Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
154 Cards in this Set
- Front
- Back
|
What are the layers of the epidermis from the surface to the base?
|
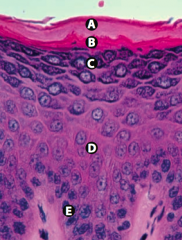
Californians Like Girls in String Bikinis:
- Stratum Corneum (keratin) - Stratum Lucidum - Stratum Granulosum - Stratum Spinosum (spines = desmosomes) - Stratum Basale (stem cell site) |
|
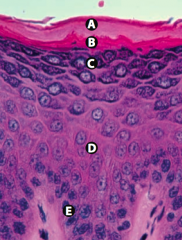
What is Layer A (epidermis)?
|
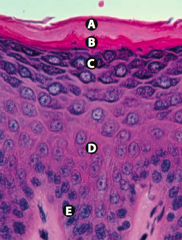
Stratum Corneum (keratin)
|
|
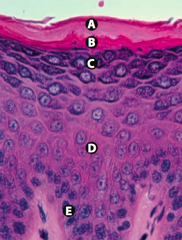
What is Layer B (epidermis)?
|
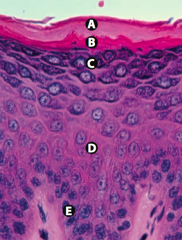
Stratum Lucidum
|
|
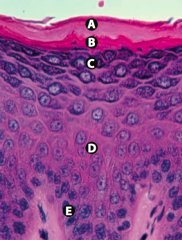
What is Layer C (epidermis)?
|
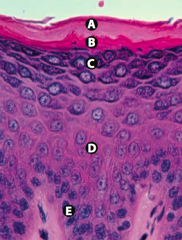
Stratum Granulosum
|
|
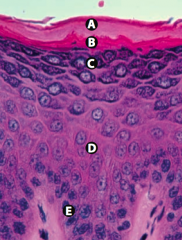
What is Layer D (epidermis)?
|

Stratum Spinosum (spines = desmosomes)
|
|

What is Layer E (epidermis)?
|
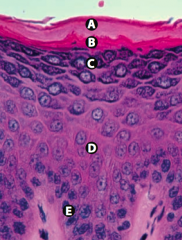
Stratum Basale (stem cell site)
|
|
|
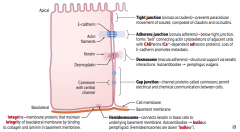
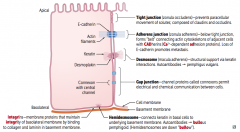
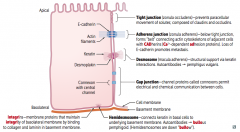
What are the types of junctions between epithelial cells?
|
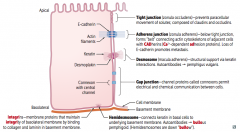
Lateral edge:
- Tight junction / Zonula Occludens - Adherens junction / Zonula Adherens - Desmosome / Macula Adherens - Gap junction Basolateral edge: - Hemidesmosome - Integrins |
|
|
Which type of epithelial cell junction prevents paracellular movement of solutes? What is it composed of?
|
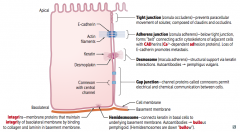
Tight Junctions / Zonula Occludens
- Composed of Claudins and Occludins |
|
|
Which type of epithelial junction is located below the tight junctions, forming a "belt"? What is it composed of?
|
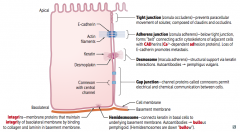
Adherens Junctions / Zonula Adherens
- Composed of actin cytoskeletons of adjacent cells with CADhereins (Ca2+ dependent ADhesion proteins) |
|
|
Which type of epithelial junction provides structural support? What is it composed of?
|
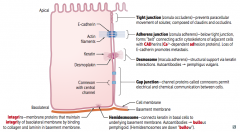
Desmosomes / Macula Adherens
- Keratin interactions - Desmoplakin |
|
|
Which type of epithelial junction permits electrical and chemical communication between cells? What is it composed of?
|
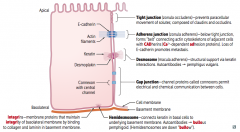
Gap Junction
- Channel proteins called Connexons |
|
|
Which type of epithelial junction connects keratin in basal cells to the underlying basement membrane?
|
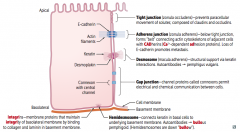
Hemidesmosomes
|
|
|
Which type of epithelial junction binds to collagen and laminin in the basement membrane?
|
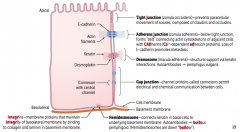
Integrins
- Membrane proteins that maintain the integrity of the basolateral membrane |
|
|
What failure of epithelial cell junctions leads to metastasis?
|
Loss of E-cadherin
|
|
|
What failure of epithelial cell junctions leads to Pemphigus Vulgaris?
|
Desmosomes / Macula Adherens
|
|
|
What failure of epithelial cell junctions leads to Bullous Pemphigoid?
|
Hemidesmosomes (remember, they are down "bullow")
|
|
|
What injury do you suspect in a patient with acute knee pain and an anterior drawer sign?
|
ACL Injury
|
|
|
What injury do you suspect in a patient with acute knee pain and a posterior drawer sign?
|
PCL injury
|
|
|
What injury do you suspect in a patient with acute knee pain and abnormal passive abduction (valgus stress)?
|
MCL injury
|
|
|
What injury do you suspect in a patient with acute knee pain and abnormal passive adduction (varus stress)?
|
LCL injury
|
|
|
What injury do you suspect in a patient with acute knee pain and pain on external rotation (McMurray test)?
|
Medial Meniscus injury
|
|
|
What injury do you suspect in a patient with acute knee pain and pain on internal rotation (McMurray test)?
|
Lateral Meniscus injury
|
|
|
What is a common injury in contact sports due to lateral force applied to a planted leg?
|
Unhappy Triad:
- Classically: damage to ACL, MCL, and medial meniscus - More common: ACL, MCL, and lateral meniscus |
|
|
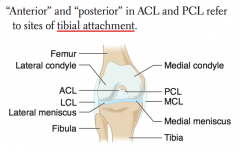
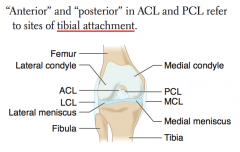
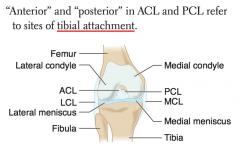
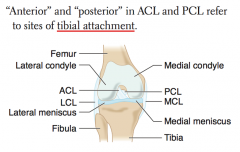
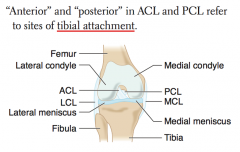
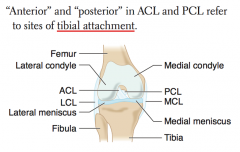
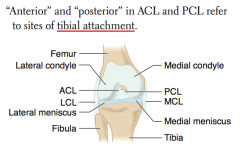
How do you determine which ligament is the ACL vs PCL?
|
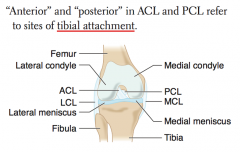
- ACL attaches anteriorly to TIBIA
- PCL attaches posteriorly to TIBIA |
|
|
What important landmark can guide you when doing a pudendal nerve block? Function?
|
- Ischial spines
- Used to relieve pain of delivery |
|
|
What is the classic location of the appendix?
|
- 2/3 of the distance between the umbilicus and the anterior superior iliac spine (ASIS)
- just proximal to the ASIS (McBurney point) |
|
|
What important landmark can guide you when doing a lumbar puncture?
|
Iliac crests
|
|
|
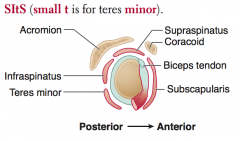
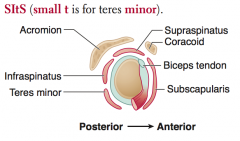
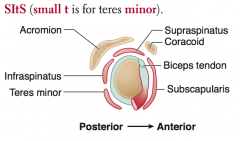
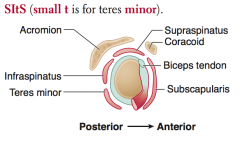
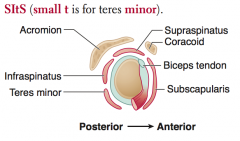
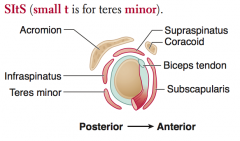
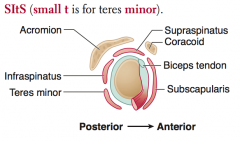
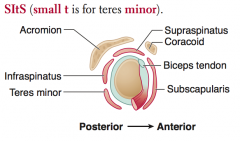
What are the rotator cuff muscles?
|
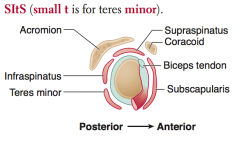
SItS (small t is for teres minor)
- Supraspinatus - Infraspinatus - Teres minor - Subscapularis |
|
|
Which nerves innervate the rotator cuff muscles? Nerve roots?
|
- Supraspinatus: suprascapular nerve
- Infraspinatus: suprascapular nerve - Teres minor: axillary nerve - Subscapularis: subscapular nerve Innervated primarily by C5-C6 |
|
|
What is the action of the rotator cuff muscles?
|
- Supraspinatus: abducts arm initially
- Infraspinatus: laterally rotates arm - Teres minor: adducts and laterally rotates arm - Subscapularis: medially rotates and adducts arm |
|
|
What is the action of the Supraspinatus? Innervation? Other?
|
- Abducts arm initially (before action of deltoid)
- Innervated by Suprascapular nerve *Most common rotator cuff injury |
|
|
What is the action of the Infraspinatus? Innervation? Other?
|
- Laterally rotates arm
- Innervated by Suprascapular nerve *Most common injury in pitchers |
|
|
What is the action of the Teres Minor? Innervation? Other?
|
- Adducts and laterally rotates arm
- Innervated by Axillary nerve |
|
|
What is the action of the Subscapularis? Innervation? Other?
|
- Medially rotates and adducts arm
- Innervated by Subscapular nerve |
|
|
What is the most common rotator cuff muscle injured?
|
Supraspinatus (suprascapular nerve)
|
|
|
What is the muscle classically injured in a pitching injury?
|
Infraspinatus (suprascapular nerve)
|
|
|
What are the bones in the wrist?
|
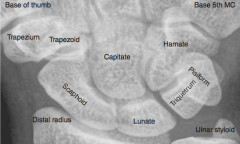
So Long To Pinky, Here Comes The Thumb
- Scaphoid - Lunate - Triquetrum - Pisiform - Hamate - Capitate - Trapezoid - Trapezium |
|
|
What is the most commonly fractured carpal bone?
|
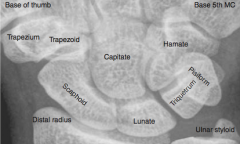
Scaphoid (palpated in anatomical snuffbox)
|
|
|
Which carpal bone is prone to avascular necrosis? Why?
|
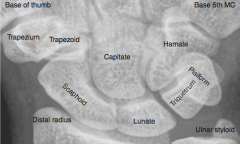
Scaphoid - owing to retrograde blood supply
|
|
|
Dislocation of what bone may cause acute carpal tunnel syndrome?
|
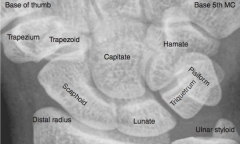
Lunate (medial bone closest to arm)
|
|
|
A fall on an outstretched hand may damage which bone and cause damage to what nerve?
|
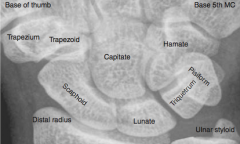
Can damage the hook of the hamate bone, which can cause ulnar nerve injury
|
|
|
What happens in Carpal Tunnel Syndrome?
|
- Entrapment of median nerve in carpal tunnel
- Nerve compression → paresthesia, pain, and numbness in distribution of median nerve |
|
|
What happens in Guyon Canal Syndrome?
|
- Compression of the ulnar nerve at the wrist or hand
- Classically seen in cyclists due to pressure from handlebars |
|
|
Which nerve syndrome is common in cyclists? Why?
|
Guyon Canal Syndrome
- Compression of the ulnar nerve at the wrist or hand - Classically seen in cyclists due to pressure from handlebars |
|
|
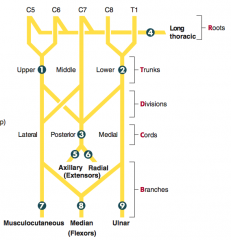
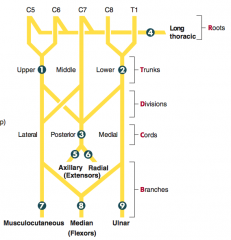
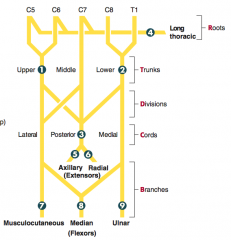
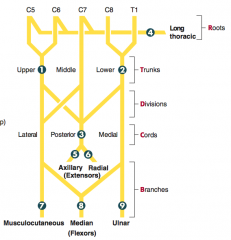
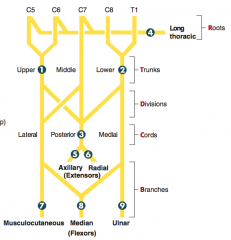
How can you remember the segments of the brachial plexus?
|
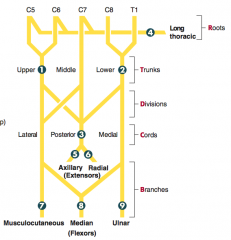
Randy Travis Drinks Cold Beer:
- Roots - Trunks - Divisions - Cords - Branches |
|
|
What are the types of brachial plexus lesions?
|
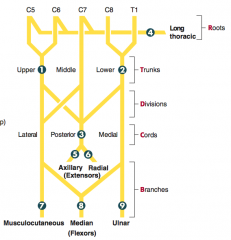
1. Erb palsy (waiter's tip)
2. Claw hand (Klumpke palsy) 3. Wrist drop 4. Winged Scapula 5. Deltoid paralysis 6. Saturday night palsy (wrist drop) 7. Difficulty flexing elbow, variable sensory loss 8. Decreased thumb function (Pope's blessing) 9. Intrinsic muscles of hand, claw hand |
|
|
What injury is caused by traction or tear of the upper trunk (C5-C6 roots)?
|

Erb Palsy (Waiter's tip):
- Deltoid / Supraspinatus deficit → no abduction (arm hangs by side) - Infraspinatus deficit → no lateral rotation (arm medially rotated) - Biceps brachii deficit → no flexion or supination (arm extended and pronated) |
|

What causes Erb Palsy?
|
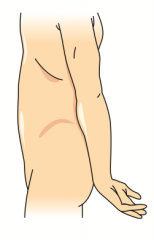
- Traction or tear of upper ("ERB-er") trunk: C5-C6 roots
- Infants: lateral traction on neck during delivery - Adults: trauma |
|
|
What injury is caused by traction or tear of the lower trunk (C8-T1 roots)?
|
Klumpke Palsy
- Intrinsic hand muscle deficits (lumbricals, interossei, thenar, and hypothenar) → Total claw hand - Lumbricals normally flex MCP joints and extend DIP and PIP joints |
|

What causes Klumpke Palsy?
|
- Traction or tear of lower trunk (C8-T1 roots)
- Infants: upward force on arm during delivery - Adults: trauma (eg, grabbing a tree branch to break a fall) |
|
|
What injury is caused by compression of the lower trunk and subclavian vessels?
|
Thoracic Outlet Syndrome
- Intrinsic hand muscle deficits (lumbricals, interossei, thenar, and hypothenar) → atrophy of intrinsic hand muscles - Ischemia, pain, and edema due to vascular compression |
|
|
What causes Thoracic Outlet Syndrome?
|
- Compression of lower trunk and subclavian vessels
- Can be caused by a cervical rib injury or Pancoast tumor |
|
|
What injury is caused by a lesion of the long thoracic nerve?
|

Winged Scapula:
- Deficit of Serratus Anterior muscle → inability to anchor scapula to thoracic cage → cannot abduct arm above horizontal position |
|

What causes Winged Scapula?
|

- Lesion of long thoracic nerve
- May be caused by an axillary node dissection after a mastectomy or stab wounds |
|
|
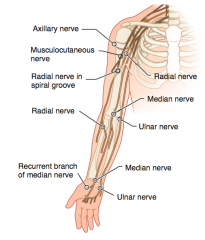
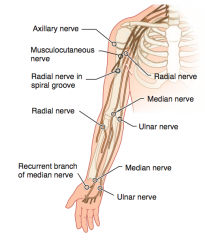
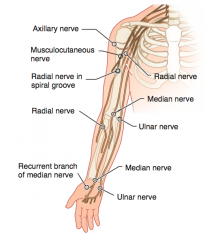
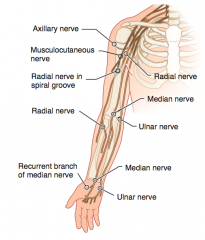
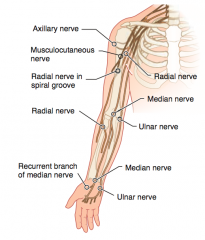
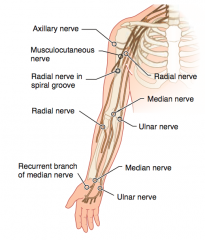
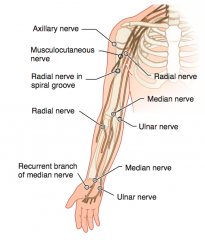
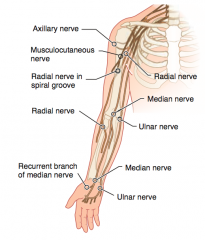
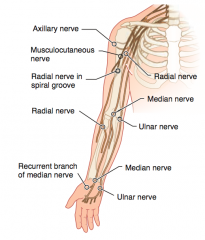
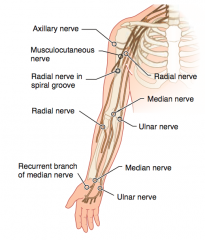
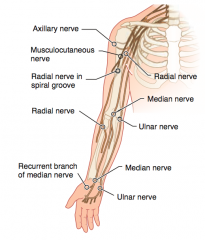
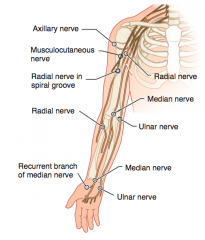
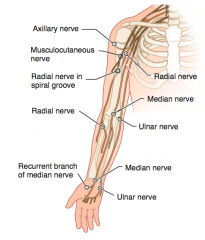
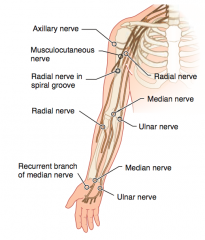
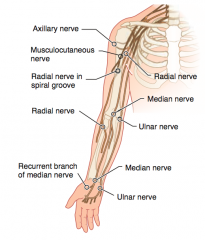
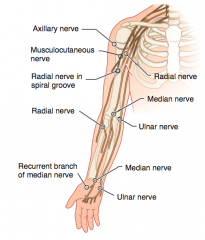
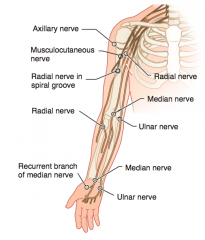
Which nerve roots supply the Axillary nerve? How can it be injured? Presentation of injury?
|

- C5-C6
- Causes of injury: fractured surgical neck of humerus, anterior dislocation of humerus - Presentation: flattened deltoid, loss of arm abduction at shoulder (>15°), loss of sensation over deltoid muscle and lateral arm |
|
|
Which nerve roots supply the Musculocutaneous nerve? How can it be injured? Presentation of injury?
|
- C5-C7
- Causes of injury: upper trunk compression - Presentation: loss of forearm flexion and supination, loss of sensation over lateral forearm |
|
|
Which nerve roots supply the Radial nerve? How can it be injured? Presentation of injury?
|
- C5-T1
- Causes of injury: midshaft fracture of humerus, compression of axilla (eg, d/t crutches or sleeping with arm over chair = Saturday night palsy) - Presentation: wrist drop - loss of elbow, wrist, and finger extension, ↓ grip strength (wrist extension necessary for maximal action of flexors), loss of sensation over posterior arm/forearm and dorsal hand |
|
|
Which nerve roots supply the Median nerve? How can it be injured? Presentation of injury?
|
- C5-T1
- Causes of injury: supracondylar fracture of humerus (proximal lesion), carpal tunnel syndrome and wrist laceration (distal lesion) - Presentation: "ape hand" and "Pope's blessing"; loss of wrist and lateral finger flexion, thumb opposition, lumbricals of 2nd and 3rd digits; loss of sensation over thenar eminence and dorsal and palmer aspects of lateral 3.5 fingers w/ proximal lesion - Tinel sign (tingling on percussion) in carpal tunnel syndrome |
|
|
Which nerve roots supply the Ulnar nerve? How can it be injured? Presentation of injury?
|
- C8-T1
- Cause of injury: fracture of medial epicondyle of humerus "funny bone" (proximal lesion); fractured hook of hamate (distal lesion) - Presentation: "Ulnar claw" on digit extension; radial deviation of wrist upon flexion (proximal lesion); loss of flexion of wrist and medial fingers, abduction and adduction of fingers (interossei), actions of medial 2 lumbrical muscles; loss of sensation over medial 1.5 fingers including hypothenar eminence |
|
|
Which nerve roots supply the recurrent branch of median nerve? How can it be injured? Presentation of injury?
|
- C5-T1
- Cause of injury: superficial laceration of palm - Presentation: "Ape hand"; loss of thenar muscle group - opposition, abduction, and flexion of thumb; no loss of sensation |
|
|
What kind of injury can cause flattening of the deltoid?
|
- Fractured surgical neck of humerus or anterior dislocation of humerus
- Injures the axillary nerve (C5-C6) |
|
|
What kind of injury can cause loss of arm abduction at the shoulder (>15 degrees)?
|
- Fractured surgical neck of humerus or anterior dislocation of humerus
- Injures the axillary nerve (C5-C6) |
|
|
What kind of injury can cause loss of sensation over the deltoid muscle and lateral arm?
|
- Fractured surgical neck of humerus or anterior dislocation of humerus
- Injures the axillary nerve (C5-C6) |
|
|
What kind of injury can cause loss of forearm flexion and supination?
|
- Upper trunk compression
- Injures the musculocutaneous nerve (C5-C7) |
|
|
What kind of injury can cause loss of sensation over the lateral forearm?
|
- Upper trunk compression
- Injures the musculocutaneous nerve (C5-C7) |
|
|
What kind of injury can cause a wrist drop (loss of elbow, wrist, and finger extension)?
|
- Midshaft fracture of humerus or compression of axilla (eg, due to crutches or sleeping with arm over chair)
- Injures the radial nerve (C5-T1) |
|
|
What kind of injury can cause decreased grip strength?
|
- Midshaft fracture of humerus or compression of axilla (eg, due to crutches or sleeping with arm over chair)
- Injures the radial nerve (C5-T1) - Wrist extension is necessary for maximal action of the flexors |
|
|
What kind of injury can cause loss of sensation over the posterior arm / foream and dorsal hand?
|

- Midshaft fracture of humerus or compression of axilla (eg, due to crutches or sleeping with arm over chair)
- Injures the radial nerve (C5-T1) |
|
|
What kind of injury can cause the hand to give the "Pope's blessing"?
|
- Supracondylar fracture of humerus (proximal lesion)
- Carpal tunnel syndrome or wrist laceration (distal lesion) - Injures the median nerve (C5-T1) |
|
|
What kind of injury can cause loss of wrist and lateral finger flexion, thumb opposition, and movement of lumbricals on 2nd and 3rd digits?
|
- Supracondylar fracture of humerus (proximal lesion)
- Carpal tunnel syndrome or wrist laceration (distal lesion) - Injures the median nerve (C5-T1) |
|
|
What kind of injury can cause loss of sensation over the thenar eminence and dorsal and palmar aspects of the lateral 3.5 fingers?
|

- Supracondylar fracture of humerus (proximal lesion)
- Injures the median nerve (C5-T1) |
|
|
What kind of injury can cause the Tinel sign (tingling on percussion)?
|

- Carpal tunnel syndrome (distal lesion)
- Injures the median nerve (C5-T1) |
|
|
What kind of injury can cause the "ulnar claw" on digit extension?
|
- Fracture of medial epicondyle of humerus "funny bone" (proximal lesion)
- Fractured hook of hamate (distal lesion) - Injures the ulnar nerve (C8-T1) |
|
|
What kind of injury causes radial deviation of the wrist upon flexion?
|
- Fracture of medial epicondyle of humerus "funny bone" (proximal lesion)
- Injures the ulnar nerve (C8-T1) |
|
|
What kind of injury causes loss of flexion of wrist and medial fingers, abduction and adduction of fingers (interossei), and actions of medial 2 lumbrical muscles?
|
- Fracture of medial epicondyle of humerus "funny bone" (proximal lesion)
- Fractured hook of hamate (distal lesion) - Injures the ulnar nerve (C8-T1) |
|
|
What kind of injury causes loss of sensation over the medial 1.5 fingers including the hypothenar eminence?
|

- Fracture of medial epicondyle of humerus "funny bone" (proximal lesion)
- Fractured hook of hamate (distal lesion) - Injures the ulnar nerve (C8-T1) |
|
|
What kind of injury causes loss of thenar muscle group movement (opposition, abduction, and flexion of thumb)?
|
- Superficial laceration of palm
- Injures the recurrent branch of the median nerve (C5-T1) |
|
|
What nerve is commonly injured in a fracture of the surgical neck of the humerus? Presentation?
|
Axillary Nerve (C5-C6)
- Flattened deltoid - Loss of arm abduction at shoulder (>15°) - Loss of sensation over deltoid muscle and lateral arm |
|
|
What nerve is commonly injured in an anterior dislocation of the humerus? Presentation?
|
Axillary Nerve (C5-C6)
- Flattened deltoid - Loss of arm abduction at shoulder (>15°) - Loss of sensation over deltoid muscle and lateral arm |
|
|
What nerve is commonly injured in an upper trunk compression? Presentation?
|
Musculocutaneous nerve (C5-C7)
- Loss of forearm flexion and supination - Loss of sensation over lateral forearm |
|
|
What nerve is commonly injured in a midshaft fracture of the humerus? Presentation?
|

Radial nerve (C5-T1)
- Wrist drop - loss of elbow, wrist, and finger extension, - ↓ Grip strength (wrist extension necessary for maximal action of flexors) - Loss of sensation over posterior arm/forearm and dorsal hand |
|
|
What nerve is commonly injured by using crutches or by sleeping with ones arm over a chair?
|

Radial nerve (C5-T1)
- Wrist drop - loss of elbow, wrist, and finger extension, - ↓ Grip strength (wrist extension necessary for maximal action of flexors) - Loss of sensation over posterior arm/forearm and dorsal hand |
|
|
What nerve is commonly injured by a suprocondylar fracture of the humerus?
|

Median nerve (C5-T1) = proximal lesion
- "Ape hand" and "Pope's blessing" - Loss of wrist and lateral finger flexion, thumb opposition, lumbricals of 2nd and 3rd digits - Loss of sensation over thenar eminence and dorsal and palmer aspects of lateral 3.5 fingers w/ proximal lesion - Tinel sign (tingling on percussion) in carpal tunnel syndrome |
|
|
What nerve is commonly injured by carpal tunnel syndrome and wrist laceration?
|

Median nerve (C5-T1) = distal lesion
- "Ape hand" and "Pope's blessing" - Loss of wrist and lateral finger flexion, thumb opposition, lumbricals of 2nd and 3rd digits - Loss of sensation over thenar eminence and dorsal and palmer aspects of lateral 3.5 fingers w/ proximal lesion - Tinel sign (tingling on percussion) in carpal tunnel syndrome |
|
|
What nerve is commonly injured by a fracture of the medial epicondyle of the humerus?
|

Ulnar nerve (C8-T1) = proximal lesion at funny bone
- "Ulnar claw" on digit extension - Radial deviation of wrist upon flexion (proximal lesion) - Loss of flexion of wrist and medial fingers, abduction and adduction of fingers (interossei), actions of medial 2 lumbrical muscles - Loss of sensation over medial 1.5 fingers including hypothenar eminence |
|
|
What nerve is commonly injured by a fractured hook of hamate?
|

Ulnar nerve (C8-T1) = distal lesion
- "Ulnar claw" on digit extension - Radial deviation of wrist upon flexion (proximal lesion) - Loss of flexion of wrist and medial fingers, abduction and adduction of fingers (interossei), actions of medial 2 lumbrical muscles - Loss of sensation over medial 1.5 fingers including hypothenar eminence |
|
|
What nerve is commonly injured by a superficial laceration of the palm?
|
Recurrent branch of the median nerve (C5-T1)
- "Ape hand" - Loss of thenar muscle group: opposition, abduction, and flexion of thumb - No loss of sensation |
|
|
At rest, what kind of balance exists in the hand?
|
Balance between the extrinsic flexors and extensors of the hand, as well as the intrinsic muscles of the hand - particularly the lumbrical muscles (flexion of MCP, extension of DIP and PIP joints)
|
|
|
What most commonly causes "clawing" of the hand?
|
Distal lesions of median or ulnar nerves
- Remaining extrinsic flexors of digits exaggerate the loss of the lumbricals → fingers extend at MCP, flex at DIP and PIP joints |
|
|
What are the implications of a lesion in the distal ulnar nerve?
|

"Ulnar Claw" sign: occurs when extending fingers / at rest
|
|
|
What are the implications of a lesion in the distal median nerve?
|

"Median Claw" sign: occurs when extending fingers / at rest
|
|
|
What are the implications of a lesion in the proximal ulnar nerve?
|

"OK gesture" (w/ digits 1-3 flexed): occurs when making a fist
|
|
|
What are the implications of a lesion in the proximal median nerve?
|

"Pope's Blessing": occurs when making a fist
|
|

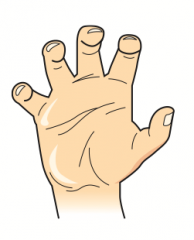
What can cause this hand presentation?
|

- Lesion of distal ulnar nerve: occurs when extending fingers / at rest (Ulnar claw)
- Lesion of proximal median nerve: occurs when making a fist (Pope's blessing) |
|

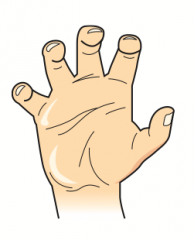
What can cause this hand presentation?
|

- Lesion of distal median nerve: occurs when extending fingers / at rest (Median claw)
- Lesion of proximal ulnar nerve: occurs when making a fist (OK gesture) |
|
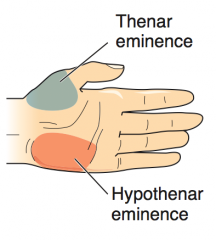
What causes atrophy of the thenar eminence (unopposable thumb)?
|
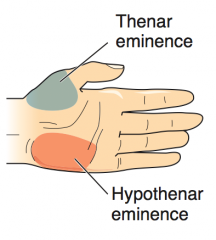
Median nerve lesions
|
|
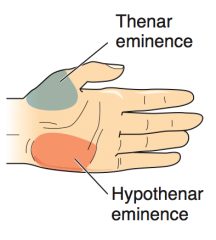
What causes atrophy of the hypothenar eminence?
|
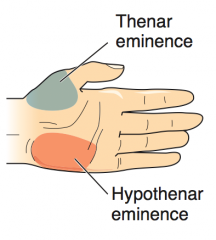
Ulnar nerve lesions
|
|
|
What are the Thenar muscles? What innervates them?
|
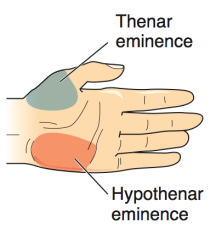
- Opponens pollicis
- Abductor pollicis brevis - Flexor pollicis brevis - Innervated by median nerve |
|
|
What are the Hypothenar muscles? What innervates them?
|
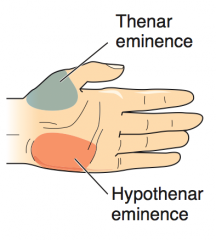
- Opponens digiti minimi
- Abductor digiti minimi - Flexor digiti minimi brevis - Innervated by ulnar nerve |
|
|
What are the types of interosseous muscles? Actions?
|
- Dorsal interosseous muscles: ABduct the fingers = DAB
- Palmar interosseous muscles: ADduct the fingers = PAD |
|
|
What is the action of the lumbrical muscles?
|
- Flex at MCP joint
- Extend PIP and DIP joints |
|
|
What are the nerves in the lower extremity? Nerve roots?
|
- Obturator (L2-L4)
- Femoral (L2-L4) - Common Peroneal (L4-S2) - Tibial (L4-S3) - Superior Gluteal (L4-S1) - Inferior Gluteal (L5-S2) |
|
|
What nerve roots supply the Obturator nerve? What can classically cause injury to this nerve? Presentation?
|
- L2-L4
- Cause of injury: pelvic surgery - Presentation: ↓ thigh sensation (medial) and ↓ adduction |
|
|
What nerve roots supply the Femoral nerve? What can classically cause injury to this nerve? Presentation?
|
- L2-L4
- Cause of injury: pelvic fracture - Presentation: ↓ thigh flexion and leg extension |
|
|
What nerve roots supply the Common Peroneal nerve? What can classically cause injury to this nerve? Presentation?
|
- L4-S2
- Cause of injury: trauma or compression of lateral aspect of leg, fibular neck fracture - Presentation: foot drop - inverted and plantarflexed at rest, loss of eversion and dorsiflexion; "steppage gait"; loss of sensation on bottom of foot |
|
|
What nerve roots supply the Tibial nerve? What can classically cause injury to this nerve? Presentation?
|
- L4-S3
- Cause of injury: knee trauma, Baker cyst (proximal lesion), tarsal tunnel syndrome (distal lesion) - Presentation: inability to curl toes and loss of sensation on sole of foot; in proximal lesions, foot everted at rest with loss of inversion and plantarflexion |
|
|
What nerve roots supply the Superior Gluteal nerve? What can classically cause injury to this nerve? Presentation?
|
- L4-S1
- Cause of injury: posterior hip dislocation, polio - Presentation: Trendelenburg sign/gait - pelvis tilts because weight-bearing leg cannot maintain alignment of pelvis through hip abduction (superior nerve → medius and minimus); lesion is contralateral to side of hip that drops, ipsilateral to extremity on which the patient stands |
|
|
What nerve roots supply the Inferior Gluteal nerve? What can classically cause injury to this nerve? Presentation?
|
- L5-S2
- Cause of injury: posterior hip dislocation - Presentation: difficulty climbing stairs, rising from seated position; loss of hip extension (inferior nerve → maximus) |
|
|
Which nerve is commonly injured by pelvic surgery? Presentation?
|
Obturator Nerve (L2-L4)
- ↓ Thigh sensation (medial) - ↓ Adduction |
|
|
Which nerve is commonly injured by pelvic fracture? Presentation?
|
Femoral Nerve (L2-L4)
- ↓ Thigh flexion - ↓ Leg extension |
|
|
Which nerve is commonly injured by trauma or compression of the lateral aspect of the leg? Presentation?
|
Common Peroneal Nerve (L4-S2)
- Foot drop: inverted and plantarflexed at rest, loss of eversion and dorsiflexion - Steppage gait - Loss of sensation on dorsum of foot *PED = Peroneal Everts and Dorsiflexes; if injured, foot dropPED* |
|
|
Which nerve is commonly injured by a fibular neck fracture? Presentation?
|
Common Peroneal Nerve (L4-S2)
- Foot drop: inverted and plantarflexed at rest, loss of eversion and dorsiflexion - Steppage gait - Loss of sensation on dorsum of foot *PED = Peroneal Everts and Dorsiflexes; if injured, foot dropPED* |
|
|
Which nerve is commonly injured by knee trauma? Presentation?
|
Tibial Nerve (L4-S3)
- Inability to curl toes - Loss of sensation on soles of foot - In proximal lesions (knee trauma or Baker cyst), foot everted at rest with loss of inversion and plantarflexion *TIP = Tibial Inverts and Plantarflexes; if injured, can't stand on TIPtoes* |
|
|
Which nerve is commonly injured by a Baker cyst? Presentation?
|
Tibial Nerve (L4-S3)
- Inability to curl toes - Loss of sensation on soles of foot - In proximal lesions (knee trauma or Baker cyst), foot everted at rest with loss of inversion and plantarflexion *TIP = Tibial Inverts and Plantarflexes; if injured, can't stand on TIPtoes* |
|
|
Which nerve is commonly injured by tarsal tunnel syndrome? Presentation?
|
Tibial Nerve (L4-S3)
- Inability to curl toes - Loss of sensation on soles of foot *TIP = Tibial Inverts and Plantarflexes; if injured, can't stand on TIPtoes* |
|
|
Which nerve is commonly injured by a posterior hip dislocation? Presentation?
|
Superior Gluteal Nerve (L4-S1)
- Trendelenburg sign / gait - Innervates gluteus medius and minimus Inferior Gluteal Nerve (L5-S2) - Difficulty climbing stairs, rising from seated position - Loss of hip extension - Innervates gluteus maximus |
|
|
Which nerve is commonly injured by polio? Presentation?
|
Superior Gluteal Nerve (L4-S1)
- Trendelenburg sign / gait - Innervates gluteus medius and minimus |
|
|
What are the characteristics of Trendelenburg sign / gait?
|
- Pelvis tilts because weight-bearing leg cannot maintain alignment of pelvis through hip abduction
- Superior nerve innervates medius and minimus - Lesion is contralateral to the side of hip that drops - Lesion is ipsilateral to extremity on which the patient stands |
|
|
What nerve roots supply the Sciatic nerve? Function?
|
- L4-S3
- Innervates posterior thigh - Splits into common peroneal and tibial nerves |
|
|
How are nerves and arteries classically named?
|
Nerves are arteries are frequently named together by the bones / regions with which they are associated
There are a few exceptions |
|
|
What are the names of the nerve and artery that supply the axilla / lateral thorax?
|
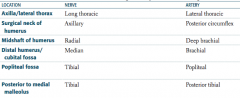
- Long thoracic nerve
- Lateral thoracic artery |
|
|
What are the names of the nerve and artery that supply the surgical neck of the humerus?
|
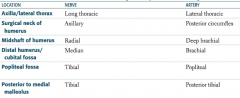
- Axillary nerve
- Posterior circumflex artery |
|
|
What are the names of the nerve and artery that supply the midshaft of the humerus?
|
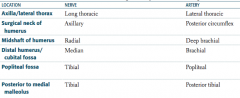
- Radial nerve
- Deep brachial artery |
|
|
What are the names of the nerve and artery that supply the distal humerus / cubital fossa?
|
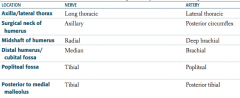
- Median nerve
- Brachial artery |
|
|
What are the names of the nerve and artery that supply the popliteal fossa?
|
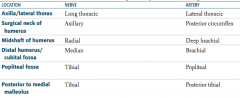
- Tibial nerve
- Popliteal artery |
|
|
What are the names of the nerve and artery that supply the posterior to medial malleolus?
|
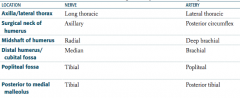
- Tibial nerve
- Posterior tibial artery |
|
|
What are the steps in muscle contraction?
|
1. AP depolarization → opens Ca2+ channels → NT release
2. Muscle cell depolarization in motor end plate 3. Depolarization of T tubules 4. Depolarization of Dihydropyridine receptor → coupled to Ryanodine receptor on SR → Ca2+ release from SR 5. Ca2+ binds Troponin C → Tropomyosin moves from binding groove on actin 6. Myosin releases ADP → power stroke → shortening of H and I bands and between Z lines |
|
|
What is the first step in muscle contraction?
|
Action potential depolarization opens presynaptic voltage-gated Ca2+ channels, inducing NT release
|
|
|
What is the second step in muscle contraction, after NT release?
|
Post-synaptic ligand binding, leads to muscle cell depolarization in the motor end plate
|
|
|
What is the third step in muscle contraction, after depolarization of the motor end plate?
|
Depolarization travels along the muscle cell and down the T tubule
|
|
|
What is the fourth step in muscle contraction, after depolarization of the T tubule?
|
Depolarization of the voltage-sensitive Dihydropyridine Receptor, mechanically coupled to the Ryanodine Receptor on the Sarcoplasmic Reticulum, inducing a conformation change, causing Ca2+ release from SR
|
|
|
What is the fifth step in muscle contraction, after Ca2+ release from SR?
|
Released Ca2+ binds to Troponin C, causing a conformational change that moves Tropomyosin out of the Myosin-Binding groove on Actin filaments
|
|
|
What is the sixth step in muscle contraction, after Ca2+ binds Troponin C?
|
- Myosin releases bound ADP and subsequently, inorganic PO4(3-) → displacement of myosin on the actin filament (power stroke)
- Contraction results in shortening of H and I bands and between Z lines (HIZ shrinkage), but the A band remains the same length (A band is Always the same length) |
|
|
A sarcomere is between what boundaries?
|
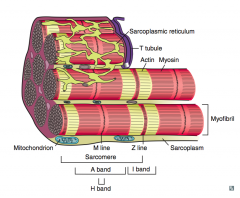
From Z line to Z line
|
|
|
What are the contents of the sarcomere?
|
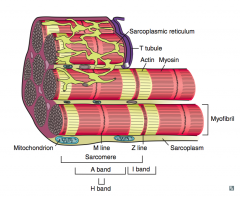
- In the middle: M line
- Surrounding M line: H band - Surrounding H band: A band - Between A bands (two sarcomeres): I band |
|
|
What are the types of muscle fibers?
|
- Type 1: slow / red ("one slow red ox")
- Type 2: fast / white |
|
|
What are the characteristics of Type 1 muscle fibers?
|
- Slow twitch
- Red fibers d/t ↑ mitochondria and myoglobin concentration - ↑ Oxidative phosphorylation → sustained contraction |
|
|
What are the characteristics of Type 2 muscle fibers?
|
- Fast twitch
- White fibers d/t ↓ mitochondria and myoglobin concentration - ↑ Anaerobic glycolysis - Weight training results in hypertrophy of fast-twitch muscle fibers |
|
|
Which muscle fibers are necessary for weight training?
|
Type 2 muscle fibers:
- Fast twitch - White fibers d/t ↓ mitochondria and myoglobin concentration - ↑ Anaerobic glycolysis |
|
|
What are the steps of smooth muscle contraction?
|

1. Action potential
2. Membrane depolarization → opening of L-type voltage gated Ca2+ channels 3. ↑ Ca2+ in smooth muscle cell , binds to Calmodulin 4. Ca2+ Calmodulin complex stimulates Myosin-Light-Chain Kinase (MLCK) 5. MLCK phosphorylates Myosin 6. Phosphorylated myosin + actin → contraction (via cross-bridging) |
|
|
What are the steps of smooth muscle relaxation?
|

1. Nitric Oxide stimulates Guanylate Cyclase
2. GC converts GTP to cGMP 3. cGMP stimulates Myosin Light Chain Phosphatase (MLCP) 4. MLCP removes the phosphate group from Myosin 5. Unphosphorylated myosin + actin → relaxation |
|
|
How are the uses of myosin light chain kinase and phosphatase different?
|

- MLCK used for contraction of smooth muscle by phoshporylating myosin
- MLCP used for relaxation of smooth muscle by removing phosphate from myosin |
|
|
What are the types of bone formation?
|
- Endochondral ossification
- Membranous ossification |
|
|
What bones use endochondral ossification?
|
Bones of axial and appendicular skeleton, and base of skull
|
|
|
What type of bone formation occurs in the axial and appendicular skeleton and the base of the skull? How is it made?
|
Endochondral Ossification:
- Cartilaginous model of bone is first made by chondrocytes - Osteoclasts and osteoblasts later replace with woven bone and then remodel to lamellar bone |
|
|
What bones use membranous ossification?
|
Bones of calvarium and facial bones
|
|
|
What type of bone formation occurs in the calvarium and facial bones? How is it made?
|
Membranous Ossification
- Woven bone formed directly without cartilage - Later remodeled to lamellar bone |
|
|
What kind of bone formation occurs after fractures and in Paget disease?
|
Woven bone formation (endochondral ossification)
|
|
|
What are the cells in the bone?
|
- Osteoblasts
- Osteoclasts |
|
|
What is the function of Osteoblasts? Source?
|
- Build bone by secreting collagen and catalyzing mineralization
- Differentiate from mesenchymal stem cells in periosteum |
|
|
What is the function of Osteoclasts? Source?
|
- Multinucleated cells that dissolve bone by secreting acid and collagenases
- Differentiate from monocytes/macrophages |
|
|
What hormones act on the bone?
|
- Parathyroid Hormone
- Estrogen |
|
|
What is the action of PTH on bones?
|
- At low, intermittent levels, exerts ANABOLIC effects (building bone) on osteoblasts and osteoclasts (indirect)
- Chronic high PTH levels (1° hyperparathyroidism) causes CATABOLIC effects (osteitis fibrosa cystica) |
|
|
What is the action of Estrogen on bones?
|
- Estrogen inhibits apoptosis in bone-forming osteoblasts and induces apoptosis in bone-resorbing osteoclasts
- Under estrogen deficiency (surgical or postmenopausal), excess remodeling cycles and boen resorption leads to osteoporosis |