Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
168 Cards in this Set
- Front
- Back
|
dark bands in skeletal muscle make up what band?
|
A band
dArk |
|
|
light bands in skeletal muscle make up what band?
|
I
Light |
|
|
muscle for the body arise from what embryologic structure?
|
somites
|
|
|
muscle for the head and neck arise from what embryologic structure
|
neural crest
|
|
|
describe prune belly syndrome and what problems are associated
|
Absence of abdominal muscles and severe kidney problems in Prune Belly Syndrome
|
|
|
during development, the dorsal muscles will end up having what action? Anterior?
|
dorsal: extensors
anterior: flexors |
|
|
this nerve : innervates most flexors in the forearm (originating from medial epicondyle), the muscles of the thenar emminence
what is it? |
median nerve
|
|
|
this nerve innervates the first two lumbricals. Needed for strong grip
|
median nerve
|
|
|
this nerve gives Cutaneous innervation covers the anterior palm digits 1, 2, 3,and ½ of 4
what is it |
median nerve
|
|
|
if you see thenar eminence wasting preceeded by tingling, what can you assume is the problem?
|
median nerve damage
|
|
|
innervates two muscles of the anterior compartment of the forearm, the flexor carpi ulnaris, and the ulnar head of the flexor digitorum profundus
what is this |
ulnar nerve
|
|
|
what innervates most of the intrinsic muscles of the hand?
|
ulnar nerve
|
|
|
list the cutaneous innervation given by the ulnar nerve
|
covers the anterior and posterior surfaces of ½ of the 4th digit and all of the 5th
|
|
|
if you cannot flex the elbow, what problem do you have?
|
musculocutaneous nerve
|
|
|
problems with the Cutaneous innervation covers the lateral forearm will be with what nerve
|
Musculocutaneous nerve
|
|
|
what muscles does the axillary nerve innervate?
|
deltoid & teres minor muscles
|
|
|
what nerve is responsible for extending the majority of the arm?
|
radial nerve
|
|
|
olecranon is the insertion for what muscles?
|
triceps
|
|
|
man comes in with shoulder, tricep and anterior arm problems. it is not clear that one nerve causes this. What are you thinking?
|
Erb-Duchenne Palsy
|
|
|
Man falls from a tree causing his head and shoulder to separate to a great degree. He has tricep and shoulder weakness. What do you think he has?
|
Erb-Duchenne Palsy
|
|
|
injury to the inferior part of the brachial plexus is known as what? Where does the injury cause problems
|
Klumpke Paralysis
distal injury (hands) |
|
|
innervates the gluteus medius, gluteus minimus, and tensor fascia lata
name it |
Superior gluteal nerve
|
|
|
man can't go up the stairs or has trouble standing from their chair. What nerve do you think they have problems with? What muscle does this innervate?
|
Inferior gluteal nerve
gluteus maximus |
|
|
what muscles play a role in aBducting the leg and can lead to Trendelenberg sign when not working
what nerve? |
gluteus medius, gluteus minimus
Superior gluteal nerve |
|
|
what innervates Flexors of the hip, and extenders of the knee
|
Femoral nerve
|
|
|
what nerve passes under the inguinal ligament near the ASIS and gives cutaneous innervation to the lateral portion of the thigh. What people complain about this?
|
Lateral cutanous nerve of the thigh
Fat people |
|
|
what innervates the hamstrings? What is the job of these muscles?
|
sciatic nerve
flex the knee |
|
|
what comes of the ischial tuberosity?
|
hamstrings
|
|
|
Plantar flexion and inversion of the ankle are done by what nerve?
|
tibial
|
|
|
you have a palsy of deep fibular nerve, what sign will you have?
|
drop foot
|
|
|
patient falls commonly, especially when on uneven surfaces, what is the problem
|
Superficial fibular nerve
|
|
|
patient has a foot drop and is unable to dorsiflex or evert his foot against resistance. What nerve jumps to mind?
Common fibular Deep fibular Sciatic Superficial fibular Tibial |
Common fibular
|
|
|
near what bony feature might you find a restriction that is responsible for the muscle weakness of the common fibular nerve
|
Fibular Head
|
|
|
what type of metabolism do Type I muscle fibers use?
|
Oxidative metabolism
|
|
|
which fiber is resistant to fatigue?
|
type I (red)
|
|
|
fast twitch fibers are what type of muscle?
|
Type II B (White) Muscle Fibers
|
|
|
which fiber is easily fatigued
|
Type II B (White) Muscle Fibers
|
|
|
Type II B (White) Muscle Fibers uses what type of metabolism?
|
Glycolytic metabolism
|
|
|
decrease tone in stretched (agonist) muscle
increases tone in adversarial muscle what does this describe? |
golgi
|
|
|
what prevents muscles from being over stretched?
|
Muscle spindle fibers
|
|
|
please go through the 6 steps that outline the travel of an upper motor neuron
|
Precentral gyrus
Posterior limb of internal capsule Medullary pyramics Cross at pyramidal decussation (in the lower medulla) Lateral corticospinal tract of spinal cord Ventral grey horn of spinal cord |
|
|
if you see weakness , atrophy, and fasciculations is this upper or lower motor neuron problem?
|
lower
|
|
|
if you see increased reflexes, increaed tone, and weakness, is this an upper or lower motor neuron lesion?
|
upper
|
|
|
if you have decreased (or no) reflex, decreased muscle tone, and atrophy what motor neuron problem is this?
|
lower
|
|
|
how does Tetanospasmin toxin work?
|
initially blocks Ach release but retrograde transport carries it to the spinal cord where it causes intense muscle contraction by inhibiting the normal inhibitory action of spinal interneurons.
|
|
|
please lay out how Ca2+ is released from the SR
|
an AP travels down the T-tubule
hits a DHPR (voltage gated channel) which is coupled with an RyR receptor this activation leads to the release of Ca2+ out of the RyRs from the SR |
|
|
what covers the active site on a muscle fiber?
|
tropomyosin
|
|
|
what band Contains only actin filaments anchored to Z line?
|
I band
|
|
|
what band Contains only myosin filaments anchored to the M line. Also has creatine kinase – catalyzes ATP formation from ADP & phosphocreatine
|
H band
|
|
|
what band Contains myosin and actin filaments sliding across each other
|
A band
|
|
|
what is dystrophin protein?
|
forms a link connecting muscle fibers to extracellular matrix and CT
allows for contraction to lead to movement largest protein |
|
|
Sharpey's fibers do what?
type of collagen? |
attach periosteum into bone
type I |
|
|
Howship’s lacuna are a sign of what? what is it
|
too much osteoclast activity
it is a depression in the bone |
|
|
what does parathyroid hormone do with respect to Ca?
|
activates osteoclasts and increases serum Ca++
|
|
|
what organ is responsible for decreasing osteoclast activity? What does it release to do this?
|
Thyroid c-cells make calcitonin
|
|
|
where is glucocorticoid produced in the body (be specific)
|
zona fasiculata and reticularis of adrenal cortex
|
|
|
Glucocorticoid means to increase serum...
|
glucose levels
|
|
|
Mineralocorticoid means to increase...
|
sodium levels (aldosterone main MC hormone)
|
|
|
what is the mechanism of action for glucocorticoids? 3 main steps
|
induce production of Lipocortin
Lipocortin inhibits the production of Arachidonic acid (via blocking phospholipase A2) this limits the production of prostiglandins AND leukotrienes |
|
|
what do glucocorticoids do to inflammation?
|
reduce it in all forms
|
|
|
is it possible to separate out the anti-inflammatory and glucocorticoid effect of a drug given? what does this mean for high doses?
|
NO
so you can get glucose related side effects (such as steroid based diabetes) |
|
|
Fludrocortisone is used for what?
|
mineralcorticoid therapy (will cause water uptake)
|
|
|
what type of drug is used with Alternate Day Therapy? What does this mean?
|
Glucocorticoids
prevents you from not having a release of ACTH, which would lead to the wasting of the adrenal cortex, thus leading to not being able to produce cortisol (death) |
|
|
if you are treating for weeks and weeks and months with GCs what can be and adverse side effect?
|
Suppression of ACTH with adrenal cortex atrophy
Rate of recovery---weeks, months, years |
|
|
what is one of the most common side effects of glucocorticoids? How does this happen?
******* |
Osteoperosis / Osteopenia
GCs interfere with absorption of Ca from the GI tract |
|
|
Thin skin
Inhibit proliferation of fibroblasts Prevent deposition of collagen Poor wound healing these are side effects of what drug use? |
glucocorticoids
|
|
|
a man is new to your office and says he has been on a drug for a while but doesn't know what. He says that he has experiencing the redistrubition of his fat from the arms and legs and it is showing up on his face and trunk. He says he has some muscle wasting too. What kind of drug was he on?
|
steroid
|
|
|
an X-linked recessive inherited disorder characterized by slowly progressive muscle weakness of the legs and pelvis describes what?
|
Becker's muscular dystrophy
|
|
|
ankylosing spondylitis has a relationship with what disease?
|
inflammatory bowel disease
|
|
|
What injury has an increased risk with osteoporosis ?
*****TEST |
vertebral compression fractures
because the bone quality is not as good |
|
|
iliolumbar ligament attachments
|
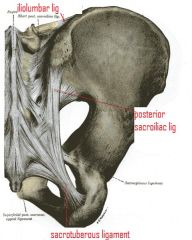
origin-transverse process of L5
attaches to medial aspect of the posterior corner of the iliac crest |
|
|
posterior sacroiliac ligament attachements?
|
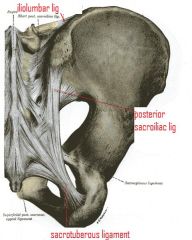
1st, second, and 3rd transverse tubricle of the sacrum
to the posterior superior iliac spine |
|
|
sacrotuberous ligament attachment
|
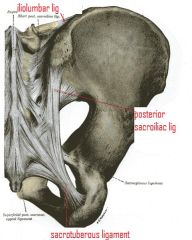
From sacrum
To tuberosity of the ischium |
|
|
gluteus maximus attachments?
|
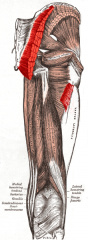
P: Ilium and sacrum, D: Iliotibial tract and gluteal tuberosity
|
|
|
gluteus medius attachment
|

P: Ilium, D: Greater trochanter
|
|
|
gluteus minimus attachment
|

P: Ilium, D: Greater trochanter
|
|
|
this pain is only in the back and/or buttock area without radiation into the legs
|
Axial
|
|
|
this pain is Caused by non-nerve injuries such as muscle, tendon, ligament or disc damage, arthritis or fractures
|
Axial
|
|
|
pain usually in the legs > back, often with leg numbness, tingling or weakness
type of pain? |
Radicular
|
|
|
Caused by nerve irritation/injury such as nerve root impingement by herniated disc or arthritis
type of pain? |
Radicular
|
|
|
pain usually in the back > legs, with normal neurologic exam
type of pain? |
Pseudoradicular
|
|
|
Caused by referred pain from injured non-nerve structures such as muscles, tendons, ligaments or joints
type of pain? |
Pseudoradicular
|
|
|
a patient has pain that is on the iliac crest, and has pain that shoots down the back of the leg. You ask if the pain is found behind the knee, specifically at the joint. The patient says that the pain skips the knee. What kind of back pain is it?
|
pseudoradicular b/c it skips the joint
|
|
|
posterior sacroiliac ligament
please list referred areas of pain |
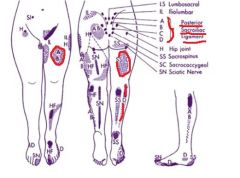
Posterior thigh and calf pain
anterior thigh pain |
|
|
iliolumbar ligament
please list referred areas of pain |
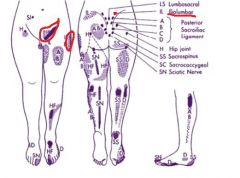
posterior on iliac crest
lateral hip inguinal |
|
|
Significant or worsening weakness in the legs with or without pain
what could this be? Emergency or seek attention? |
severe nerve or spinal cord damage
emergency |
|
|
Acute changes in bowel or bladder function with or without pain
what could this be? Emergency or seek attention? |
conus medullaris syndrome.
emergency |
|
|
Numbness along the insides of both thighs (“saddle anesthesia”)
what could this be? Emergency or seek attention? |
cauda equina syndrome.
emergency |
|
|
Acute back pain with fever, chills, and/or night sweats
what could this be? Emergency or seek attention? |
infection of the spine.
emergency |
|
|
Acute back pain with a tearing sensation and bounding pulse in the stomach area
what could this be? Emergency or seek attention? |
dissecting or ruptured aortic aneurysm
emergency |
|
|
a patient with pain with a structural origin (e.g. arthritis, myofascial, ligamentous or tendinous dysfunction) and/or functional deficits (e.g. decreased strength, flexibility, activity tolerance, work capacity) should see what type of physician
|
Musculoskeletal physiatrist
|
|
|
if a patient has well-localized pain generators without profound neurologic deficits (e.g. painful radiculopathy, facet arthropathy, discogenic pain), unresponsive to other conservative treatments such as physical therapy, OMT, or medications what type of physician should they see?
|
Interventional pain specialist (spinal injections under fluoroscopic guidance)
|
|
|
patient has Localized pain with/without pain in other joint areas, particularly the hands, and associated findings such as rash (e.g. lupus, psoriatic arthritis, dermatomyositis) or lab abnormalities (e.g. elevated ESR, ANA or rheumatoid factor).
who should they see ? |
Rheumatologist
|
|
|
patient has peripheral neurologic deficits without an identifiable structural cause (low motor neuron lesions, e.g. peripheral neuropathy, ALS), or central nervous system deficits (upper motor neuron lesions, e.g. multiple slerosis, stroke, ALS
who should they see |
Neurologist
|
|
|
person has profound and/or emergent neurologic deficits from structural causes (e.g. large disc herniation causing severe radiculopathy, spondylosis causing severe spinal stenosis), unresponsive to other treatments such as medications or spinal injections
who should they see? |
Neurosurgeon
|
|
|
good for bones (e.g. fractures, arthritis, alignment and dynamic stability with flexion/extension views).
what diagnostic test? |
Plain radiograph (X-ray)
|
|
|
excellent for bones, discs, joints, nerves, soft tissue.
what diagnostic test? |
MRI (magnetic resonance imaging):
|
|
|
excellent for bony anatomy (e.g. complex fractures, arthritis, alignment)
what diagnostic test? |
CT (computed tomography):
|
|
|
pt comes in with history of prostate cancer and some back pain. Should he use an MRI or Nuclear Bone Scan?
|
Nuclear Bone Scan
|
|
|
excellent for vascular problems (aneurysms, aortic dissection, and arterial stenosis
what diagnostic test? |
Angiogram
|
|
|
spondylosis
spondylolysis spondylolisthesis NEED TO KNOW**** |
spondylosis:arthritis of the spine
spondylolysis: fracture at the pars spondylolisthesis: decapitation of the pars, entire lumbar segment slides forward |
|
|
a patient is having problems with sensation of their inner thigh closet to the pubic bone, what spinal root is this most likely due to?
|

L1
|
|
|
a patient is having sensation problems starting from the outer hip down the middle of the thigh, extending down the shin to the medial ankle. What is the problem?
|

problem with L4 spinal root
|
|
|
patient is having problems with sensation on the top of their foot including their big toe.. what is the problem?
|

L5 spinal root
|
|
|
patient is a gymnast who has pain worse with flexion or extension. You see a step-off sign at spinous process, paraspinal spasm, and foraminal narrowing causing rediculopathy. What does this patient have?
|
spondylolistheis
|
|
|
patient has a radiograph with"Scottie dog" neck broken. What does this patient have?
|
spondylolistheis
|
|
|
pt has achieness in muscles, pain in the hip and shoulder girdle, CPK is elevated. Patient is on medicine for high cholesterol. What do they likely have?
|
statin-induced myopathy
|
|
|
electrodiagnostic studies can give what kind of information
**** |
Diagnostic AND prognostic
|
|
|
what are the 2 parts of an EMG?
**** |
nerve conduction study
Needle EMG (motor unit potentials |
|
|
how do you look to study a brachial nerve plexopathy? (what nerves do you test)
**** |
medial and lateral antibrachial cutaneous nerves are tested
|
|
|
patient has Weakness or numbness that does not follow a single radicular or peripheral nerve distribution , what should you order?
|
EMG
|
|
|
patient has Unexplained numbness or weakness what should you order?
|
EMG
|
|
|
what should you order if you see a patient with history of leg pain and physical exam positive for numbness and weakness who has a lumbar MRI that is negative for nerve root impingment
|
EMG
|
|
|
what should you order if you see a patient with a history of neck pain and radiation therapy for breast cancer who has numbness along multiple dermatomes and also has a positive Tinel sign at the wrist – differential diagnosis includes cervical radiculopathy, brachial plexopathy, median neuropathy at the wrist
|
EMG
|
|
|
if a patient has a nerve injury, how long do you have to wait to test with an EMG?
**** |
3 weeks
|
|
|
a prognostic test for certain conditions, such as carpal tunnel syndrome, to determine the need for surgical intervention describes?
**** |
EMG
|
|
|
if you have an abnormal EMG and A non-focal peripheral neuropathy or myopathy, what should you do?
|
send to a neuromuscular specialist
|
|
|
if your EMG Is abnormal and you have a focal area of nerve injury what should be the next 2 things you do?
|
imaging studies may need to be ordered to confirm the diagnosis
referral for treatment (e.g. interventional spine specialist for spinal nerve root block or neurosurgeon for surgical decompression) is required |
|
|
if you EMG is normal, but the physical exam is abnormal, what should you evaluate? using what?
|
the central nervous system (e.g. stroke, spinal cord injury, brain or spinal cord tumor, spinal stenosis) via MRI or referral to Neurology.
|
|
|
patient has nerve traction or compression from lateral fall on head, obstectrical injury, sports-related ("stinger") what does this person have?
|
Erb's Palsy: C5-C6 nerve roots or upper trunk gets stretched
|
|
|
patient presents with an arm that becomes adducted, internally rotated, extended, pronated, with the wrist flexed. What do they have? What is this clinical presentation called?
|
Erb’s palsy: C5–C6 nerve roots or upper trunk
Waiter's tip position |
|
|
obstetrical traction injury causes?
|
Klumpke palsy: C8–T1 nerve roots or lower trunk
|
|
|
The patient may have wasting of the small hand muscles and a claw hand deformity (lumbrical weakness). The shoulder girdle muscle function is preserved.
What do they have? |
Klumpke palsy: C8–T1 nerve roots or lower trunk
|
|
|
what leads to claw hand deformity in Klumpke palsy
|
get extension at MCP and then get passive flexion at DIP and PIP
|
|
|
a secondary plexopathy can arise from these tumors and their treatment...
**** |
Lung/breast tumor
|
|
|
what are the muscles controlled by the median nerve?
|
1/2 LOAF
Lumbricals (1,2) Opponens pollicis Abductor pollicis brevis Flexor pollicis brevis (superficial head |
|
|
is there a motor or sensory loss in Superficial radial neuropathy
|
ONLY SENSORY
|
|
|
this affects all ulnar-innervated sensation and muscles except the flexor carpi ulnaris...
|
Cubital Tunnel Syndrome
|
|
|
What causes cubital tunnel syndrome? where does it normally occur
|
entrapment of ulnar nerve
compression of the elbow |
|
|
please list the muscles controlled by the deep motor branch of the ulnar nerve
|
“4,3,2,1,1/2 muscles”
Palmaris brevis 4 Dorsal interossei—(“DAB”: Abduction) 3 Palmar interossei—(“PAD”: Adduction) 2 Lumbricals 1 Adductor pollicis 1/2 Flexor pollicis brevis (deep head) |
|
|
Affects all ulnar-innervated intrinsic muscles of the hand, but dorsal ulnar cutaneous nerve (DUC) nerve is spared.
|
Guyon’s canal (a.k.a. Cycler’s or Biker’s palsy)
|
|
|
Due to cycling activities, wrist ganglions or rheumatoid arthritis. What is this? What is affected and what nerve is spared?
|
Guyon’s canal (a.k.a. Cycler’s or Biker’s palsy)
Affects all ulnar-innervated intrinsic muscles of the hand, but dorsal ulnar cutaneous nerve (DUC) is spared. |
|
|
Due to compression at the wrist from a wristwatch, tight handcuffs, etc.
Pure sensory syndrome with paresthesias on dorsal radial aspect of the hand. |
Superficial radial neuropathy (a.k.a. Cheiralgia Paraesthetica, Wristwatch syndrome, Handcuff palsy)
|
|
|
Superficial radial neuropathy (a.k.a. Cheiralgia Paraesthetica, Wristwatch syndrome, Handcuff palsy)
|
Due to compression at the wrist from a wristwatch, tight handcuffs, etc.
Pure sensory syndrome with paresthesias on dorsal radial aspect of the hand. |
|
|
patient has been on crutches and now has problems with triceps and lost sensation over the posterior arm and forearm. What do they have?
|
crutch palsy involving the radial nerve
|
|
|
patient has been on crutches and now has problems with shoulder flexion and abduction, and external rotation. What is going on?
|
axillary neruopathy due to crutch use
|
|
|
in a fulminant case of gas gangrene caused by clostridium perferinges, what would be the most important treatment?
*********TEST |
Debride the wound of infection
|
|
|
most common cause of septic arthritis in the adult population?
*********TEST |
Staph Aureus
|
|
|
T/F multiple joint involvement is a typical clinical feature of septic arthritis
*********TEST |
FALSE
only one joint normally |
|
|
Osteomyelitis caused by hematogenous spread is most likely found i what age group and what type of bones?
*********TEST |
Teenagers
Long bones/vertebrae |
|
|
True or False:
In An implanted prosthesis the cementing substance appears to be predisposed toward infection with staphylococcus epidermidis. The mechanism is due to a "slime" substance *********TEST |
TRUE
|
|
|
Themost common cause of septic arthritis in children under 5 is?
*********TEST |
Haemophilius influenzae
|
|
|
in which of the following disease is staph aureus NOT the most common etiologic agent?
a) infection in an implanted prosthesis b)osteomyelitis due to hematogenous spread c)pyomositis d)psoas abscess in young children e)septic arthritis in adults *********TEST |
a) infection in an implanted prostheses
|
|
|
after a bowel surgery a patient develops a severe muscle infection of the buttocks. The wound has a particular foul odor with crepitus present in the surrounding tissue. A smear of the seropurulent exudate reveals Gram-Positive cocci in chains and many pleomorphic rods. The likely clinical disease is?
a)pyomyositis b)clostridial myonecrosis (clostridial gangrene) c)synergistc nonclostidial anarobic myonecrosis *********TEST *********TEST |
c)synergistic nonclostridial anarobic myonecrosis
|
|
|
T/F: toxin production by clostridium perfringens requires a high (+) oxidation reduction potential
*********TEST |
FALSE
|
|
|
T/F: often in the course of systemic infections muscle involvement takes the form of myalgia, weakness, and wasting. This appears to be due to an "acute phase" host response inititiated by IL-1 which ultimately leads to accelerated catabolism of skeletal muscle
|
TRUE
|
|
|
Bone infections occur most frequently at what part of long bone?
*********TEST |
Metaphysis
|
|
|
48 hours after a compound fracture of the femur a patient develops a severe infection in the surrounding muscle tissue. The wound has a particular foul odor with crepitus present. A smear of the dark fluid reveals large Gram-positive rods. What is this likely
*********TEST |
CLOSTRIDIUM GANGRENE
(gram positive RODS) |
|
|
T/F growth of anaerobes requires a low oxidation potential and reduced O2 tension
*********TEST |
TRUE
|
|
|
T/F postinfectious arthritis that develops in persons after Shigella, Salmonella, Campylobacter, and Yersinia gastritis frequently have the histocompatibility antigen HLA B27
*********TEST |
TRUE
|
|
|
A 20 y/o football player suffers a sprain of the MCL. On exam he has tenderness over the ligament and pain with valgus stress but no joint laxity is apparent. You would classify this sprain as...
*********TEST |
Grade I
|
|
|
after performing the preparticipation physical exam you detect that the pt has Hypertrophic Cardiomyopathy. When discussing this diagnosis with the pt, you tell them...
a) it is a benign condition and it will not limit his participation b)this condition could result in sudden cardiac death c)he can continue to participate as long as he is asymptomatic d)he will eventually outgrow the condition *********TEST |
b) this condition could result in sudden cardiac death
|
|

|
Bone scan
|
|
|
|
he can expect longer recovery
|
|
|
|
Patellofemoral syndrome
|
|
|
|
It is the most effective PPE
|
|

|
Osgodd-Schlatter
|
|

|
MCL
|
|
|
|
Complete Rest
|
|

|
Anterior talofibular
(if you said ligament of treitz, please pack up your things and go home) |
|
|
|
Avoid activities that cause lumbar hyperextension (that is what caused it!)
|
|

|
Continued participation is gonna F up that knee
|
|
|
|
progressive activity will result in improved activity tolerance
|
|
|
|
decrease inflammatory response
|
|

|
Grade II sponylolisthesis
|
|
|
if you see negative birefringent what do you think?
|
GOUT
|
|
|
if you see positive birefringent what are you thinking
|
pseudogout
|
|
|
what does desmin do?
how bout dystrophin? |
anchors nearby muscle fibers to each other
anchors muscle fiber bundles to CT |