Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
20 Cards in this Set
- Front
- Back
|
What are the clinical diagnostic dcriteria for a diagnosis of ARDS?
|
This will be a test question:
4 of them: -Acute (6 hrs - 3 days0 -Diffuse bilateral infiltrates on CXR -Hypoxic: PaO2/FiO2 < 200 -Non-cardiogenic: PCWP<18 |
|
|
What are common causes of direct lung injury that can lead to ARDS?
|
Pneumonia (any cause)
Aspiration of gastric contents Uncommon: Pulmonary confusion Fat embolism Amniotic fluid embolism Near-drowning Inhalational injury Reperfusion injury post-transplant |
|
|
What are common causes of indirect lung injury that can lead to ARDS?
|
Common causes:
SEPSIS! Severe trauma with shock Acute pancreatitis Uncommon: Multiple transfusions Drug overdose Diffuse intravascular coagulation |
|
|
What other pulmonary conditions can present acutely with bilateral infiltrates and hypoxemia?
|
CHF
Pneumonia Alveolar hemorrhage Aspiration |
|
|
What is the pathogenesis of ARDS?
|
1. Acute insult to the lungs
2. Invasion of inflammatory cells 3. Damage of the alveolar surface (epithelium, type 1 cells) 4. Inactivation of surfactant --> increased surface tension 5. LEAKAGE OF PROTEIN-RICH FLUID INTO THE ALVEOLI 6. Matrix formed on surface of alveoli of fibrin: "Hyaline membrane" |
|
|
What does ARDS look like on CT?
|
Heterogenous white infiltrates on CT
|
|
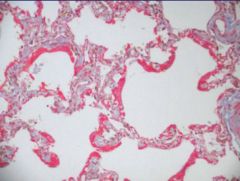
What features of ARDS are present on this slide?
|
Thickened alveoli
Hyaline deposits |
|
|
What are the phases of ARDS?
|
Exudative
Proliferative Fibrotic All are a week apart |
|
|
What processes occur during the exudative phase of ARDS?
|
1. Damage to capillary membranes--> alveolar flooding
2. Oxygenation falls 3. Decreased compliance of lungs All of this leads to bilateral infiltrates on CXR |
|
|
What processes occur during the proliferative phase of ARDS?
|
1. Lung repair
2. Resolution of the infiltrates You can't really distinguish this clinically from the exudative phase |
|
|
What processes occur during the fibrotic phase of ARDS?
|
Permanent remodeling of the lung--> loss of long term function
|
|
|
What do you need to keep in mind for patients with ARDS on a vent?
|
Lungs have less volume, are less compliant
Give them a smaller tidal volume |
|
|
With ventilating patients, what is a problem of high respiratory rates? What do you have to do sometimes to achieve this?
|
Hypercapnea
This is acceptable due to the fact that damaging their lungs is worse than having them have a low blood pH Sedate them. |
|
|
How should you decide on PEEP for a patient? Why is this a concern"
|
Titrate to the level at which you have the best O2 sats
You can impair venous return |
|
|
What position is best for improving oxygenation in patients? Why?
|
Prone position
Best matches V and Q |
|
|
What is the ventilation limit for RR in ARDS? Pressure? TV?
|
35 bpm
30 cm H20 6 cc/kg |
|
|
What is a risk of keeping someone on 100% O2 for too long?
|
Oxygen toxicity long term
|
|
|
What are some ways not related to ventilator settings that you can improve oxygenation?
|
Prone positioning
Inhaled NO |
|
|
What are some medications that you can give to people for improving the symptoms from ARDS? What is the effect of doing this?
|
Diuretics to decrease the amount of lung water
Gets them off the vent earlier, but doesn't improve mortality Only give this to patients if they're hemodynamically stable! If they're super hypotensive, don't do it! |
|
|
When in the course of ARDS should you consider giving systemic steroids?
|
Late in the course.
|