphragmatic hernia
|
most common posterolateral (Bockdalek in back), 9/1 on left
solid at birth until swallowed air fills loops may cause pulmonary hypoplasia |
|
|
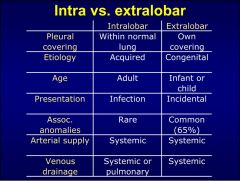
sequestration
|
developments anomaly resulting in disorganized lung parenchyma
intralobe vs extralobar both have systemic art supply favor left lung base |
|
|
bronchogenic cyst
|
cystic anomaly of ventral foregut (dorsal forms esophagus)
most common intrathoracic forgut cyst, more common than esoph duplication cyst usually contain fluid or mucus, with water or high density material mediastinal 86%, intrapulmonary 14% |
|
|
pulmonary avm
|
associated with HHT/OWR
1/3 mult, 1/6 bilat right to left shunt, 20% cardiac output for 1 cm diam dyspnea, cyanosis, clubbing, hemoptysis, paradoxical embo tx with large coils, detach balloons |
|
|
unresectable nonsmall cell lung ca
|
stage 3b and up
anything that has either... t4-tumor invades mediastinal structures, separate tumor nodules in same lobe, tumor with malignant pericardial, pleural effusion n3-mets to contralateral mediastinum or hila, ipsilateral or contralateral scalene, or supraclavicular lymph nodes m1-distant mets including separate lobes |
|
|
lung bx risks
|
pneuthorax 20%
chest tube req 5-10% hemoptysis 5% malignant seeding 0.01% air embolism 0.1% death 0.2% |
|
|
calcified lung masses
|
ddx
metastatic osteosarcoma pulmonary microlithiasis calcified pleural hematoma metastatic calcification calcified tuberculoma |
|
|
airway masses
|
squamous cell ca (distal)
adenoid cystic ca carcinoid direct invasion from esophagus or lung primary mets ie breast, melanoma benign tumors ie hamartomas, papillomas |
|
|
cannonball lung metastases
term for smaller number of large mets typically gi, gu |
ddx
colon ca renal cell ca testicular/ovarian ca osteosarc (often ca++) |
|
|
immunodeficient lung mass
|
PTLD
pulmonary lymphoma kaposis sarcoma-flame shaped nodule, irregular, oblong and hazy margins; usually have mucocutaneous dz bronchogenic ca mass-like infection |
|
|
wegeners granulomatosis
|
systemic small vessel vasculitis assoc with cough, hemoptysis
90% c-anca+ multiple nodules or masses, often with cavitation 50%, less commonly pulm hemorrhage look for sinus, renal dz |