![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
48 Cards in this Set
- Front
- Back
|
Define drug addiction |
A behavioural pattern of drug use, characterized by overwhelming involvement with the use of a drug, the securing of its supply, and a high tendency to relapse after withdrawal |
|
|
Define substance dependence |
Disorder involving excessive and harmful drug use by an individual |
|
|
Explain the gateway theory of drug use |
Proposes the existence of developmental stages of drug use in adolescence who progress from one substance to another over time |
|
|
Describe the physical dependence model of addiction |
Once physically dependent, attempts at abstinence lead to highly unpleasant withdrawal symptoms, thus motivating the user to take the drug again to alleviate the symptoms. (common with alcohol & opiates) |
|
|
Discuss the neural mechanism of reward |
The reward-circuit: involves the DA pathway from the VTA to the nucleus accumbens (mesolimbic DA pathway). Activation of the pathway (i.e. from drugs) causes DA levels in the Nuc. Acc. to rise. |
|
|
The VTA is home to what two pathways? (VTA= Ventral Tegmental Area) |
Mesolimbic Pathway (extending from the VTA to the nucleus accumbens Mesocortical Pathway (extending from the VTA to the cerebral cortex) VTA is home to a large amount of DA neurons |
|
|
The anti-reward system |
Activated during drug withdrawal. Negative reinforcement produced by alleviating aversive withdrawal symptoms with drug use |
|
|
Incentive-sensitization model |
In drug addiction, the user "wants" the drug more, even though he doesn't "like" the drug more. Thought to occur because repeated drug use causes sensitization to the "wanting" system, but not like "liking" system. |
|
|
Opponent-process model |
The initial positive response to a drug is followed by an opposing withdrawal response as the drug wears off |
|
|
Describe the disease model of addiction |
Most widely accepted model Based largely on the dysregulation of brain function in addiction Has helped society have more remorse+understanding rather than blame. a.k.a. The Medical Model |
|
|
Explain how comorbidity and self-medication are relevant to compulsive substance use |
The presence of some other diagnosis (i.e. mood, anxiety, or personality disorder) can cause a person to develop a substance abuse issue by attempting to self-medicate |
|
|
Describe the process of alcohol metabolism |
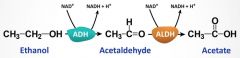
In the liver, alcohol dehydrogenase (ADH) converts alcohol to acetaldehyde, which is then rapidly converted to acetic acid by acetaldehyde dehydrogenase (ALDH) |
|
|
What are DTs? |
Delirium Tremens Severe withdrawal effects. Irritability, headaches, confusion, agitation, convulsions, total disorientation, hallucinations, delirium. Small % of alcoholics withdrawing will experience DTs |
|
|
Discuss the neurotoxic effects of heavy alcohol consumption |
Produces a serious deficiency in Vitamin B1 (thiamine) causing cell death. Can lead to Wernicke-Korsakoff syndrome. Enlarged ventricles due to shrinkage of brain tissue. Too much acetaldehyde can cause brain damage. |
|
|
Describe the effects of alcohol in other body organs systems |
Cardiovascular: B.P. up, stroke, inflammation, enlarged heart Renal: reduced secretion of antidiuretic hormone = more fluid loss thru urine Reproductive: Impotence, testicular atrophy, reduced ovarian function, increase menstrual disorders GI: Stomach irritation, inflammation, diarrhea, reduced absorption of vits and minerals Liver: Fatty liver, alcoholic hepatitis, cirrhosis |
|
|
How does alcohol affect glutamate? |
Acutely inhibits glutamate transmission by reducing the effectiveness of glutamate at the NMDA receptor. Alcohol = glutamate antagonist |
|
|
Discuss the major psychological factors associated with alcoholism |
Alcoholism can be a result of attempting to deal with stress. Alcohol abuse and anxiety are related. Family history is a risk factor. Novelty seeking may also play a role. |
|
|
What are the 2 major pharmacotherapeutic approaches in treating alcoholism? |
1) Making alcohol ingestion unpleasant 2) Reducing its reinforcing qualities |
|
|
Describe the drugs used in alcohol treatment |
Disulfram (a.k.a. Antabuse) - inhibits ALDH. Makes the person feel very sick. Naltrexone - gamma receptor antagonist Nalmefene - opioid receptor antagonist Acamprostate - partial antagonist at the glutamate NMDA receptor, blocks glutamate release that occurs during alcohol withdrawal |
|
|
What are narcotic analgesics? Describe their source. |
Opioid medications used to treat pain. Source = opium, from the poppy plant |
|
|
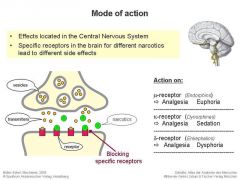
Mechanism of Actions - Opioids |
|
|
|
Major types of opioid receptors? Describe their function |
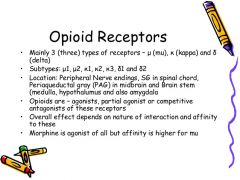
Mu Kappa Delta |
|
|
Opioid receptors continued.. |
Mu: brain and spinal cord. Morphine induced analgesia, feeding, positive reinforcement
Kappa: striatum, amygdala, hypothalamus & pituitary. Pain perception, gut motility, dysphoria, water balance, feeding, temperature control. Delta: forbrain (neocortex, striatium, olfactory, NAcc). Modulating olfaction, motor integration, reinforcement, cognitive function. NOP-R: CNS and PNS. Cerebral cortex, limbic areas, thalamus, brain stem, spinal cord. Analgesia, feeding, motor function. |
|
|
How do opioids reduce synaptic transmission? |
1) Postsynaptic inhibition 2) Axoaxonic inhibition 3) Presynaptic autoreceptors |
|
|
Polarized = Depolarized = |
Polarized = more negative on the inside of the neuron than the outside Depolarized = the positive ions flow into the neuron, making it more positive |
|
|
Describe the pathways of early pain |
Early pain is transmitted from the spinal cord via the spinothalamic tract to the posteroventrolateral (PVL) of the thalamus before going directly to the primary and then secondary somatosensory cortex. |
|
|
How do opioids regulate pain? |
Opioids bind to receptors to mimic the inhibitory action of the endogenous opioids at many stages of pain transmission.
1) Within the spinal cord by small inhibitory interneurons 2) By 2 significant descending pathways 3) At higher brain sites explaining why opioids effect emotional and hormonal aspects of pain response |
|
|
Explain dopamine's role in opioid reinforcement |
When opioids enter the VTA, dopamine firing increases which subsequently increases the release of DA in the NAcc) |
|
|
Major consequences of long-term opiate use? |
Tolerance (reduced effect of the drug leading to using a higher dose) Cross-tolerance (reduced effectiveness of chemically similar drugs) Sensitization (increase in feelings of cravings) Physical dependence (shown with withdrawal symptoms) |
|
|
What is the significance of methadone maintenance? |
The program provides a daily, supervised, oral dose of methadone so opioid addicts can focus their efforts and energy on positive activities like employment. -methadone offers a long-lasting, stable drug effect -orally, it doesn't produce a high or rush -reduced HIV, criminality, mortality, and support self-supporting lifestyles |
|
|
What is cocaine? |
An alkaloid derived from the leaves of the coca plant. It is then converted to hyrdochloride salt and is crystallized. |
|
|
What is crack? |
It is made by dissolving hydrochloride (HCl) cocaine, drying it, and adding substances to it to make it smokable. |
|
|
Cocaine's mechanism of action |
Binds to the transporters of DA, Serotonin, and NE - blocking the re-uptake of these neurotransmitters. This increases synaptic concentrations of each transmitte, therefore enhancing monoamine transmission through the neurons |
|
|
Briefly discuss dopamine's role in the behavioral effects of psychostimulant drugs |
Inhibition of DA reuptake causes an increase in synaptic DA levels. |
|
|
Explain what sensitization is and describe it's phases |
Chronic exposure leading to increased responsiveness to the psychostimulant. (characterized by increased DA release) 2 phases: 1) induction: process by which sensitization response if manifested 2) expression: process by which the sensitized response if manifested |
|
|
How can pharmacotherapy be used in treating cocaine dependence? |
Various drugs that MAY be beneficial act on DA, 5-hT, glutamate, & GABA systems. The 2 most popular are: Modafinil - narcolepsy/sleep apnea, various effects on the DA, NE, Glut & GABA sytems Disulfiram - "antabuse" dopamine beta-hydroxylase (DBH) inhibition = main mechanism |
|
|
What is amphetamine? How is it used therapeutically? |
Parent compound of a family of synthetic psychostimulants. Resembles Dopamine. Can be used to treat ADHD, narcolepsy, very rare cases of obesity. Has a high abuse potential, therefore not a common therapeutic drug. |
|
|
Describe the behavioural effects that amphetamine can have on users |
Heightened alertness Confidence Feelings of exhilaration Reduced fatigue Improved performance on some tasks Delay in sleep onset |
|
|
What is MDMA? How can it affect brain pathways? |
3,4-methylenedioxymethamphetamine Stimulates the release of 5-HT It can reduce the amount of 5-HT fibres in the brain by long-lasting depletion of 5-HT (a.k.a. serotonergic toxicity) |
|
|
What is nicotine? How does it work? |
An alkaloid found in tobacco leaves. Works by activating nicotinic cholinergic receptors. (nAChRs) |
|
|
Describe the effects of nicotine at high doses |
Nicotine poisoning Nausea, excessive salivation, abdominal pain, vomiting, diarrhea, cold sweat, headache, disturbed hearing and vision, mental confusion, weakness. |
|
|
Describe the abstinence syndrome associated with nicotine |
Happens when there is a drop/removal of nicotine from the bloodstream. Cravings, irritability, impatience restlessness, anxiety, insomnia, difficulty concentrating, hunger + weight gain. Most side effects finally subsided to baseline at around 4 weeks. |
|
|
Discuss 2 kinds of nicotine replacement therapy |
Gum: Advtanges - easy, flexible dosing, OTC, rapid nicotine delivery, mouth absorption Disadvantages - frequent dosing, side effects (i.e. mouth/jaw soreness) Patch: Advantages - easy, OTC, no morning cravings, few side effects Disadvantages - less flexible dosing, slower delivery, overnight use = possible insomnia |
|
|
What is caffeine? |
The principle psychoactive ingredient in coffee and tea |
|
|
What are the main behavioural/psychological effects of caffeine? |
Stimulation, fatigue reducing, feelings of well-being, increased alertness, increase confidence and motivation, increase performance, increased blood pressure and respiration, diuresis, stimulation of catecholamine release. |
|
|
Caffeine's mechanism of action |
Blocks A1 and A2a adenosine receptors Higher adenosine levels = wakefulness and alertness (Does NOT influence catecholamine systems) |
|
|
Describe the pattern of tolerance with chronic caffeine users |
Tolerance can develop to some of caffeine's effects. I.e. a chronic caffeine user may be able to drink coffee before bed without any disruption of sleep. They also might not experience the cardiovascular effects. |
|
|
What is caffeinism? |
Chronic ingestion of excessive amounts of caffeine (typically 1000mg+ per day). Restlessness, insomnia, tachycardia, GI upset. |