Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
41 Cards in this Set
- Front
- Back
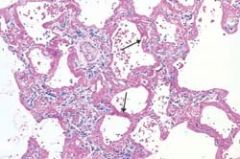
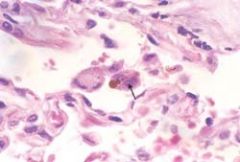
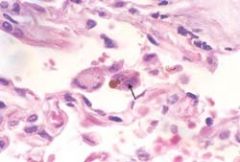
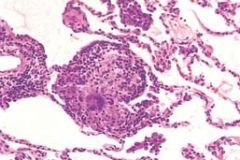
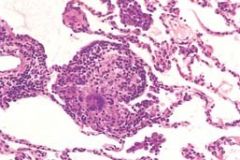
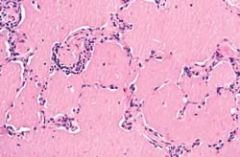
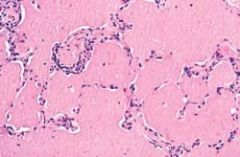
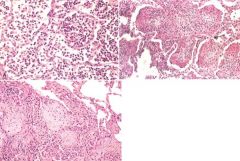
What disease process is occuring here
|
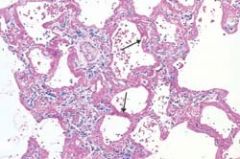
Diffuse alveolar damage (acute respiratory distress syndrome) shown in a photomicrograph. Some of the alveoli are collapsed; others are distended. Many contain dense proteinaceous debris, desquamated cells, and hyaline membranes (arrows).
|
|
|
What are the three types of Atelectasis
|
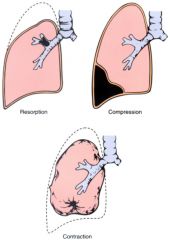
Resorption (obstruction)
Compression Contraction |
|

What disease processes are shown here
|

A, Centriacinar emphysema. Central areas show marked emphysematous damage (E), surrounded by relatively spared alveolar spaces. B, Panacinar emphysema involving the entire pulmonary architecture
|
|
|
What are the two main types of Emphysema
|
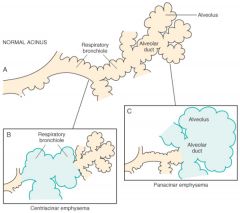
Centriacinar and Panacinar
|
|

What disease is demonstrated here
|

Bullous emphysema with large subpleural bullae (upper left).
|
|
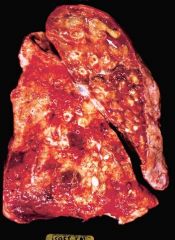
What is shown here
|
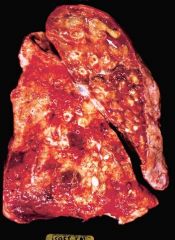
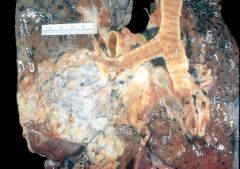
Bronchiectasis in a patient with cystic fibrosis, who underwent lung transplantation. Cut surface of lung shows markedly distended peripheral bronchi filled with mucopurulent secretions.
|
|
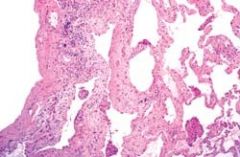
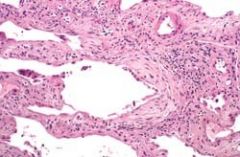
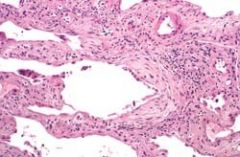
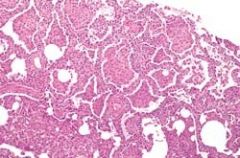
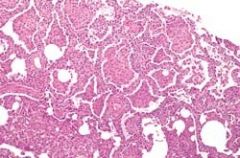
What is shown here
|
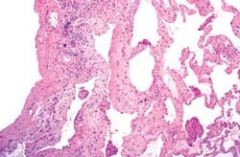
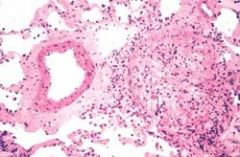
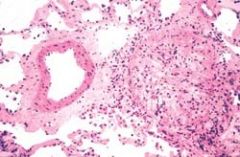
Usual interstitial pneumonia. The fibrosis, which varies in intensity, is more pronounced in the subpleural region
|
|
What is shown here
|
Usual interstitial pneumonia. Fibroblastic focus with fibers running parallel to surface and bluish myxoid extracellular matrix
|
|
What is shown here
|
Cryptogenic organizing pneumonia (COP). Alveolar spaces are filled with balls of fibroblasts (Masson bodies), while the alveolar walls are relatively normal
|
|
What is shown here
|
Progressive massive fibrosis superimposed on coal workers' pneumoconiosis. The large, blackened scars are located principally in the upper lobe. Note the extensions of scars into surrounding parenchyma and retraction of adjacent pleura
|
|

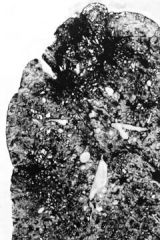
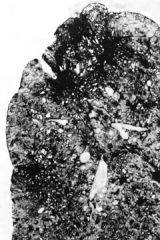
What is shown here
|

Advanced silicosis seen on transection of lung. Scarring has contracted the upper lobe into a small dark mass (arrow). Note the dense pleural thickening
|
|
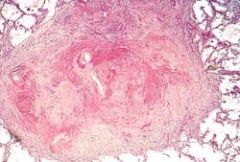
What is shown here
|
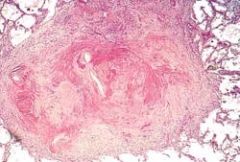
Several coalescent collagenous silicotic nodules.
|
|
What is shown here
|
High-power detail of an asbestos body, revealing the typical beading and knobbed ends (arrow).
|
|

What is shown here
|

Asbestos exposure evidenced by severe, discrete, characteristic fibrocalcific plaques on the pleural surface of the diaphragm.
|
|
What is shown here
|
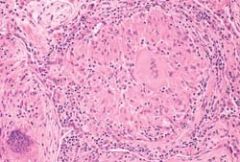
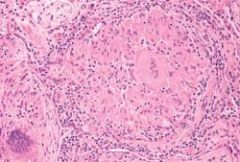
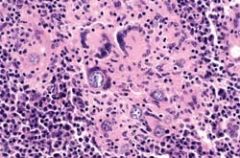
Characteristic sarcoid noncaseating granulomas in lung with many giant cells.
|
|
What is shown here
|
Hypersensitivity pneumonitis, histologic appearance. Loosely formed interstitial granulomas and chronic inflammation are characteristic
|
|
What is shown here
|
Desquamative interstitial pneumonia: medium-power detail of lung to demonstrate the accumulation of large numbers of mononuclear cells within the alveolar spaces with only mild fibrous thickening of the alveolar walls.
|
|
What is shown here
|
Pulmonary alveolar proteinosis, histologic appearance. The alveoli are filled with a dense, amorphous, protein-lipid granular precipitate, while the alveolar walls are normal.
|
|

What is shown here
|

Large saddle embolus from the femoral vein lying astride the main left and right pulmonary arteries.
|
|

What is shown here
|

Recent, small, roughly wedge-shaped hemorrhagic pulmonary infarct.
|
|
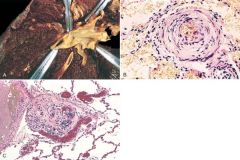
What do these pictures demonstrate
|
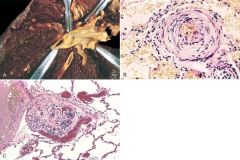
Vascular changes in pulmonary hypertension. A, Gross photograph of atheroma formation, a finding usually limited to large vessels. B, Marked medial hypertrophy. C, Plexogenic lesion characteristic of advanced pulmonary hypertension seen in small arteries
|
|
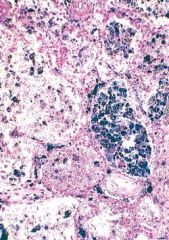
What does this picture demonstrate
|
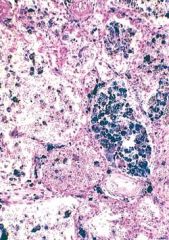
Acute intra-alveolar hemorrhage and hemosiderin-laden macrophages, reflecting previous hemorrhage, are common features of the diffuse pulmonary hemorrhage syndromes (Prussian blue stain for iron).
|
|
|
Compare Bronchopneumonia with Lobar Pneumonia
|
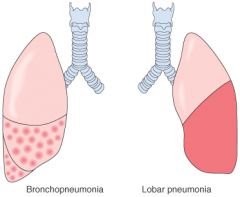
Patchy consolidation of the lung is the dominant characteristic of bronchopneumonia
Lobar pneumonia is an acute bacterial infection resulting in fibrinosuppruative consolidation of a large portion of a lobe or of an entire lobe |
|

What does this picture demonstrate
|

Bronchopneumonia. Gross section of lung showing patches of consolidation (arrows).
|
|

What does this picture demonstrate
|

Lobar pneumonia—gray hepatization, gross photograph. The lower lobe is uniformly consolidated
|
|
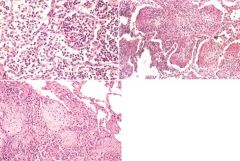
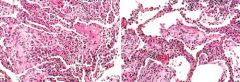
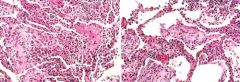
What do these pictures demonstrate
|
A, Acute pneumonia. The congested septal capillaries and extensive neutrophil exudation into alveoli corresponds to early red hepatization. Fibrin nets have not yet formed. B, Early organization of intra-alveolar exudate, seen in areas to be streaming through the pores of Kohn (arrow). C, Advanced organizing pneumonia (corresponding to gray hepatization), featuring transformation of exudates to fibromyxoid masses richly infiltrated by macrophages and fibroblasts.
|
|
What does this picture demonstrate
|
Pyemic lung abscess in the center of section with complete destruction of underlying parenchyma within the focus of involvement.
|
|

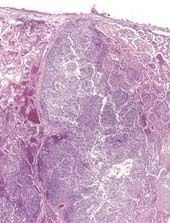
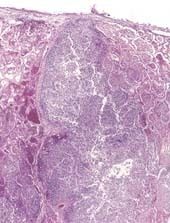
What does this picture demonstrate
|

Laminated Histoplasma granuloma of the lung
|
|
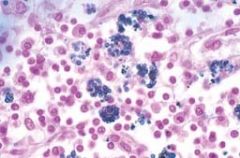
What does this picture demonstrate
|
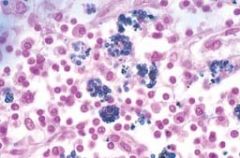
Histoplasma capsulatum yeast forms fill phagocytes in a lymph node of a patient with disseminated histoplasmosis
|
|
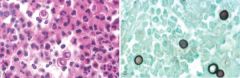
What do these pictures demonstrate
|
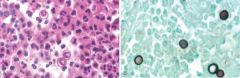
Blastomycosis. A, Rounded budding yeasts, larger than neutrophils, are present. Note the characteristic thick wall and nuclei (not seen in other fungi). B, Silver stain.
|
|
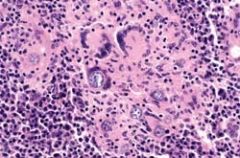
What does this picture demonstrate
|
Coccidioidomycosis with intact spherules within multinucleated giant cells
|
|
What does this picture demonstrate
|
Chronic rejection of lung allograft, with total occlusion of bronchiole (bronchiolitis obliterans). Adjacent pulmonary artery branch is normal
|
|

What does this picture demonstrate
|
Lung carcinoma. The gray-white tumor tissue is seen infiltrating the lung substance. Histologically, this large tumor mass was identified as a squamous cell carcinoma.
|
|

What do these pictures demonstrate
|

Cytologic diagnosis of lung cancer is often possible. A, A sputum specimen shows an orange-staining, keratinized squamous carcinoma cell with a prominent hyperchromatic nucleus (arrow). B, A fine-needle aspirate of an enlarged lymph node shows clusters of tumor cells from a small cell carcinoma, with molding and nuclear atypia characteristic of this tumor; note the size of the tumor cells compared with normal polymorphonuclear leukocytes in the left lower corner
|
|
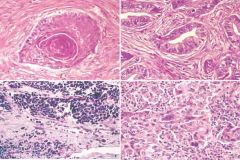
What do these pictures demonstrate
|
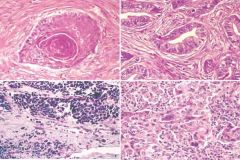
Histologic appearance of lung carcinoma. A, Well-differentiated squamous cell carcinoma showing keratinization. B, Gland-forming adenocarcinoma. C, Small cell carcinoma with islands of small deeply basophilic cells and areas of necrosis. D, Large cell carcinoma, featuring pleomorphic, anaplastic tumor cells and absence of squamous or glandular differentiation.
|
|
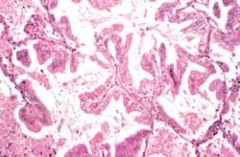
What does this picture demonstrate
|
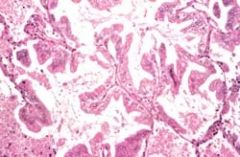
Bronchioloalveolar carcinoma with characteristic growth along pre-existing alveolar septa, without invasion
|
|
What do these pictures demonstrate
|
A, Bronchial carcinoid growing as a spherical, pale mass (arrow) protruding into the lumen of the bronchus. B, Histologic appearance of bronchial carcinoid, demonstrating small, rounded, uniform cells
|
|

What is shown here
|

Numerous metastases from a renal cell carcinoma.
|
|

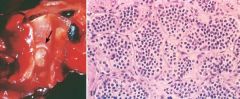
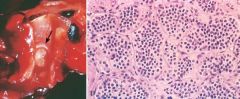
What is shown here
|

Malignant mesothelioma. Note the thick, firm, white pleural tumor tissue that ensheathes this bisected lung
|
|
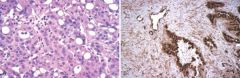
What is shown here
|
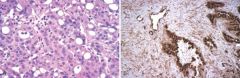
A, Malignant mesothelioma, epithelial type. B, Malignant mesothelioma, mixed type, stained for calretinin (immunoper-oxidase method). The epithelial component is strongly positive (dark brown), while the sarcomatoid component is less so.
|
|
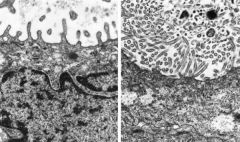
What do these EMs show
|
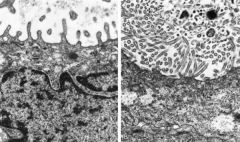
Ultrastructural features of pulmonary adenocarcinoma (A), characterized by short, plump microvilli, contrasted with those of mesothelioma (B), in which microvilli are numerous, long, and slender.
|